Intersession-Online: A Smartphone Application for Systematic Recording and Controlling of Intersession Experiences in Psychotherapy

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
- Investigating the relationship between in-session and intersession experiences from a psychodynamic perspective [34].
- Development of a smartphone application for economic and systematic assessment of intersession experiences.
- Randomized-control trial to investigate the efficacy of the smartphone application.
Aims
- Economic and systematic ambulatory assessment of intersession experiences.
- Automated evaluation and summary of results for psychotherapists.
- Interventions to promote positive intersession experiences.
3. Results
3.1. Functions
3.1.1. Users
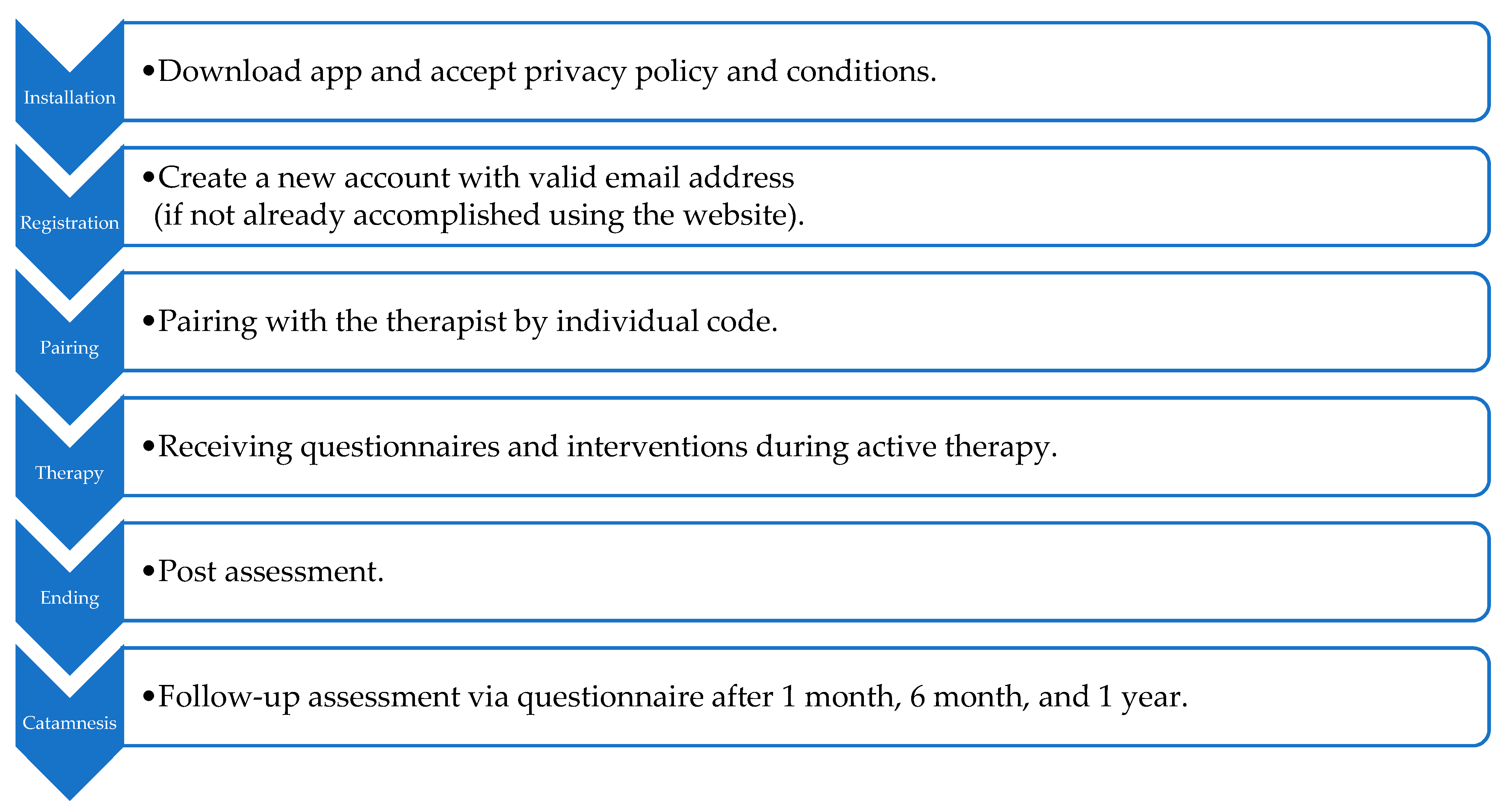
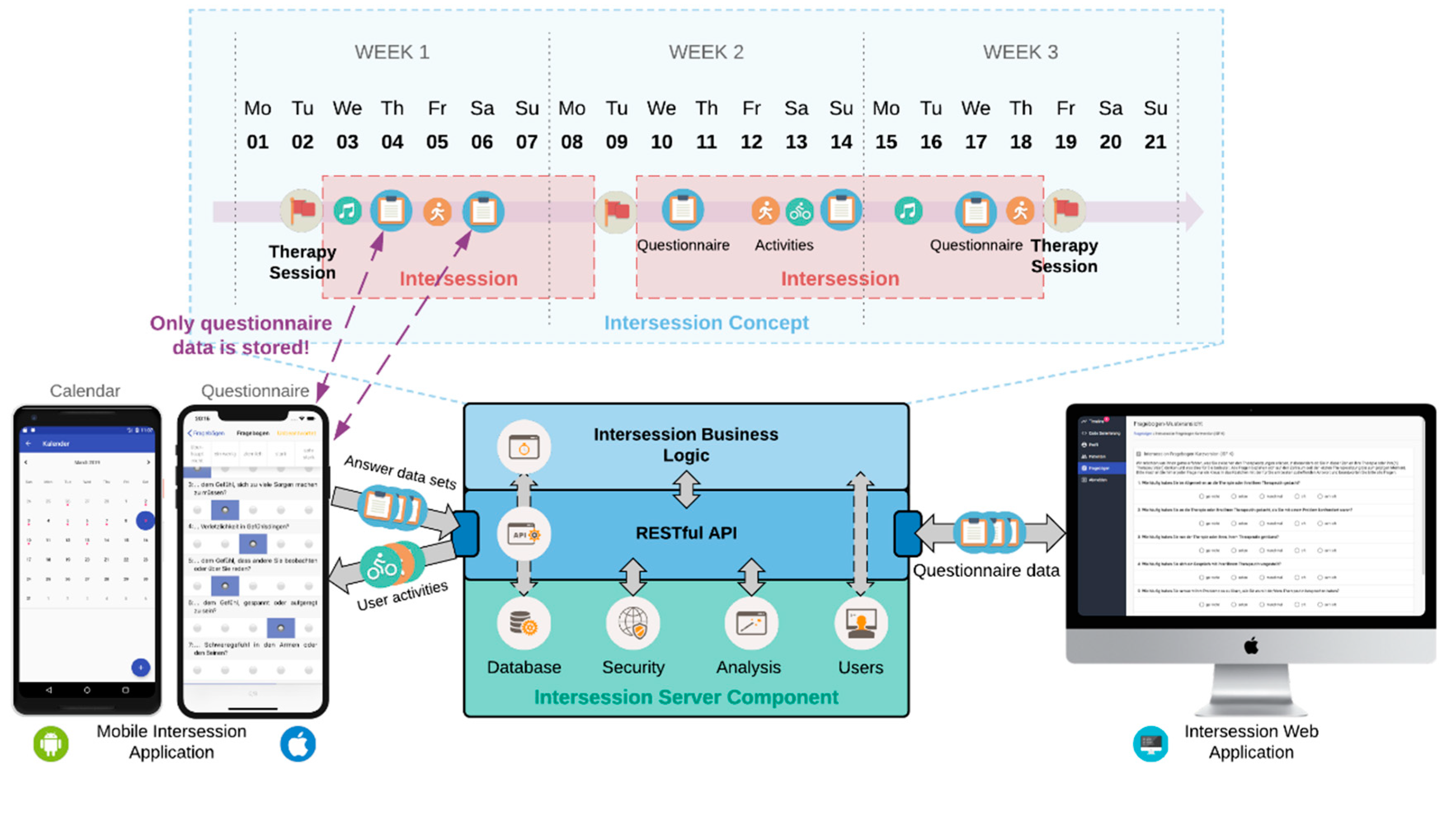
3.1.2. Procedure
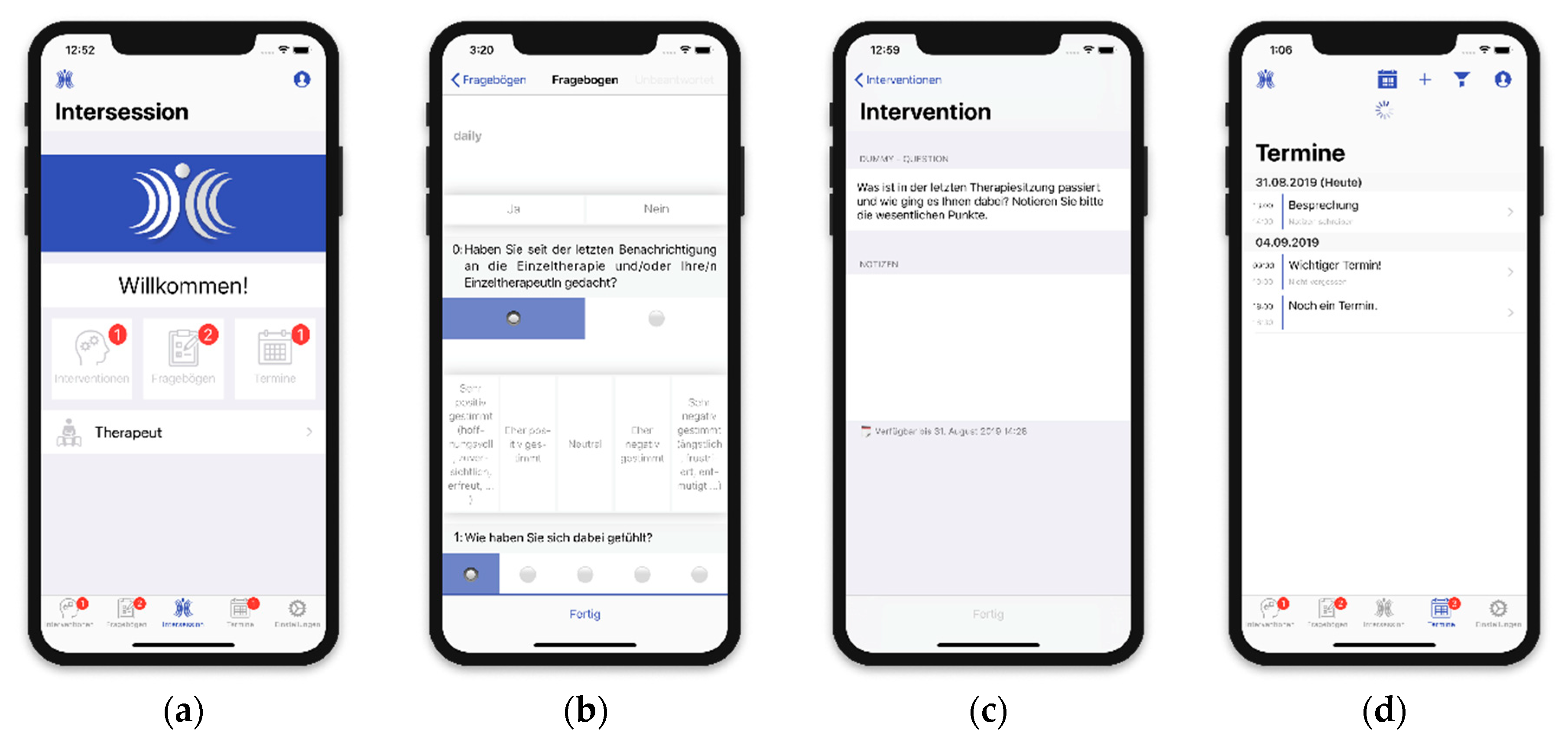
3.1.3. Features
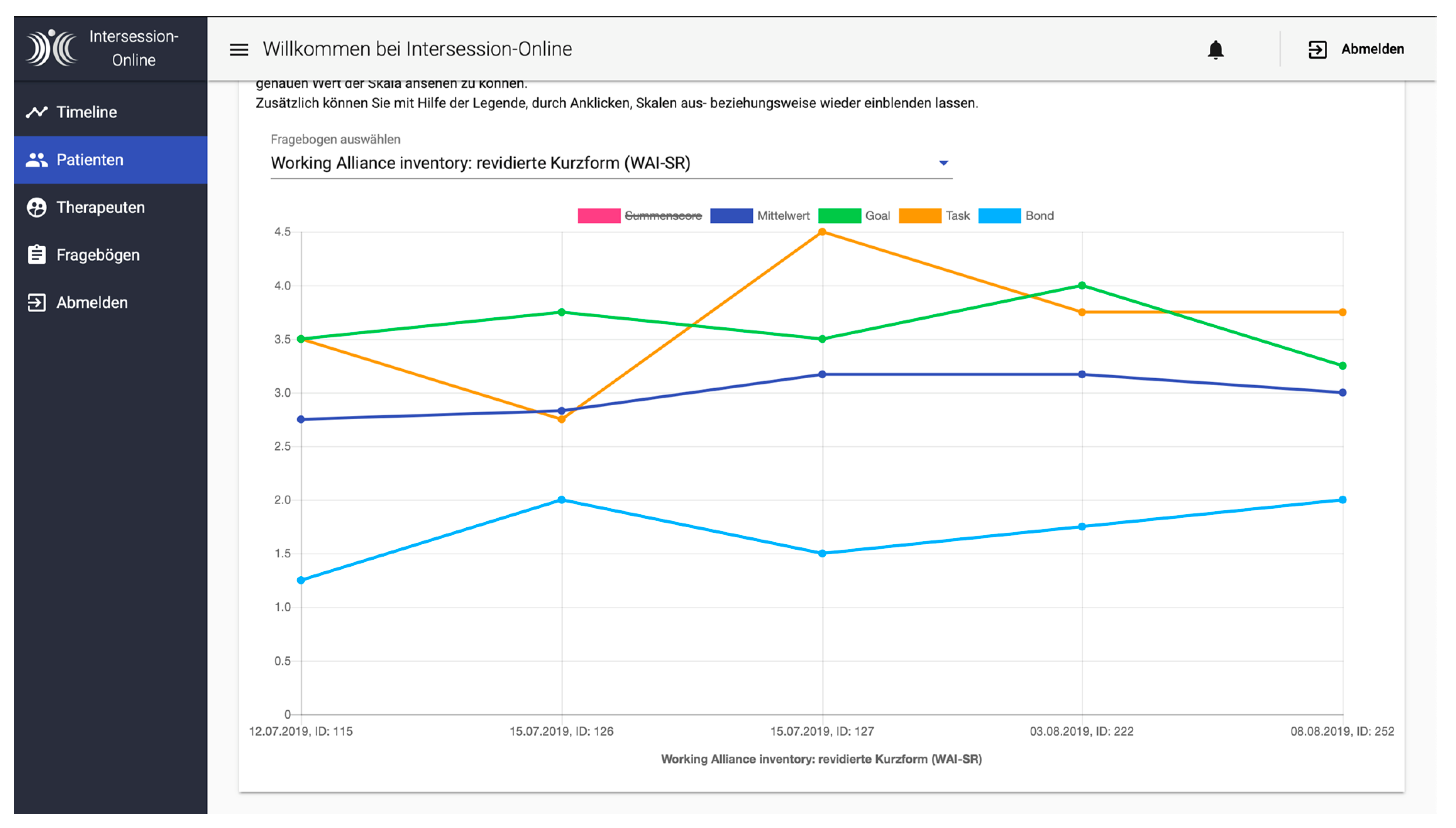
3.1.4. Data Collection/Monitoring
- Pre- and post-treatment assessment at the beginning and end of therapy.
- Daily ambulatory assessment.
- Post-session assessment.
- Weekend assessment.
- Follow-up assessment.
Pre- and Post-Treatment Assessment
Daily Ambulatory Assessment
Post-Session Assessment
Weekend Assessment
3.1.5. Interventions
3.1.6. Introduction and Implementation of Intersession-Online in Psychotherapeutic Practice
3.1.7. Privacy Issues
Privacy Protection on the Phone
Privacy Protection on the Server
Server Requirements
3.1.8. Research with Intersession-Online
4. Limitations
5. Discussion
6. Summary and Outlook
Author Contributions
Funding
Acknowledgments
Ethics Approval
Conflicts of Interest
References
- Lui, J.H.L.; Marcus, D.K.; Barry, C.T. Evidence-based apps? A review of mental health mobile applications in a psychotherapy context. Prof. Psychol. Res. Pract. 2017, 48, 199–210. [Google Scholar] [CrossRef]
- Ruwaard, J.; Kristjansdottir, O.; Donker, T.; Petrie, K.; Proudfoot, J.; Clarke, J.; Birch, M.-R.; Christensen, H. Smartphones for smarter delivery of mental health programs: A systematic review. J. Med Internet Res. 2013, 15, e247. [Google Scholar]
- World Health Organization. MHealth: New Horizons for Health Through Mobile Technologies; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Menon, V.; Rajan, T.M.; Sarkar, S. Psychotherapeutic Applications of Mobile Phone-based Technologies: A Systematic Review of Current Research and Trends. Indian J. Psychol. Med. 2017, 39, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Prentice, J.L.; Dobson, K.S. A review of the risks and benefits associated with mobile phone applications for psychological interventions. Can. Psychol. Can. 2014, 55, 282–290. [Google Scholar] [CrossRef]
- Pryss, R.; Reichert, M.; John, D.; Frank, J.; Schlee, W.; Probst, T. A personalized sensor support tool for the training of mindful walking. In Proceedings of the IEEE 15th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Las Vegas, NV, USA, 4–7 March 2018; pp. 114–117. [Google Scholar]
- Pryss, R.; John, D.; Schlee, W.; Schlotz, W.; Schobel, J.; Kraft, R.; Spiliopoulou, M.; Langguth, B.; Reichert, M.; O’Rourke, T.; et al. Exploring the time trend of stress-levels while using the crowdsensing mHealth platform TrackYourStress and the influence of stress reactivity. JMIR mHealth 2019, 7, e13978. [Google Scholar]
- Bush, N.E.; Armstrong, C.M.; Hoyt, T.V. Smartphone apps for psychological health: A brief state of the science review. Psychol. Serv. 2019, 16, 188–195. [Google Scholar] [CrossRef]
- Last John, M. A Dictionary of Epidemiology, 4th ed.; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]
- Pryss, R.; Probst, T.; Schlee, W.; Schobel, J.; Langguth, B.; Neff, P.; Spiliopoulou, M.; Reichert, M. Prospective crowdsensing versus retrospective ratings of tinnitus variability and tinnitus–stress associations based on the TrackYourTinnitus mobile platform. Int. J. Data Sci. Anal. 2018, 43, 88. [Google Scholar] [CrossRef]
- Orlinsky, D.E.; Geller, J.D.; Tarragona, M.; Farber, B. Patient’s representations of psychotherapy: A new focus for psychodynamic research. J. Consult. Clin. Psychol. 1993, 61, 596–610. [Google Scholar] [CrossRef]
- Orlinsky, D.E.; Geller, J.D. Patient’s Representations of Their Therapists and Therapy: New Measures; Miller, N.E., Ed.; Psychodynamic treatment research. A handbook for clinical practice; BasicBooks: New York, NY, USA, 1993; pp. 423–466. [Google Scholar]
- Hartmann, A.; Orlinsky, D.; Zeeck, A. The structure of intersession experience in psychotherapy and its relation to the therapeutic alliance. J. Clin. Psychol. 2011, 67, 1044–1063. [Google Scholar] [CrossRef]
- Hartmann, A. Therapie Zwischen den Stunden: Explorationen von Intersession-Prozessen [Therapy Between Therapy Sessions: Exploration of Intersession Experiences]; P. Lang: Frankfurt, Germany, 1997. [Google Scholar]
- Orlinsky, D.E. The generic model of psychotherapy after 25 years: Evolution of a research-based metatheory. J. Psychother. Integr. 2009, 19, 319–339. [Google Scholar] [CrossRef]
- Sol, G.L.; Bergin, E.A. (Eds.) Handbook of Psychotherapy and Behavior Change, 3rd ed.; Wiley: New York, NY, USA, 1986. [Google Scholar]
- Stewart, S.; Schröder, T. Emotional homework: A systematic literature review of patients’ intersession experiences. J. Psychother. Integr. 2015, 25, 236–252. [Google Scholar] [CrossRef]
- Tarragona, M.; Orlinsky, D.E. Patient’s experience of therapy between sessions. In Proceedings of the 18th Annual Meeting of the Society for Psychotherapy Research, Ulm, Germany, 16–20 June 1987. [Google Scholar]
- Orlinsky, D.E.; Tarragona, M. Patient’s representations of the therapist and experiences in therapy sessions: Further findings. In Proceedings of the 20th Annual Meeting of the Society for Psychotherapy Research, Toronto, ON, Canada, 21–24 June 1989. [Google Scholar]
- Geller, J.; Farber, B. Factors influencing the process of internalization in psychotherapy. Psychother. Res. 1993, 3, 166–180. [Google Scholar] [CrossRef]
- Andreas, S.; Gablonski, T.-C.; Hiesberger, S.; Senft, B.; Koller, I.; Schulz, H. Intersession-Prozesse in stationärer psychotherapeutischer Behandlung: Ist die Einzel-oder die Gruppentherapie entscheidender für die therapeutische Beziehung und das Therapieergebnis? [Intersession-Processes in inpatient therapy: Are the individual or group therapy important for the therapeutic relationship and the outcome?]. Psychodyn. Psychother. 2016, 15, 206–218. [Google Scholar]
- Knox, S.; Goldberg, J.L.; Woodhouse, S.S.; Hill, C.E. Client’s internal representations of their therapists. J. Couns. Psychol. 1999, 46, 244–256. [Google Scholar] [CrossRef][Green Version]
- Owen, J.; Quirk, K.; Hilsenroth, M.J.; Rodolfa, E. Working through: In-session processes that promote between-session thoughts and activities. J. Couns. Psychol. 2012, 59, 161–167. [Google Scholar] [CrossRef]
- Geller, J.D.; Cooley, R.S.; Hartley, D. Images of psychotherapist: A theoretical and methodological perspective. Imagin. Cogn. Personal. 1981, 1, 123–146. [Google Scholar] [CrossRef]
- Hartmann, A.; Orlinsky, D.; Weber, S.; Sandholz, A.; Zeeck, A. Session and intersession experience related to treatment outcome in bulimia nervosa. Psychother. Theory Res. Pract. Train. 2010, 47, 355–370. [Google Scholar] [CrossRef]
- Zeeck, A.; Hartmann, A. Relating therapeutic process to outcome: Are there predictors for the short-term course in anorexic patients? Eur. Eat. Disord. Rev. 2005, 13, 245–254. [Google Scholar] [CrossRef]
- Bender, D.S.; Farber, B.A.; Sanislow, C.A.; Dyck, I.R.; Geller, J.D.; Skodol, A.E. Representations of therapists by patiens with personality disorder. Am. J. Psychother. 2003, 57, 219–236. [Google Scholar] [CrossRef][Green Version]
- Gablonski, T.-C.; Hiesberger, S.; Senft, B.; Andreas, S. The relationship between intersession processes and level of personality functioning in patients with mental disorders. In Proceedings of the 46th International Annual Meeting of the Society for Psychotherapy Research (SPR), Philadelphia, PA, USA, 24–27 June 2015. [Google Scholar]
- Almut, Z.; Hartmann, A.; Herzog, W.; Wild, B.; deZwaan, M.; Zipfel, S.; Sahin, Z. Outpatient psychotherapy for anorexia nervosa: exploring the Inter-Session-Process in the ANTOP-study. In Proceedings of the 46th International Annual Meeting of the Society for Psychotherapy Research (SPR), Philadelphia, PA, USA, 24–27 June 2015. [Google Scholar]
- Hartmann, A.; Almut, Z.; Herzog, W.; Wild, B.; deZwaan, M.; Zipfel, S.; Sahin, Z. The inter-session-process in psychodynamic and cognitive-behavioral psychotherapy for anorexia nervosa and its relation to outcome. In Proceedings of the 46th International Annual Meeting of the Society for Psychotherapy Research (SPR), Philadelphia, PA, USA, 24–27 June 2015. [Google Scholar]
- Pomnitz Fabiane, B.; Schattenburg, S.L.; Wünsch-Leiteritz, W.; Leiteritz, A.; Schreiber-Willnow, K.; Dobersch, J.; Moffenter, J.; Nickel, R.; Huber, T.; Braks, K. Was erleben Patienten in stationärer Psychotherapie zwischen den Gruppentherapie-Sitzungen? Eine Erprobung des Inter-Session-Fragebogens in der Klinik. Psychother. Psych. Med. 2016, 66, 21–30. [Google Scholar] [CrossRef]
- Orlinsky, D.E.; Tarragona, M. Intersession Experience Questionnaire (Patient Form); University of Chicago Committee on Human Development: Chicago, IL, USA, 1986. [Google Scholar]
- Hartmann, A.; Orlinsky, D.E.; Geller, J.D.; Zeeck, A. Der Inter-Session-Fragebogen (ISF) [The Intersession Experience Questionnaire]. Psychother. Psych. Med. 2003, 53, T67–T75. [Google Scholar]
- Gablonski, T.-C.; Kadur, J.; Lüdemann, J.; Wirth, L.; Lutz, G.; Andreas, S. Intersession experiences and its association with in-session-processes and outcome. In Proceedings of the 50th International Annual Meeting of the Society for Psychotherapy Research (SPR), Buenos Aires, Argentina, 3–6 July 2019. [Google Scholar]
- Fabian, W.; Munder, T.; Leonhart, R.; Herzog, T.; Plassmann, R.; Barth, J.; Wolfgang Linster, H. Die deutschsprachige Version des Working Alliance Inventory-short revised (WAI-SR)-Ein schulenübergreifendes, ökonomisches und empirisch validiertes Instrument zur Erfassung der therapeutischen Allianz. Klin. Diagn. Eval. 2008, 1, 343–358. [Google Scholar]
- Huber, J. Conception and Realization of a REST-based Application Programming Interface for Intersession-Management in Psychology. Bachelor’s Thesis, Ulm University, Ulm, Germany, 2019. [Google Scholar]
- Pryss, R.; Schobel, J.; Reichert, M. Requirements for a flexible and generic API enabling mobile crowdsensing mhealth applications. In Proceedings of the 4th International Workshop on Requirements Engineering for Self-Adaptive, Collaborative, and Cyber Physical Systems (RESACS), Bannf, AB, Canada, 20 August 2018; pp. 24–31. [Google Scholar]
- Almut, Z.; Hartmann, A.; Orlinsky, D.E. Inter-Session-Prozesse: Ein vernachlässigtes Thema der Psychotherapieforschung. Psychother. Psych. Med. 2004, 54, 236–242. [Google Scholar]
- Klinitzke, G.; Romppel, M.; Häuser, W.; Brähler, E.; Glaesmer, H. Die deutsche Version des Childhood Trauma Questionnaire (CTQ)-psychometrische Eigenschaften in einer bevölkerungsrepräsentativen Stichprobe. Psychother. Psychosom. Med. Psychol. 2012, 62, 47–51. [Google Scholar] [CrossRef]
- Sammet, I.; Leichsenring, F.; Schauenburg, H.; Andreas, S. Self-ratings of pathogenic beliefs: A study based on the psychodynamic control-mastery theory. Psychotherapy research. J. Soc. Psychother. Res. 2007, 17, 494–503. [Google Scholar] [CrossRef]
- Hausberg, M.C.; Schulz, H.; Piegler, T.; Happach, C.G.; Klöpper, M.; Brütt, A.L.; Sammet, I.; Andreas, S. Is a self-rated instrument appropriate to assess mentalization in patients with mental disorders? Development and first validation of the mentalization questionnaire (MZQ). Psychotherapy Research. 2012, 22, 699–709. [Google Scholar]
- Fonagy, P.; Gergely, G.; Jurist, E.L.; Target, M. Affect Regulation, Mentalization, and the Development of the Self; Other Press: New York, NY, USA, 2002. [Google Scholar]
- Bateman, A.; Fonagy, P. (Eds.) Handbook of Mentalizing in Mental Health Practice; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2012. [Google Scholar]
- Bartholomew, K.; Horowitz, L.M. Attachment styles among young adults: A test of a four-category model. J. Pers. Soc. Psychol. 1991, 61, 226–244. [Google Scholar] [CrossRef]
- Dammann, G.; Smole, S.; Kraus, C.; Buchheim, P. IPO-2001: Inventory of Personality Organization; Psychosomatische Poliklinik: Munich, Germany, 2002. [Google Scholar]
- Kerber, A.; Schultze, M.; Knaevelsrud, C.; Wright, A.G.C.; Spitzer, C.; Zimmermann, J. Persönlichkeitsinventar für DSM-5 und ICD-11—Kurzform (PID5BF+); American Psychiatric Association: Philadelphia, PA, USA, 2019. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. DSM-5; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. ICD-11-MMS: International Classification of Diseases for Mortality and Morbidity Statistics; W.H.O.: Geneva, Switzerland, 2019. [Google Scholar]
- Rabung, S.; Harfst, T.; Koch, U.; Schulz, H. Hamburger Module zur Erfassung allgemeiner Aspekte psychosozialer Gesundheit für die therapeutische Praxis (Health-49); Universitätsklinikum Hamburg Eppendorf: Hamburg, Germany, 2007. [Google Scholar]
- Klaghofer, R.; Brähler, E. Konstruktion und teststatistische Prüfung einer Kurzform der SCL-90-R. Zeitschrift für Klinische Psychologie. Psychiatr. Psychother. 2001, 49, 115–124. [Google Scholar]
- Wolf, M.; Kraft, S.; Tschauner, K.; Bauer, S.; Becker, T.; Puschner, B. User activity in a mobile phone intervention to assist mindfulness exercises in people with depressive symptoms. Ment. Health Prev. 2016, 4, 57–62. [Google Scholar] [CrossRef]
- Pryss, R.; Schlee, W.; Hoppenstedt, B.; Reichert, M.; Spiliopoulou, M.; Langguth, B.; Probst, T. Applying Machine Learning on the Daily Life Data of the TrackYourTinnitus mHealth Crowdsensing Platform Predicts the Mobile Operating System with High Accuracy. JMIR 2019. preprints. [Google Scholar]
- Schickler, M.; Pryss, R.; Schlee, W.; Probst, T.; Langguth, B.; Schobel, J.; Reichert, M. Usability Study on Mobile Processes Enabling Remote Therapeutic Interventions. In Proceedings of the IEEE 31st International Symposium on Computer-Based Medical Systems (CBMS), Karlstad, Sweden, 18–21 June 2018; pp. 146–151. [Google Scholar]
- Schickler, M.; Pryss, R.; Schobel, J.; Reichert, M. Supporting Remote Therapeutic Interventions with Mobile Processes. In Proceedings of the IEEE International Conference on AI & Mobile Services (AIMS), Honolulu, HI, USA, 25–30 June 2017; pp. 30–37. [Google Scholar]
- Schickler, M.; Pryss, R.; Stach, M.; Schobel, J.; Schlee, W.; Probst, T.; Reichert, M. An IT Platform Enabling Remote Therapeutic Interventions. In Proceedings of the IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS), Thessaloniki, Greece, 22–24 June 2017; pp. 111–116. [Google Scholar]
- Nocross, J.C.; Lambert, M.J. Evidence-based therapy relationships. In Psychotherapy Relationships That Work. Evidence-Based Responsiveness; Norcross, J.C., Ed.; Oxford University Press: New York, NY, USA, 2011; pp. 3–21. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intersession Experience Questionnaire (IEQ) | |
|---|---|
| Factors | Item Example |
| A1: Intensity | Since your last session, how much have you thought about what is happening in your therapy |
| B1: Problem-solving context | Since your last session, how much did you find yourself thinking about your therapy or therapist while feeling bad about something? |
| B2: Dreaming-drowsy context | Since your last session, how much did you find yourself thinking about your therapy or therapist while daydreaming? |
| C1: Recreating dialogue | Since your last session, how often did you find yourself imagining a conversation with your therapist? |
| C2: Applying | Since your last session, how often did you find yourself doing something your therapist had suggested? |
| C3: Relationship fantasies | Since your last session, how often did you find yourself thinking about your relationship to your therapist? |
| D1: Positive emotions | Thinking about therapy or my therapist made me feel hopeful. |
| D2: Negative Emotions | Thinking about therapy or my therapist made me feel anxious. |
| E1: Significant others, sharing intersession experiences | Since your last session, did you talk about your therapy or therapist with a family member? |
| Function | Details | Platform | User |
|---|---|---|---|
| Manage account | Create Account | Website/Apps | All |
| E-Mail Validation | Website/Apps | All | |
| Login / Logout | Website/Apps | All | |
| Password Reset | Website/Apps | All | |
| Profile View/Change | Website/Apps | All | |
| Pairing | Generate Code | Website | Researcher/Therapist |
| Enter Code | Apps | Patient | |
| Questionnaires | Send Out | Website | Researcher/Therapist |
| Receive and answer | Apps | Patient | |
| Results | Website | Researcher/Therapist | |
| Data Export | Website | Researcher | |
| Interventions | Send Out | Website | Researcher/Therapist |
| Receive and work through | Apps | Patient | |
| Calendar | Managing Appointments | Apps | Patient |
| Notifications | Notifications | Apps | Patient |
| Timeline | Overview of Activities | Website | Researcher / Therapist |
| Settings | Notification Settings | Apps | Patients |
| Profile Settings | Website/Apps | All | |
| Data Privacy Statement | Apps | Patients | |
| Data Privacy | Apps | Patients | |
| General Information | Apps | Patients | |
| Imprint and Contact | Apps | Patients |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gablonski, T.-C.; Pryss, R.; Probst, T.; Vogel, C.; Andreas, S. Intersession-Online: A Smartphone Application for Systematic Recording and Controlling of Intersession Experiences in Psychotherapy. J 2019, 2, 480-495. https://doi.org/10.3390/j2040031
Gablonski T-C, Pryss R, Probst T, Vogel C, Andreas S. Intersession-Online: A Smartphone Application for Systematic Recording and Controlling of Intersession Experiences in Psychotherapy. J. 2019; 2(4):480-495. https://doi.org/10.3390/j2040031
Chicago/Turabian StyleGablonski, Thorsten-Christian, Rüdiger Pryss, Thomas Probst, Carsten Vogel, and Sylke Andreas. 2019. "Intersession-Online: A Smartphone Application for Systematic Recording and Controlling of Intersession Experiences in Psychotherapy" J 2, no. 4: 480-495. https://doi.org/10.3390/j2040031
APA StyleGablonski, T.-C., Pryss, R., Probst, T., Vogel, C., & Andreas, S. (2019). Intersession-Online: A Smartphone Application for Systematic Recording and Controlling of Intersession Experiences in Psychotherapy. J, 2(4), 480-495. https://doi.org/10.3390/j2040031