Abstract
Background: The objective of this study was to compare the facial pattern according to Steiner’s cephalometric analysis with other facial measurement methods (Ricketts, Björk-Jarabak, and McNamara). Methods: 200 patients from a university orthodontic clinic were studied. Measurements were taken using Ricketts, Steiner, Björk-Jarabak, and McNamara methods. Results were compared using standard deviation proportions. Results: Significant differences were found between Steiner’s method and the gold standard. No differences were observed between mixed and permanent dentition groups. Errors were noted in facial type classification: 54.8% in the brachyfacial group, 80% in the mesofacial group and 14.5% in the dolichofacial group. Conclusion: The mandibular angle of Steiner tends to make a diagnosis more towards the dolichofacial type compared to other methods. A protocol is proposed to adjust the value of the mandibular angle of Steiner to the other three methods in a Spanish population.
1. Introduction
A good diagnosis of the facial biotype is crucial since, when planning a treatment plan, it will help us to diagnose not only verticality but also sagittal problems. In addition, it influences the choice of orthodontic mechanics and to establish the prognosis of the case. However, these mechanics can generate different responses when applied to patients with similar malocclusions, but with different growth patterns [1]. Cephalometry is a very useful technique in dentistry and especially in orthodontics, since it allows measurements of the cranium to be obtained from X-rays that are then captured on acetate to establish the most significant anatomical points, measure distances and relate the different craniofacial structures according to different criteria and then compare them with normal patterns [2,3,4]. Cephalometry allows us to have an understanding of the morphology, physiology and craniofacial pathology and permits us to individualize a therapeutic procedure [5,6]. According to Ricketts, “cephalometry helps us characterize the dentofacial anomaly, compare some problems with others to differentiate them, classify the findings detected in the study and communicate the data found with other colleagues” [7]. Many authors, Robert Murray Ricketts, Jarabak or McNamara, published their own cephalometric studies, such as Cecil C. Steiner in his article “Cephalometrics for you and for me” [8,9,10,11,12,13]. These cephalometrics differ in the layout and anatomical points selected. However, they share the same diagnostic fields. Thus, in practice, the orthodontist can rely on various cephalometric studies to make his or her own diagnosis. However, the diagnosis can be more complicated, if a study cephalometric interpretation differs from each other. In that case, one could ask: Which cephalometric study is the most reliable for the orthodontist? There are few studies in the scientific literature that relate the same diagnostic fields among different authors, such as facial biotype. The objective of this study was to analyze the facial pattern based on Steiner’s cephalometric analysis, comparing it with the other measures of facial pattern from the Ricketts, Björk-Jarabak and McNamara cephalometric study.
2. Materials and Methods
2.1. Study Type and Design
A cross-sectional observational study was conducted using four cephalometric tracings published by world-renowned authors.
2.2. Study Population
Two hundred (200) patients treated by the orthodontic master’s degree at the Rey Juan Carlos University in Alcorcón (Madrid), were randomly selected without exclusion criteria applied in terms of race, sex, or age.
2.3. Ethical Considerations
The study protocol was reviewed and approved by the Ethics Committee of Rey Juan Carlos University, with internal number (1506202216422). The objective of the study was explained to the participants and the confidentiality of the information collected was ensured. All patients who agreed to participate in the study signed an informed consent form.
2.4. Instruments and Measures
The X-rays and the measurements of the angles were carried out by the same operator, using a computer-assisted technique, following methods validated in the literature for obtaining lateral teleradiographs [14,15,16,17].
- -
- The patient was positioned in a cephalostat with the focal point-sensor, focal point- subject and sensor-subject distance fixed.
- -
- Patient in a standing position, with the back straight, in a stable position, relaxed and without moving, looking towards the horizon at eye level.
- -
- Teeth in occlusion with lips at rest.
- -
- The Frankfort plane of the patient: horizontal and parallel to the floor.
- -
- The external auditory canals aligned at the same height.
The following variables were used:
- -
- The SN-GoGn angle of Steiner’s cephalometry.
- -
- Ricketts’ Facial Axis angle, the angle formed by the basocranial plane (Basion—Nasion) with the facial axis plane (Pterygoid—Gnation).
- -
- Jarabak modified Björk cephalometric facial height ratio value (relationship between posterior facial height and anterior facial height).
- -
- McNamara’s vertical dimension measure. This last variable allowed the sample to be divided into mixed dentition, male permanent dentition, and female permanent dentition.
2.5. Analysis of Data
A statistical analysis was performed using SPSS v28 (SPSS Inc., Chicago, IL, USA). The data analysis included descriptive statistics and the Kolmogorov–Smirnov test to evaluate the assumption of normality, which was confirmed. The values of each cephalometry were converted into fractions of standard deviation (SD) to enable comparison between them. The classifications were mesofacial (SD = 1 to −1), dolichofacial (SD > 1), and brachyfacial (SD < −1). Using the mean SD of McNamara, Ricketts, and Björk-Jarabak, a “gold standard” (GS) group was created. A repeated means test was performed with the SD of Steiner and the SD of the other authors, repeating the same test for dentition (mixed/permanent). In addition, a repeated measures ANOVA was performed to assess whether the error was similar in mixed and permanent dentition. To compare Steiner’s cephalometric biotype with that of the other authors (individually), a McNemar test was performed. Finally, to relate Steiner SD with the Gold Standard (SD), a linear regression was performed using the mean standard deviations of Steiner as the dependent variable and the mean standard deviations of the three other authors as the independent variable. The significance was set at p < 0.01.
3. Results
3.1. Descriptive Analysis of the Sample
The sample is made up of 41% children/young (mixed dentition), 29% male “adults” (permanent dentition) and 30% female “adults” (permanent dentition). We found 47% of the brachyfacial biotype, 22% mesofacial and 31% dolichofacial according to our “Gold Standard” group.
3.2. Comparison of Facial Pattern Diagnostics for Steiner Versus Gold Standard
Significant differences were found between Steiner SD (0.81 ± 3.06) and Gold Standard SD (−0.43 ± 4.35) (t = 5.71, p < 0.01). If we compare with each of the authors we find significant differences results. Jarabak SD (−1.32 ± 2.71, p < 0.01), Ricketts SD (0.38 ± 1.34, p < 0.05) and McNamara SD (−0.53 ± 10.35, p < 0.05). In all cases Steiner is more prone to a dolichofacial pattern than the rest.
3.3. Error According to the Type of Dentition
In the mixed dentition group (N = 82), significant differences were found in the facial pattern for Steiner (0.56 ± 3.13) and SD Gold Standard (−0.69 ± 3.11), (p < 0.001). For the permanent dentition group (N = 118), significant differences were found in the facial pattern for SD Steiner (0.91 ± 2.98) and SD Gold Standard (−0.35 ± 5.01), (p < 0.01). No difference in error was found between the mixed and permanent dentition groups (p = 0.992). See Figure 1.
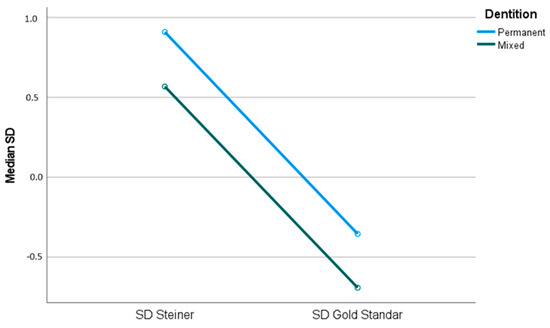
Figure 1.
Comparison SD Steiner-SD Gold Standard in permanent and mixed dentition.
3.4. Error According to Facial Biotype
Analyzing the results differentiating the three patterns (mesofacial, brachyfacial, dolichofacial), the level of coincidence (between Steiner and Gold Standard) for brachyfacial is 45.2%, for dolichofacial it is 85.5%, and for mesofacial it is 20%. The error in the brachyfacial group is 54.8%, the error in the mesofacial group is 80% and the error in the dolichofacial group is 14.5% (Table 1).

Table 1.
Cross table of facial patterns in Steiner with the other authors mentioned.
3.5. Differences between Steiner Values and Each of the Three Authors
In the McNemar’s test table, significant differences were found between Steiner/Jarabak, Steiner/Ricketts and Steiner/McNamara (p < 0.001) (Table 2).
Table 2.
Comparison of the frequency of cases classified as mesofacial, dolichofacial and brachyfacial according to Steiner and the other authors.
3.6. Relationship between the Steiner Values and the Mean of the Three Other Authors
The three other authors were found to predict 65% of the Steiner standard deviation (R2 =0.69, R2 adjusted= 0.48, F (1198) = 186.54, p < 0.001). With a regression slope of Y = −0.18 + 0.23X (Figure 2).
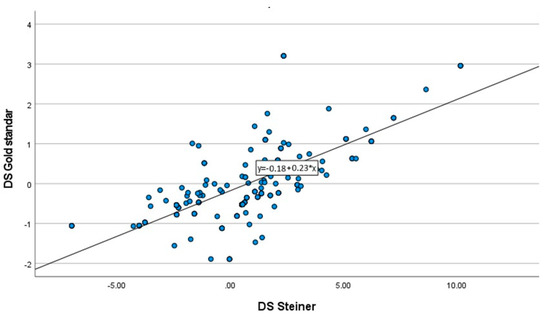
Figure 2.
Dispersion diagram of the mean of the standard deviation of the three authors (Value “gold standard”) by Steiner’s (Steiner value).
4. Discussion
In the present study it is shown that Steiner’s mean values (standard deviation) tend more towards a dolichofacial pattern compared to the rest of the authors. It could be explained by the possible biases of the article “Cephalometrics for you and me” by Steiner [8]. The skill of the operator at the time of taking radiographs is important, to avert errors on the part of the orthodontist when identifying the anatomical structures, as well as when measuring the angles and measurements could be crucial [18,19]. In addition, in 1953, the date of publication of the article, the radiographs did not have the same quality as today’s. Steiner also recognized in his article that offsets in the overlaps of paired anatomical structures such as the condyles or the angle of the mandible could be sources of error. Finally, it must be remembered that Steiner published his study based on a small sample of 50 normal occlusions selected in a beauty contest in a mostly restricted geographical area (North America). It is known that, throughout history, and according to the parts of the world, the criteria of beauty have changed and evolved. The current trend is convex and protrusive profiles that give the individual a more youthful appearance [20,21,22]. In this study, three cephalometries widely used in the world of orthodontics were taken as “gold standard” values of the pattern. It is considered that taking the average of these three cephalometrics, an accuracy pattern was obtained that could then be compared with the pattern given in the Steiner cephalometrics. It cannot be said that there is a world standard for the mesofacial pattern. Different populations have different “normality” parameters. Depending on their geographical location, an author would adapt their cephalometric study calibrated to the normality of their population, such as Björk, who published his study based on a Swedish sample [23], therefore the characteristics of the population influence the measurement norm. In addition, with globalization, there are variations in the same populations. For example, the Colombian population tends to have a “long face” when the ancestry is Mestizo. However, there is a higher percentage of “short face” in Colombians of indigenous descent [24].
Next, categorizing the sample into permanent/mixed dentition, it was found that Steiner’s mean values for mixed dentition as well as permanent dentition are more likely to give a dolichofacial pattern than those of other authors. Therefore, the type of dentition does not seem to have a decisive influence.
Likewise, when the rest of the authors diagnose a mesofacial, it is when Steiner makes the most errors (80%) in his diagnosis, that can be explained by the low proportion of mesofacial in the sample. Because patients were randomly selected, it was not possible to create a group with mesofacial patients. The range of a mesofacial is between −1 and 1 standard deviation. The range of a brachyfacial is between −1 and −∞, and that of a dolichofacial between 1 and ∞. Thus, the difference in size of the standard deviation fraction ranges between mesofacial and dolichofacial/brachyfacial contributes to increasing population bias. When a patient is truly dolichofacial, Steiner has a 14.5% error rate. When it is brachyfacial, Steiner is 54.8% erroneous. Also, Steiner has a high percentage of error in patients with a mesofacial pattern (80%). This high percentage of error in mesofacial is explained in part by the population bias described above. The proportion of dolichofacial in Steiner is higher (46.5%) than in the group of other authors (27.5%) in the sample. Consequently, in a given population, Steiner diagnoses more hyperdivergent patients than the three other authors.
Steiner was found to differ significantly from Jarabak and Ricketts. This observation is confirmed by the research work of Sciaraffia Rubio, et al., which found a strongly negative Pearson correlation coefficient between the Steiner SN-GoGn Angle and the Björk-Jarabak ratio (−0.96) [25]. We might ask ourselves if the choice of the three “gold standard” cephalometrics was the most correct or, on the contrary, others could have been selected. This divergence could, in the future, be investigated to help orthodontists choose the cephalometric measurements that could be more accurate in terms of their population while making a diagnosis.
It was found as the regression slope: Y= −0.18 + 0.23 × X, with X, the standard deviation of Steiner and Y, the mean of the standard deviations of the three other authors. This equation allows the standard deviation given by Steiner’s cephalometry to be corrected according to the three authors, adjusting it to a value more in line with the other authors in this sample.
4.1. Limitations of the Study and Avenues for Future Research
The value of the mandibular angle norm of the Steiner cephalometry could not be modified due to the different standard deviations. Mathematically, it is difficult to relate angles with standard deviations that are not equal. Therefore, it was decided to count and calculate within standard deviations. A protocol was found to uniquely modify the value of the Steiner jaw angle, but the length of the protocol requires mathematical skills not easily performed in an office environment.
Furthermore, the sample is small (N = 200) with representative subjects limited to Alcorcón, making it applicable to that geographical area. It would be necessary to regionalize the representation of the population at the European level using a larger sample to increase the validity of the formula. As said before, it is known that the sample of subjects with the mesofacial biotype is low. A mesofacial group could be considered during subject selectionto ensure more statistical support. By changing the method of selecting the subjects and selecting them by type of facial pattern, it would be possible to equalize the ratio between the three biotypes. However, this method would bring sample selection bias into the study.
In this study, Steiner’s cephalometrics were analyzed in detail and compared with the mean of three other cephalometrics published by world-renowned authors. It would be necessary to expand the number of cephalometrics in the “Gold standard” group to find a more significant “real pattern” value. In addition, other cephalometries could be analyzed using this method.
4.2. Practical Implications
The results given by Steiner for the facial pattern according to the SN-Go-Gn angle do not differ from the “gold standard” group of the three other authors. However, when it does occur, the patient very often falls out of the growth pattern distribution group, resulting in a high probability that the facial biotype diagnosed by the orthodontist, based solely on the Steiner study will be erroneous. Rather than proposing a protocol for adjusting the Steiner facial pattern in a Spanish population, this research demonstrates the limits of cephalometry in diagnosis. For this reason, it is important to rely on the cephalometric interpretation without forgetting the different means of diagnosis that are offered to the orthodontist. A cephalometric analysis, whether by Steiner or by other authors, is indicative. The orthodontist must manage the anthropology of the population of his or her patients, taking into account the variations of the norm that may exist in the different analyzes. However, the proposed adjustments to Steiner’s angle highlighted in this study are preliminary, and further validation is needed before these adjustments can be considered for widespread adoption. It is recommended that each practitioner of the science of orthodontics is advised to rely on and consult several cephalometrics while making their diagnosis.
5. Conclusions
The norm of the mandibular angle described by Downs and used in the study by Steiner swings statistically more towards the dolichofacial side than the mean of the other three cephalometries.
Regardless of whether it is permanent or mixed dentition, the values in Steiner tend more to give a dolichofacial pattern than the average of the three other authors.
Steiner’s facial biotype diagnosis differs considerably from the rest when the three other authors give mesofacial (80% error) and brachifacial (54.8% error). However, only 14.5% error is found when diagnosing a dolichofacial patient.
Steiner standard deviation values differ significantly with Björk-Jarabak, Ricketts and McNamara.
A protocol is proposed to be able to adjust the value of Steiner’s mandibular angle to the three other authors in a Spanish population.
Author Contributions
Conceptualization, T.M. and M.J.G.-O.; methodology, M.J.G.-O.; software, M.J.G.-O.; validation, T.M., M.M.-L. and M.R.; formal analysis, M.J.G.-O.; investigation, T.M.; resources, M.M.-L.; data curation, M.J.G.-O.; writing—original draft preparation, M.M.-L.; writing—review and editing, T.M.; visualization, C.N.-M.; supervision, M.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee of Rey Juan Carlos University protocol code 1506202216422 and date of approval 15/06/2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
To David Blackburn for his support in translation and linguistic interpretation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Girardot, R.A., Jr. Comparison of Condylar Position in Hyperdivergent and Hypodivergent Facial Skeletal Types. Angle Orthod. 2001, 71, 240–246. [Google Scholar]
- Broadbent, B.A.; New X-Ray Technique, I. A new X-ray technique and its application to orthodontia. Angle Orthod. 1931, 1, 45–60. [Google Scholar]
- Bergman, R.T. Cephalometric Soft Tissue Facial Analysis. Am. J. Orthod. Dentofacial Orthop. 1999, 116, 373–389. [Google Scholar] [CrossRef]
- Power, G.; Breckon, J.; Sherriff, M.; McDonald, F. Dolphin Imaging Software: An Analysis of the Accuracy of Cephalometric Digitization and Orthognathic Prediction. Int. J. Oral. Maxillofac. Surg. 2005, 34, 619–626. [Google Scholar] [CrossRef]
- Nielsen, I.L. Cephalometric Morphological Analysis: What Information Does It Give You? Int. Orthod. 2011, 9, 316–324. [Google Scholar] [CrossRef]
- Barahona, C.; Benavides, S.J. Principales Análisis Cefalométricos Utilizados Para El Diagnóstico Ortodóntico. Rev. Científica Odontológica 2006, 2, 11–27. [Google Scholar]
- Gregoret, J.; Tuber, E.; Escobar, L.H.; Matos Da Fonseca, A. Interpretación de la cefalometría lateral. In Orthodontics and Orthognathic Surgery: Diagnosis and Planning, 2nd ed.; Amolca: Amlwch, UK, 2015. [Google Scholar]
- Steiner, C.C. Cephalometrics for You and Me. Am. J. Orthod. 1953, 39, 729–755. [Google Scholar] [CrossRef]
- Ricketts, R.M. Cephalometric Analysis and Synthesis. Angle Orthod. 1961, 31, 141–156. [Google Scholar]
- Gregoret, J.; Tuber, E.; Escobar, L.H. Matos Da Fonseca, A. Biotipo facial. In Orthodontics and Orthognathic Surgery: Diagnosis and Planning, 2nd ed.; Amolca: Amlwch, UK, 2015. [Google Scholar]
- Solow, B.; Houston, W.J. Mandibular Rotations: Concepts and Terminology. Eur. J. Orthod. 1988, 10, 177–179. [Google Scholar] [CrossRef]
- Björk, A.; Skieller, V. Normal and Abnormal Growth of the Mandible. A Synthesis of Longitudinal Cephalometric Implant Studies over a Period of 25 Years. Eur. J. Orthod. 1983, 5, 1–46. [Google Scholar] [CrossRef]
- McNamara, J.A., Jr. A Method of Cephalometric Evaluation. Am. J. Orthod. 1984, 86, 449–469. [Google Scholar] [CrossRef]
- Baldini, B.; Cavagnetto, D.; Baselli, G.; Sforza, C.; Tartaglia, G.M. Cephalometric measurements performed on CBCT and reconstructed lateral cephalograms : A cross-sectional study providing a quantitative approach of differences and bias. BMC Oral. Health 2022, 22, 98. [Google Scholar] [CrossRef]
- Gupta, A. On imaging modalities for cephalometric analysis: A review. Multimed. Tools Appl. 2023, 82, 36837–36858. [Google Scholar] [CrossRef]
- Helal, N.M.; Basri, O.A. Significance of Cephalometric Radiograph in Orthodontic Treatment Plan Decision. J. Of. Contemp. Dent. Pract. 2019, 20, 789–793. [Google Scholar] [CrossRef]
- La Rosa, S.; Leonardi, R.; Ronsivalle, V.; Cicciù, M.; Lo Giudice, A. Radiographic and diagnostic approaches for mandibular asymmetries in orthodontic practice : A narrative review. J. Of. Clin. Pediatr. Dent. 2024, 48, 1. [Google Scholar]
- Bajaj, K.; Rathee, P.; Jain, P.; Panwar, V.R. Comparison of the Reliability of Anatomic Landmarks Based on PA Cephalometric Radiographs and 3D CT Scans in Patients with Facial Asymmetry. Int. J. Clin. Pediatr. Dent. 2011, 4, 213–223. [Google Scholar]
- Lee, W.-J.; Kim, D.-M.; Lee, U.-Y.; Cho, J.-H.; Kim, M.-S.; Hong, J.-H.; Hwang, Y.-I. A Preliminary Study of the Reliability of Anatomical Facial Landmarks Used in Facial Comparison. J. Forensic Sci. 2019, 64, 519–527. [Google Scholar] [CrossRef]
- Gandia Franco, J.L. CapÌtulo 6. Estética en Ortodoncia. In El Manual de Odontología; Masson Salvat Odontología: Barcelona, Spain, 1995; pp. 1258–1261. [Google Scholar]
- Kashmar, M.; Alsufyani, M.A.; Ghalamkarpour, F.; Chalouhi, M.; Alomer, G.; Ghannam, S.; El Minawi, H.; Saedi, B.; Hunter, N.; Alkobaisi, A.; et al. Consensus Opinions on Facial Beauty and Implications for Aesthetic Treatment in Middle Eastern Women. Plast. Reconstr. Surg. 2019, 7, e2220. [Google Scholar] [CrossRef]
- Sands, N.B.; Adamson, P.A. Global Facial Beauty: Approaching a Unified Aesthetic Ideal. Facial Plast. Surg. 2014, 30, 93–100. [Google Scholar] [CrossRef]
- Björk, A. Prediction of Mandibular Growth Rotation. Am. J. Orthod. 1969, 55, 585–599. [Google Scholar] [CrossRef]
- Bedoya, A.; Osorio, J.C.; Tamayo, J.A. Biotipo Morfológico Facial En Tres Grupos Étnicos Colombianos: Una Nueva Clasificación Por Medio Del Índice Facial. Rev. Int. De Morfol. 2012, 30, 677–682. [Google Scholar] [CrossRef][Green Version]
- Sciaraffia Rubio, C.V.; Peralta, B.C.; Rivera Rothgaenger, M.; Schulz, R. Correlación Entre Área Del Rectángulo de Ricketts y El Biotipo Facial Definido Por Björk-Jarabak, Steiner y Ricketts En Individuos Eugnásicos. Chilenos. Thesis, Universidad de Chile, Santiago de Chile, Chile, 2016. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).