


Coil- and Plug-Assisted Transvenous Retrograde Obliteration (CARTO/PARTO) in the Treatment of Gastric Varices: A European Single Centre Experience

 , ,
, ,
Abstract
1. Introduction
2. Results
Safety
3. Materials and Methods
3.1. Methods
3.2. Technique
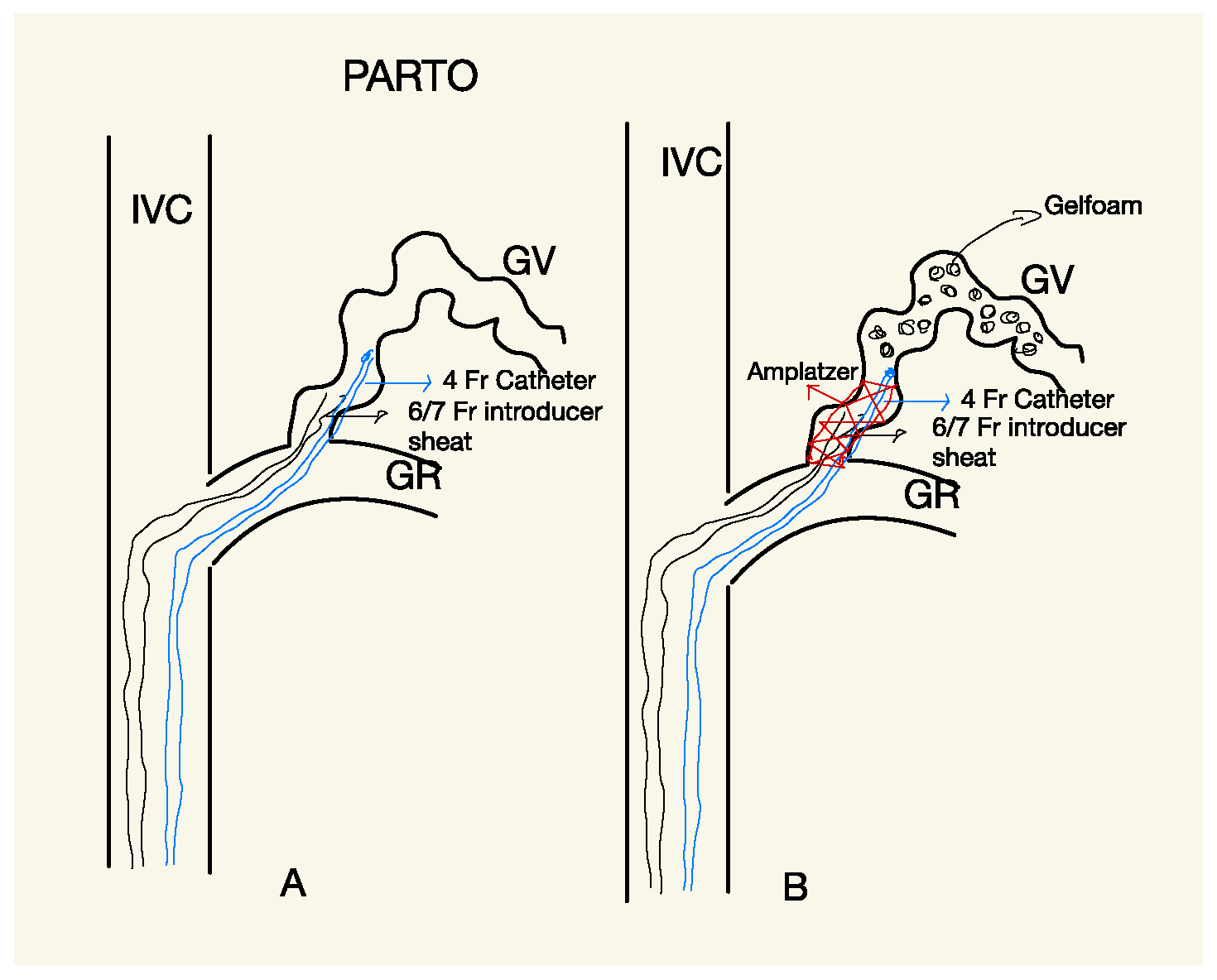
3.2.1. PARTO
3.2.2. CARTO
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sarin, S.K.; Lahoti, D.; Saxena, S.P.; Murthy, N.S.; Makwana, U.K. Prevalence, classification and natural history of gastric varices: A long-term follow-up study in 568 portal hypertension patients. Hepatology 1992, 16, 1343–1349. [Google Scholar] [CrossRef] [PubMed]
- Paleti, S.; Nutalapatim, V.; Fathallah, J.; Jeepalyam, S.; Rustagi, T. Balloon-Occluded Retrograde Transvenous Obliteration (BRTO) Versus Transjugular Intrahepatic Portosystemic Shunt (TIPS) for Treatment of Gastric Varices Because of Portal Hypertension a Systematic Review and Me-ta-Analysis. Swathi. J. Clin. Gastroenterol. 2019, 54, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Schubert, T.T.; Schnell, G.A.; Walden, J.M. Bleeding from varices in the gastric fundus complicating sclerotherapy. Gastrointest. Endosc. 1989, 35, 268–269. [Google Scholar] [CrossRef] [PubMed]
- Florentina, R.I.; Nikolaos, T.; Pyrsopoulos, M.J.; Ion, C.T.; Zhonghua, S. Liver Diseases a Multidisciplinary Textbook; Springer Nature Switzerland AG: Cham, Switzerland, 2020; ISBN 978-3-030-24431-6. [Google Scholar]
- Kim, M.Y.; Um, S.H.; Baik, S.K.; Seo, Y.S.; Park, S.Y.; Lee, J.I.; Lee, J.W.; Cheon, G.J.; Sohn, J.H.; Kim, T.Y.; et al. Clinical features and outcomes of gastric variceal bleeding: Retrospective Korean multicenter data. Clin. Mol. Hepatol. 2013, 19, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Emenena, I.; Emenena, B.; Kweki, A.G.; Aiwuyo, H.O.; Osarenkhoe, J.O.; Iloeje, U.N.; Ilerhunmwuwa, N.; Torere, B.E.; Akinti, O.; Akere, A.; et al. Model for End Stage Liver Disease (MELD) Score: A Tool for Prognosis and Prediction of Mortality in Patients with Decompensated Liver Cirrhosis. Cureus 2023, 15, e39267. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chang, M.-Y.; Kim, M.-D.; Kim, T.; Shin, W.; Shin, M.; Kim, G.M.; Won, J.Y.; Park, S.I.; Lee, D.Y. Plug-Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Variceal Hemorrhage. Korean J. Radiol. 2016, 17, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Gwon, D.I.; Ko, G.-Y.; Yoon, H.-K.; Sung, K.-B.; Kim, J.H.; Shin, J.H.; Ko, H.K.; Song, H.-Y. Gastric Varices and Hepatic Encephalopathy: Treatment with Vascular Plug and Gelatin Sponge–assisted Retrograde Transvenous Obliteration—A Primary Report. Radiology 2013, 268, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Gwon, D.I.; Kim, Y.H.; Ko, G.-Y.; Kim, J.W.; Ko, H.K.; Kim, J.H.; Shin, J.H.; Yoon, H.-K.; Sung, K.-B. Vascular Plug–Assisted Retrograde Transvenous Obliteration for the Treatment of Gastric Varices and Hepatic Encephalopathy: A Prospective Multicenter Study. J. Vasc. Interv. Radiol. 2015, 26, 1589–1595. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Yoo, J.-J.; Kim, S.G.; Jeong, S.W.; Jang, J.Y.; Lee, S.H.; Kim, H.S.; Lee, J.M.; Shim, J.J.; Cheon, G.J.; et al. Change in Portal Pressure and Clinical Outcome in Cirrhotic Patients with Gastric Varices after Plug-Assisted Retrograde Transvenous Obliteration. Gut Liver 2020, 14, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.W.; Saab, S.; Gomes, A.S.; Busuttil, R.; McWilliams, J.; Durazo, F.; Han, S.-H.; Goldstein, L.; Tafti, B.A.; Moriarty, J.; et al. Coil-Assisted Retrograde Transvenous Obliteration (CARTO) for the Treatment of Portal Hypertensive Variceal Bleeding: Preliminary Results. Clin. Transl. Gastroenterol. 2014, 5, e61. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, A.; Jogo, A.; Kageyama, K.; Sohgawa, E.; Hamamoto, S.; Hamuro, M.; Kamino, T.; Miki, Y. Utility of Coil-Assisted Retrograde Transvenous Obliteration II (CARTO-II) for the Treatment of Gastric Varices. Cardiovasc. Interv. Radiol. 2020, 43, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Saad, W.E. Balloon-Occluded Retrograde Transvenous Obliteration of Gastric Varices: Concept, Basic Techniques, and Outcomes. Semin. Intervent. Radiol. 2012, 29, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Waguri, N.; Osaki, A.; Watanabe, Y.; Matsubara, T.; Yamazaki, S.; Yokoyama, H.; Kimura, K.; Wakabayashi, T.; Mito, M.; Yakubo, S.; et al. Balloon-occluded retrograde transvenous obliteration for gastric varices improves hepatic functional reserve in long-term follow-up. JGH Open 2021, 5, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Saad, W.E.A.; Wagner, C.; Al-Osaimi, A.; Bliebel, W.; Lippert, A.; Davies, M.G.; Sabri, S.S.; Turba, U.C.; Matsumoto, A.H.; Angle, J.; et al. The Effect of Balloon-Occluded Transvenous Obliteration of Gastric Varices and Gastrorenal Shunts on the Hepatic Synthetic Function: A Comparison Between Child-Pugh and Model for End-Stage Liver Disease Scores. Vasc. Endovasc. Surg. 2013, 47, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Sasaki, R.; Nishimura, T.; Matsuda, T.; Maeda, M.; Iwamoto, T.; Saeki, I.; Hidaka, I.; Takami, T.; Sakaida, I. Comparison of patients with hepatic encephalopathy and those with gastric varices before and after balloon-occluded retrograde transvenous obliteration. Hepatol. Res. 2018, 48, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Saad, W.E.A.; Sabri, S.S. Balloon-occluded Retrograde Transvenous Obliteration (BRTO): Technical Results and Outcomes. Semin. Interv. Radiol. 2011, 28, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Masood, I.; Moshksar, A.; Wong, B.; Khan, H.; Saleem, A. A comprehensive review of transvenous obliteration techniques in the management of gastric varices. Diagn. Interv. Radiol. 2023, 29, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kim, Y.H.; Kim, C.S.; Kang, U.R.; Kim, S.H.; Kim, J.H. Comparison of balloon-occluded retrograde transvenous obliteration (BRTO) using ethanolamine oleate (EO), BRTO using sodium tetradecyl sulfate (STS) foam and vascular plug-assisted retro-grade transvenous obliteration (PARTO). Cardiovasc. Intervent. Radiol. 2016, 39, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Taehwan, K.; Heechul, Y.; Chun, K.L.; Gun, B.K. Vascular Plug Assisted Retrograde Transvenous Obliteration (PARTO) for Gastric Varix Bleeding Patients in the Emergent Clinical Setting. Yonsei Med. J. 2016, 57, 973–979. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Sex | Causes of Liver Cirrhosis | MELD Score | Child–Pugh Class | GOV Type | Previous GV Bleeding | Technique | Vascular Access | Material | Time (min) | Postprocedural Complications | Follow-Up (1 year) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 41 | F | alcoholic | 5 | A | GOV1 | Yes | PARTO | Jugular | 8 mm Amplatzer | 165 | minor ascites hydrothorax | no GV varices |
| 2 | 92 | M | hepatitis C virus | 13 | B | IGV1 | Yes | PARTO | Jugular | 12 mm Amplatzer | 159 | None | abundant ascites/no GV varices |
| 3 | 56 | F | alcoholic | 12 | B | GOV1 | Yes | PARTO | Jugular | 7 mm Amplatzer | 145 | None | no GV varices |
| 4 | 51 | M | NASH | 11 | A | GOV1 | No | CARTO | Femoral | Detachable Coils | 120 | minor portal thrombosis | no GV varices |
| 5 | 54 | F | hepatitis C virus | 15 | B | GOV1 | Yes | CARTO | Femoral | Detachable Coils | 48 | minor ascites/hydrothorax | no GV varices |
| 6 | 54 | M | alcoholic | 15 | B | IGV1 | Yes | CARTO | Femoral | Detachable Coils | 85 | None | transplantation 7 months after |
| 7 | 63 | M | alcoholic | 9 | A | GOV1 | Yes | CARTO | Femoral | Detachable Coils | 97 | None | no GV varices |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelle, G.; Andresciani, F.; Messina, M.; Nardelli, S.; Ridola, L.; Notarianni, E.; Saltarelli, A.; Gioia, S.; Tanzilli, A.; Ambrogi, C. Coil- and Plug-Assisted Transvenous Retrograde Obliteration (CARTO/PARTO) in the Treatment of Gastric Varices: A European Single Centre Experience. Gastrointest. Disord. 2024, 6, 742-752. https://doi.org/10.3390/gidisord6030050
Pelle G, Andresciani F, Messina M, Nardelli S, Ridola L, Notarianni E, Saltarelli A, Gioia S, Tanzilli A, Ambrogi C. Coil- and Plug-Assisted Transvenous Retrograde Obliteration (CARTO/PARTO) in the Treatment of Gastric Varices: A European Single Centre Experience. Gastrointestinal Disorders. 2024; 6(3):742-752. https://doi.org/10.3390/gidisord6030050
Chicago/Turabian StylePelle, Giuseppe, Flavio Andresciani, Massimo Messina, Silvia Nardelli, Lorenzo Ridola, Ermanno Notarianni, Adelchi Saltarelli, Stefania Gioia, Alessandro Tanzilli, and Cesare Ambrogi. 2024. "Coil- and Plug-Assisted Transvenous Retrograde Obliteration (CARTO/PARTO) in the Treatment of Gastric Varices: A European Single Centre Experience" Gastrointestinal Disorders 6, no. 3: 742-752. https://doi.org/10.3390/gidisord6030050
APA StylePelle, G., Andresciani, F., Messina, M., Nardelli, S., Ridola, L., Notarianni, E., Saltarelli, A., Gioia, S., Tanzilli, A., & Ambrogi, C. (2024). Coil- and Plug-Assisted Transvenous Retrograde Obliteration (CARTO/PARTO) in the Treatment of Gastric Varices: A European Single Centre Experience. Gastrointestinal Disorders, 6(3), 742-752. https://doi.org/10.3390/gidisord6030050