

The Relationship between Sleep, Chronotype, and Dental Caries—A Narrative Review



Abstract
1. Introduction
2. Dental Caries
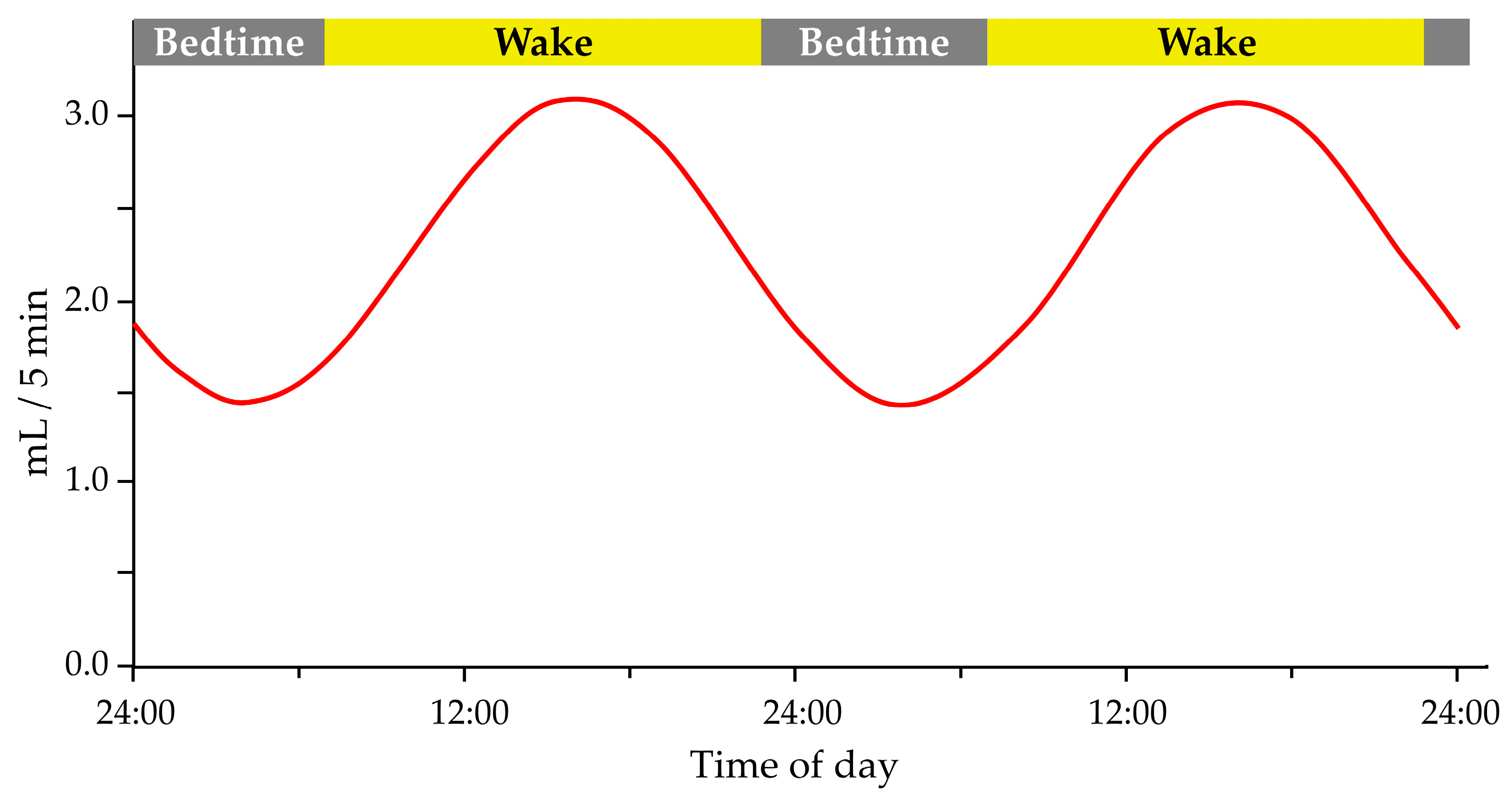
Saliva
3. Sleep Homeostasis
3.1. Insufficient Sleep and Caries
3.2. Sleep Duration and Caries Prevalence

{kind=link}
{kind=link}
| Study | Country | Study Design | Population Description | Sleep Assessment | Study Period | Age Range | Sample Size (Sex) | Primary Outcome |
|---|---|---|---|---|---|---|---|---|
| Watanabe et al., 2014 [69] | Japan | Cohort study | Children participated in routine dental examinations at 1.5 years old at Kobe City Public Health Center in Japan | Parents or guardians reported children’s bedtime (before 9 p.m., between 9 and 11 p.m., after 11 p.m., or irregular) | Between June 2006 and August 2009 and between April 2008 and March 2011 | 1.5 years old at baseline and 3 years at a dental check-up | 31,202 children (16,052 male and 15,150 female) | Late bedtime is a risk factor for the development of dental caries |
| Chen et al., 2018 [50] | Japan | Cohort study | Municipal health check-ups for children aged 0–3 years in Kobe City, Japan | Parents reported their child’s wake time and bedtime on a standardized questionnaire | From 31 March 2004 to 1 April 2014 | 1.5 years old at baseline and 3 at a dental check-up | 71,069 children (36,245 male and 34,824 female) | Late bedtime and short sleep duration are associated with an increased risk of caries |
| Kitsaras et al., 2018 [48] | UK | Cross-sectional study | Participants were recruited through an active study on General Dental Anaesthetic teeth extraction and through General Dental Practices | Interactive text survey for the assessment of bedtime routines | From March to June 2017 | Range from 3 to 5 years old | 50 children (24 male and 26 female) | Children with optimal bedtime routines had fewer cavities and missing teeth than children with suboptimal bedtime routines |
| Zhou et al., 2019 [71] | China | Cross-sectional study | Children from 3 to 5 years old residing in Zhejiang province, living there for more than six months | Structured questionnaire completed by the children’s parents or guardian | From January to June 2016 | Range from 3 to 5 years | 1591 children (821 male and 770 female) | Longer sleeping (≥12 h) is associated with lower caries’ prevalence |
| Asaka et al., 2020 [53] | Japan | Cross-sectional study | Children participated in the Super Shokuiku School Project in Takaoka City, Toyama Prefecture | Parents completed the questionnaires on their child’s sleep duration (short sleep duration was defined as <8 h) | March 2016 | Range from 6 to 12 years | 1699 children (848 male and 851 female) | Short sleep duration is associated with higher dental caries’ prevalence |
| Alqaderi et al., 2020 [9] | Kuwait | Cohort study | Children across the six governorates of Kuwait | Questionnaire-based interviews with parents or guardians on child’s bedtime and sleep duration | In 2012 and a dental check-up in 2014 | 10 years at baseline and 12 years at a check-up | 5456 children (2103 male and 3353 female) | Late bedtime is associated with increased dental caries’ incidence |
| Ogawa et al., 2022 [63] | Japan | Observational cross-sectional study | Children in five kindergartens, nursery schools, and early childhood education and care centers in Chitose, Japan | Parents filled out a questionnaire on their child’s sleeping status | During October 2020 | Range from 3 to 6 years | 332 children (178 male and 154 female) | The negative correlation between sleep durations and the number of caries |
| Topaloglu-Ak et al., 2022 [61] | Turkey | Cross-sectional study | Children referred to the Department of Pediatric Dentistry at the Faculty of Dentistry of Istanbul Aydin University | Children’s Sleep Habits Questionnaire completed by child’s parents | From 2 March 2020 to 29 May 2020 | Range from 6 to 13 years | 100 children (45 male and 55 female) | The presence of caries is associated with awakening from sleep at night and sleep fragmentation |
| Arroyo Buenestado et al., 2023 [76] | Spain | Cross-sectional study | Dental clinic Clínica María Isabel Rodríguez, Pozoblanco, Córdoba | Parents or caregiver filled out a Spanish version of the Paediatric Sleep Questionnaire | From January to March 2021 | Range from 2 to 5 years | 80 children (40 male and 40 female) | Higher caries’ prevalence among later bedtime and later wake-up time |
4. Circadian Rhythm
4.1. Chronotype and Caries’ Prevalence
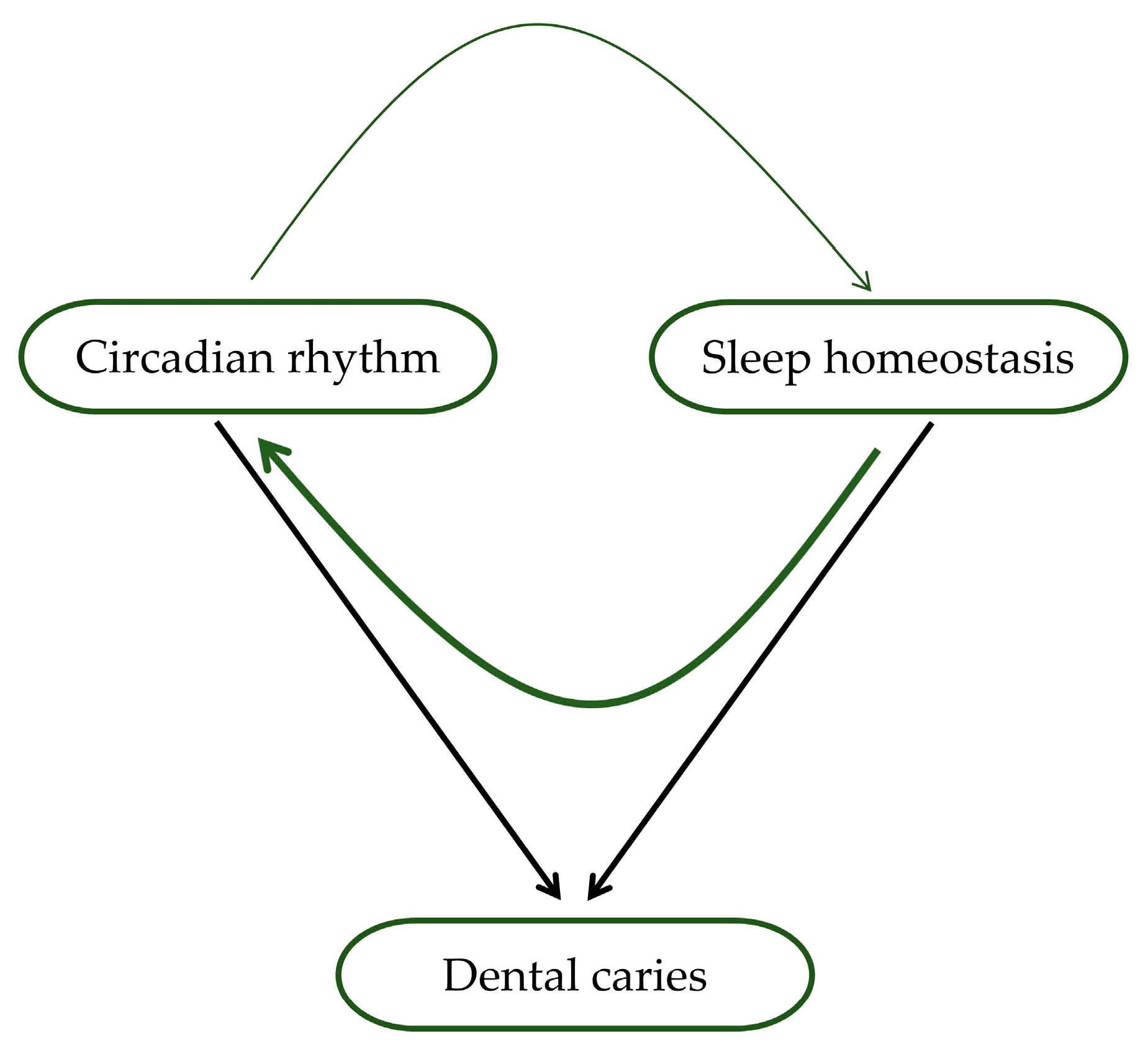
4.2. Importance of Circadian Rhythm and Sleep Homeostasis in Caries’ Development
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Oral Health Status Report: Towards Universal Health Coverage for Oral Health by 2030; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Alhabdan, Y.A.; Albeshr, A.G.; Yenugadhati, N.; Jradi, H. Prevalence of dental caries and associated factors among primary school children: A population-based cross-sectional study in Riyadh, Saudi Arabia. Environ. Health Prev. Med. 2018, 23, 60. [Google Scholar] [CrossRef]
- Kale, S.; Kakodkar, P.; Shetiya, S.; Abdulkader, R. Prevalence of dental caries among children aged 5–15 years from 9 countries in the Eastern Mediterranean Region: A meta-analysis. East. Mediterr. Health J. 2020, 26, 726–735. [Google Scholar] [CrossRef]
- Roberts, W.E.; Mangum, J.E.; Schneider, P.M. Pathophysiology of Demineralization, Part II: Enamel White Spots, Cavitated Caries, and Bone Infection. Curr. Osteoporos. Rep. 2022, 20, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Hernández, P.; Sánchez, M.C.; Llama-Palacios, A.; Ciudad, M.J.; Collado, L. Strategies to Combat Caries by Maintaining the Integrity of Biofilm and Homeostasis during the Rapid Phase of Supragingival Plaque Formation. Antibiotics 2022, 11, 880. [Google Scholar] [CrossRef]
- Aldabal, L.; Bahammam, A. Metabolic, endocrine, and immune consequences of sleep deprivation. Open Respir. Med. J. 2011, 5, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Karaaslan, F.; Dikilitaş, A. The association between stage-grade of periodontitis and sleep quality and oral health-related quality of life. J. Periodontol. 2019, 90, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Prather, A.A.; Hall, M.; Fury, J.M.; Ross, D.C.; Muldoon, M.F.; Cohen, S.; Marsland, A.L. Sleep and antibody response to hepatitis B vaccination. Sleep 2012, 35, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Alqaderi, H.; Tavares, M.; Al-Mulla, F.; Al-Ozairi, E.; Goodson, J.M. Late bedtime and dental caries incidence in Kuwaiti children: A longitudinal multilevel analysis. Community Dent. Oral Epidemiol. 2020, 48, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Grover, V.; Malhotra, R.; Kaur, H. Exploring association between sleep deprivation and chronic periodontitis: A pilot study. J. Indian Soc. Periodontol. 2015, 19, 304–307. [Google Scholar] [CrossRef]
- McEwen, B.S.; Karatsoreos, I.N. Sleep Deprivation and Circadian Disruption Stress, Allostasis, and Allostatic Load. Sleep Med. Clin. 2015, 17, 253–262. [Google Scholar] [CrossRef]
- Castilho, R.L.; Matsumoto, L.H.; Castilho, G.L.; Weber, S.A.T. The interface between dentistry and respiratory sleep disorders in children. Sleep Sci. 2020, 13, 220–223. [Google Scholar]
- Škrlec, I.; Milić, J.; Cilenšek, I.; Petrovič, D.; Wagner, J.; Peterlin, B. Circadian clock genes and myocardial infarction in patients with type 2 diabetes mellitus. Gene 2019, 701, 98–103. [Google Scholar] [CrossRef]
- Farhud, D.; Aryan, Z. Circadian Rhythm, Lifestyle and Health: A Narrative Review. Iran. J. Public Health 2018, 47, 1068. [Google Scholar]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between Clocks: Daily Temporal Patterns of Human Chronotypes. J. Biol. Rhythm. 2003, 18, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Partonen, T. Chronotype and Health Outcomes. Curr. Sleep Med. Rep. 2015, 1, 205–211. [Google Scholar] [CrossRef]
- Kanerva, N.; Kronholm, E.; Partonen, T.; Ovaskainen, M.L.; Kaartinen, N.E.; Konttinen, H.; Broms, U.; Männistö, S. Tendency toward eveningness is associated with unhealthy dietary habits. Chronobiol. Int. 2012, 29, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Nauha, L.; Jurvelin, H.; Ala-Mursula, L.; Niemelä, M.; Jämsä, T.; Kangas, M.; Korpelainen, R. Chronotypes and objectively measured physical activity and sedentary time at midlife. Scand. J. Med. Sci. Sport. 2020, 30, 1930–1938. [Google Scholar] [CrossRef] [PubMed]
- da Silveira, K.S.R.; Prado, I.M.; Abreu, L.G.; Serra-Negra, J.M.C.; Auad, S.M. Association among chronotype, dietary behaviours, and caries experience in Brazilian adolescents: Is there a behavioural pattern? Int. J. Paediatr. Dent. 2018, 28, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Nicoll, A.; Adair, P.; Pine, C. Risk factors for dental caries in young children: A systematic review of the literature. Community Dent. Health 2004, 21, 71–85. [Google Scholar]
- Kirthiga, M.; Murugan, M.; Saikia, A.; Kirubakaran, R. Risk Factors for Early Childhood Caries: A Systematic Review and Meta-Analysis of Case Control and Cohort Studies. Pediatr. Dent. 2020, 41, 95. [Google Scholar]
- Abed, R.; Bernabe, E.; Sabbah, W. Family Impacts of Severe Dental Caries among Children in the United Kingdom. Int. J. Environ. Res. Public Health 2020, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Sugars and Dental Caries. Available online: https://www.who.int/news-room/fact-sheets/detail/sugars-and-dental-caries (accessed on 22 August 2022).
- Inchingolo, A.D.; Malcangi, G.; Semjonova, A.; Inchingolo, A.M.; Patano, A.; Coloccia, G.; Ceci, S.; Marinelli, G.; Di Pede, C.; Ciocia, A.M.; et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children 2022, 9, 1014. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.S.; Chu, C.H.; Yu, O.Y. Oral Microbiome and Dental Caries Development. Dent. J. 2022, 10, 184. [Google Scholar] [CrossRef] [PubMed]
- Sardana, D.; Galland, B.; Wheeler, B.J.; Yiu, C.K.Y.; Ekambaram, M. Effect of sleep on development of early childhood caries: A systematic review. Eur. Arch. Paediatr. Dent. 2023, 24, 1–14. [Google Scholar] [CrossRef]
- Arvidsson, L.; Birkhed, D.; Hunsberger, M.; Lanfer, A.; Lissner, L.; Mehlig, K.; Mårild, S.; Eiben, G. BMI, eating habits and sleep in relation to salivary counts of mutans streptococci in children—The IDEFICS Sweden study. Public Health Nutr. 2016, 19, 1088–1092. [Google Scholar] [CrossRef]
- Aas, J.A.; Griffen, A.L.; Dardis, S.R.; Lee, A.M.; Olsen, I.; Dewhirst, F.E.; Leys, E.J.; Paster, B.J. Bacteria of Dental Caries in Primary and Permanent Teeth in Children and Young Adults. J. Clin. Microbiol. 2008, 46, 1407. [Google Scholar] [CrossRef]
- Rathee, M.; Sapra, A. Dental Caries; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Corcoran, B.M.; Stanton, C.; Fitzgerald, G.F.; Ross, R.P. Survival of Probiotic Lactobacilli in Acidic Environments Is Enhanced in the Presence of Metabolizable Sugars. Appl. Environ. Microbiol. 2005, 71, 3060. [Google Scholar] [CrossRef] [PubMed]
- Larsen, T.; Fiehn, N.E. Dental biofilm infections—An update. APMIS 2017, 125, 376–384. [Google Scholar] [CrossRef]
- Tennert, C.; Reinmuth, A.C.; Bremer, K.; Al-Ahmad, A.; Karygianni, L.; Hellwig, E.; Vach, K.; Ratka-Krüger, P.; Wittmer, A.; Woelber, J.P. An oral health optimized diet reduces the load of potential cariogenic and periodontal bacterial species in the supragingival oral plaque: A randomized controlled pilot study. Microbiologyopen 2020, 9, e1056. [Google Scholar] [CrossRef]
- Pitts, N.B.; Twetman, S.; Fisher, J.; Marsh, P.D. Understanding dental caries as a non-communicable disease. Br. Dent. J. 2021, 231, 749. [Google Scholar] [CrossRef]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- Sambunjak, D.; Nickerson, J.W.; Pericic, T.P.; Johnson, T.M.; Imai, P.; Tugwell, P.; Worthington, H.V. Flossing for the management of periodontal diseases and dental caries in adults. Cochrane Database Syst. Rev. 2019, 2019, CD008829. [Google Scholar] [CrossRef]
- Pratyusha, N.; Vinay, C.; Uloopi, K.S.; Rojaramya, K.S.; Ahalya, P.; Devi, C. Association of serum Vitamin D and salivary calcium and phosphorus levels in 3-11-year-old schoolchildren with dental caries. J. Indian Soc. Pedod. Prev. Dent. 2021, 39, 240–245. [Google Scholar]
- Cassolato, S.F.; Turnbull, R.S. Xerostomia: Clinical aspects and treatment. Gerodontology 2003, 20, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Kanduti, D.; Sterbenk, P.; Artnik, B. Fluoride: A review of use and effects on health. Mater. Socio-Med. 2016, 28, 133. [Google Scholar] [CrossRef] [PubMed]
- Çolak, H.; Dülgergil, Ç.; Dalli, M.; Hamidi, M. Early childhood caries update: A review of causes, diagnoses, and treatments. J. Nat. Sci. Biol. Med. 2013, 4, 29. [Google Scholar] [CrossRef] [PubMed]
- Gati, D.; Vieira, A.R. Elderly at greater risk for root caries: A look at the multifactorial risks with emphasis on genetics susceptibility. Int. J. Dent. 2011, 2011, 647168. [Google Scholar] [CrossRef] [PubMed]
- Cogulu, D.; Saglam, C. Genetic aspects of dental caries. Front. Dent. Med. 2022, 3, 1060177. [Google Scholar] [CrossRef]
- Sabbarwal, B.; Puranik, M.P.; Uma, S.R. Association between Parental Behavior and Child’s Oral Health among 3–5-year-old Children in Bengaluru City. Int. J. Clin. Pediatr. Dent. 2020, 13, 677. [Google Scholar] [CrossRef]
- Moriyama, C.M.; Velasco, S.R.M.; Butini, L.; Abanto, J.; Antunes, J.L.F.; Bönecker, M. How oral health literacy and parental behavior during the meals relate to dental caries in children. Braz. Oral Res. 2022, 36, e131. [Google Scholar] [CrossRef]
- Goto, Y.; Wada, K.; Konishi, K.; Uji, T.; Koda, S.; Mizuta, F.; Yamakawa, M.; Watanabe, K.; Ando, K.; Ueyama, J.; et al. Association between exposure to household smoking and dental caries in preschool children: A cross-sectional study. Environ. Health Prev. Med. 2019, 24, 9. [Google Scholar] [CrossRef] [PubMed]
- Akinkugbe, A.A.; Brickhouse, T.H.; Nascimento, M.M.; Slade, G.D. Prenatal smoking and the risk of early childhood caries: A prospective cohort study. Prev. Med. Rep. 2020, 20, 101201. [Google Scholar] [CrossRef]
- Lam, P.P.Y.; Chua, H.; Ekambaram, M.; Lo, E.C.M.; Yiu, C.K.Y. Does Early Childhood Caries Increase Caries Development among School Children and Adolescents? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 13459. [Google Scholar] [CrossRef]
- Moradi, G.; Bolbanabad, A.M.; Moinafshar, A.; Adabi, H.; Sharafi, M.; Zareie, B. Evaluation of Oral Health Status Based on the Decayed, Missing and Filled Teeth (DMFT) Index. Iran. J. Public Health 2019, 48, 2050. [Google Scholar] [CrossRef]
- Kitsaras, G.; Goodwin, M.; Allan, J.; Kelly, M.P.; Pretty, I.A. Bedtime routines child wellbeing & development. BMC Public Health 2018, 18, 386. [Google Scholar] [CrossRef]
- Radić, M.; Benjak, T.; Vukres, V.D.; Rotim, Ž.; Zore, I.F. Presentation of DMFT/dmft Index in Croatia and Europe. Acta Stomatol. Croat. 2015, 49, 275. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Tanaka, S.; Arai, K.; Yoshida, S.; Kawakami, K. Insufficient Sleep and Incidence of Dental Caries in Deciduous Teeth among Children in Japan: A Population-Based Cohort Study. J. Pediatr. 2018, 198, 279–286.e5. [Google Scholar] [CrossRef]
- Feng, G.; Zhao, J.; Peng, J.; Luo, B.; Zhang, J.; Chen, L.; Xu, Z. Circadian clock—A promising scientific target in oral science. Front. Physiol. 2022, 13, 2388. [Google Scholar] [CrossRef] [PubMed]
- González-González, J.M. Circadian rhythms and dental caries. Int. J. Curr. Res. 2018, 10, 71616–71618. [Google Scholar]
- Asaka, Y.; Sekine, M.; Yamada, M.; Tatsuse, T.; Sano, M. Association of short sleep duration and long media use with caries in school children. Pediatr. Int. 2020, 62, 214–220. [Google Scholar] [CrossRef]
- Roestamadji, R.I.; Nastiti, N.I.; Surboyo, M.D.C.; Irmawati, A. The Risk of Night Shift Workers to the Glucose Blood Levels, Saliva, and Dental Caries. Eur. J. Dent. 2019, 13, 323. [Google Scholar] [CrossRef] [PubMed]
- Dawes, C. Circadian rhythms in human salivary flow rate and composition. J. Physiol. 1972, 220, 529. [Google Scholar] [CrossRef]
- Zheng, L.; Seon, Y.J.; McHugh, J.; Papagerakis, S.; Papagerakis, P. Clock Genes Show Circadian Rhythms in Salivary Glands. J. Dent. Res. 2012, 91, 783. [Google Scholar] [CrossRef]
- Nishide, S.; Yoshihara, T.; Hongou, H.; Kanehira, T.; Yawaka, Y. Daily life habits associated with eveningness lead to a higher prevalence of dental caries in children. J. Dent. Sci. 2019, 14, 302–308. [Google Scholar] [CrossRef]
- Wada, M.; Orihara, K.; Kamagata, M.; Hama, K.; Sasaki, H.; Haraguchi, A.; Miyakawa, H.; Nakao, A.; Shibata, S. Circadian clock-dependent increase in salivary IgA secretion modulated by sympathetic receptor activation in mice. Sci. Rep. 2017, 7, 8802. [Google Scholar] [CrossRef] [PubMed]
- Buzalaf, M.A.R.; Hannas, A.R.; Kato, M.T. Saliva and dental erosion. J. Appl. Oral Sci. 2012, 20, 493. [Google Scholar] [CrossRef]
- Archer, S.N.; Oster, H. How sleep and wakefulness influence circadian rhythmicity: Effects of insufficient and mistimed sleep on the animal and human transcriptome. J. Sleep Res. 2015, 24, 476–493. [Google Scholar] [CrossRef]
- Topaloglu-Ak, A.; Kurtulmus, H.; Basa, S.; Sabuncuoglu, O. Can sleeping habits be associated with sleep bruxism, temporomandibular disorders and dental caries among children? Dent. Med. Probl. 2022, 59, 517–522. [Google Scholar] [CrossRef]
- Lam, L.T.; Lam, M.K. Sleep Disorders in Early Childhood and the Development of Mental Health Problems in Adolescents: A Systematic Review of Longitudinal and Prospective Studies. Int. J. Environ. Res. Public Health 2021, 18, 11782. [Google Scholar] [CrossRef]
- Ogawa, M.; Ogi, H.; Nakamura, D.; Nakamura, T.; Izawa, K.P. Association between Insufficient Sleep and Dental Caries among Preschoolers in Japan: A Cross-Sectional Multicentre Study. Eur. J. Investig. Health Psychol. Educ. 2021, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Moro, J.; Santos, P.; Giacomin, A.; Cardoso, M.; Bolan, M. Association between trouble sleeping and oral conditions among schoolchildren. Rev. Paul. Pediatr. 2021, 39, e2019342. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.S.; Jeon, H.S.; Mun, S.J. Association between sleep habits and symptoms of oral disease in adolescents: The 2017 Korea Youth Risk Behavior Web-based Survey. BMC Oral Health 2021, 21, 233. [Google Scholar] [CrossRef] [PubMed]
- Papagerakis, S.; Zheng, L.; Schnell, S.; Sartor, M.A.; Somers, E.; Marder, W.; McAlpin, B.; Kim, D.; McHugh, J.; Papagerakis, P. The circadian clock in oral health and diseases. J. Dent. Res. 2014, 93, 27–35. [Google Scholar] [CrossRef]
- Adeola, H.A.; Papagerakis, S.; Papagerakis, P. Systems biology approaches and precision oral health: A circadian clock perspective. Front. Physiol. 2019, 10, 399. [Google Scholar] [CrossRef]
- Schroeder, K.; Gurenlian, J.R. Recognizing Poor Sleep Quality Factors During Oral Health Evaluations. Clin. Med. Res. 2019, 17, 20. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Wang, D.H.; Ijichi, A.; Shirai, C.; Zou, Y.; Kubo, M.; Takemoto, K.; Masatomi, C.; Ogino, K. The Influence of Lifestyle on the Incidence of Dental Caries among 3-Year-Old Japanese Children. Int. J. Environ. Res. Public Health 2014, 11, 12611–12622. [Google Scholar] [CrossRef]
- Potter, G.D.M.; Skene, D.J.; Arendt, J.; Cade, J.E.; Grant, P.J.; Hardie, L.J. Circadian Rhythm and Sleep Disruption: Causes, Metabolic Consequences, and Countermeasures. Endocr. Rev. 2016, 37, 584. [Google Scholar] [CrossRef]
- Zhou, N.; Zhu, H.; Chen, Y.; Jiang, W.; Lin, X.; Tu, Y.; Chen, D.; Chen, H. Dental caries and associated factors in 3 to 5-year-old children in Zhejiang Province, China: An epidemiological survey. BMC Oral Health 2019, 19, 9. [Google Scholar] [CrossRef]
- Tenelanda-López, D.; Valdivia-Moral, P.; Castro-Sánchez, M. Eating Habits and Their Relationship to Oral Health. Nutrients 2020, 12, 2619. [Google Scholar] [CrossRef]
- Kubala, E.; Strzelecka, P.; Grzegocka, M.; Lietz-Kijak, D.; Gronwald, H.; Skomro, P.; Kijak, E. A Review of Selected Studies That Determine the Physical and Chemical Properties of Saliva in the Field of Dental Treatment. BioMed Res. Int. 2018, 2018, 6572381. [Google Scholar] [CrossRef]
- Sotozono, M.; Kuriki, N.; Asahi, Y.; Noiri, Y.; Hayashi, M.; Motooka, D.; Nakamura, S.; Yamaguchi, M.; Iida, T.; Ebisu, S. Impact of sleep on the microbiome of oral biofilms. PLoS ONE 2021, 16, e0259850. [Google Scholar] [CrossRef]
- Nakai, Y.; Mori-Suzuki, Y. Impact of Dietary Patterns on Plaque Acidogenicity and Dental Caries in Early Childhood: A Retrospective Analysis in Japan. Int. J. Environ. Res. Public Health 2022, 19, 7245. [Google Scholar] [CrossRef] [PubMed]
- Arroyo Buenestado, A.; Ribas-Pérez, D. Early Childhood Caries and Sleep Disorders. J. Clin. Med. 2023, 12, 1378. [Google Scholar] [CrossRef] [PubMed]
- Martinez, D.; Sfreddo Lenz, M. Circadian rhythm sleep disorders. Indian J. Med. Res. 2010, 131, 141–149. [Google Scholar]
- Škrlec, I.; Talapko, J.; Džijan, S.; Cesar, V.; Lazić, N.; Lepeduš, H. The Association between Circadian Clock Gene Polymorphisms and Metabolic Syndrome: A Systematic Review and Meta-Analysis. Biology 2022, 11, 20. [Google Scholar] [CrossRef]
- Škrlec, I.; Milic, J.; Heffer, M.; Peterlin, B.; Wagner, J. Genetic variations in circadian rhythm genes and susceptibility for myocardial infarction. Genet. Mol. Biol. 2018, 41, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Škrlec, I. The Influence of Dental Implants on the Circadian Clock and the Role of Melatonin in the Oral Cavity. Explor. Res. Hypothesis Med. 2022. [Google Scholar] [CrossRef]
- De Sousa Né, Y.G.; Lima, W.F.; Mendes, P.F.S.; Baia-da-Silva, D.C.; Bittencourt, L.O.; Nascimento, P.C.; de Souza-Rodrigues, R.D.; Paranhos, L.R.; Martins-Júnior, P.A.; Lima, R.R. Dental Caries and Salivary Oxidative Stress: Global Scientific Research Landscape. Antioxidants 2023, 12, 330. [Google Scholar] [CrossRef] [PubMed]
- Uchida, H.; Ovitt, C.E. Novel impacts of saliva with regard to oral health. J. Prosthet. Dent. 2022, 127, 383. [Google Scholar] [CrossRef]
- Roenneberg, T.; Kuehnle, T.; Juda, M.; Kantermann, T.; Allebrandt, K.; Gordijn, M.; Merrow, M. Epidemiology of the human circadian clock. Sleep Med. Rev. 2007, 11, 429–438. [Google Scholar] [CrossRef]
- Škrlec, I.; Milić, J.; Heffer, M.; Wagner, J.; Peterlin, B. Circadian clock genes and circadian phenotypes in patients with myocardial infarction. Adv. Med. Sci. 2019, 64, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Lang, C.; Richardson, C.; Micic, G.; Gradisar, M. Understanding Sleep-Wake Behavior in Late Chronotype Adolescents: The Role of Circadian Phase, Sleep Timing, and Sleep Propensity. Front. Psychiatry 2022, 13, 785079. [Google Scholar] [CrossRef]
- Lin, S.Y.; Chung, K.K.H. Chronotype and trait self-control as unique predictors of sleep quality in Chinese adults: The mediating effects of sleep hygiene habits and bedtime media use. PLoS ONE 2022, 17, e0266874. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Huang, J.; Yang, M. Association between Chronotype and Sleep Quality among Chinese College Students: The Role of Bedtime Procrastination and Sleep Hygiene Awareness. Int. J. Environ. Res. Public Health 2022, 20, 197. [Google Scholar] [CrossRef]
- Kurnaz, S.; Kandeger, A. Do chronotype differences and night eating syndrome affect dental health? Int. J. Dent. Hyg. 2020, 18, 378–383. [Google Scholar] [CrossRef]
- Lundgren, A.M.; Öhrn, K.; Jönsson, B. Do adolescents who are night owls have a higher risk of dental caries?—A case-control study. Int. J. Dent. Hyg. 2016, 14, 220–225. [Google Scholar] [CrossRef]
- Lucassen, E.A.; Zhao, X.; Rother, K.I.; Mattingly, M.S.; Courville, A.B.; de Jonge, L.; Csako, G.; Cizza, G. Evening chronotype is associated with changes in eating behavior, more sleep apnea, and increased stress hormones in short sleeping obese individuals. PLoS ONE 2013, 8, e56519. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, J.D.; Smith, B.M.; Spresser, C.; Harkins, P.; Zolton, L.; Williams, K. The relationship of night eating to oral health and obesity in community dental clinic patients. Gen. Dent. 2010, 58, e134–e139. [Google Scholar]
- Janjić, K.; Agis, H. Chronodentistry: The role & potential of molecular clocks in oral medicine. BMC Oral Health 2019, 19, 32. [Google Scholar] [CrossRef]
- Folayan, M.O.; El Tantawi, M.; Oginni, O.; Arowolo, O. Is chronotype profile a risk indicator for caries in children and adolescents in sub-urban Nigeria? Int. J. Paediatr. Dent. 2021, 31, 627–633. [Google Scholar] [CrossRef]
- Roenneberg, T.; Foster, R.G.; Klerman, E.B. The circadian system, sleep, and the health/disease balance: A conceptual review. J. Sleep Res. 2022, 31, e13621. [Google Scholar] [CrossRef] [PubMed]
- Deboer, T. Sleep homeostasis and the circadian clock: Do the circadian pacemaker and the sleep homeostat influence each other’s functioning? Neurobiol. Sleep Circadian Rhythm. 2018, 5, 68. [Google Scholar] [CrossRef] [PubMed]


| Sociodemographic Factors | Dietary Factors | Oral Hygiene |
|---|---|---|
| Low socioeconomic status | Daily sweet snacks | <2 daily brushings |
| Parental smoking | High sugar foods | Lack of fluoride toothpaste |
| Long screen time | Daily sweet drinks | |
| Gender (male) | Frequently snaking | |
| Nighttime eating | ||
| Breakfast skipping | ||
| Vitamin D deficiency | ||
| Low levels of calcium |
| Insufficient Sleep | Sleep Duration | Sleep Disorders |
|---|---|---|
| Irregular bedtime routines | Less than 8 h | Insomnia |
| Late bedtime (after 11 p.m.) | Longer than 10 h | Sleep-related breathing disorders |
| Sleep fragmentation | Sleep–wake circadian rhythm disorders |
| Study | Country | Study Design | Population Description | Chronotype Measurement | Study Period | Age Range | Sample Size Sex | Primary Outcome |
|---|---|---|---|---|---|---|---|---|
| Lundgren et al., 2016 [89] | Sweden | A comparative cross-sectional, case–control study | Patients at the Public Dental Service in Uppsala County Council examined during 2004 and 2005 | The instrument developed by Östberg in 1973 and modified by Torvall and Akerstedt in 1980 | 2006 | Adolescents aged 15 to 16 years | 196 adolescents (101 male and 95 female) | The evening type had a higher risk of caries than the morning type |
| da Silveira et al., 2018 [19] | Brazil | Cross-sectional study | Adolescents aged 12 years of all public and private schools in the municipality of Brumadinho, in the state of Minas Gerais participated in the study | Brazilian Portuguese version of the Puberty and Phase Preference Scale (PPPS) | Between August and December 2016 | Adolescents aged 12 years | 245 adolescents (109 male and 136 female) | Chronotype was not associated with DMFT scores |
| Nishide et al., 2019 [57] | Japan | Cross-sectional study | Outpatients age range 1 to 16 in the university hospital in Japan at the Division of Dentistry for Children and Disabled Persons | Self-reported sleep–wake time | - | Children aged 1 to 16 years (7.2 ± 3.5 years) | 140 children (77 male and 63 female) | Evening type has a higher prevalence of dental caries |
| Kurnaz et al., 2020 [89] | Turkey | Cross-sectional study | Patients applied at the dental clinic of the Faculty of Dentistry of Kutahya Health Sciences University | Morningness–Eveningness Questionnaire (MEQ) | Between March and September 2018 | Patients aged 18 to 63 years (36.02 ± 8.91 years) | 210 patients (100 male and 110 female) | Chronotype was not associated with DMFT scores |
| Folayan et al., 2021 [93] | Nigeria | Cross-sectional study secondary analysis | Adolescents attending private and public primary and secondary schools in Ife Central Local Government Area, Ile-Ife, Osun State, Nigeria | Horne–Östberg Morningness–Eveningness Questionnaire (MEQ) | 2019 | Adolescents aged 6 to 16 years | 1001 children (452 male and 549 female) | Chronotype was not associated with caries’ prevalence |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kurtović, A.; Talapko, J.; Bekić, S.; Škrlec, I. The Relationship between Sleep, Chronotype, and Dental Caries—A Narrative Review. Clocks & Sleep 2023, 5, 295-312. https://doi.org/10.3390/clockssleep5020023
Kurtović A, Talapko J, Bekić S, Škrlec I. The Relationship between Sleep, Chronotype, and Dental Caries—A Narrative Review. Clocks & Sleep. 2023; 5(2):295-312. https://doi.org/10.3390/clockssleep5020023
Chicago/Turabian StyleKurtović, Anamaria, Jasminka Talapko, Sanja Bekić, and Ivana Škrlec. 2023. "The Relationship between Sleep, Chronotype, and Dental Caries—A Narrative Review" Clocks & Sleep 5, no. 2: 295-312. https://doi.org/10.3390/clockssleep5020023
APA StyleKurtović, A., Talapko, J., Bekić, S., & Škrlec, I. (2023). The Relationship between Sleep, Chronotype, and Dental Caries—A Narrative Review. Clocks & Sleep, 5(2), 295-312. https://doi.org/10.3390/clockssleep5020023