
Design and Evaluation of the Internal Space Layout of High-Speed Health Trains Based on Improved Systematic Layout Planning


Abstract
:1. Introduction
2. Theoretical Foundation and Methods
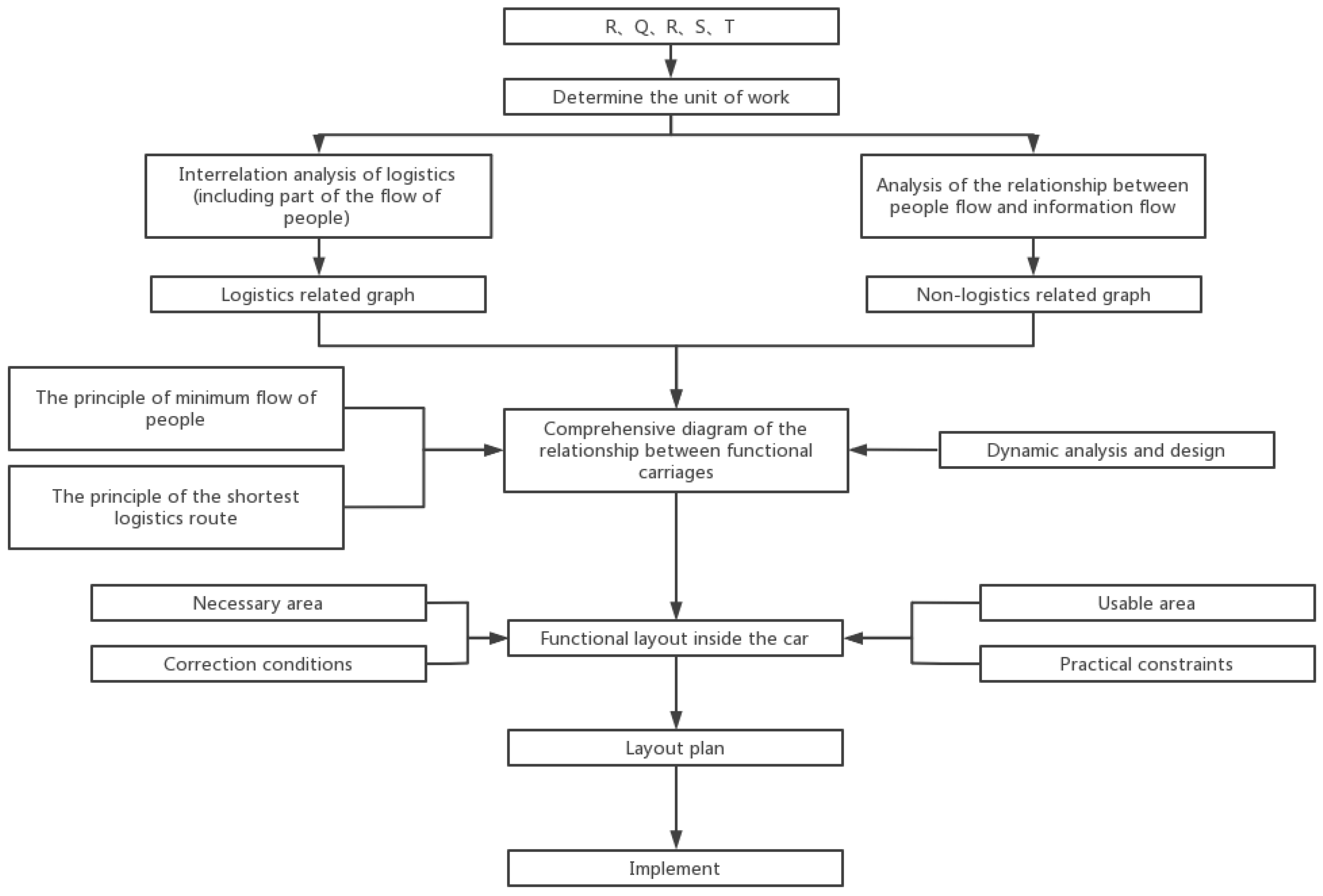
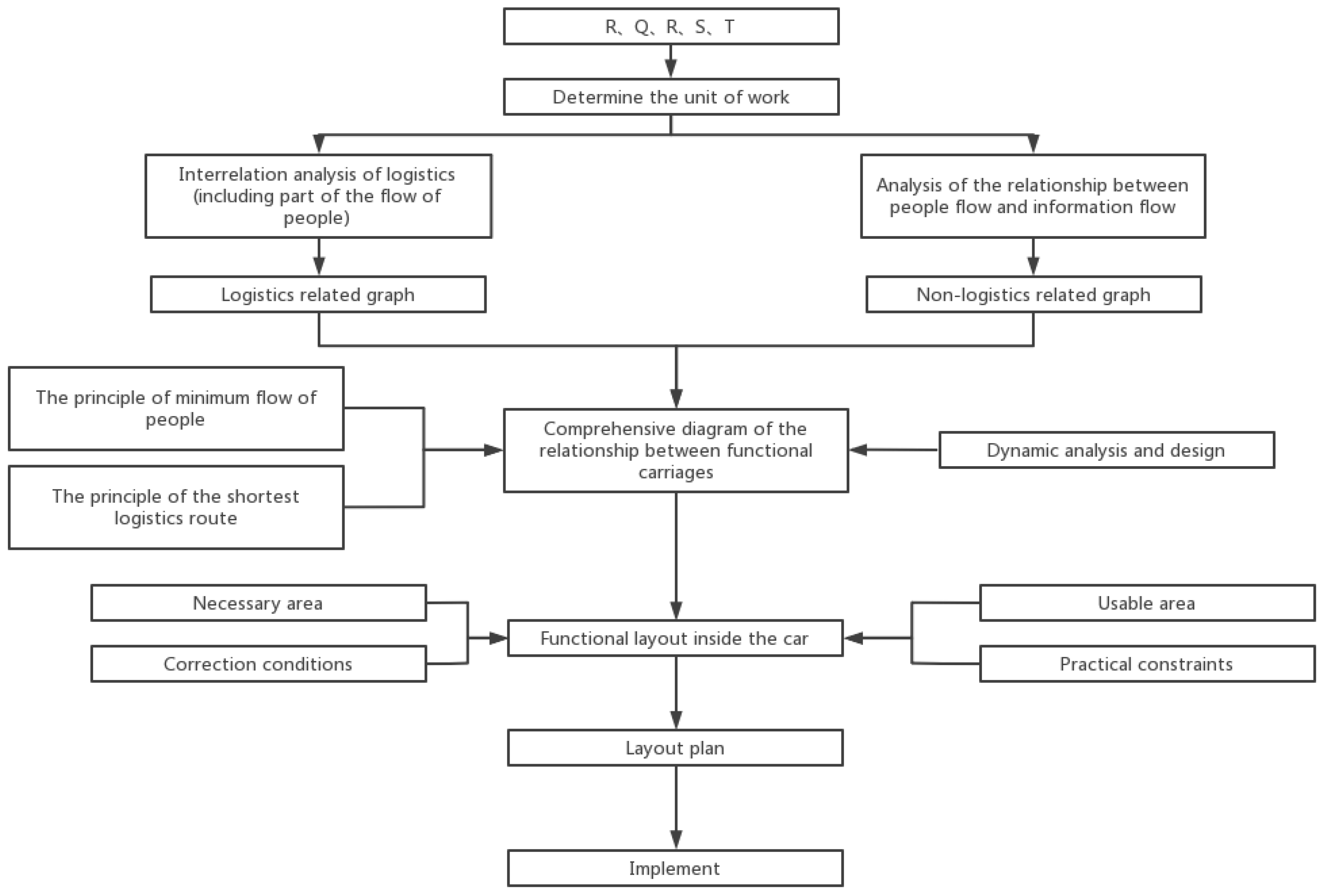
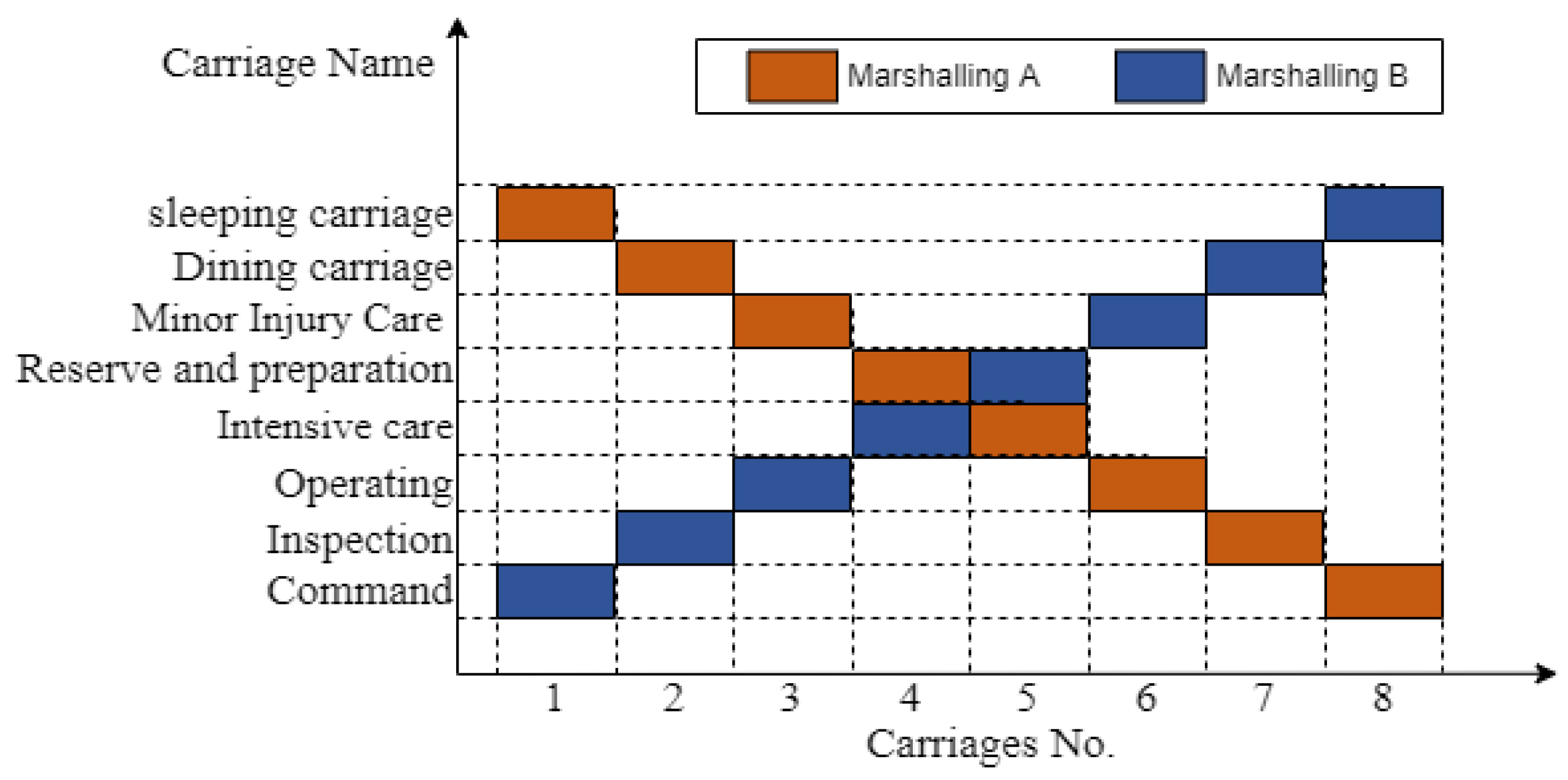
2.1. SLP Improvement and Carriage Marshaling
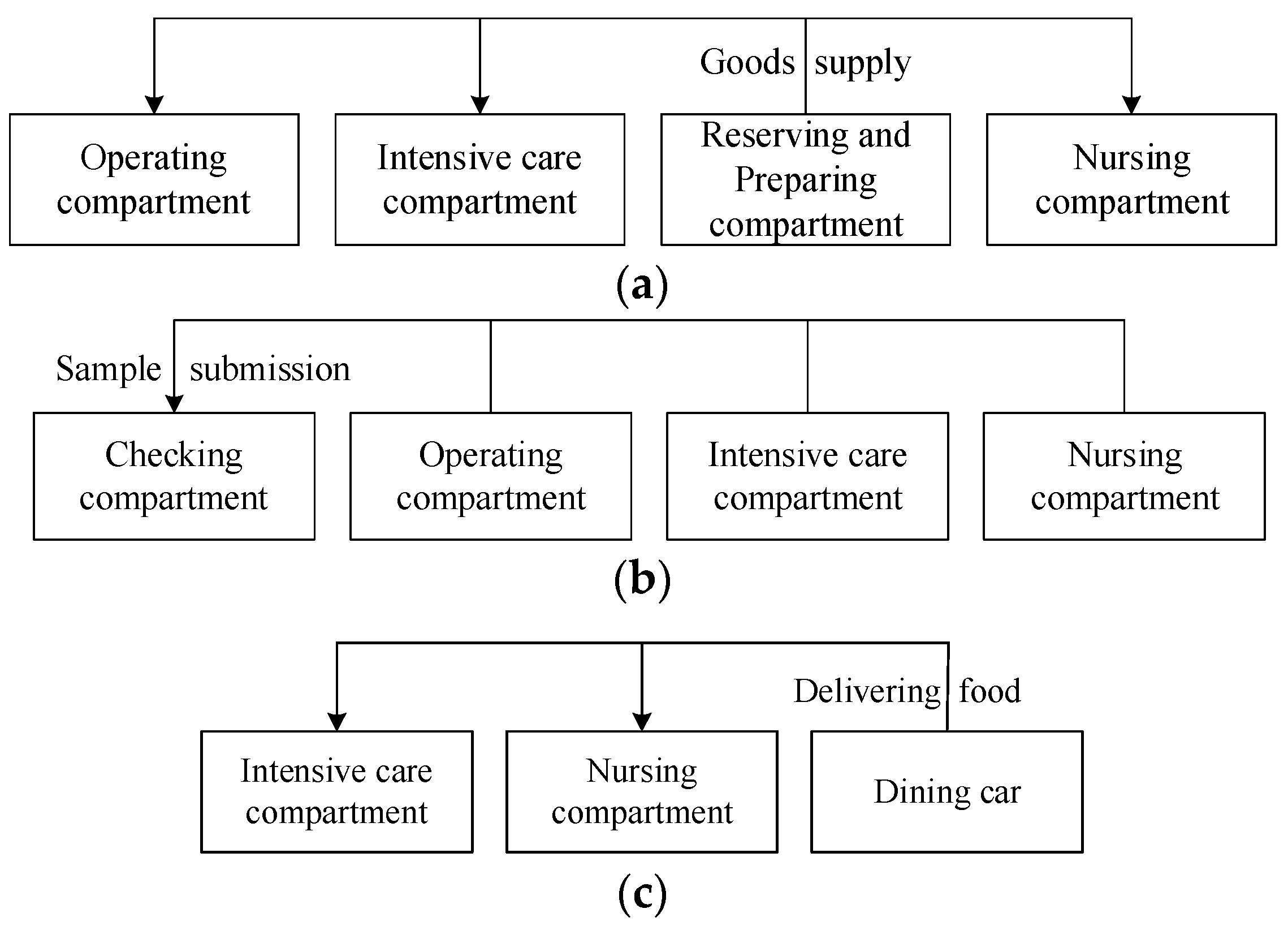
2.2. Analysis of the Relationship between Logistics and Non-Logistics
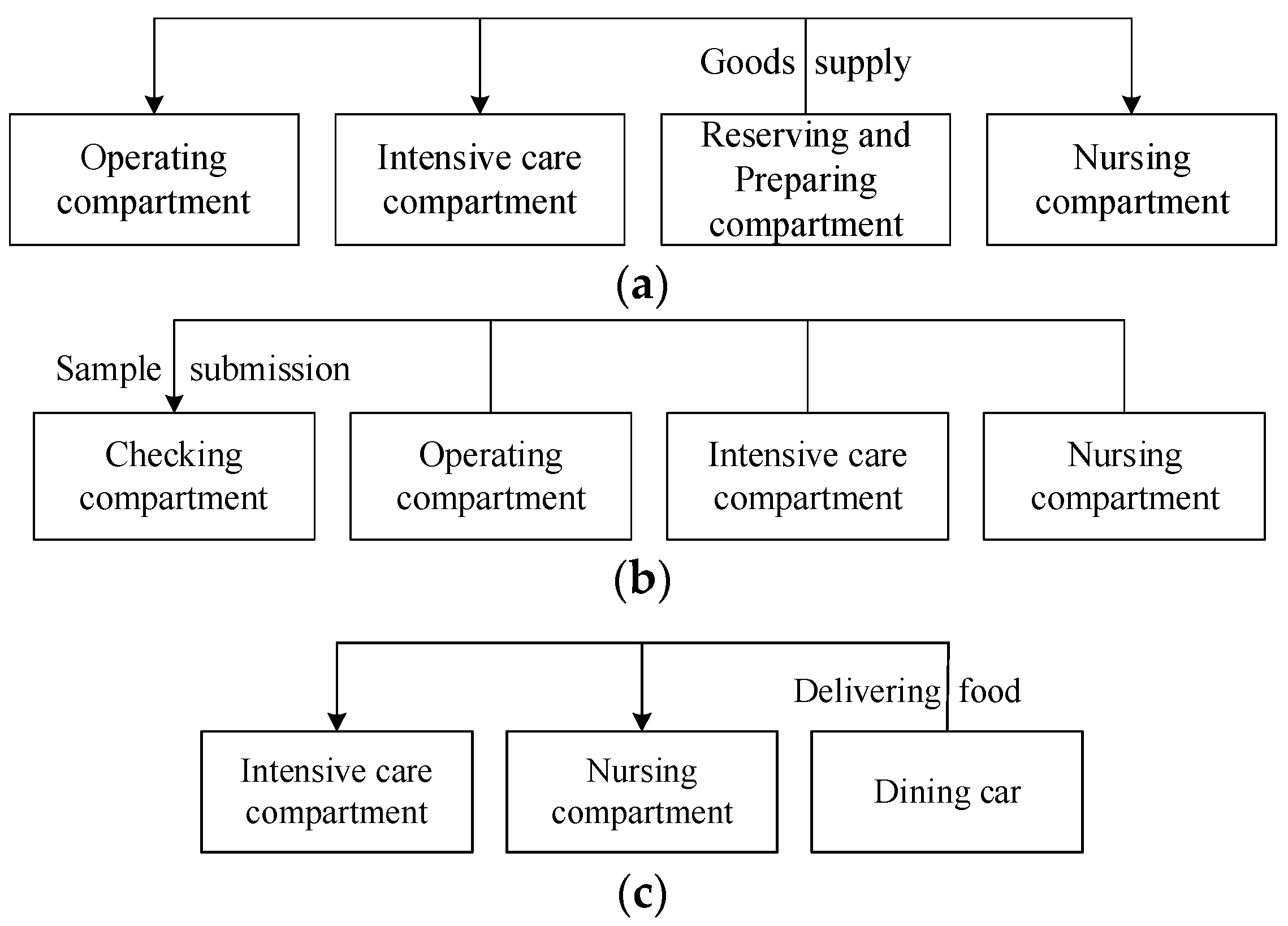
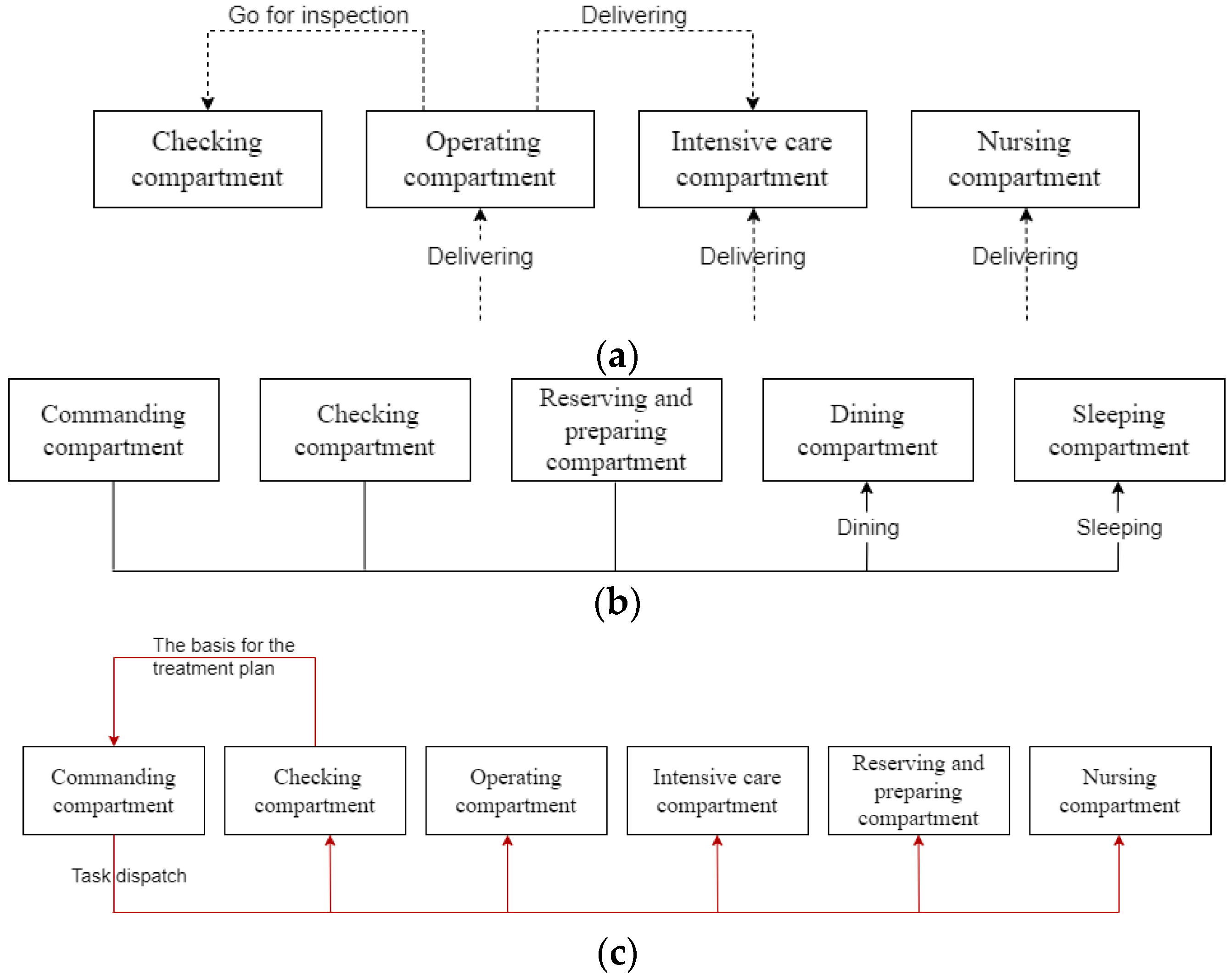
2.2.1. Logistics Relationship Analysis
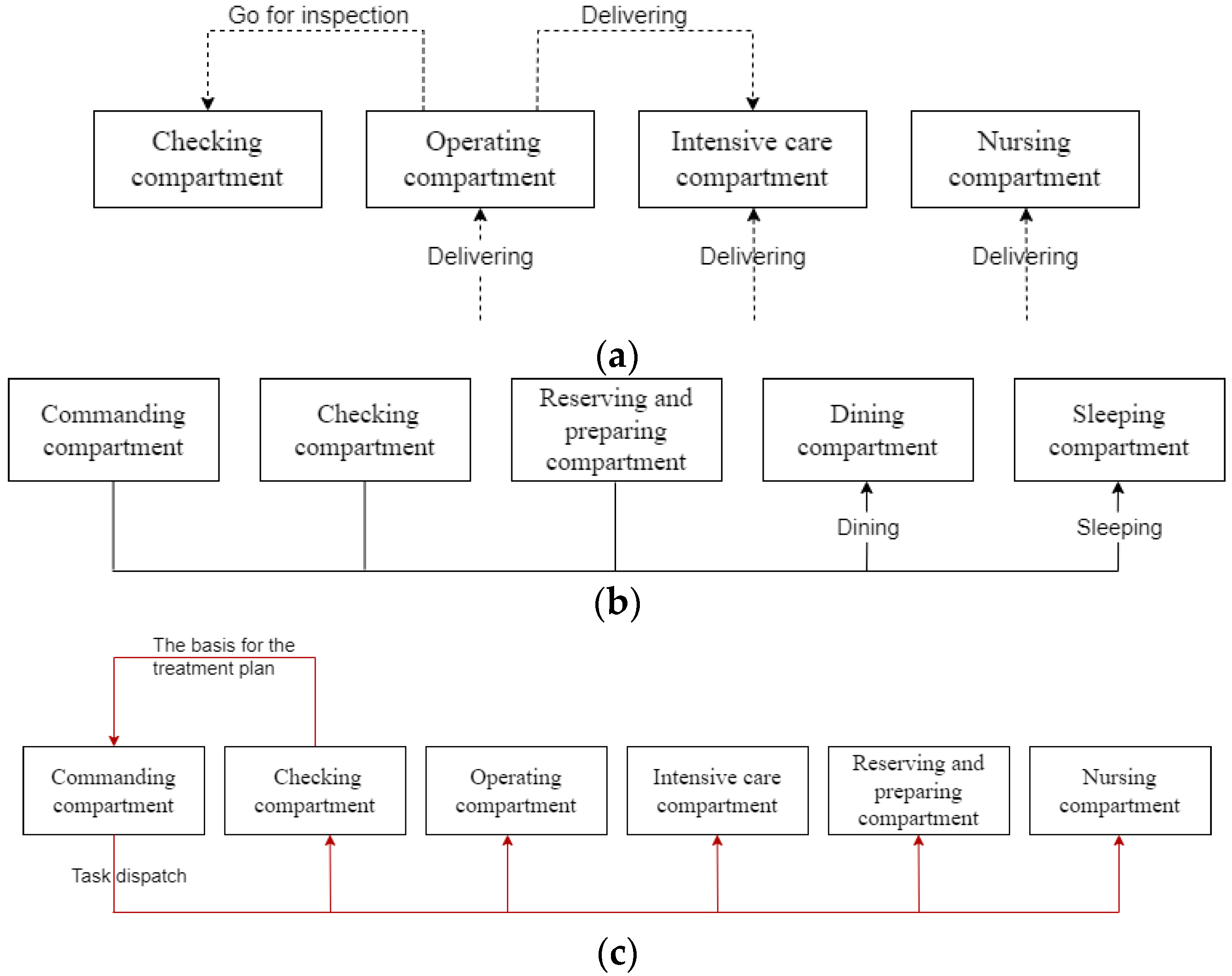
2.2.2. Non-Logistics-Related Graphs
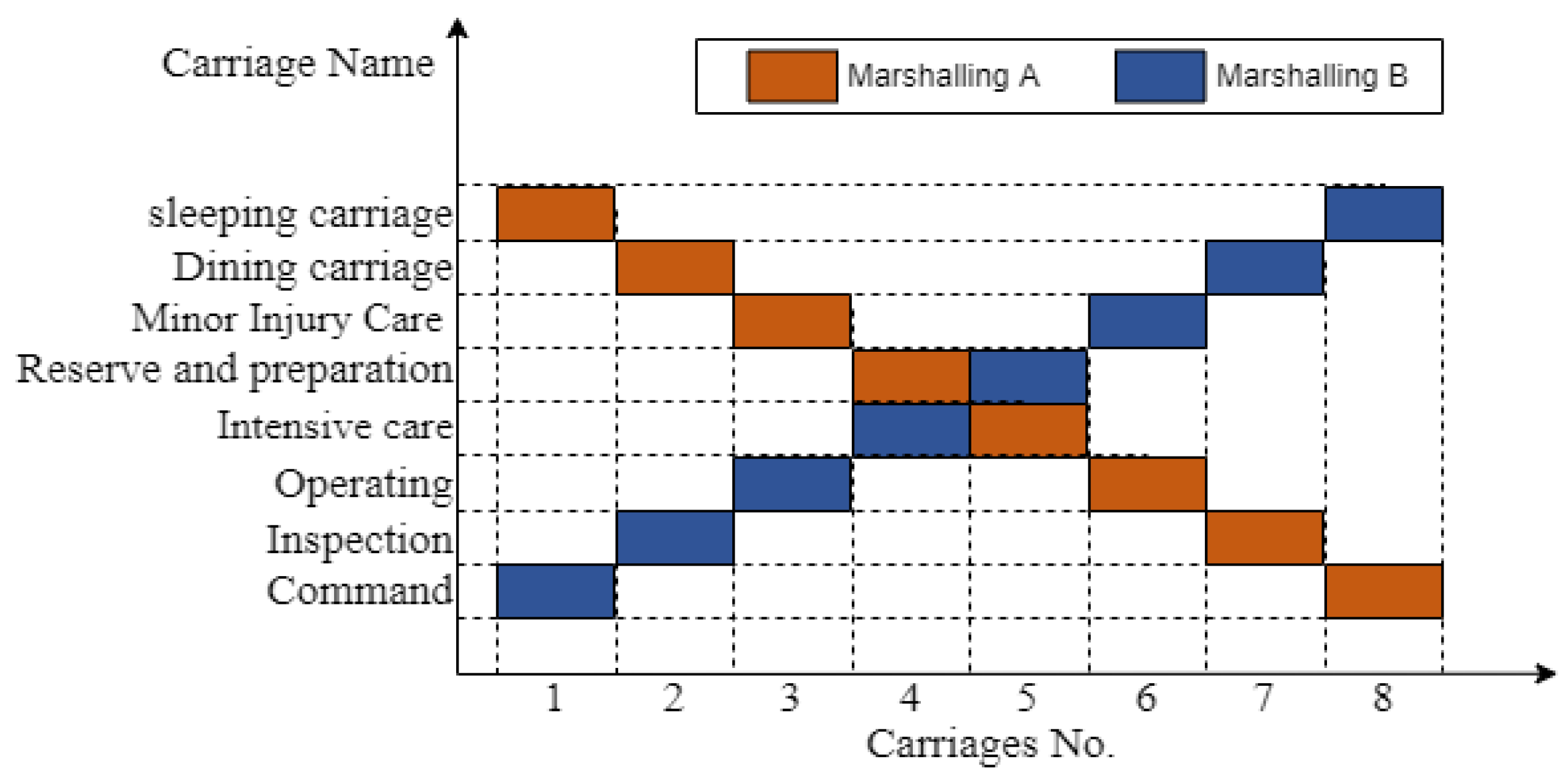
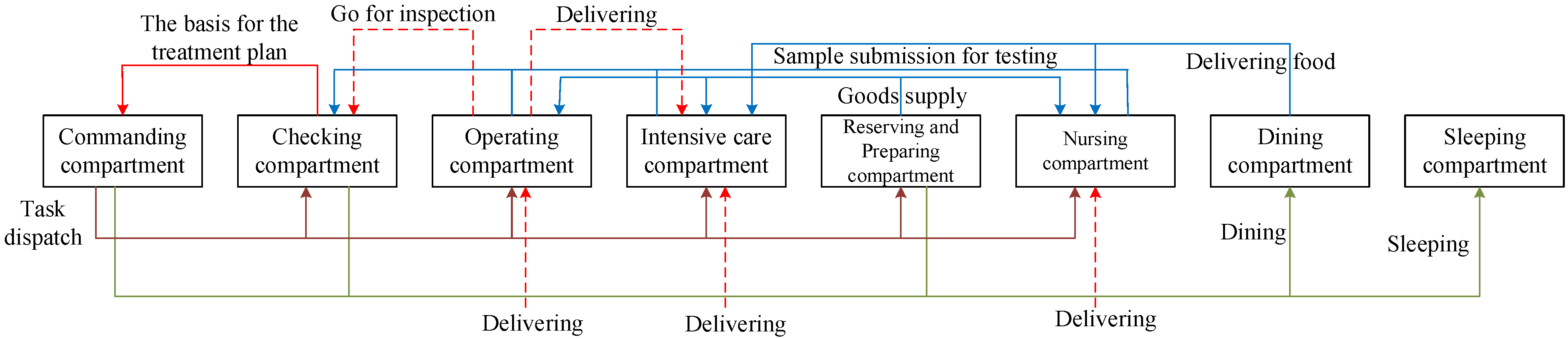
2.3. Analysis of the Relationship between Carriages
3. Carriage Layout Design Method
3.1. Requirements for Ergonomics
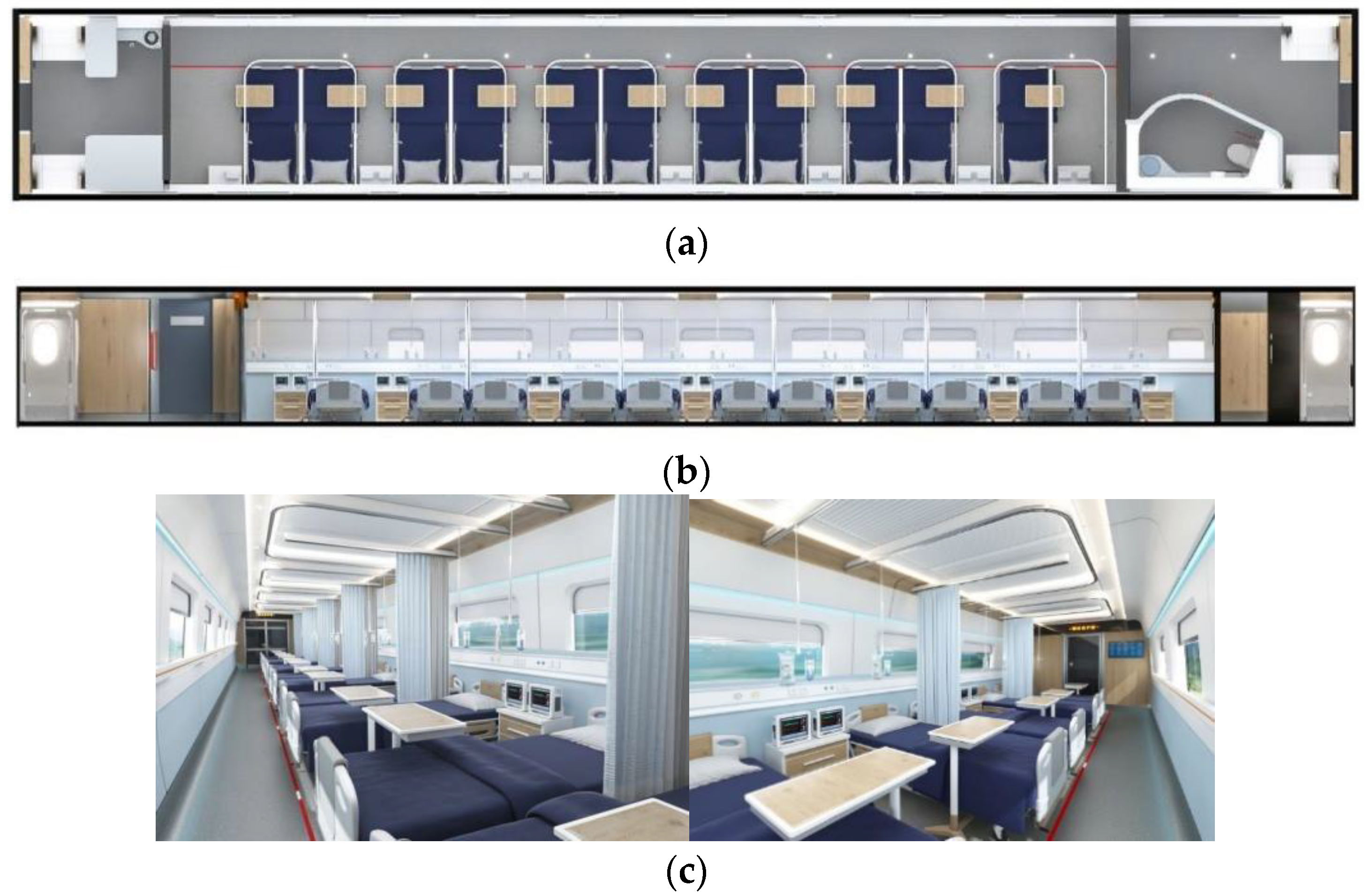
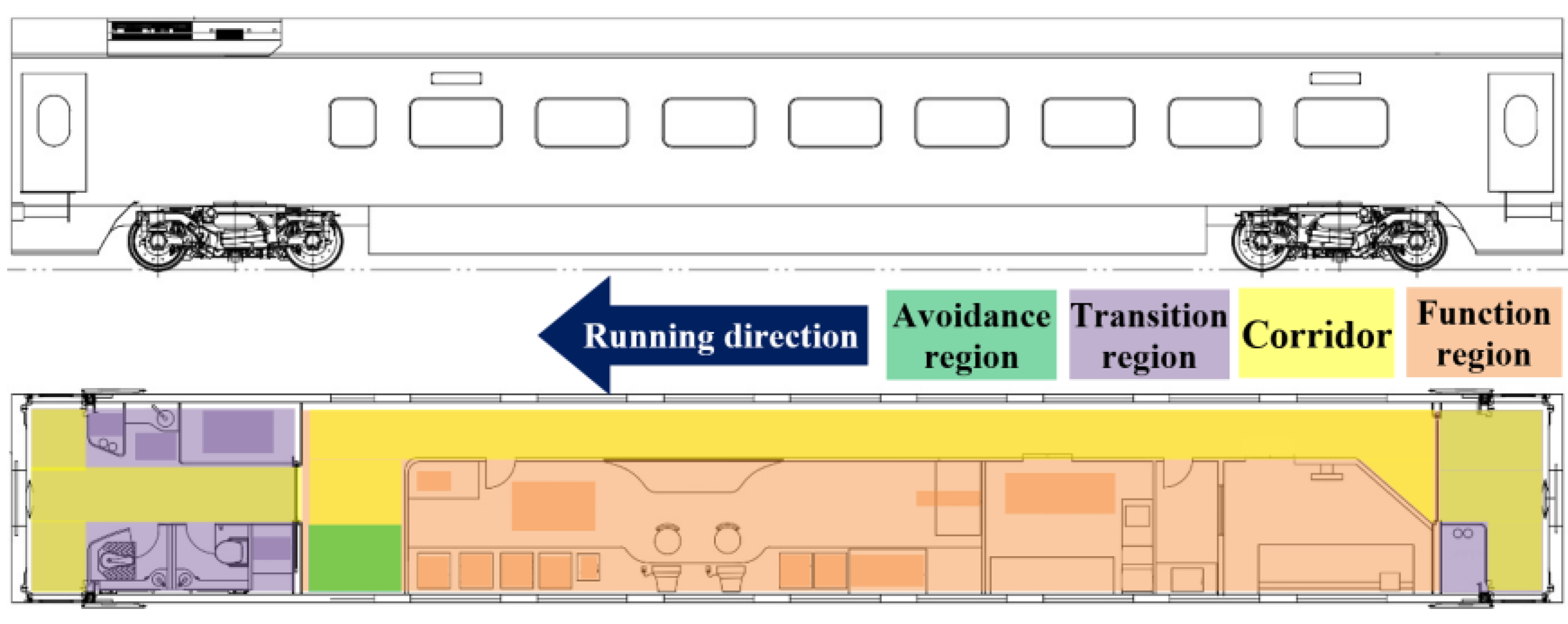
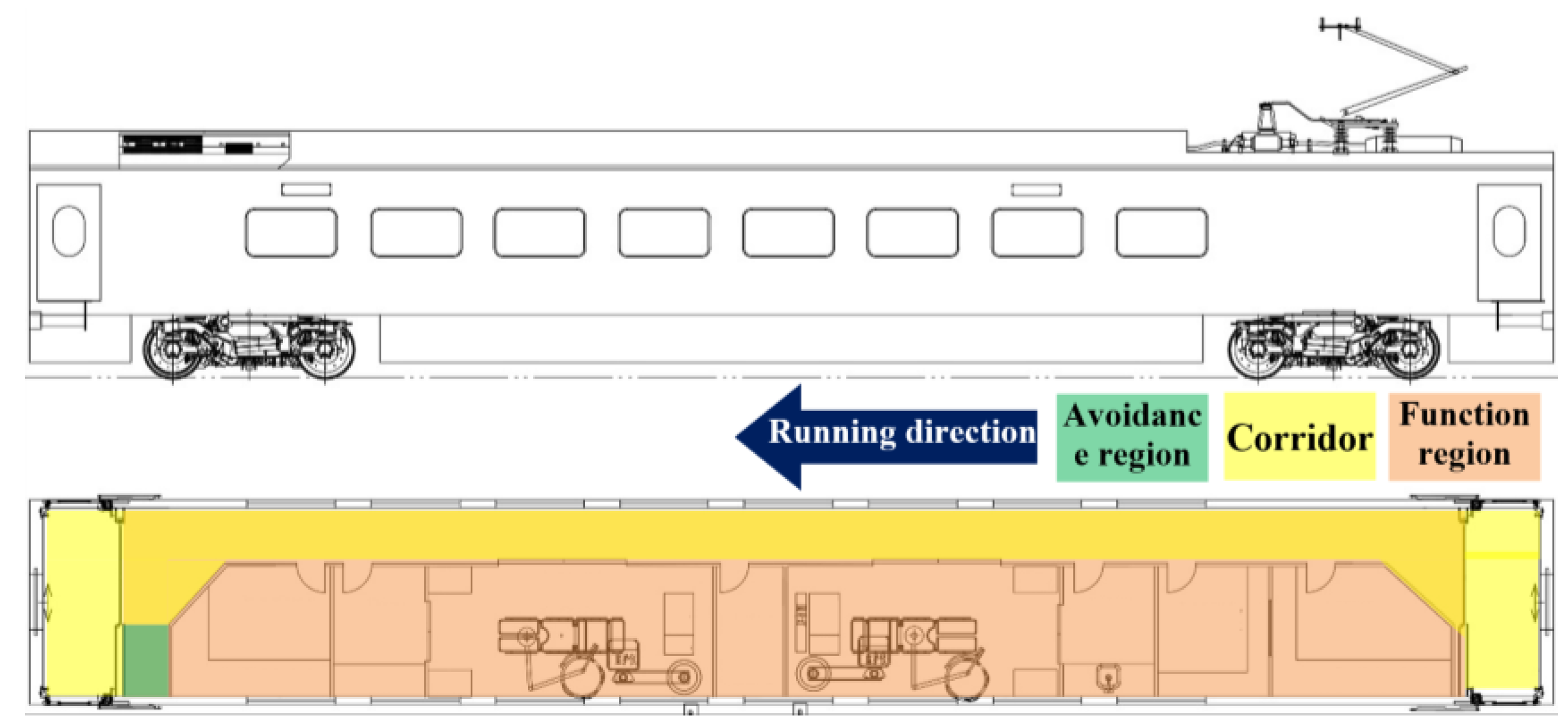
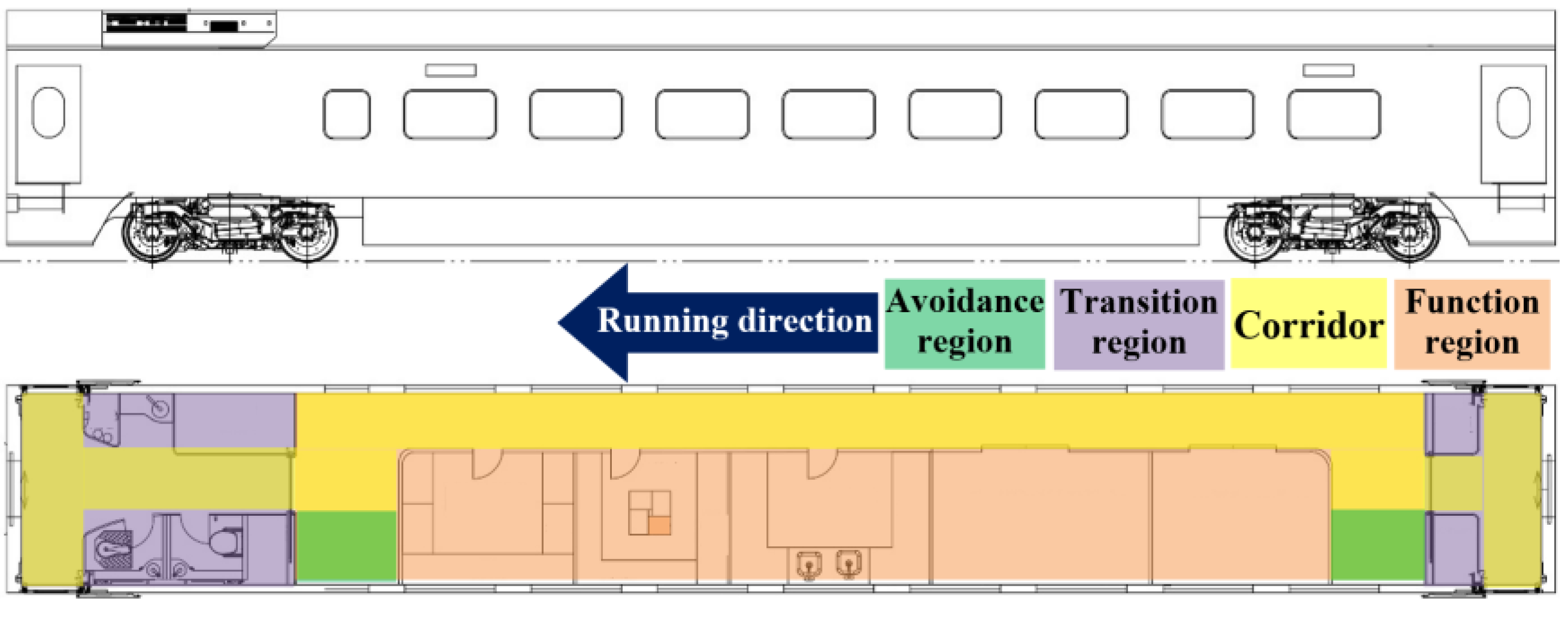
3.2. Space Layout Design of the Carriage
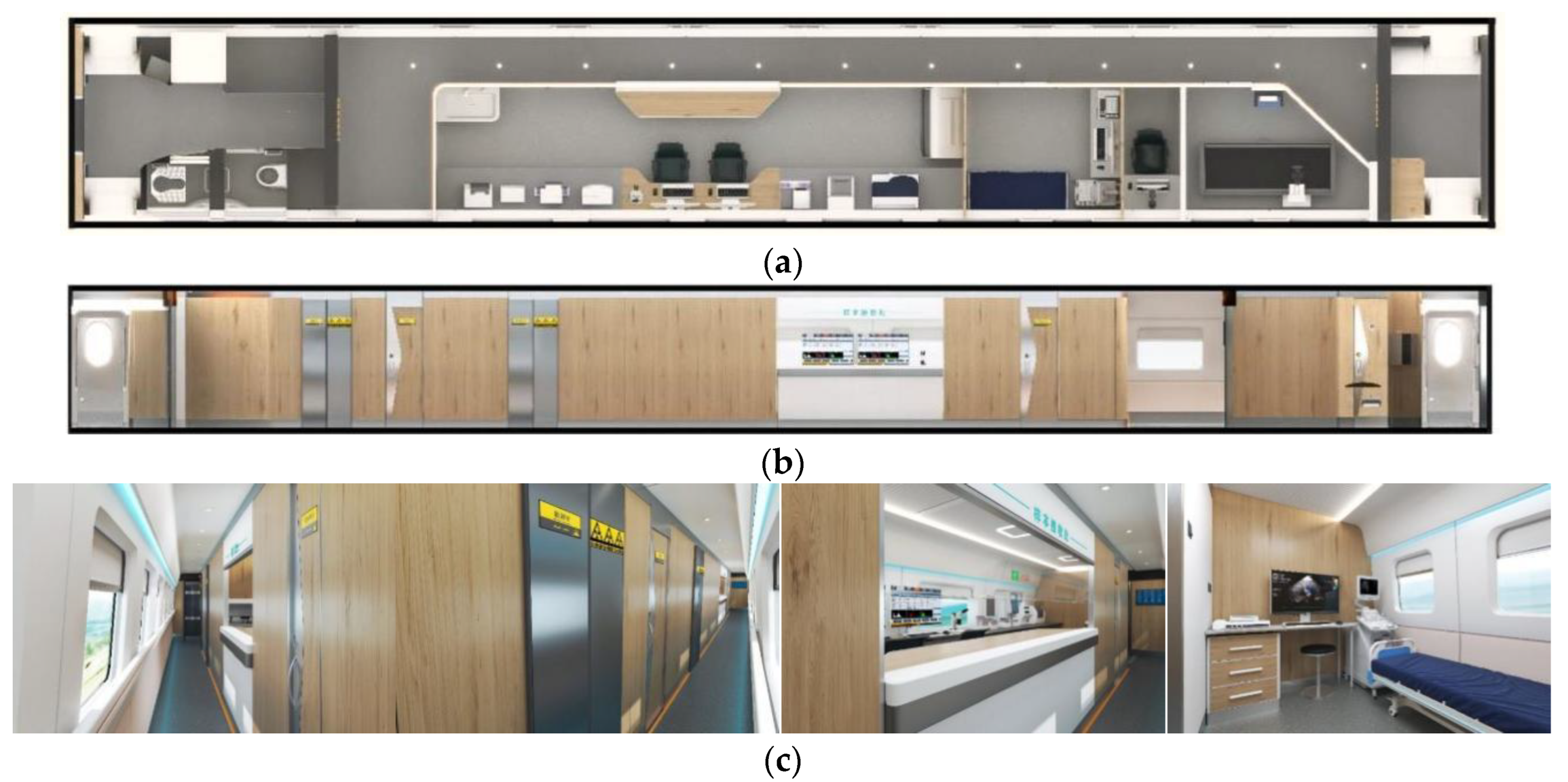
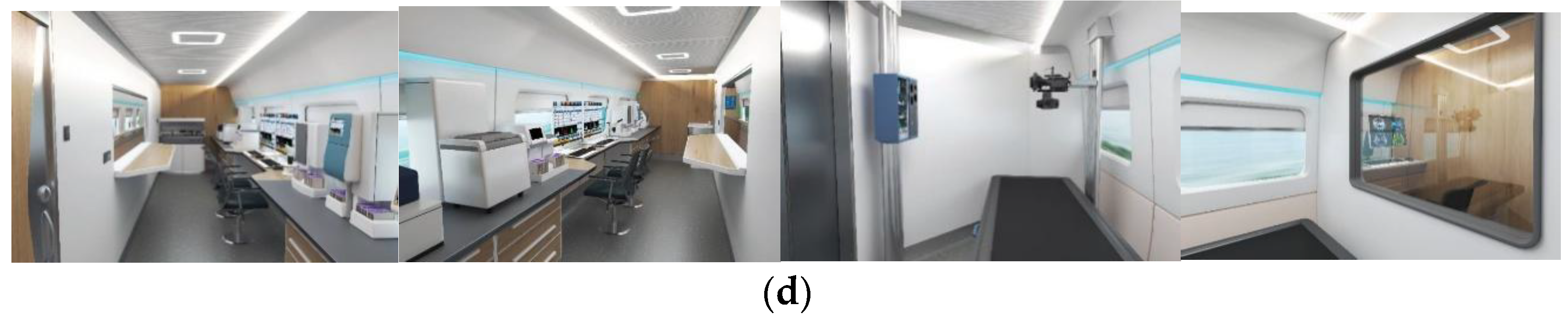
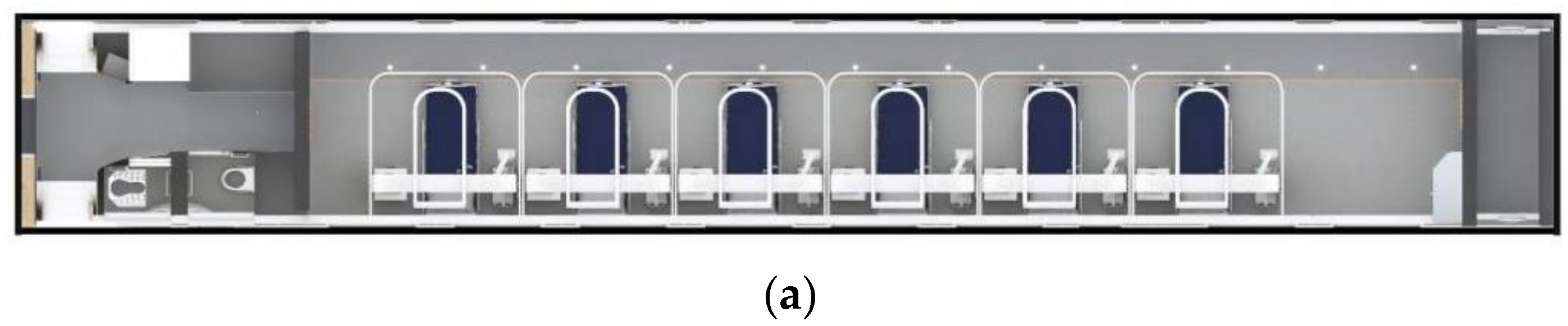
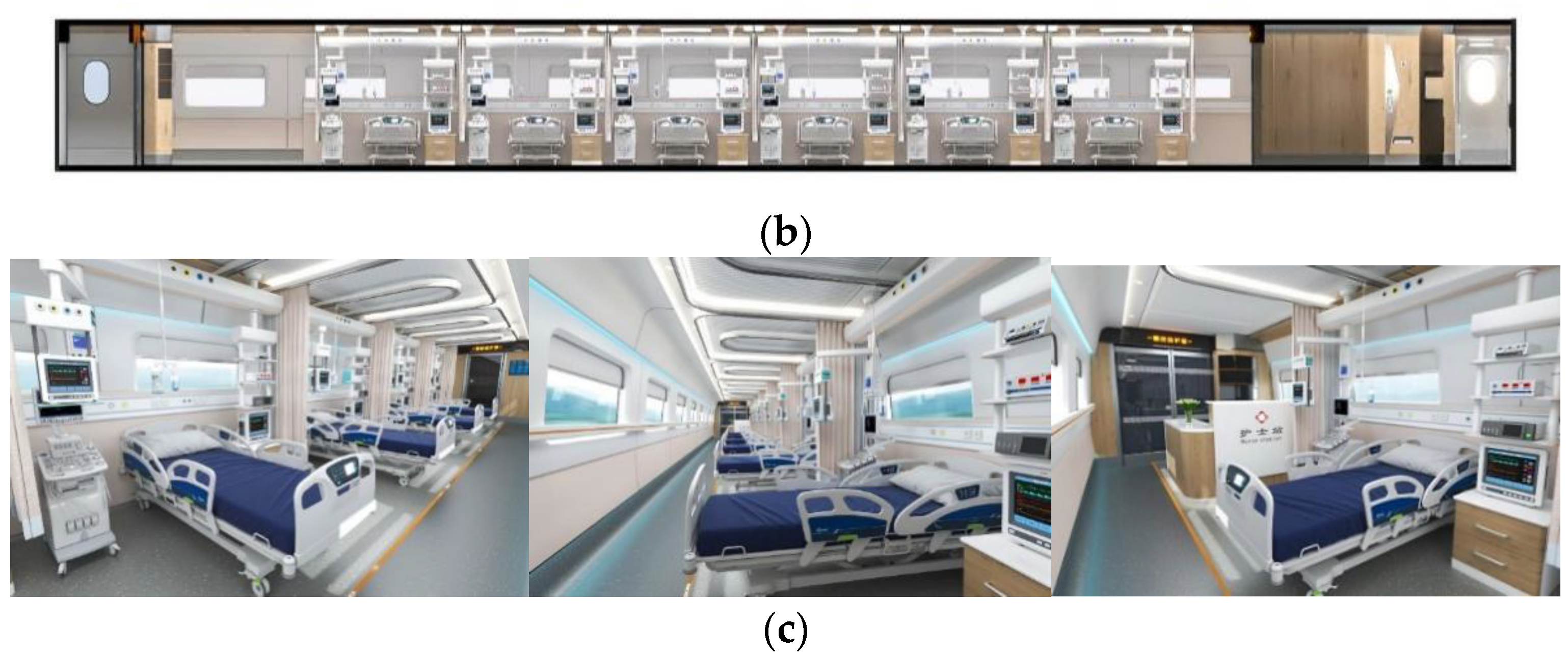
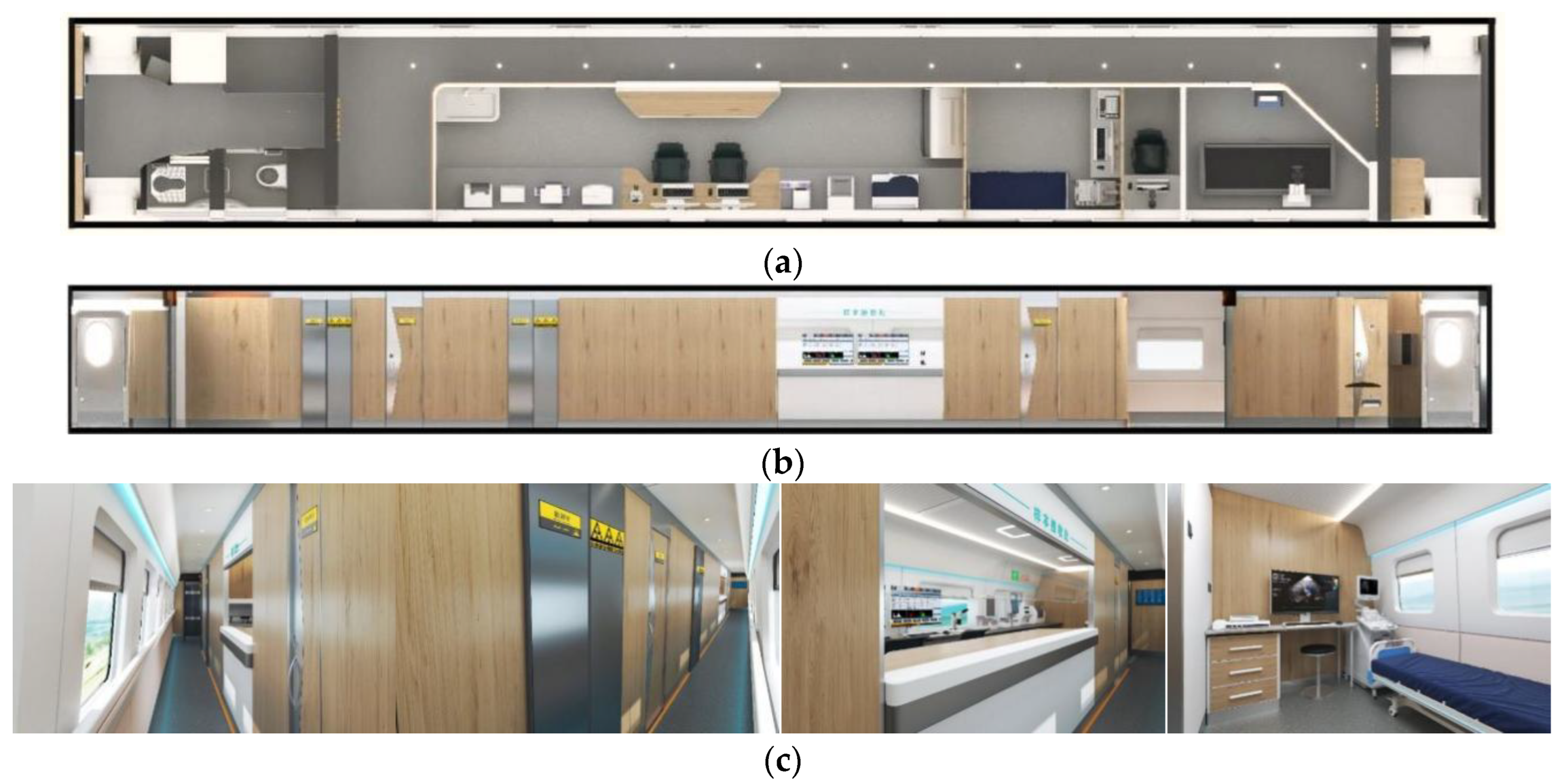
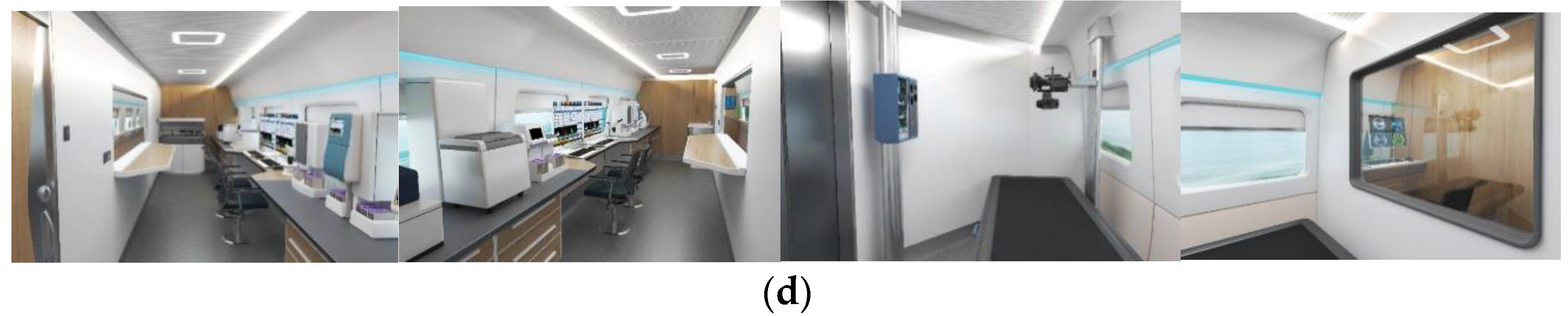
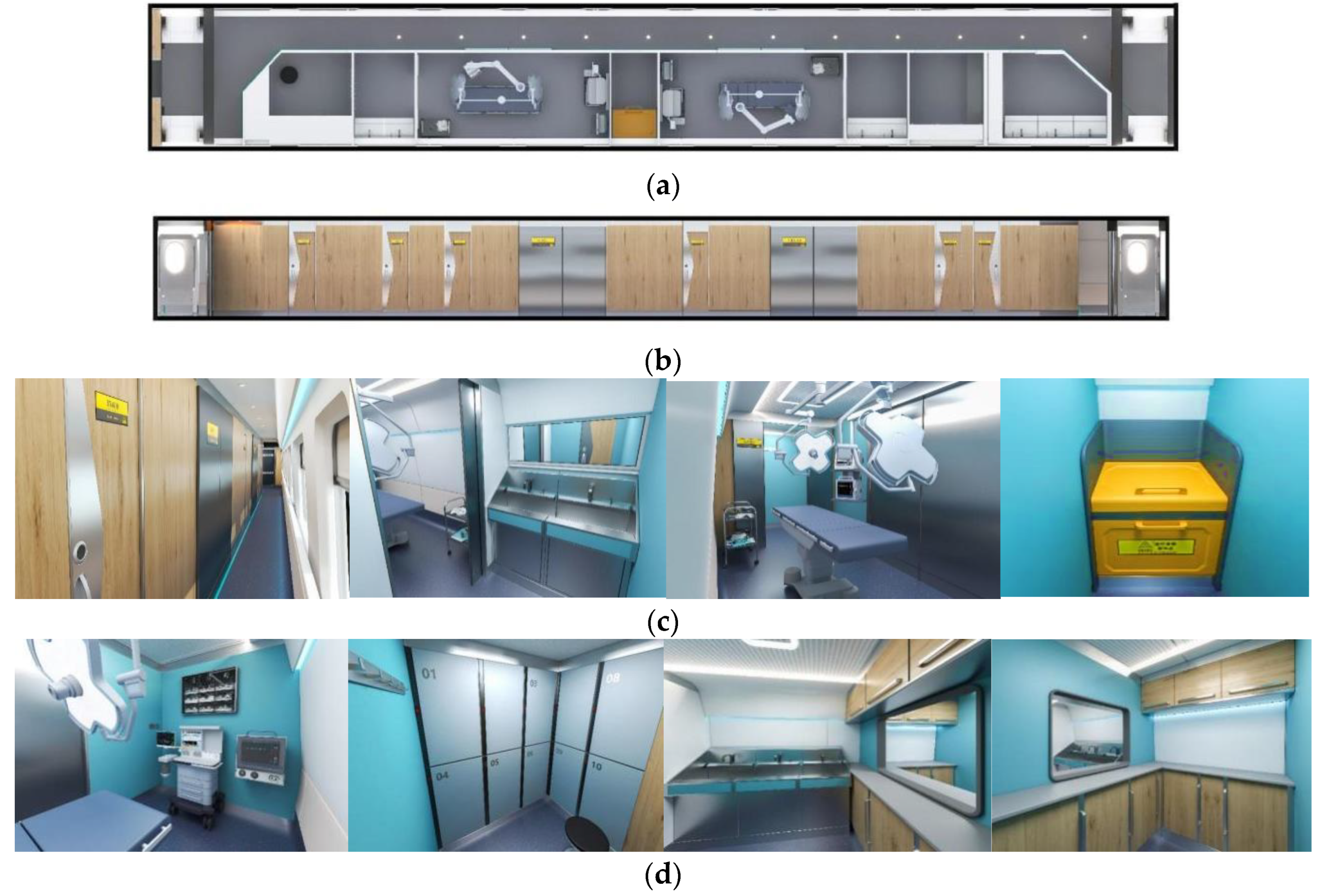
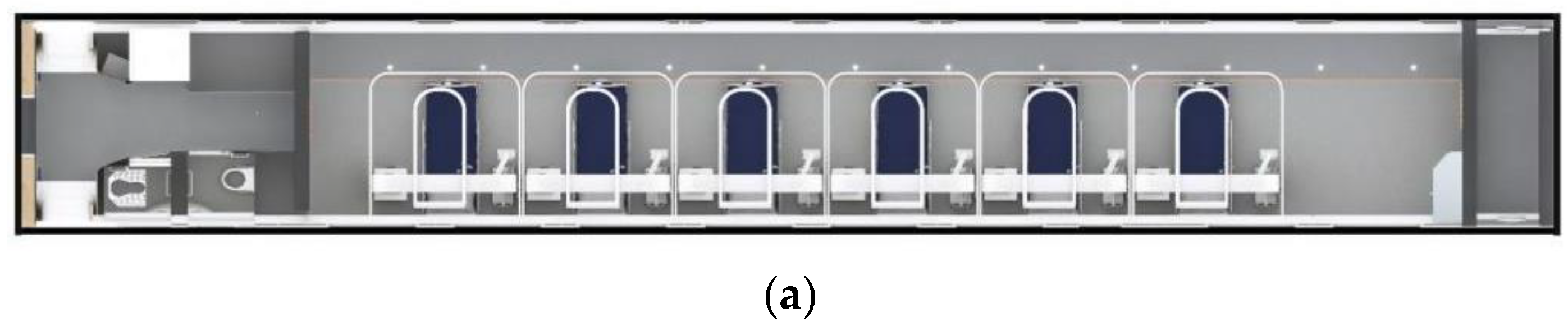
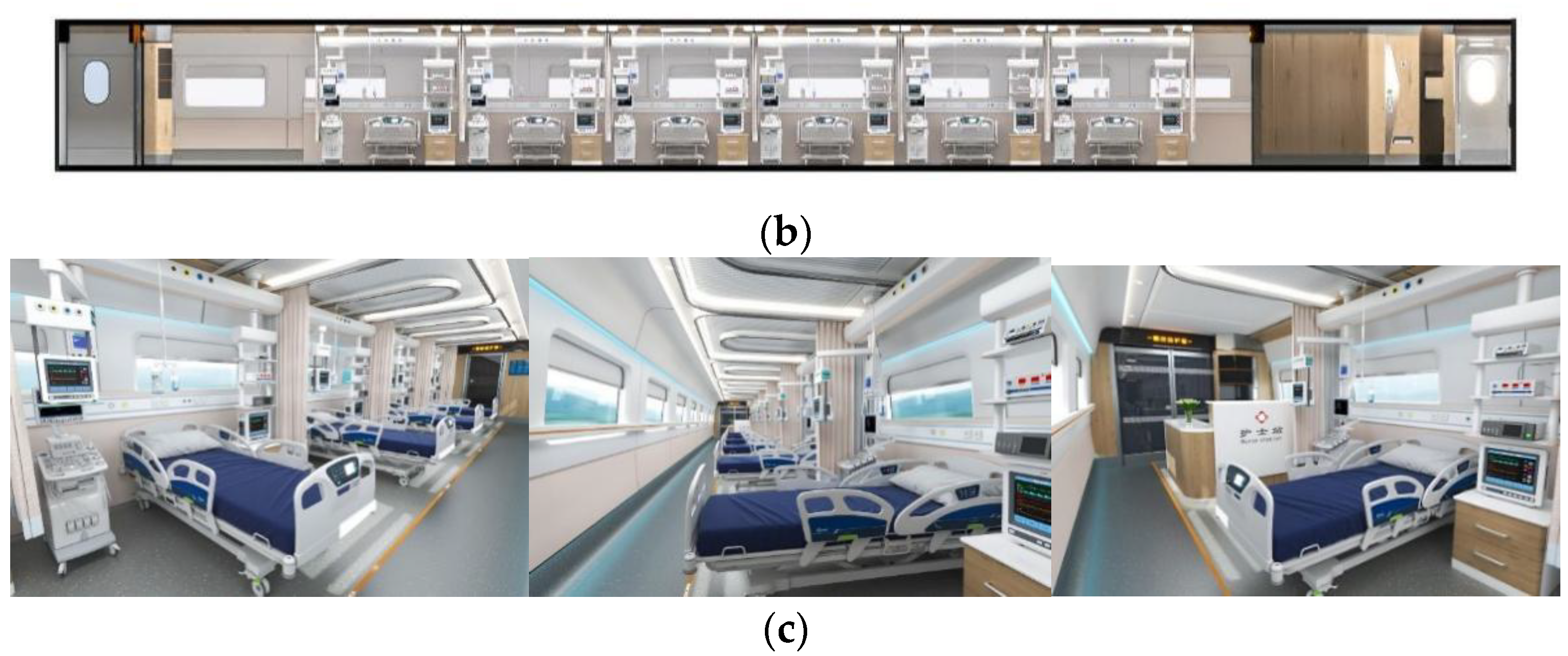
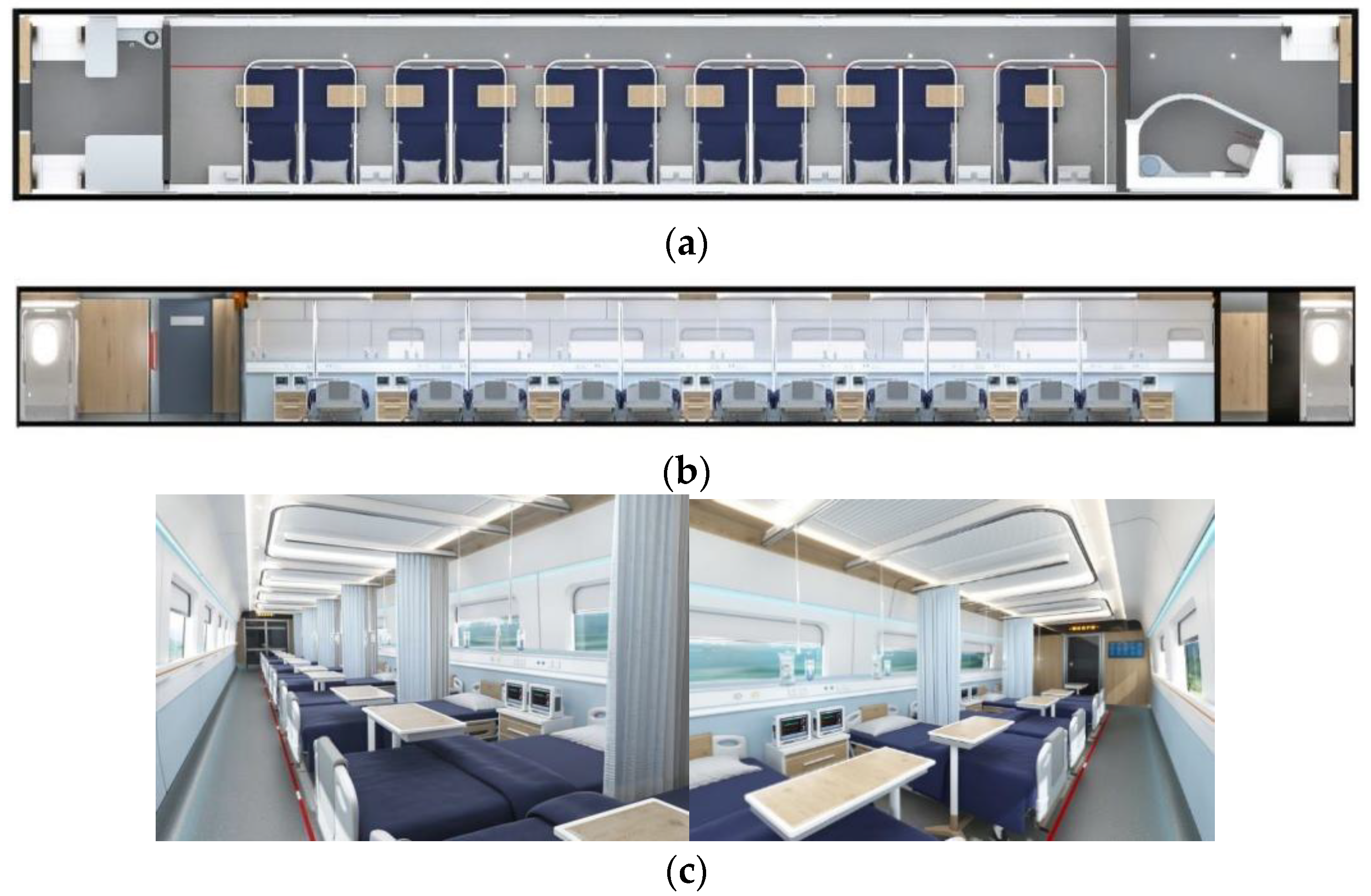
3.3. Interior Design Effect of the Carriage

4. Results
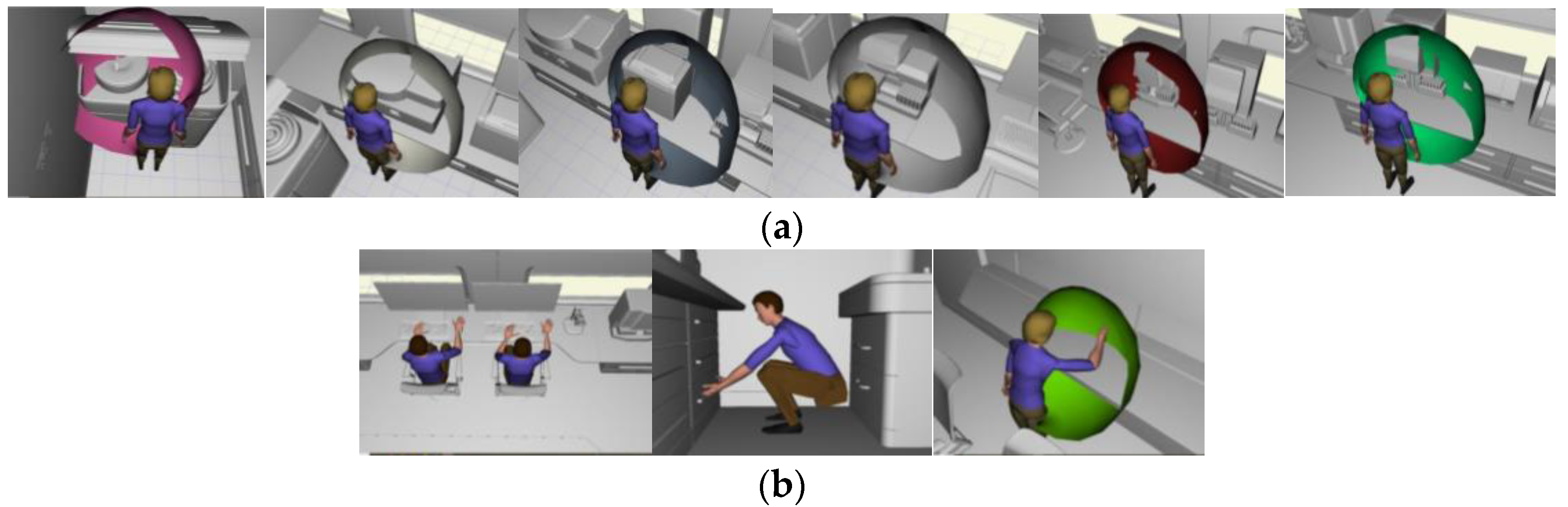
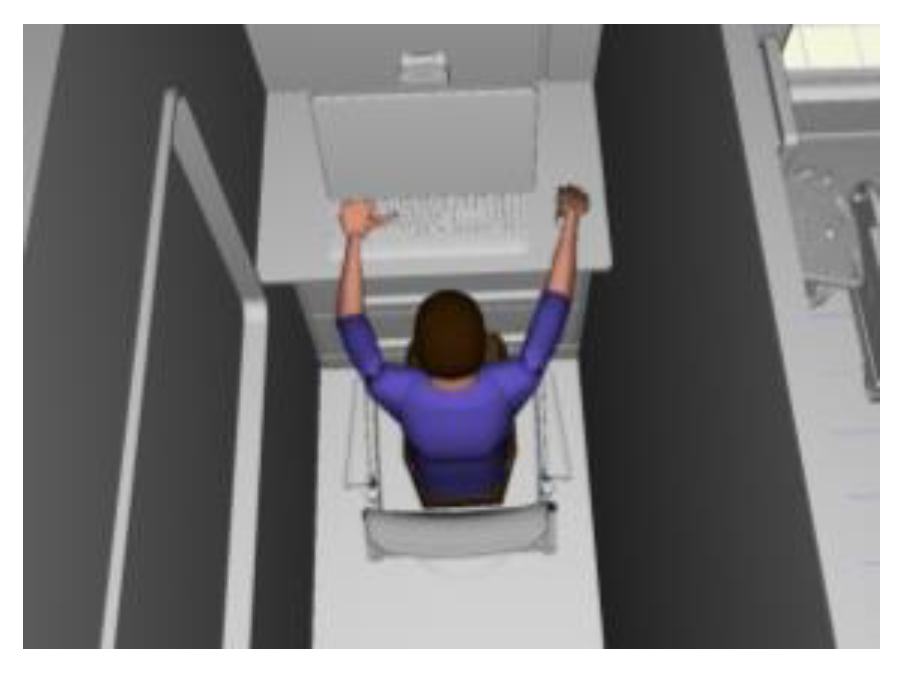
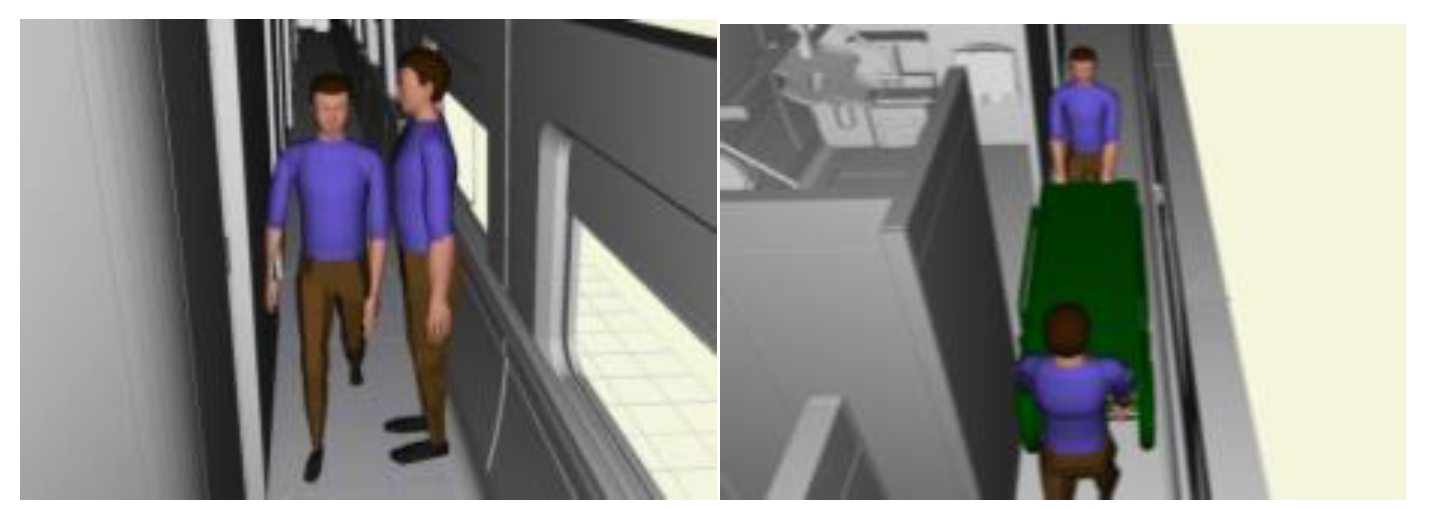
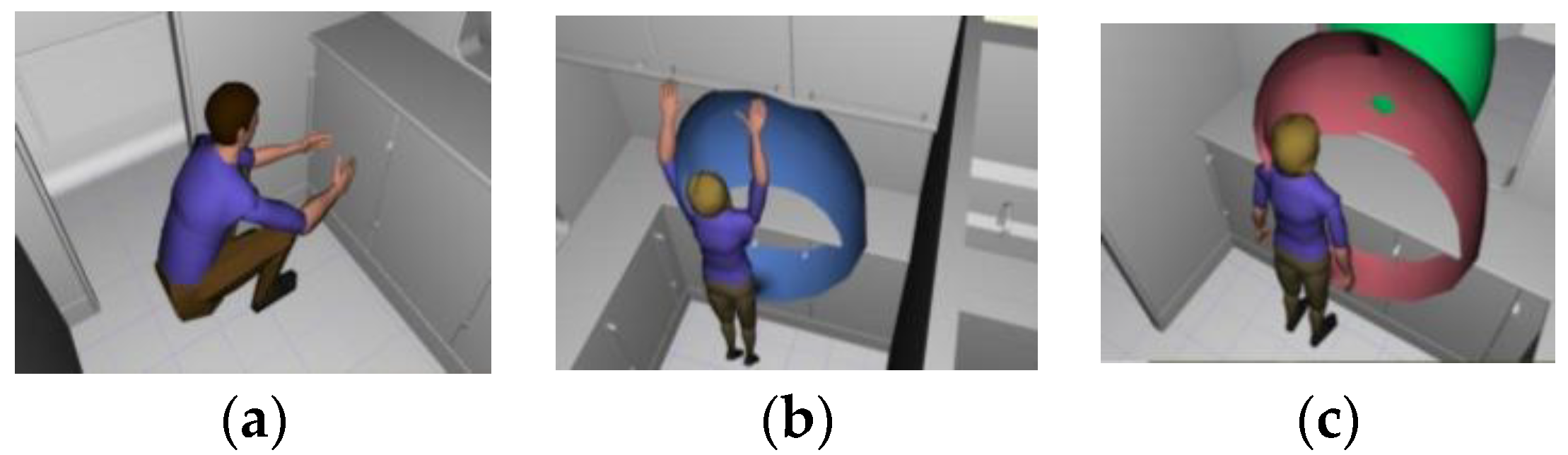
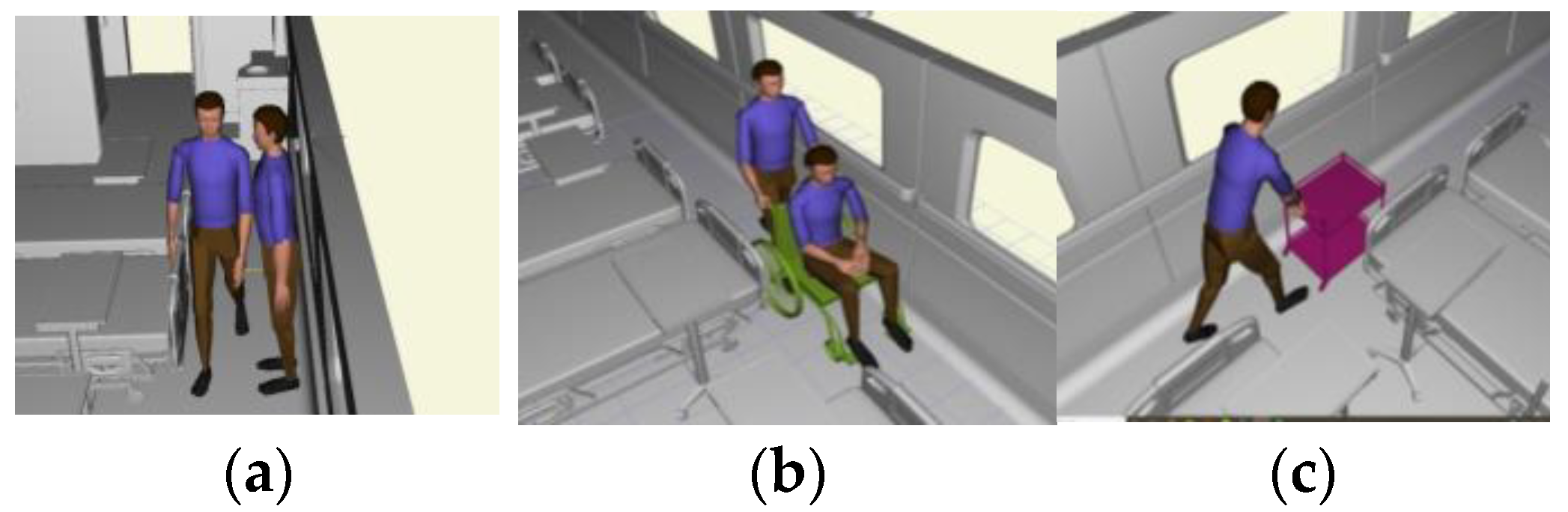
4.1. Virtual Simulation Evaluation
4.1.1. Software Simulation Process
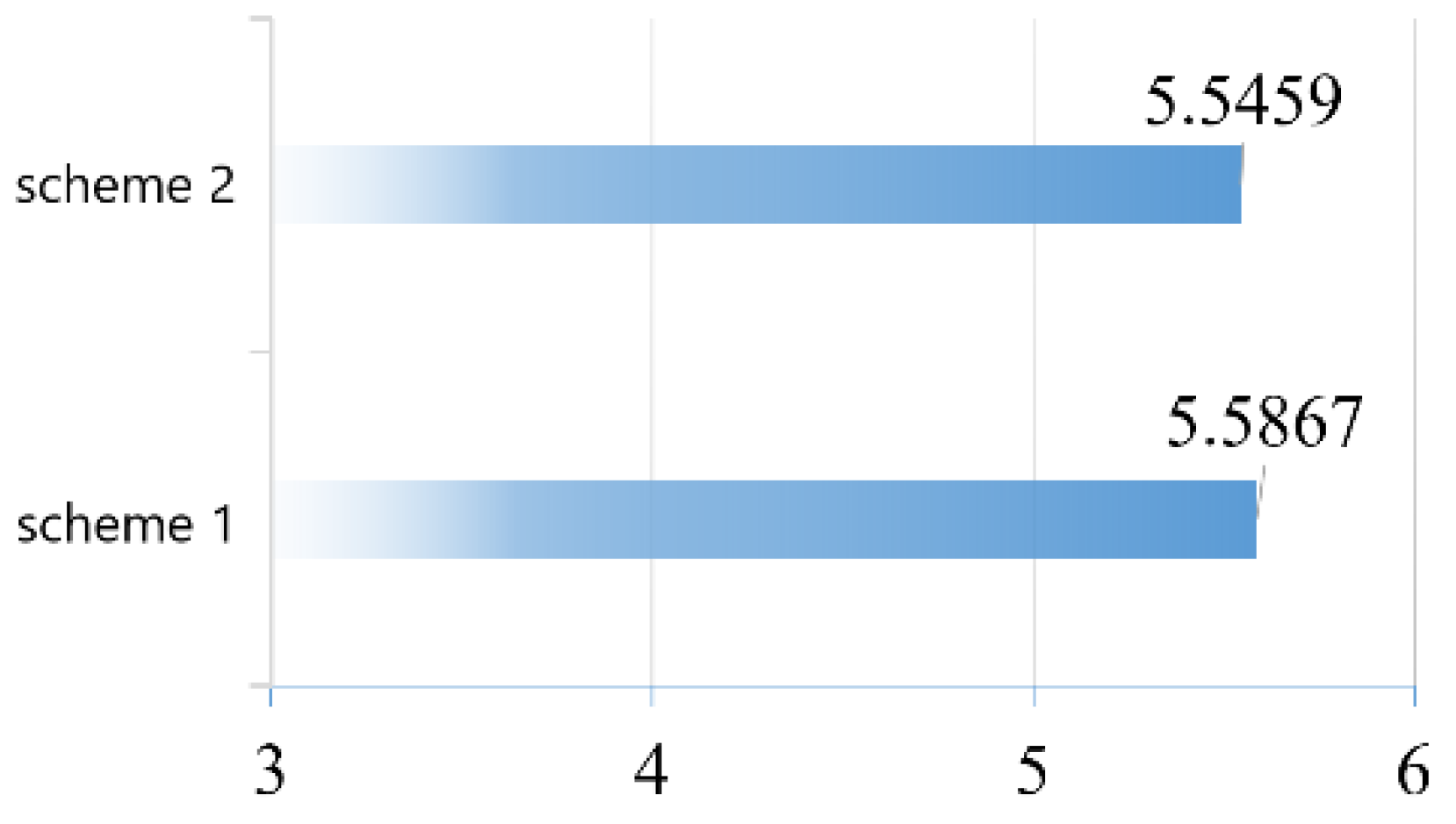
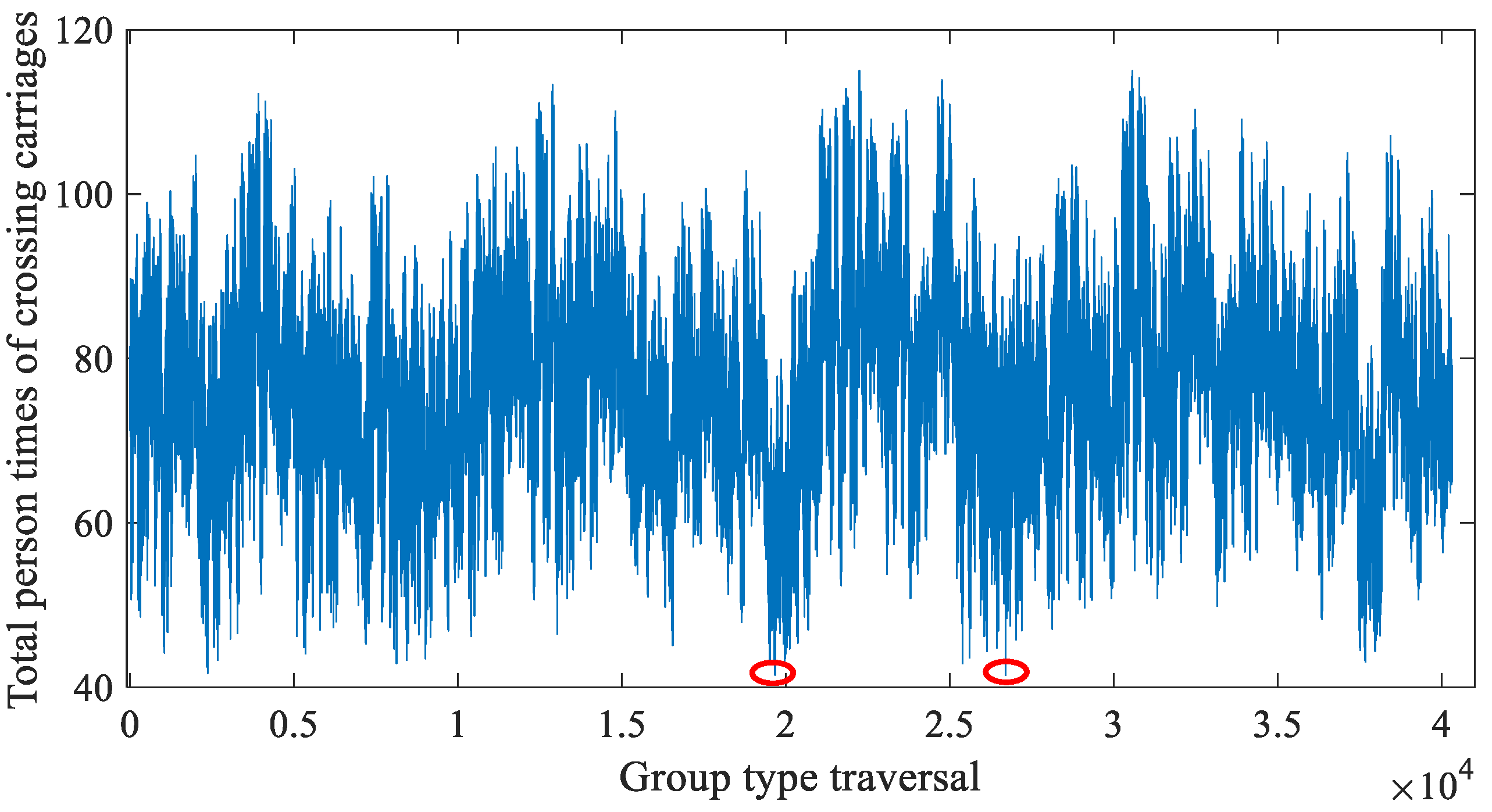
4.1.2. Simulation Results and Analysis
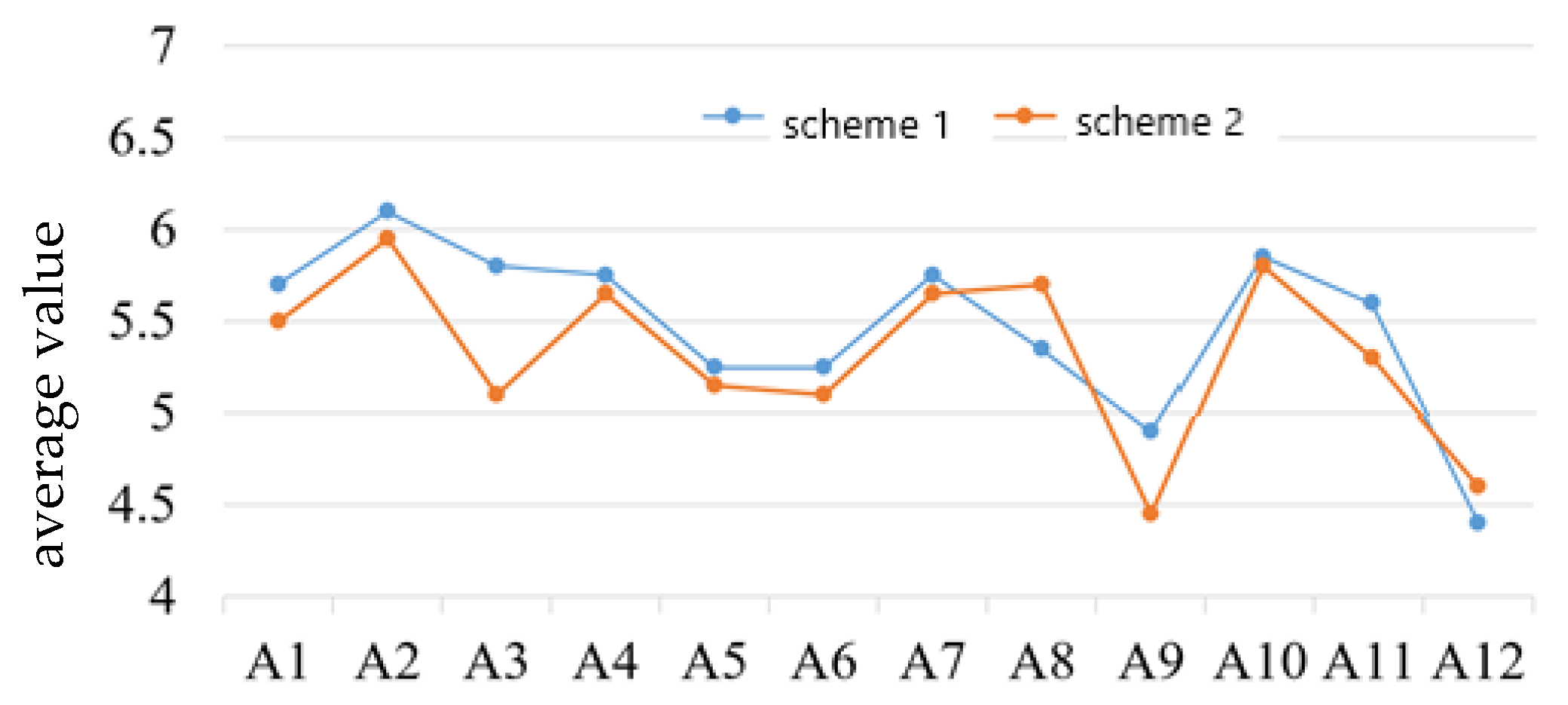
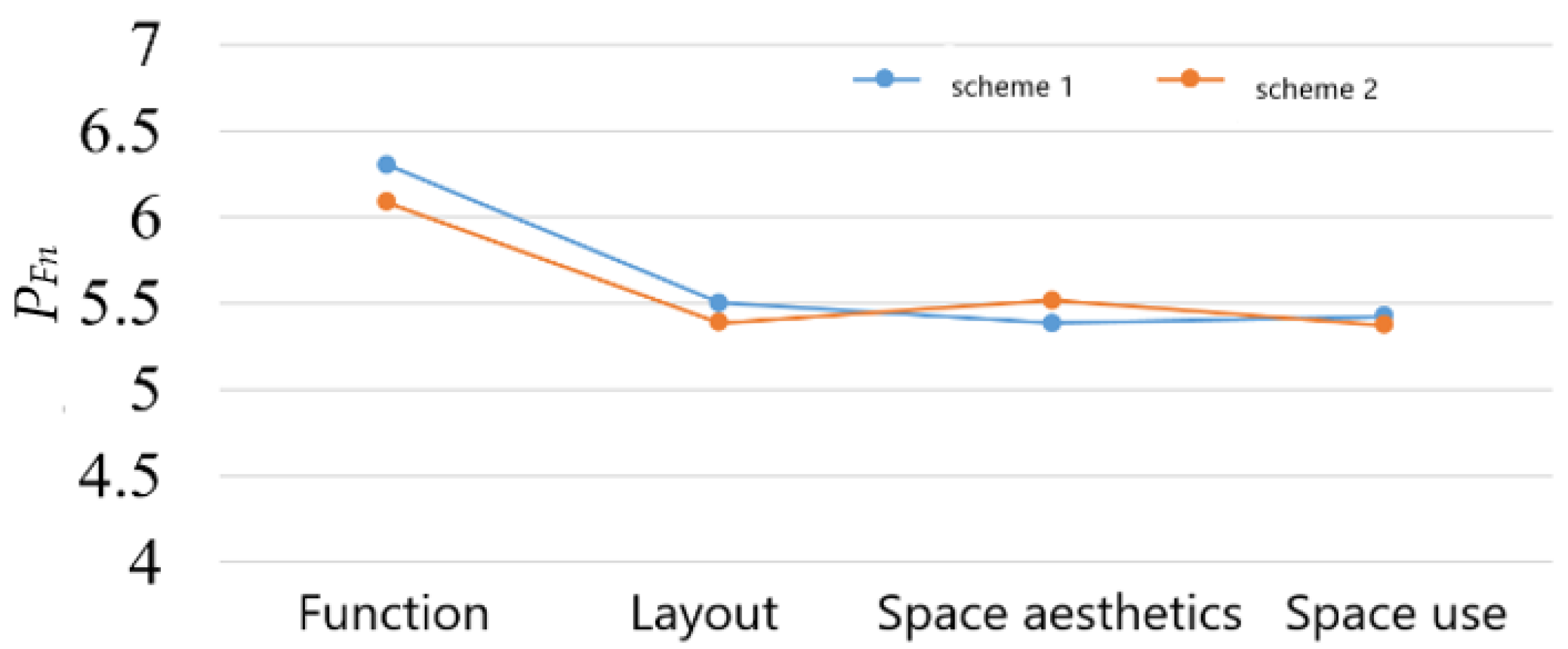
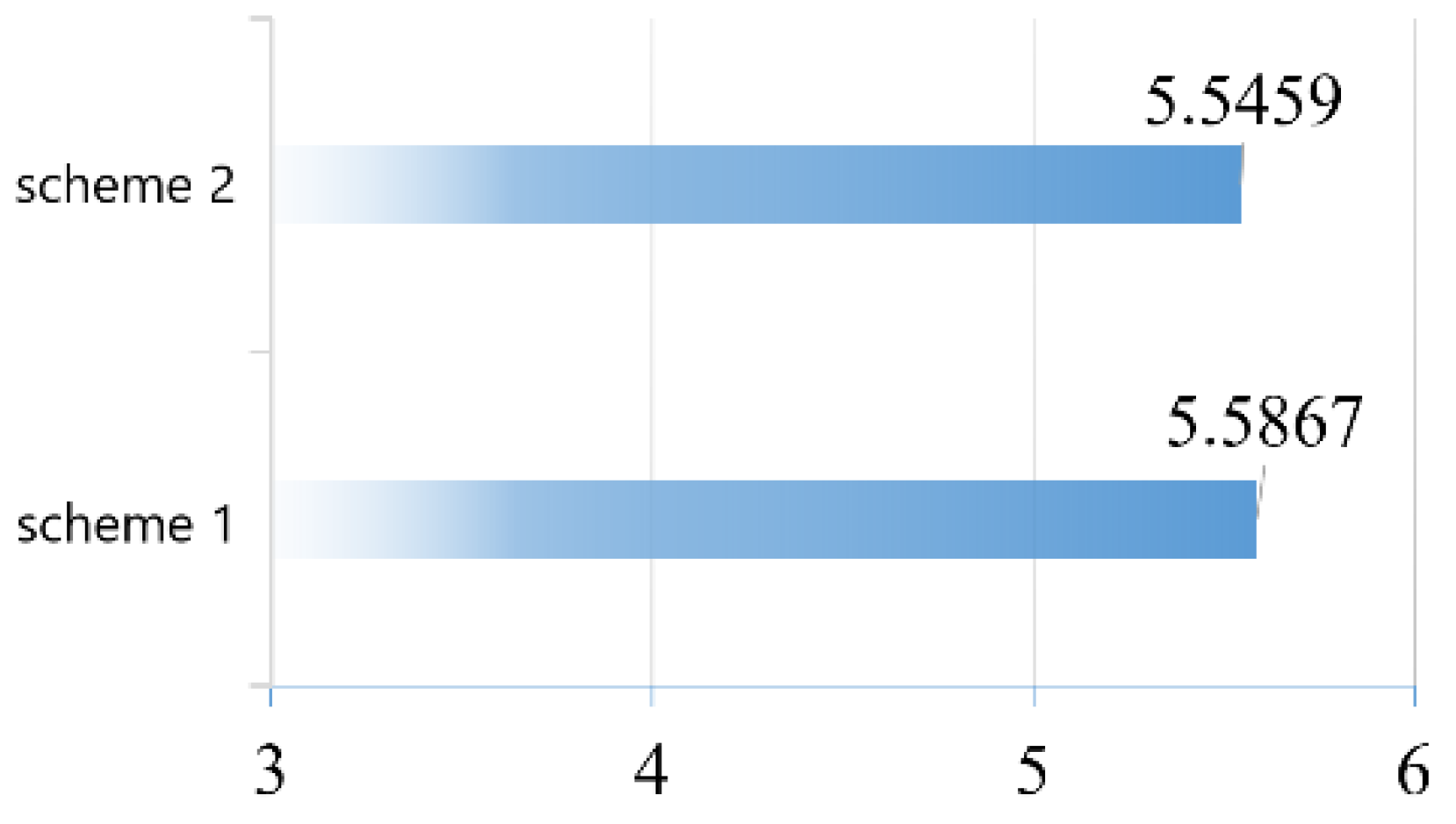
4.2. Subjective Fuzzy Evaluation
4.2.1. Evaluation Course
4.2.2. Evaluation Results and Analysis
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Chatterjee, P. Hospital train provides lifeline to rural India. Lancet 2010, 375, 1860–1861. [Google Scholar] [CrossRef] [PubMed]
- Mommsen, P.; Bradt, N.; Zeckey, C.; Andruszkow, H.; Petri, M.; Frink, M.; Hildebrand, F.; Krettek, C.; Probst, C. Comparison of helicopter and ground Emergency Medical Service: A retrospective analysis of a German rescue helicopter base. Technol. Health Care 2012, 20, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Mishra, P.; Dasar, P.; Sandesh, N.; Kumar, S.; Chand, B.R.; Airen, B.; Jain, D.; Warekar, S. Dental Camp Experience in Lifeline Express (LLE) Train among Rural Population of Central, India. J. Clin. Diagn. Res. JCDR 2014, 8, ZC72–ZC74. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.S.; Huang, C.J.; Jing, J.B.; Yao, L.; Chen, Y.; Lin, H. Development of Land Large Mobile Medical Emergency Equipment for Disaster Medical Rescue. Hosp. Adm. J. Chin. People’s Lib. Army 2014, 21, 918–919. [Google Scholar]
- Deng, M.J.; Tao, J.; Jing, J.B.; Sun, H.J.; Li, H.; Shi, W.F. Rescue-Dedicated Train for Transportation of the Wounded in Earthquake: Organization and Management. Hosp. Adm. J. Chin. People’s Lib. Army 2008, 15, 1112–1114. [Google Scholar]
- Wu, Z.W.; Ding, L.F. EMU Body Structure and Equipment; Beijing Jiaotong University Press: Beijing, China, 2012. [Google Scholar]
- Li, J.; Xu, B.C. Analysis of High-speed Train Seat Design Procedure under the System Design Conception. Packag. Eng. 2011, 32, 30–33. [Google Scholar]
- Wu, F.; Li, Y.M.; Zhang, H.J.; Yang, X.G.; Wang, K.Y.; Ma, X.; Cai, F.; Zhao, Y.; Tan, Y.J. Formation form and module function of medical train based on China standard EMU. Chin. Med. Equip. J. 2016, 37, 32–34. [Google Scholar]
- Li, Y.M.; Zhang, H.J.; Yang, B.; Yang, X.-G.; Wu, F.; Ma, X.; Cai, F.; Zhao, Y.; Tan, Y.J. Application of medical train and prospects of high-speed railway medical train in China and foreign countries. Chin. Med. Equip. J. 2016, 37, 118–120. [Google Scholar]
- Zhao, Y.; Wu, Y.M.; Hu, D.; Xiang, Z.R.; Zhi, J.Y.; Xu, B.C. HTA-based Modeling Study of the Process of Medical Transport Tasks in High-speed Health Trains. Technol. Health Care 2023, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kocev, I.; Achkoski, J.; Bogatinov, D.; Koceski, S.; Trajkovik, V.; Stevanoski, G.; Temelkovski, B. Novel approach for automating medical emergency protocol in military environment. Technol. Health Care 2018, 26, 249–261. [Google Scholar] [CrossRef] [PubMed]
- Xing, C.H.; Liu, G.; Hu, X.B.; Jiang, D.Y.; Guo, S. Multi-region single and double rows equipment layout optimization based on SLP improved genetic algorithm. J. Sichuan Univ. (Nat. Sci. Ed.) 2022, 59, 70–78. [Google Scholar]
- Xu, Y.; Zhou, Y. Optimization of outpatient hall based on pedestrian simulation technology: Shortening of flow line and one-way walking were the targets. In Proceedings of the 2022 National Academic Symposium on Digital Technology Teaching and Research in Architecture of Architectural Colleges and Departments, Xiamen, China, 3 December 2022; pp. 81–86. [Google Scholar]
- Gui, Y.; Ma, X.Z.; Gu, M.Y. Research on the optimization of the layout of inpatient department in hospital based on ergonomics. J. Jilin Inst. Chem. Technol. 2022, 39, 50–53. [Google Scholar]
- Li, C.Y.; Hu, Y.X.; Lu, J. Spatial design and layout optimization of acupuncture rooms based on medical and nursing needs—Taking three hospitals in Ningbo as examples. Chin. Hosp. Archit. Equip. 2021, 22, 34–39. [Google Scholar]
- Kumar, A.; Bhatia, S.; Chiang, I.-J. Deployment of an in-house designed training process in a quaternary care hospital. Technol. Health Care 2013, 21, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Khariwal, S.; Kumar, P.; Bhandari, M. Layout improvement of railway workshop using systematic layout planning (SLP)–A case study. Mater. Today Proc. 2021, 44, 4065–4071. [Google Scholar] [CrossRef]
- Yuan, G.Q.; Zhang, Y.Q. Design Analysis and Applied Research Based on Color Management of Medical Space. JU SHE 2021, 36, 22–24. [Google Scholar]
- Kamal, S.M.; Dawi, N.B.M.; Sim, S.; Tee, R.; Nathan, V.; Aghasian, E.; Namazi, H. Information-based analysis of the relation between human muscle reaction and walking path. Technol. Health Care 2020, 28, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhi, J.Y.; Xiang, Z.R.; Tan, Y.J.; Li, Y.M.; Wu, F.; He, S.J.; Zhao, Y.; Li, J. Feasibility analysis of health train based on high-speed EMU. Chin. Med. Equip. J. 2019, 40, 65–77. [Google Scholar]
- Zeng, D.; Chen, Y.M. Application Research of Fuzzy Synthetic Evaluation in Product Sculpt Design. Mod. Manuf. Eng. 2010, 8, 119–123. [Google Scholar]
- Lu, P. Operation Room of China High Speed Train Research on Environment Integration Design; Southwest Jiaotong University: Chengdu, China, 2019. [Google Scholar]
- Niu, Z.K. Research on Design of Medical Laboratory Interior on High-Speed Train; Southwest Jiaotong University: Chengdu, China, 2019. [Google Scholar]
- Guan, H. The Design Studies of High Speed Nursing Car; Southwest Jiaotong University: Chengdu, China, 2019. [Google Scholar]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
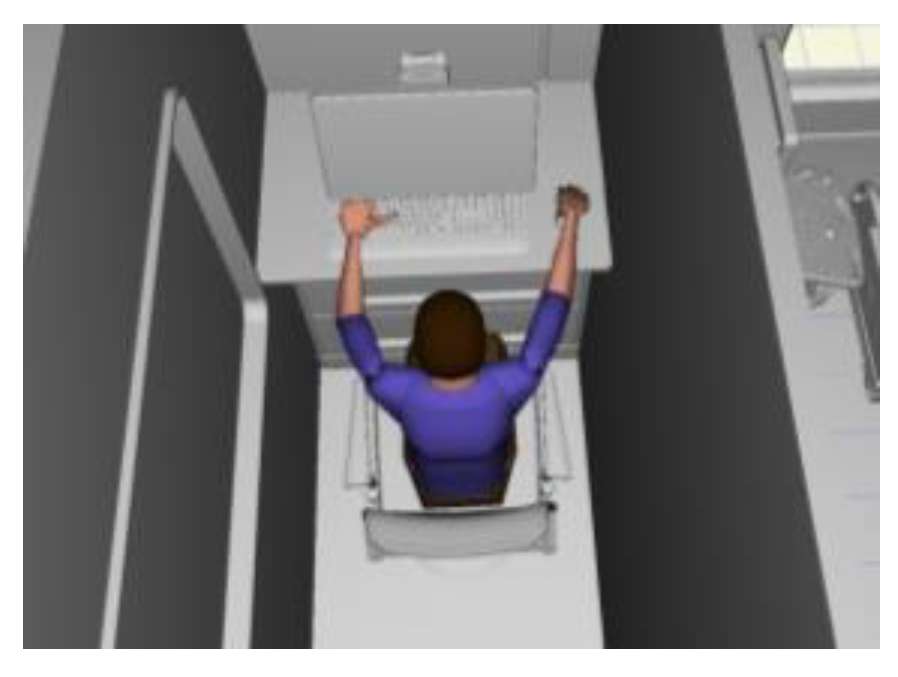
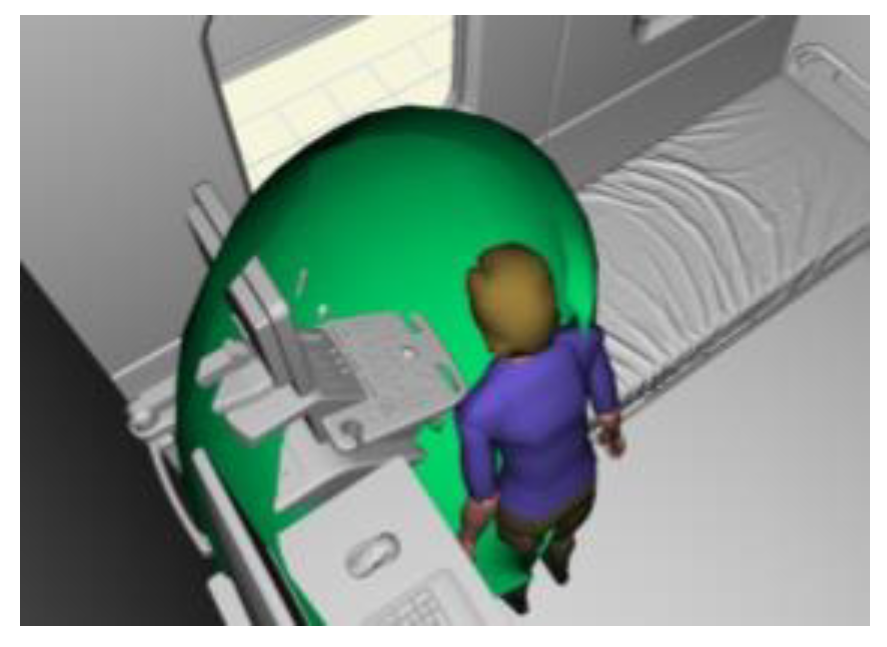
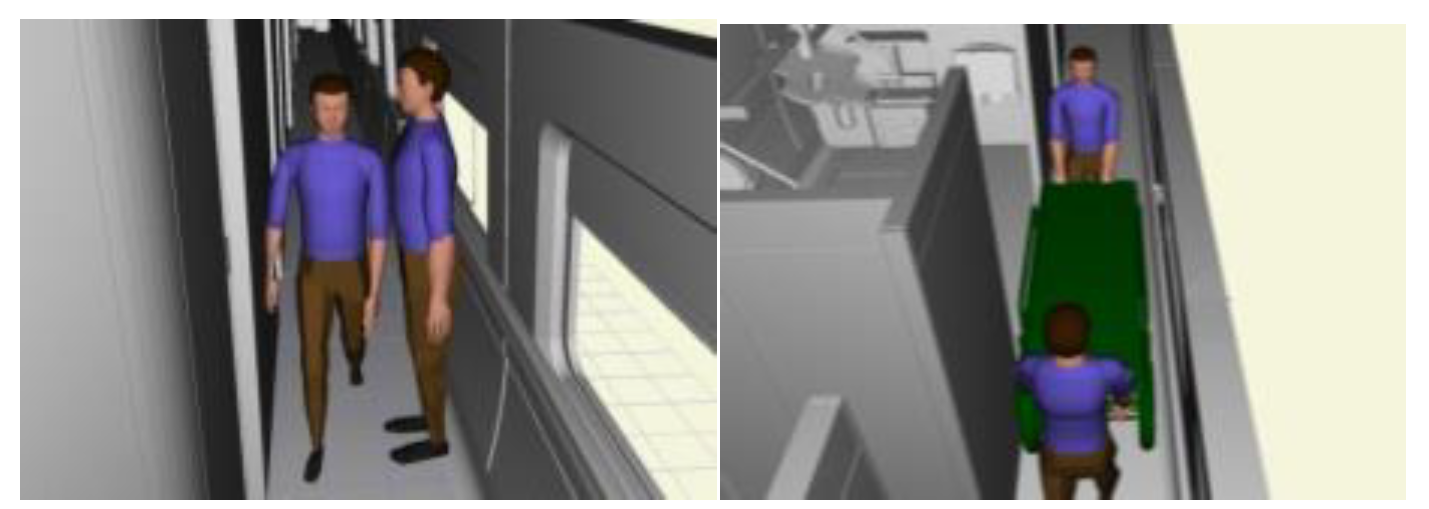
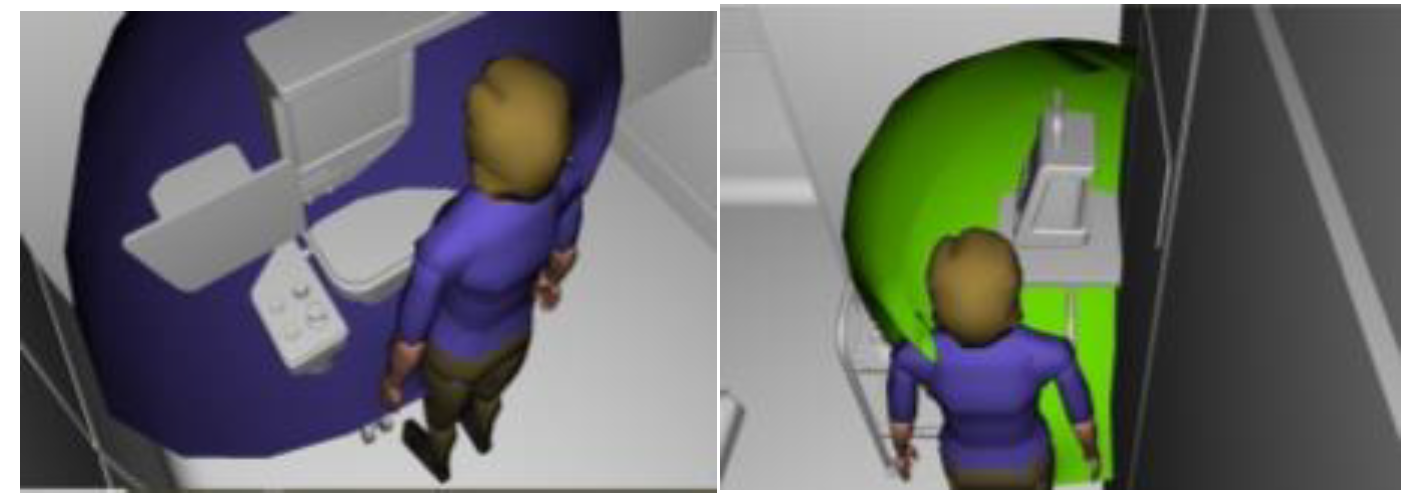
| Type | Behavior | Activity | Scenario |
|---|---|---|---|
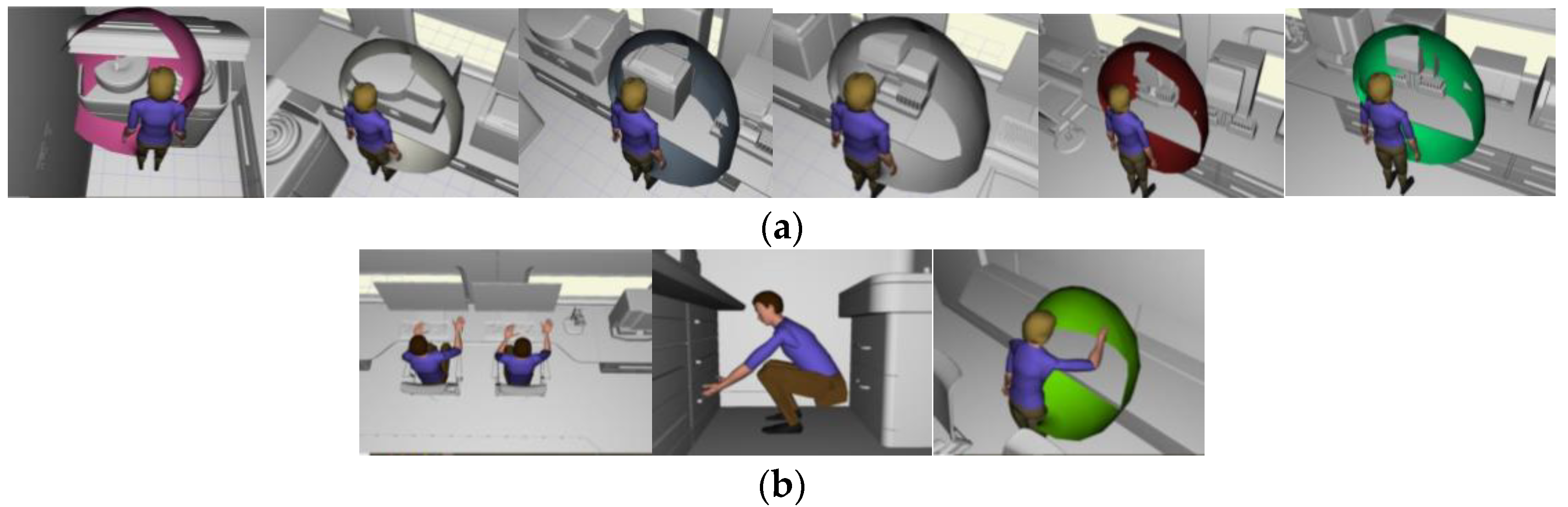
| Static | Sitting posture | Office work | Comprehensive laboratory, ultrasonic laboratory, X-ray observation room |
| Operating instrument | Comprehensive laboratory, ultrasonic laboratory | ||
| Standing posture | Operating instrument | Comprehensive laboratory, operating room, drying and packing room, cleaning room, intensive care unit | |
| Accessing items | Comprehensive laboratory, drying and packing room, cleaning room | ||
| Squatting posture | Accessing items | Comprehensive laboratory, drying and packing room, cleaning room | |
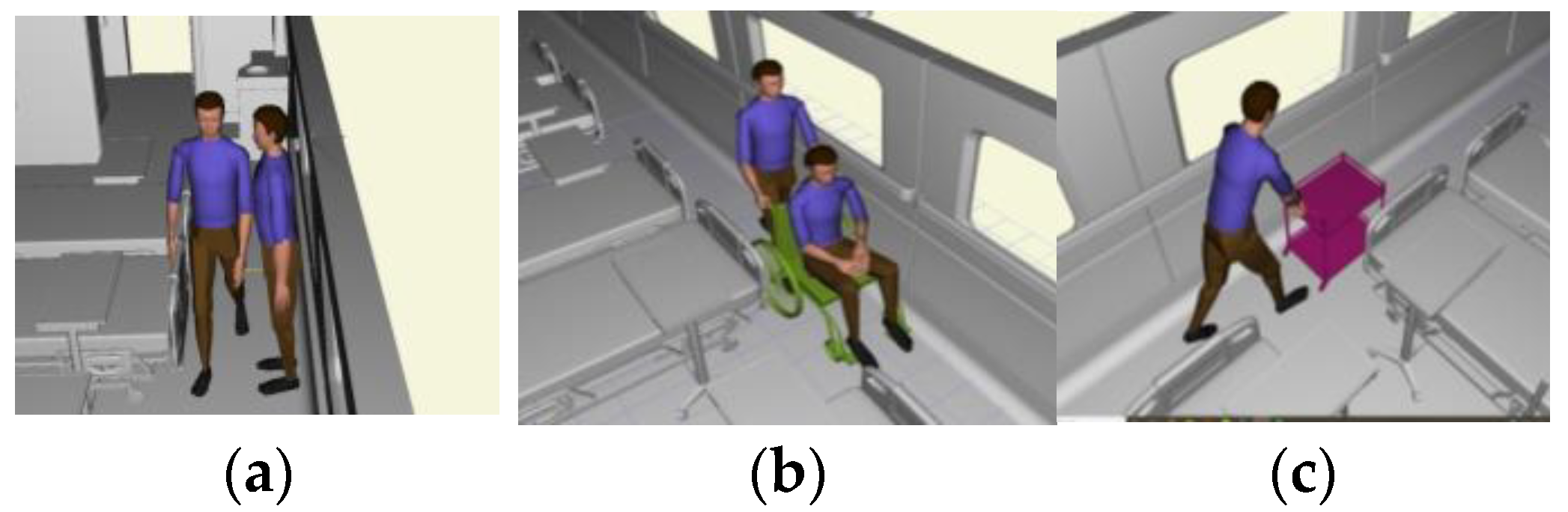
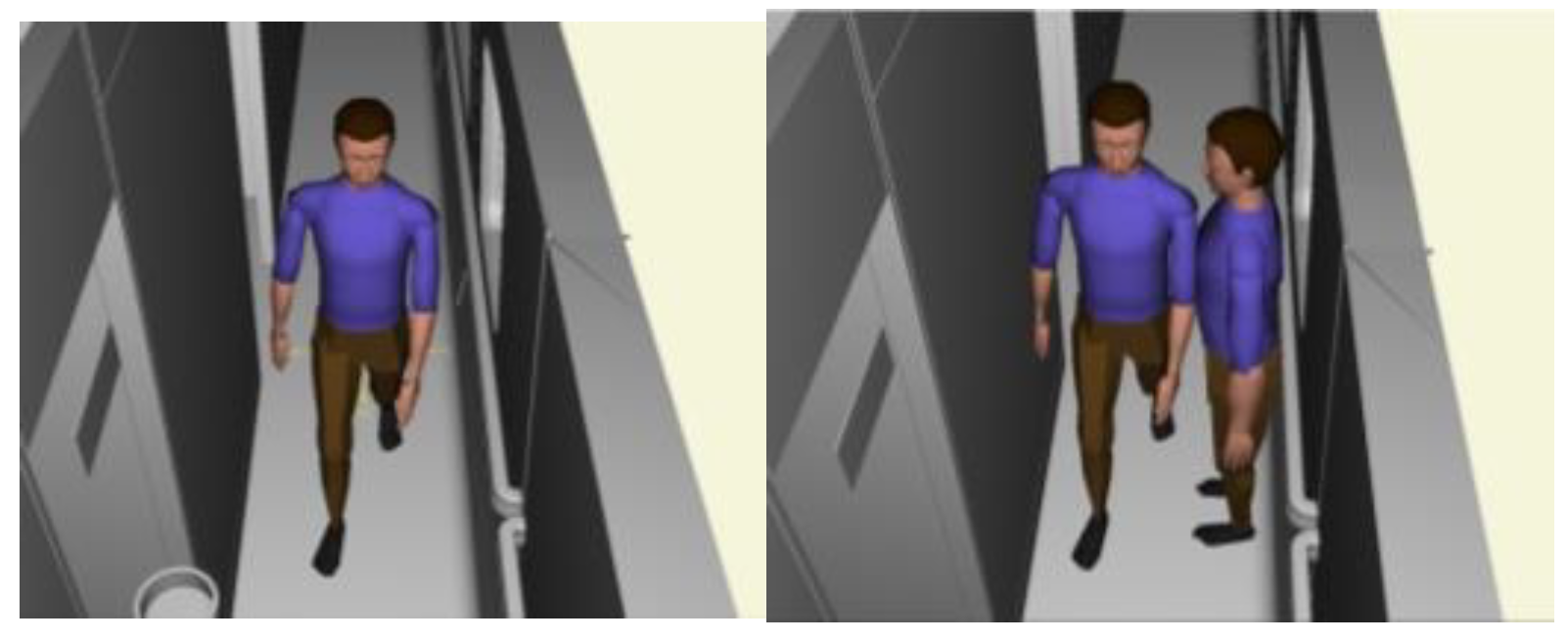
| Dynamic | Walking | Single peer | Interior of carriage and corridor |
| Personnel intersection | Interior of carriage and corridor | ||
| Load carriage | Medical care implementation | Intensive care carriage, minor injury care carriage | |
| Double-push wheel-lifting stretcher | Operation compartment and intensive care compartment | ||
| Double-carry stretcher | Intensive care carriage | ||
| Wheelchair access | Wheelchair for nursing staff | Minor injury care carriage | |
| Use of a wheelchair by the patient | Minor injury care carriage |
| Index Types | Index |
|---|---|
| F1 Function | A1 Comprehensive functional configuration |
| A2 Reasonable functional configuration | |
| A3 Spatial isolation | |
| F2 Layout | A4 Rationality of carriage formation |
| A5 The rationality of space layout in the carriage | |
| A6 Rationality of equipment layout in department | |
| F3 Space aesthetics | A7 Modeling harmony |
| A8 Colour harmony | |
| A9 Delicate details | |
| F4 Space use | A10 Space utilization |
| A11 Medical carrying capacity | |
| A12 Injury-carrying capacity |
| Scale | Meaning |
|---|---|
| 1 | Compared to two elements, they have the same importance |
| 3 | Compared to the two elements, the former is slightly more important than the latter |
| 5 | Compared to the two elements, the former is significantly more important than the latter |
| 7 | Compared to the two elements, the former is more strongly important than the latter |
| 9 | Compared to the two elements, the former is extremely important compared to the latter |
| 2, 4, 6, 8 | Intermediate value of adjacent judgments mentioned above |
| Reciprocal | If the importance ratio of element i to element j is aij, then the importance ratio of element j to element i is 1/aij |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Wu, Y.; Zhao, M.; Xiang, Z.; Zhi, J.; Xu, B. Design and Evaluation of the Internal Space Layout of High-Speed Health Trains Based on Improved Systematic Layout Planning. J 2023, 6, 361-383. https://doi.org/10.3390/j6030025
Zhao Y, Wu Y, Zhao M, Xiang Z, Zhi J, Xu B. Design and Evaluation of the Internal Space Layout of High-Speed Health Trains Based on Improved Systematic Layout Planning. J. 2023; 6(3):361-383. https://doi.org/10.3390/j6030025
Chicago/Turabian StyleZhao, Yi, Yongmeng Wu, Mingjing Zhao, Zerui Xiang, Jinyi Zhi, and Bochu Xu. 2023. "Design and Evaluation of the Internal Space Layout of High-Speed Health Trains Based on Improved Systematic Layout Planning" J 6, no. 3: 361-383. https://doi.org/10.3390/j6030025
APA StyleZhao, Y., Wu, Y., Zhao, M., Xiang, Z., Zhi, J., & Xu, B. (2023). Design and Evaluation of the Internal Space Layout of High-Speed Health Trains Based on Improved Systematic Layout Planning. J, 6(3), 361-383. https://doi.org/10.3390/j6030025