
Insights into Personal Perceptions and Experiences of Colonoscopy after Positive FIT in the Flemish Colorectal Cancer Screening Program



Abstract
1. Introduction
2. Results
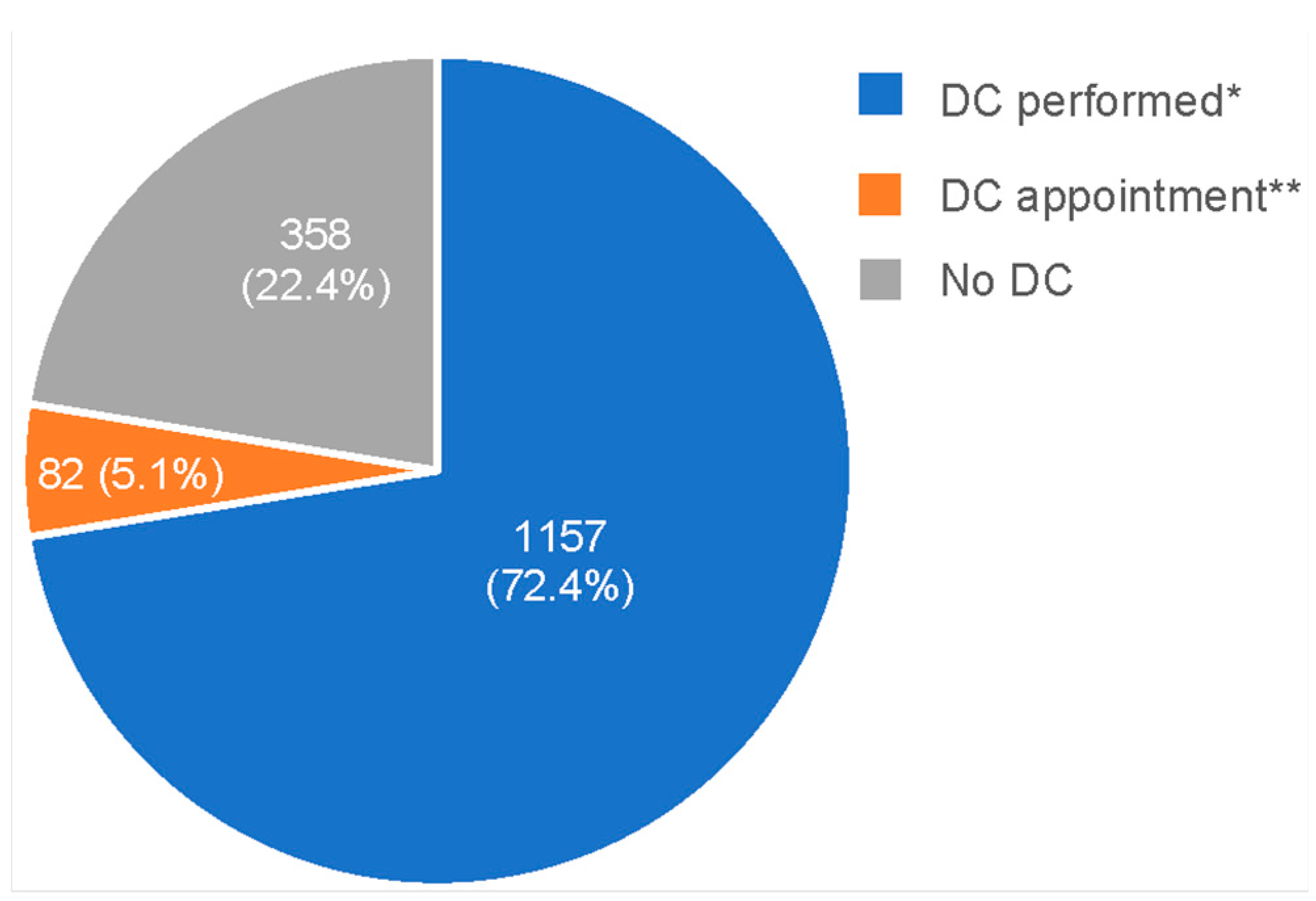
2.1. Characteristics of Study Population and Survey Response Rate
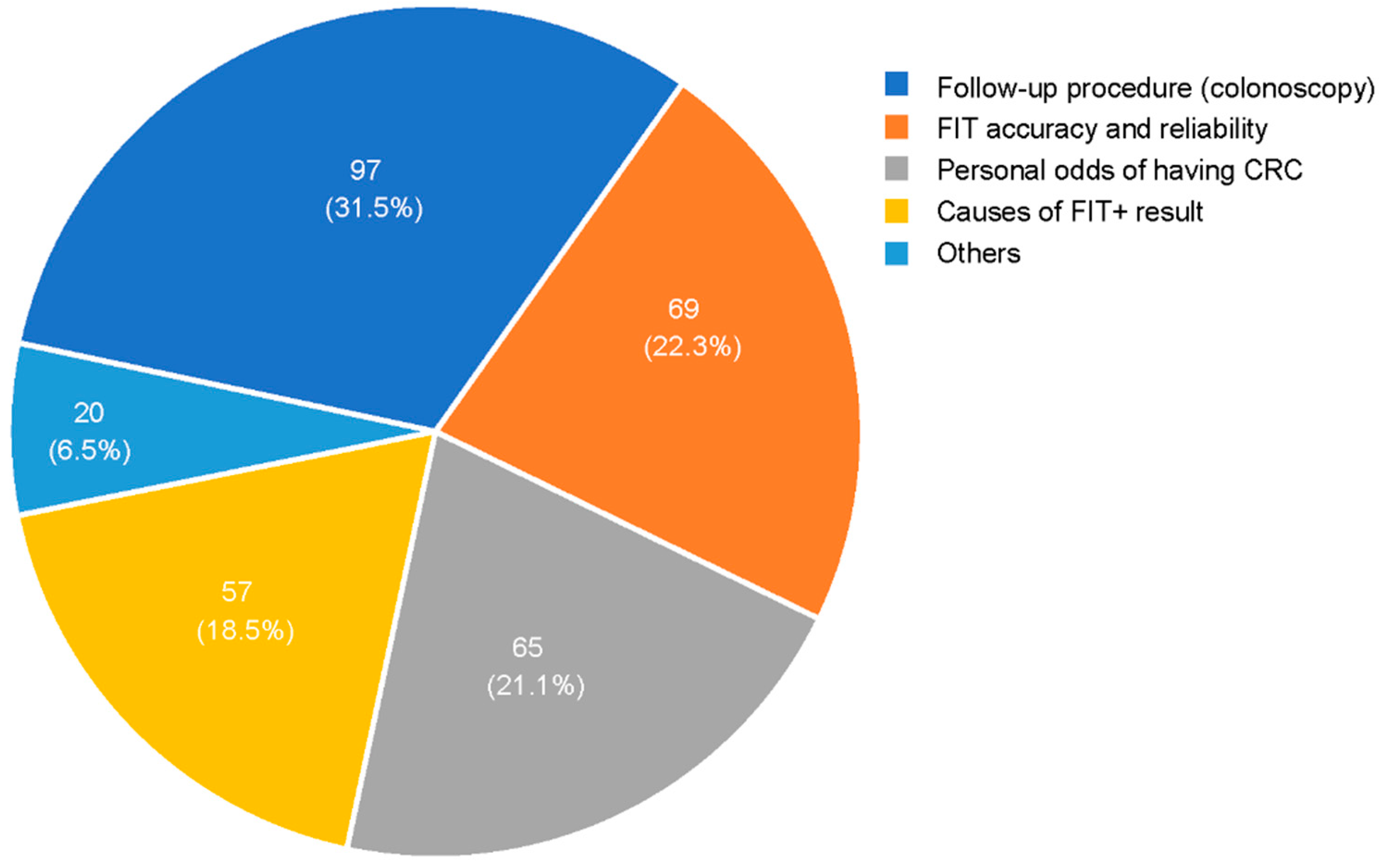
2.2. Survey Question Results
3. Discussion
4. Material and Methods
Study Design—Online Survey
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hoeck, S.; van de Veerdonk, W.; De Brabander, I. Do socioeconomic factors play a role in nonadherence to follow-up colonoscopy after a positive faecal immunochemical test in the Flemish colorectal cancer screening programme? Eur. J. Cancer Prev. 2020, 29, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Meeus, A.; Demyttenaere, B. Study Colonoscopy [Studie Colonoscopie]; Nationaal Verbond van Socialistische Mutualiteiten: Brussel, Belgium, 2020. [Google Scholar]
- Centre for Cancer Detection & Belgian Cancer Registry. Monitoring Report of the Flemish Colorectal Cancer Screening Programme. 2021. Available online: https://dikkedarmkanker.bevolkingsonderzoek.be/sites/default/files/2022-03/Jaarrapport%202021%20BVO%20naar%20kanker_0.pdf (accessed on 23 May 2023).
- Gingold-Belfer, R.; Leibovitzh, H.; Boltin, D.; Issa, N.; Tsadok Perets, T.; Dickman, R.; Niv, Y. The compliance rate for the second diagnostic evaluation after a positive fecal occult blood test: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2019, 7, 424–448. [Google Scholar] [CrossRef] [PubMed]
- Selby, K.; Senore, C.; Wong, M.; May, F.P.; Gupta, S.; Liang, P.S. Interventions to ensure follow-up of positive fecal immunochemical tests: An international survey of screening programs. J. Med. Screen. 2021, 28, 51–53. [Google Scholar] [CrossRef]
- Segnan, N.; Patnick, J.; von Karsa, L. (Eds.) European Guidelines for Quality Assurance in Colorectal Cancer Screening and Diagnosis, 1st ed.; Publications Office of the European Union: Luxembourg, 2010. [Google Scholar]
- Corley, D.A.; Jensen, C.D.; Quinn, V.P.; Doubeni, C.A.; Zauber, A.G.; Lee, J.K.; Schottinger, J.E.; Marks, A.R.; Zhao, W.K.; Ghai, N.R.; et al. Association Between Time to Colonoscopy After a Positive Fecal Test Result and Risk of Colorectal Cancer and Cancer Stage at Diagnosis. JAMA 2017, 317, 1631–1641. [Google Scholar] [CrossRef] [PubMed]
- Zorzi, M.; Battagello, J.; Selby, K.; Capodaglio, G.; Baracco, S.; Rizzato, S.; Chinellato, E.; Guzzinati, S.; Rugge, M. Non-compliance with colonoscopy after a positive faecal immunochemical test doubles the risk of dying from colorectal cancer. Gut 2022, 71, 561–567. [Google Scholar] [CrossRef]
- Hoeck, S.; De Schutter, H.; Van Hal, G. Why do participants in the Flemish colorectal cancer screening program not undergo a diagnostic colonoscopy after a positive fecal immunochemical test? Acta Clin. Belg. 2022, 77, 760–766. [Google Scholar] [CrossRef]
- Jidkova, S.; Hoeck, S.; Kellen, E.; le Cessie, S.; Goossens, M.C. Flemish population-based cancer screening programs: Impact of COVID-19 related shutdown on short-term key performance indicators. BMC Cancer 2022, 22, 183. [Google Scholar] [CrossRef]
- Hoeck, S.; Janssens, S.; Van Hal, G.; Van Herck, K. Self-Reported and Objective Impact of the COVID-19 Pandemic on Planning, Compliance and Timeliness of a Diagnostic Colonoscopy after a Positive FIT Screening Result in the Flemish Colorectal Cancer Screening Program. Gastrointest. Disord. 2022, 4, 129–140. [Google Scholar] [CrossRef]
- Mutneja, H.R.; Bhurwal, A.; Arora, S.; Vohra, I.; Attar, B.M. A delay in colonoscopy after positive fecal tests leads to higher incidence of colorectal cancer: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2021, 36, 1479–1486. [Google Scholar] [CrossRef]
- Dalton, A.R.H. Incomplete diagnostic follow-up after a positive colorectal cancer screening test: A systematic review. J. Public Health 2018, 40, e46–e58. [Google Scholar] [CrossRef]
- Kerrison, R.S.; Travis, E.; Dobson, C.; Whitaker, K.L.; Rees, C.J.; Duffy, S.W.; von Wagner, C. Barriers and facilitators to colonoscopy following fecal immunochemical test screening for colorectal cancer: A key informant interview study. Patient Educ. Couns. 2022, 105, 1652–1662. [Google Scholar] [CrossRef] [PubMed]
- Llovet, D.; Serenity, M.; Conn, L.G.; Bravo, C.A.; McCurdy, B.R.; Dube, C.; Baxter, N.N.; Paszat, L.; Rabeneck, L.; Peters, A.; et al. Reasons For Lack of Follow-up Colonoscopy Among Persons With A Positive Fecal Occult Blood Test Result: A Qualitative Study. Am. J. Gastroenterol. 2018, 113, 1872–1880. [Google Scholar] [CrossRef] [PubMed]
- Amlani, B.; Radaelli, F.; Bhandari, P. A survey on colonoscopy shows poor understanding of its protective value and widespread misconceptions across Europe. PLoS ONE 2020, 15, e0233490. [Google Scholar] [CrossRef] [PubMed]
- Mog, A.C.; Liang, P.S.; Donovan, L.M.; Sayre, G.G.; Shaukat, A.; May, F.P.; Glorioso, T.J.; Jorgenson, M.A.; Wood, G.B.; Mueller, C.; et al. Timely Colonoscopy After Positive Fecal Immunochemical Tests in the Veterans Health Administration: A Qualitative Assessment of Current Practice and Perceived Barriers. Clin. Transl. Gastroenterol. 2022, 13, e00438. [Google Scholar] [CrossRef] [PubMed]
- Bertels, L.; Lucassen, P.; van Asselt, K.; Dekker, E.; van Weert, H.; Knottnerus, B. Motives for non-adherence to colonoscopy advice after a positive colorectal cancer screening test result: A qualitative study. Scand. J. Prim. Health Care 2020, 38, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Olchowska-Kotala, A.; Bajcar, B. Predictors of Undergoing Colonoscopy, Does Time Horizon Matter? J. Prim. Prev. 2020, 41, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Issaka, R.B.; Bell-Brown, A.; Snyder, C.; Atkins, D.L.; Chew, L.; Weiner, B.J.; Strate, L.; Inadomi, J.M.; Ramsey, S.D. Perceptions on Barriers and Facilitators to Colonoscopy Completion After Abnormal Fecal Immunochemical Test Results in a Safety Net System. JAMA Netw. Open 2021, 4, e2120159. [Google Scholar] [CrossRef]
- Bobridge, A.; Bampton, P.; Cole, S.; Lewis, H.; Young, G. The psychological impact of participating in colorectal cancer screening by faecal immuno-chemical testing—The Australian experience. Br. J. Cancer 2014, 111, 970–975. [Google Scholar] [CrossRef]
- Kapidzic, A.; Korfage, I.J.; van Dam, L.; van Roon, A.H.; Reijerink, J.C.; Zauber, A.G.; van Ballegooijen, M.; Kuipers, E.J.; van Leerdam, M.E. Quality of life in participants of a CRC screening program. Br. J. Cancer 2012, 107, 1295–1301. [Google Scholar] [CrossRef]
- Bynum, S.A.; Davis, J.L.; Green, B.L.; Katz, R.V. Unwillingness to participate in colorectal cancer screening: Examining fears, attitudes, and medical mistrust in an ethnically diverse sample of adults 50 years and older. Am. J. Health Promot. 2012, 26, 295–300. [Google Scholar] [CrossRef]
- Decruz, G.M.; Ng, C.H.; Lim, K.T.; Devi, M.K.; Lim, F.; Tai, C.H.; Chong, C.S. Afterthoughts on colonoscopy. Was it that bad? J. Med. Screen. 2021, 28, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Vemulapalli, K.C.; Lahr, R.E.; Rex, D.K. 2021 Patient Perceptions Regarding Colonoscopy Experience. J. Clin. Gastroenterol. 2023, 57, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Flugelman, A.A.; Stein, N.; Segol, O.; Lavi, I.; Keinan-Boker, L. Delayed Colonoscopy Following a Positive Fecal Test Result and Cancer Mortality. JNCI Cancer Spectr. 2019, 3, pkz024. [Google Scholar] [CrossRef] [PubMed]
- Hochbaum, G.; Rosenstock, I.; Kegels, S. Health Belief Model; Public Health Service: Washington, DC, USA, 2016. (Original Work Published 1952). [Google Scholar]
- Cheng, S.Y.; Li, M.C.; Chia, S.L.; Huang, K.C.; Chiu, T.Y.; Chan, D.C.; Chiu, H.M. Factors affecting compliance with confirmatory colonoscopy after a positive fecal immunochemical test in a national colorectal screening program. Cancer 2018, 124, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Selby, K.; Baumgartner, C.; Levin, T.R.; Doubeni, C.A.; Zauber, A.G.; Schottinger, J.; Jensen, C.D.; Lee, J.K.; Corley, D.A. Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests: A Systematic Review. Ann. Intern. Med. 2017, 167, 565–575. [Google Scholar] [CrossRef]
- DeGroff, A.; Schroy, P.C., 3rd; Morrissey, K.G.; Slotman, B.; Rohan, E.A.; Bethel, J.; Murillo, J.; Ren, W.; Niwa, S.; Leadbetter, S.; et al. Patient Navigation for Colonoscopy Completion: Results of an RCT. Am. J. Prev. Med. 2017, 53, 363–372. [Google Scholar] [CrossRef]
- Silvester, J.A.; Kalkat, H.; Graff, L.A.; Walker, J.R.; Singh, H.; Duerksen, D.R. Information seeking and anxiety among colonoscopy-naive adults: Direct-to-colonoscopy vs traditional consult-first pathways. World J. Gastrointest. Endosc. 2016, 8, 701–708. [Google Scholar] [CrossRef]
- Parker, S.; Zipursky, J.; Ma, H.; Baumblatt, G.L.; Siegel, C.A. A Web-based Multimedia Program Before Colonoscopy Increased Knowledge and Decreased Anxiety, Sedation Requirement, and Procedure Time. J. Clin. Gastroenterol. 2018, 52, 519–523. [Google Scholar] [CrossRef]
- Bertels, L.; van der Heijden, S.; Hoogsteyns, M.; Dekker, E.; van Asselt, K.; van Weert, H.; Knottnerus, B. GPs’ perspectives on colorectal cancer screening and their potential influence on FIT-positive patients: An exploratory qualitative study from a Dutch context. BJGP Open 2019, 3, bjgpopen18X101631. [Google Scholar] [CrossRef]
- Correia, A.; Rabeneck, L.; Baxter, N.N.; Paszat, L.F.; Sutradhar, R.; Yun, L.; Tinmouth, J. Lack of follow-up colonoscopy after positive FOBT in an organized colorectal cancer screening program is associated with modifiable health care practices. Prev. Med. 2015, 76, 115–122. [Google Scholar] [CrossRef]
- Mastrokostas, A.; Gavana, M.; Gkrizioti, M.; Smyrnakis, E.; Cholongitas, E.; Benos, A.; Haidich, A.-B. Discrepancies and misconceptions of perceived colorectal cancer screening barriers between primary health professionals and unscreened population. A comparative study in Greece. J. BUON 2018, 23, 67–76. [Google Scholar]

{kind=link}
{kind=link}
| Eligible Population * (% Out of Total) | Email Address ** | Response Rate *** | |
|---|---|---|---|
| Total | 6829 (100%) | 5134 (75.2%) (% out of eligible population) | 1597 (31.1%) (% out of people having an email address) |
| Sex | |||
| Male | 3797 (55.6%) | 2989 (58.2%) | 922 (57.7%) |
| Female | 3032 (44.4%) | 2145 (41.8%) | 675 (42.3%) |
| Age | |||
| 50–54 | 1019 (14.9%) | 872 (17.0%) | 296 (18.5%) |
| 55–59 | 1104 (16.2%) | 920 (17.9%) | 332 (20.8%) |
| 60–64 | 1558 (22.8%) | 1223 (23.8%) | 341 (21.4%) |
| 65–69 | 1258 (18.4%) | 916 (17.8%) | 346 (21.7%) |
| 70+ | 1890 (27.7%) | 1203 (23.4%) | 282 (17.7%) |
| DC Performed (N = 1157) | DC Appointment (N = 82) | No DC (N = 358) | Total (N = 1597) | ||
|---|---|---|---|---|---|
| Q1: Ever had colonoscopy? | no | 716 (61.9%) | 51 (62.2%) | 281 (78.5%) | 1048 (65.6%) |
| yes | 441 (38.1%) | 31 (37.8%) | 77 (21.5%) | 549 (34.4%) | |
| Q2: Anxious due to result letter? | very much | 119 (10.3%) | 7 (8.5%) | 20 (5.6%) | 146 (9.1%) |
| moderately | 480 (41.5%) | 37 (45.1%) | 96 (26.8%) | 613 (38.4%) | |
| rather not–not at all | 558 (48.2%) | 38 (46.3%) | 242 (69.5%) | 838(52.5%) | |
| Q6: Talked with GP about positive result? | no | 239 (20.7%) | 16 (19.5%) | 96 (26.8%) | 351 (22%) |
| yes | 918 (79.3%) | 66 (80.5%) | 262 (73.2%) | 1246 (78.0%) | |
| If contact with GP: who took initiative? | I contacted GP | 709 (77.2%) | 52 (78.8%) | 197 (75.2%) | 958 (76.9%) |
| GP contacted me | 209 (22.8%) | 14 (21.2%) | 65 (24.8%) | 288 (23.1%) | |
| Q7: Estimated risk of having CRC after receiving the positive result? | very low–low | 564 (48.7%) | 35 (42.7%) | 233 (65.1%) | 832 (52.1%) |
| not low, not high | 436 (37.7%) | 36 (43.9%) | 111 (31.0%) | 583 (36.5%) | |
| high–very high | 157 (13.6%) | 12 (13.4%) | 14 (3.9%) | 182 (11.4%) | |
| Q8: Know someone who has had a colo? | no | 226 (19.5%) | 23 (28.0%) | 108 (30.3%) | 357 (22.4%) |
| yes | 931 (80.5%) | 59 (72.0%) | 250 (69.8%) | 1240 (77.6%) | |
| Q9: How did they experience the colo? | not annoying | 276 (27.9%) | 7 (11.5%) | 39 (14.7%) | 322 (24.5%) |
| neutral | 152 (15.4%) | 8 (13.1%) | 29 (11.0%) | 189 (14.4%) | |
| a bit annoying | 346 (35.0%) | 22 (36.1%) | 96 (36.4%) | 464 (35.3%) | |
| very annoying | 110 (11.1%) | 12 (19.7%) | 66 (25.0%) | 188 (14.3%) | |
| some annoying, others not | 66 (6.7%) | 5 (8.2%) | 22 (8.3%) | 93 (7.1%) | |
| I don’t know | 39 (3.9%) | 7 (11.5%) | 12 (7.7%) | 58 (4.4%) | |
| Q10: Have their experiences influenced your decision to have a DC? | no | 823 (88.4%) | 51 (86.4%) | 202 (80.8%) | 1076 (86.8%) |
| yes | 108 (11.6%) | 8 (13.6%) | 48 (19.2%) | 164 (13.2%) | |
| Q11: Anyone advised you to have a DC? | no | 617 (53.3%) | 42 (51.2%) | 222 (62.0%) | 881 (55.2%) |
| yes | 540 (46.7%) | 40 (48.8%) | 136 (38.0%) | 716 (44.8%) | |
| Q12: If yes, who advised you? | my partner | 154 (20.5%) | 5 (10.4%) | 41 (23.8%) | 200 (20.6%) |
| my GP or specialist | 463 (61.6%) | 37 (77.0%) | 86 (50.0%) | 586 (60.3%) | |
| relative or friend | 135 (17.9%) | 6 (12.5%) | 45 (26.2%) | 186 (19.1%) |
| Statements | Absolute Number of Respondents Agreed with the Statement * | |
|---|---|---|
| DC-Performed (N = 1157) | No DC (N = 358) | |
| Advised by others to plan a DC | ||
| My doctor wants me to undergo a colonoscopy after a positive stool test. | 1067 (92.2%) | 199 (55.6%) |
| My loved ones believe it is important that I undergo a colonoscopy after a positive stool test. | 1064 (91.9%) | 198 (55.3%) |
| Perceptions of DC aspects | ||
| I would only undergo a (new) colonoscopy if performed under complete sedation. | 675 (58.4%) | 162 (45.3%) |
| The bowel preparation (e.g., drinking special fluids) was/seems annoying. | 619 (53.5%) | 220 (61.4%) |
| I expected/expect that a colonoscopy is very painful. | 306 (26.5%) | 149 (41.6%) |
| The diet a few days prior to the colonoscopy (e.g., avoiding fibers) was/seems annoying. | 181 (15.7%) | 122 (34.1%) |
| The waiting for the results of the colonoscopy was/seems annoying. | 100 (8.6%) | 114 (31.9%) |
| Having a colonoscopy performed is very painful. | 74 (6.4%) | NA |
| The colonoscopy procedure itself was/seems annoying. | 62 (5.4%) | 206 (57.6%) |
| The side effects of the colonoscopy (e.g., abdominal pain) were/seem annoying. | 59 (5.1%) | 164 (45.8%) |
| The side effects of the sedation were/seem annoying. | 23 (2.0%) | 139 (38.8%) |
| Fear of DC and DC results | ||
| I’m very anxious about having a colonoscopy. | NA | 162 (45.2%) |
| I’m afraid of the possible complications that can occur during a colonoscopy. | NA | 133 (37.1%) |
| I’m afraid of the possible results (lesions found) during the colonoscopy. | NA | 122 (34.1%) |
| I’m afraid of having CRC. | NA | 65 (18.2%) |
| Feelings of shame/taboo | ||
| I felt/would feel embarrassed during colonoscopy. | 37 (3.2%) | 109 (30.4%) |
| Performing a colonoscopy affects my personal integrity. | NA | 78 (21.8%) |
| I refuse a colonoscopy because it is unnatural to have a medical instrument inserted anally. | NA | 64 (17.9%) |
| I wouldn’t let others know if I had a colonoscopy done. | NA | 55 (15.3%) |
| I’m a bit embarrassed to talk about a colonoscopy with others. | NA | 38 (10.6%) |
| Perception of false positive FIT/DC not needed | ||
| I have no complaints and thus believe a colonoscopy is not needed. | NA | 197 (55.1%) |
| I doubt whether the result of the stool test is correct. | NA | 143 (40%) |
| If I had CRC, I would have complaints. | NA | 140 (39.1%) |
| I don’t think it is necessary to undergo a medical examination because I have no complaints. | NA | 134 (37.4%) |
| I’m convinced that I do not have CRC. | NA | 123 (34.4%) |
| I have hemorrhoids and that’s why the stool test was abnormal, so I didn’t do a colonoscopy. | NA | 123 (34.4%) |
| CRC does not occur in my family, which is why I did not have a colonoscopy. | NA | 93 (25.9%) |
| My medication may have influenced the result of the stool test, so I did not do a colonoscopy. | NA | 84 (23.4%) |
| Financial/practical issues | ||
| I have other medical issues that are now a priority. | NA | 106 (29.6%) |
| I have other non-medical issues that are now a priority. | NA | 60 (16.8%) |
| I don’t have anyone who can take me home after the colonoscopy. | NA | 36 (10.0%) |
| I believe the personal amount I need to pay for a colonoscopy is too high. | NA | 25 (7.0%) |
| Questions | N (%) |
|---|---|
| Reasons for having/planning a DC (DC performed and DC appointment, N = 1239) | |
| Advised by others | 700 (56.5%) |
| 571 (46.1%) |
| 129 (10.4%) |
| Importance of explaining the blood in the stool/positive FIT/prevention | 380 (30.6%) |
| Motivated because of medical history/symptoms/familial risk | 98 (7.9%) |
| Others (e.g., anxiety, CRC is a common disease) | 44 (4.9%) |
| Missing | 17 (1.4%) |
| Experiences with DC (DC performed, N = 1157) | |
| Discussed the colonoscopy afterwards with someone (except the doctor)? | |
| 1.094 (96.6%) |
| 63 (5.4%) |
| How did the colonoscopy go? | |
| 499 (43.1%) |
| 163 (14.1%) |
| 460 (39.8%) |
| 11 (1.0%) |
| Future intention (DC performed, N = 1157) | |
| Undergo a colonoscopy again if needed? | |
| 1.147 (99.1%) |
| 10 (0.9%) |
| Questions | N (%) |
|---|---|
| Reasons not to have a DC | |
| 79 (22%) |
| 65 (18.2%) |
| 64 (17.9%) |
| 29 (8.1%) |
| 25 (7.0%) |
| 24 (6.6%) |
| 21 (6%) |
| 21 (5.9%) |
| 30 (8.3%) |
| Decision-making process | |
| Who was most decisive in making the decision not to do a colonoscopy? | |
| 256 (71.5%) |
| 71 (19.8%) |
| 19 (5.3%) |
| 12 (3.4%) |
| Has anyone discouraged you to have a colonoscopy? | |
| 21 (5.9%) |
| 337 (94.1%) |
| Other follow-up examination (instead of colonoscopy) after the FIT+ result | |
| 250 (69.8%) |
| 71 (19.8%) |
| 21 (5.9%) |
| 16 (4.2%) |
| Potential motivations to undergo a DC | |
| Based on self-reported answers (one answer per person) | |
| 75 (21%) |
| 63 (17.5%) |
| 50 (14%) |
| 27 (7.5%) |
| 22 (6%) |
| 21 (6%) |
| 17 (5%) |
| 13 (3.5%) |
| 13 (3.5%) |
| 57 (16%) |
| Based on fixed statements (completely or rather agree with a given statement): ‘I would perform a DC if:…’ | |
| 258 (72.1%) |
| 142 (39.7%) |
| 107 (29.8%) |
| 91 (25.4%) |
| 138 (38.5%) |
| 109 (30.4%) |
| 134 (37.4%) |
| 112 (31.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoeck, S.; Tran, T.N. Insights into Personal Perceptions and Experiences of Colonoscopy after Positive FIT in the Flemish Colorectal Cancer Screening Program. Gastrointest. Disord. 2024, 6, 49-63. https://doi.org/10.3390/gidisord6010004
Hoeck S, Tran TN. Insights into Personal Perceptions and Experiences of Colonoscopy after Positive FIT in the Flemish Colorectal Cancer Screening Program. Gastrointestinal Disorders. 2024; 6(1):49-63. https://doi.org/10.3390/gidisord6010004
Chicago/Turabian StyleHoeck, Sarah, and Thuy Ngan Tran. 2024. "Insights into Personal Perceptions and Experiences of Colonoscopy after Positive FIT in the Flemish Colorectal Cancer Screening Program" Gastrointestinal Disorders 6, no. 1: 49-63. https://doi.org/10.3390/gidisord6010004
APA StyleHoeck, S., & Tran, T. N. (2024). Insights into Personal Perceptions and Experiences of Colonoscopy after Positive FIT in the Flemish Colorectal Cancer Screening Program. Gastrointestinal Disorders, 6(1), 49-63. https://doi.org/10.3390/gidisord6010004