The researcher developed this literature review by analyzing the scholarly research focused on older adults’ technology acceptance, IoT developments for them to age at home longer, and the context in which researchers applied the theories. The focus of this study was older adults’ voluntary acceptance of IoT technologies in their home to realize the purported benefits. Not all older adults had Internet access in their homes, the latest smartphone, or tablet technologies [
43,
63]. Older adults may not have comprehended the price burden to purchase the services and technologies to enable their use. Older adults were growing faster than any other population group, were predicted to reach 71 million by 2030, and to overwhelm the healthcare industry due to insufficient assisted living infrastructures and healthcare professionals to support them [
64]. The deployment of IoT into the healthcare industry resulted in a 41% increase in economic growth, the largest of any market, and was purported to allow older adults to age in their own homes longer, safer, and with more independence [
15,
23,
63,
65].
2.2.1. The Internet of Things and Aging in Place
The introduction to
Section 1 provided a high-level explanation of the Internet of Things (IoT). This section provides more details and context into the IoT as it relates to the technologies for older adults to age in their homes longer, increase safety, security, and maintain quality of life standards. The IoT is the concept that virtual and physical objects (e.g., refrigerators, stoves, and carbon monoxide monitors) have unique identifiers, are connected to the Internet, and communicate with each other [
26,
66,
67]. In the context of aging in place, a human could also be connected to, and automatically communicate with, objects through a wearable or implanted medical device [
68]. Heartbeat, glucose, respiration, or temperature monitors have been used to continuously monitor patient vitals and send that data to a cloud environment where a health practitioner could retrieve and analyze it [
69,
70,
71].
In addition to objects and humans, the IoT connects animals, plants, buildings, automobiles, and scooters [
72]. This ubiquitous communication enabled new healthcare solutions for aging adults, such as IoT-based rehabilitation, telemedicine, and activity tracking [
73,
74]. Sensors, actuators, networking, wireless, computers, and software were combined to collect, send, receive, process, and analyze data. These technologies combined with preventative healthcare were viewed as the optimal means to ensure that older adults remained healthy and active, supporting their independence [
8,
17].
The ratio of adults above the age of 60 to working age adults in the U.S. was increasing significantly, and organizations expect the total number of older adults to exceed the number of persons under the age of 18 by 2035 [
75]. Researchers studying life expectancy across 35 countries reported that an increase in older adults would be a global reality [
76,
77]. If these predictions are correct, older adults will comprise 30% of the population and will likely continue to increase due to a consistent decline in population growth [
75]. As people age, their vision, hearing, cognitive, and physical abilities may decline, which can contribute to unsafe conditions. These include wandering outside the home at night, forgetting to turn off the stove, falling in the bathroom, or tripping over an object.
The rapid growth of the aging population, their naturally declining health, and the increasing demand on healthcare providers spurred research into technologies that could be used by older adults to maintain independence, health, safety, and quality of life [
73,
74,
77,
78]. Researchers combined IoT technologies in different ways for older adults to monitor their home environments, provide safety alerts, communicate over the Internet, and overcome disabilities [
21,
74,
78,
79]. Virtual assistants such as Alexa, Amazon Echo, and Google Home enabled vision impaired persons to obtain news, set reminders, and communicate with others [
80].
The academic literature on IoT solutions to age in place longer focused heavily on technologies, frameworks, and experiments driven by industry requirements (e.g., healthcare, or technical developers) rather than the needs of the older adults [
70,
71,
74,
81]. Several themes emerged from synthesizing the academic literature, which correlated some of the constructs of the UTAUT. These included effort expectancy, behavioral intention to use, performance expectancy, facilitating conditions, habit, and price value. Many researchers did not demonstrate an understanding of older adults’ characteristics and the barriers to their acceptance of technology. Older adults had less experience with and confidence in using newer technologies [
82,
83,
84]. They preferred to continue using old, outdated technologies instead of adopting the newer [
15,
43,
63,
85]. Most of the IoT solutions proposed or experimented with required newer technologies and user familiarity with them [
81,
83,
86,
87].
In some cases, the older adults were physically unable to manipulate the technology. They required training, ongoing technical support, coaching, and experience with new technologies before they adopted [
15,
43,
84,
88]. Older adults who suffered from cardiovascular disease, heart failure, stroke, chronic illness, with a fall history, or diminishing capabilities were more willing to adopt new technologies to compensate as a perceived benefit [
45,
46,
63,
65,
89]. Older adults were sensitive to the cost of new technologies, which was an adoption barrier [
83,
84,
90]. Many of the researchers did not limit their target population to older adults, which made up a small percentage of the samples [
39,
45,
74,
91,
92]. Finally, most of the researchers did not demonstrate an understanding of their chosen technology acceptance model’s designed context. Researchers investigated consumer adoption with corporate adoption models and vice versa [
30,
67,
93,
94,
95,
96].
2.2.2. Conflicting Technology Acceptance Models in Research
The main topic of this research was technology acceptance, and to investigate this problem one needed to assess technology acceptance theories. Research on technology acceptance began when different industries were looking to leverage computing in their business processes, which was a significant investment [
97]. Employees were not familiar with the technology, and industries were hesitant to invest in computing that would not be adopted or used by personnel. Researchers lacking a technology acceptance theory turned to behavioral decision theory, or the study of decision-making, which was rooted in probability studies and risk taking psychology [
98]. Researchers used the behavior decision theory, qualitatively and quantitatively. Businesses financed research to understand the cost and effort of adopting technology in their processes and to measure users’ perceptions of the involuntary technology, which led to the development of the technology acceptance model TAM [
99]. Davis [
100] eventually established the reliability and validity of the model, where perceived usefulness and perceived ease of use forecasted user intention to use technology in businesses. Since then, the TAM has been one of the most used models in predicting intention to use from the corporate and consumer perspective, although not designed for the later.
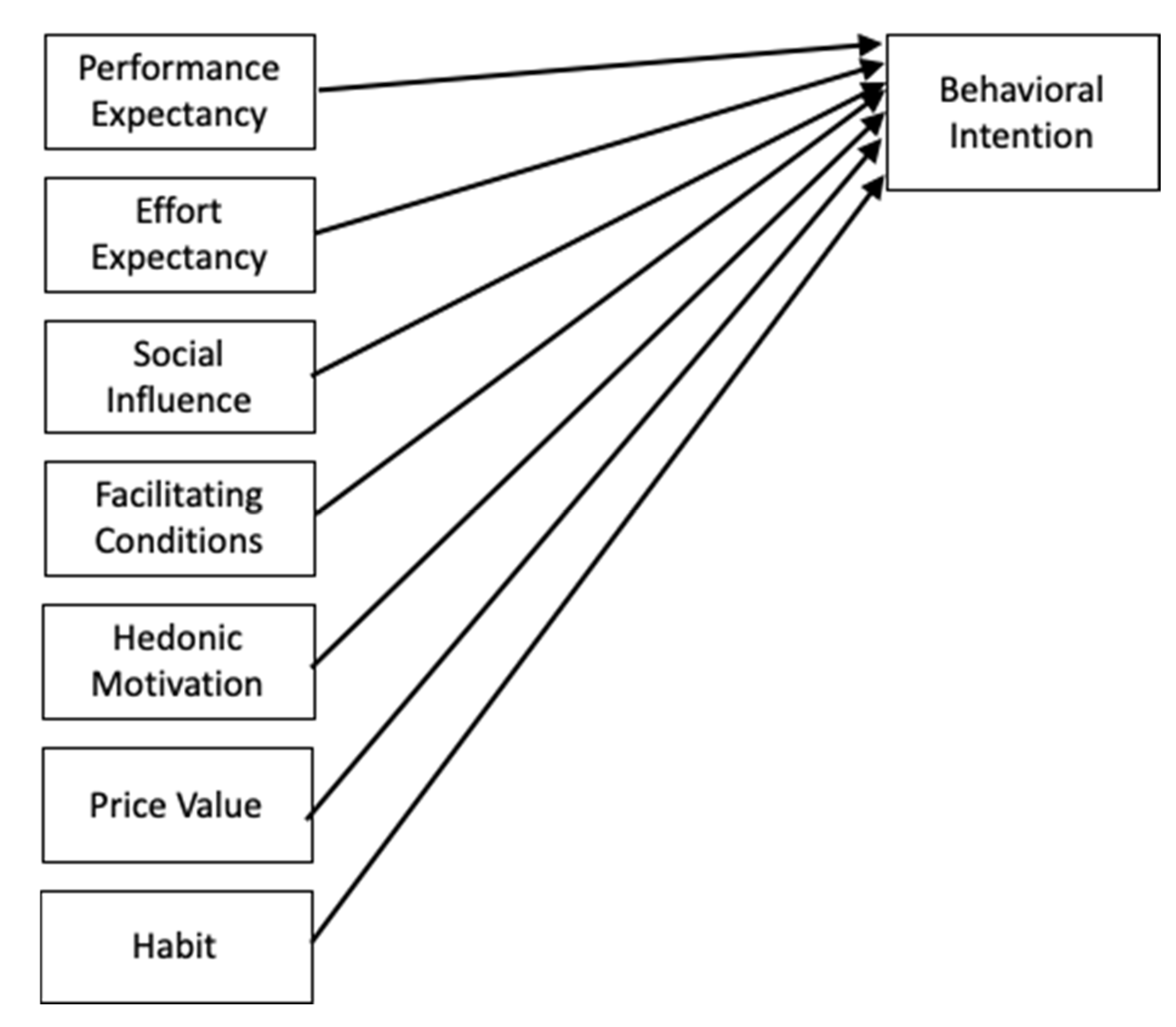
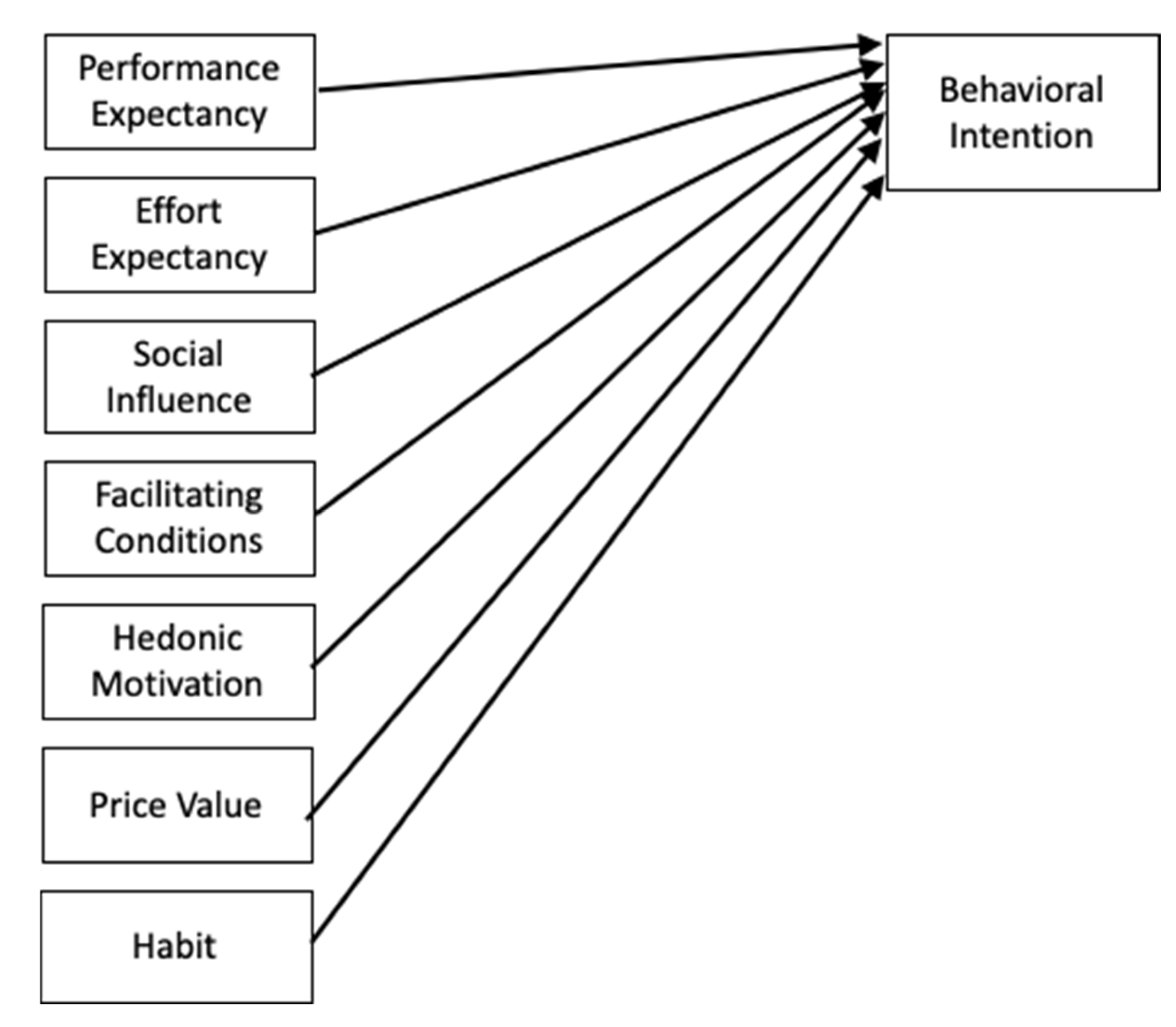
In 2003, Venkatesh et al. developed a unified theory that leveraged the contributions of many theoretical models developed up to that time. They evaluated each of these models, synthesizing them to develop the unified theory of acceptance and use of technology (UTAUT). However, the contextual focus was still on business organizations where technology acceptance is involuntary. The researchers developed, tested, and validated the survey instrument for reliability. The predictor variables were performance expectancy, effort expectancy, social influence to use technology, facilitating conditions, which represents training and support, and behavioral intention. The moderating variables were gender, age, experience with the technology, and voluntariness of use. The dependent variable of the model was use behavior. The researchers’ results indicated that performance expectancy, effort expectancy, and social influence of the users of the technology to improve their job effectiveness were direct predictors of intention to use from a business perspective. Many researchers have continued to use the UTAUT to predict consumer intention and adoption, even though it was designed to predict use in the business context.
The UTAUT was combined with the TAM and other theories by researchers, adding such constructs as personal innovativeness, device anxiety, ubiquity value, and cognitive feedback [
101]. Regardless, the TAM and the UTAUT were developed and demonstrated as reliable for involuntary business situations. A recent survey of the academic literature on technology to assist older adults showed that more than 60% of the studies used no theory, 20% used the TAM, and 8% used the UTAUT [
62]. A more recent and contextually appropriate theory was developed, and explicitly designed for voluntary consumer technology acceptance (UTAUT2).
From a theoretical and practical perspective, researchers used technology acceptance models and theories developed within a business environment to apply to noncorporate contexts with varying and conflicting results. Researchers studying technology acceptance used the UTAUT, UTAUT2, TAM, and qualitative discovery methods. The results were difficult to correlate because the researchers used a variety of constructs and often used a model or theory to predict technology acceptance out of the contextual environment for which they were developed. Researchers used the models inconsistently, resulting in variations of the predictors, as shown in
Table 1 [
30].
Researchers identified performance expectancy, effort expectancy, social influence, and habit as the most significant predictors, with habit identified as such in three studies, and the others occurred as significant in two studies. Findings for the second most influential predictors were just as varied as the primary. Additionally, only four of the studies included the construct, price value, and it was only significant in one. The variance in the findings provides a researcher with cause to scrutinize the research designs more closely.
Ain et al. [
102] explored students’ acceptance of a learning management system (LMS) with the UTAUT2. In this study, the educational institution chose the learning management system and provided it to the students, who had no choice in purchasing the tool or using it. The researchers removed the price value construct and substituted learning value. Learning value and social influence were the most significant predictors of behavioral intention, followed by performance expectancy. A similar study by Nair et al. [
106] using UTAUT2 showed that performance expectancy and habit were the most significant and positive predictors of behavioral intention. Researchers also reported that price value in the context of students’ fees was a significant predictor.
Magsamen-Conrad et al. [
20] performed a UTAUT study investigating whether there were multigenerational differences in adopting tablet technology. Researchers developed the UTAUT for the business environment where acceptance of the technology is involuntary, and performance expectancy was the single most significant predictor to acceptance [
16]. Magsamen-Conrad et al. [
20] reported that the most significant generational differences to tablet adoption were effort expectancy, facilitating conditions, and performance expectancy, which were all significant in the UTAUT2, indicating that the researchers should have used the later. Gao et al. [
104] investigated users’ adoption of wearable fitness technology using the consumer focused UTAUT2 and added a construct for risk. Although the researchers used a consumer-focused theory, they did not include the constructs of hedonic motivation, price value, or habit, which were significant predictors in the UTAUT2. They reported that participants’ perceived privacy risk had the most significant and negative impact on their behavioral intention to use the devices over social influence.
However, it had a positive statistical significance. Effort expectancy was a significant predictor, and consistently so when the technology was health related. This construct was the only one from the UTAUT2 that was not rejected and found to be significant in the study by Koivumäki et al. [
91] on acceptance of databased preventative healthcare services. Koivumäki et el. did not test the construct price value because there was no known cost model for the healthcare services at the time of the study. As one might expect of an emerging technological market, many of the IoT solutions studied were technical proof of concepts or experimentations. Much of the academic research literature on IoT technology to help older adults age at home longer focused on IoT for human activity monitoring [
2,
71,
81,
107,
108], remote healthcare [
39,
87,
109], and the technical challenges caused by the implementation of IoT in these environments [
25,
30,
110,
111].
2.2.3. Explicit IoT Research for Older Adults to Age in Place
An increasing number of IoT technologies called smart home devices were in the consumer market explicitly designed for older adults. These included remote monitoring, automatic stove shutoff, voice activated assistants, smart phone applications to control lights, and emergency alert systems. Arthanat et al. [
46] examined older adult ownership of these types of smart home devices. The researchers explicitly targeted the population of adults 60 years or older. Women ages 60 to 70 years old who had an impairment, fall history, and were experienced with technology were early adopters of the devices. The researchers reported that the IoT technologies promoted or used in experiments for older adults to age in place longer were the least desired by them. Older adults rejected remote home monitoring, using a smartphone to control appliances, motion activated cameras, voice activated assistants, and emergency alerting systems.
Conversely, they reported that a significant number of older adults in the study were using carbon monoxide alarms, manually programmable or automatic set thermostats, motion sensing lights, and backup generators. The results indicated that older adults who were concerned about safety were interested in purchasing water leak detectors, backup generators, and automatic shutoff technologies for the stove. However, they did not own these technologies at the time of the study. This study confirmed others in that older adults who perceived their independence or health declining were more likely to adopt the solutions to compensate for their condition [
15,
46,
63,
65]. The adoption of technology also presumes that the beneficiaries (older adults) will have Internet access in their homes or use a smartphone to go online [
46,
112].
Irizarry et al. [
112] studied older adults’ perceptions of a health portal as a means for them to receive laboratory results, communicate with caregivers, and ask questions. The themes that emerged support many other studies. The researchers reported that older adults required training and support for technology (facilitating conditions). Many of the study’s participants stated they had little to no experience with computers and no Internet access in their homes. Although persons in the U.S. are increasingly using their smartphones to go online over in-home broadband [
113], prior research showed that older adults held onto older technology longer than younger persons, as previously stated [
15,
63]. Seriously or chronically ill participants found the health portal convenient for obtaining lab results. Still, they felt their conditions were too complicated to effectively communicate with caregivers through secure messaging as the only means [
112]. They perceived the portal as a poor substitute for direct interaction with clinical personnel.
Researchers reported that technology contributed to further isolation of older adults and less communication with the broader community in several studies [
15,
58,
65,
83,
84]. Developers of IoT solutions for adults to age in place longer should consider the potential isolation caused by implementing remote monitoring sensors, pushing health portals as a single solution, and supplementing caregivers with autonomous robots. The Technology in Later Life study was designed to determine if there was a digital divide between rural and urban adults aged 70 and above in the U.K. and Canada [
114]. This qualitative study found that facilitating conditions, access to technology, and security influenced older adults’ technology use. Detractors to technology use were apprehensions, lack of interest, and difficultly in learning how to use it [
30].
2.2.4. Older Adults’ Acceptance of IoT to Age in Place
Cardiovascular disease, heart failure, stroke, chronic illness, a fall history, or diminishing capabilities were shown to positively influence older adults to adopt new technologies [
45,
46,
63,
65,
89]. In the U.S., cardiovascular disease is the primary cause of death and rising healthcare costs for older adults, and as much as 30% were hospitalized again within a month [
90]. Healthcare providers and researchers started investigating the use of mobile health capabilities for home based cardiac rehabilitation instead of the traditional center-based approach [
90,
115]. A center-based cardiac rehabilitation approach proved to play an essential role in preventing secondary cardiovascular disease events. However, more than 80% of the patients eligible for the services in the U.S. did not participate, and only 50% of the doctor referred patients participated [
115]. Additionally, older adults were under referred and, a significant number of those who were, did not complete the rehabilitation sessions required.
In the European Union (EU), approximately 30% of cardiovascular disease patients received rehabilitative treatment, and few older adults willingly participated [
88]. Many of the researchers purported that the home-based option would increase patient participation [
104,
106]. The academic literature discussed several ongoing trials and clinical studies [
88,
115,
116]. For example, researchers in Australia published their trial results indicating that patients who used a smartphone-based home method were 30% more likely to participate in rehabilitation, and 32% more likely to complete the intervention as prescribed (as cited in [
115]).
Researchers recently published results from a four-year observational study on cardiac rehabilitation in elderly patients across western Europe [
117]. The researchers of the European Cardiac Rehabilitation programs in the Elderly (EU-CaRE) assessed the effectiveness of cardiac rehabilitation centers in eight European Union countries for adults 65 years and older. The research design included patients who declined traditional cardiac rehabilitation and randomly assigned to either the experimental group or the control group. The experimental group received personalized in-home mobile cardiac rehabilitation, and the control group received no intervention [
88]. The in-home cardiac rehabilitation approach included a smartphone, heartrate monitoring, and coaching. Results indicated that after six months of the in-home rehabilitation, older adults’ vitals and health significantly improved as compared to those in the control group who received no rehabilitative care [
117]. These results indicated the importance of understanding older adults’ perceptions of the proposed solutions [
30].
2.2.5. IoT Adoption Challenges
The most prominent barrier to adopting IoT technologies to age in place was that most researchers approached the subject from the perspective of healthcare providers or technologists [
71,
81,
107,
108,
118]. The academic literature showed that older adults were reluctant to change to newer technologies [
63,
85,
119], lacked sufficient experience [
41,
82,
83,
84], required extensive support [
15,
41,
43,
84,
88], and resisted adoption unless they were seriously ill, impaired, or suffered a chronic illness [
45,
46,
63,
65,
89]. These findings indicated that as their health declined, older adults were more inclined to adopt and use newer technologies, regardless of their experience with it, knowledge of it, and the associated risks. Sixty-seven percent of older adults fell victim to an online scam, malicious software, or a hack [
120]. The most common and successful attack vector used by adversaries was through people [
121]. These facts raise ethical considerations and concerns that healthcare providers, IoT researchers, and developers should recognize and dealt with [
30].
The academic literature on IoT solutions to age in place longer focused heavily on technologies, frameworks, and experiments driven by industry requirements (e.g., healthcare or technology developers) rather than the needs of the older adults [
2,
70,
71,
74,
81]. Solutions driven by technological and organizational capabilities, and developed without user involvement will not likely meet their needs and requirements [
16,
17,
47]. In addition, the researchers focused on technical solutions neglected the social issues of increased isolation and exclusion [
14,
85,
119,
122,
123]. A few recent research efforts specifically focused on involving older adults in the development and design of IoT solutions to counter this barrier to adoption [
41,
42,
124].





{kind=link}
{kind=link}
{kind=link}