Abstract
Mobile health technologies have become more and more important in psychotherapy research and practice. The market is being flooded by several psychotherapeutic online services for different purposes. However, mobile health technologies are particularly suitable for data collection and monitoring, as data can be recorded economically in real time. Currently, there is no appropriate method to assess intersession experiences systematically in psychotherapeutic practice. The aim of our project was the development of a smartphone application framework for systematic recording and controlling of intersession experiences. Intersession-Online, an iOS- and Android-App, offers the possibility to collect data on intersession experiences easily, to provide the results to therapists in an evaluated form and, if necessary, to induce or interrupt intersession experiences with the primary aim to improve outcome of psychotherapy. In general, the smartphone application could be a helpful, evidence-based tool for research and practice. Overall speaking, further research to investigate the efficacy of Intersession-Online is necessary.
1. Introduction
Over the last decade, mobile health technologies have become more and more important in medicine and especially in psychotherapy [1] and have been termed as mobile health or short mHealth [2]. mHealth, as defined by the World Health Organization [3], is “[…] medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants (PDAs), and other wireless devices.” mHealth creates the possibility to offer support and interventions in real time [4] and implicates several benefits—both for the patient and the therapist [5]. Advantages of mHealth are among others: overcome barriers associated with waiting-time, mobility, or costs. Furthermore, the use of mHealth is connected to less stigma and more privacy and can be used every time and everywhere like in stressful situations as a therapist in the pocket [6,7]. It is also an easy way for the patient to communicate with the therapist and can be used for patient monitoring and to give access to relevant information for the psychotherapeutic process (i.e., psychoeducation). In a systematic review, Lui et al. (2017) [1] showed that most of the evidence-based apps for psychotherapy are designed as a therapeutic alternative to face-to-face therapy. Main features are symptom monitoring, therapeutic skills, self-management [1], and data collection [8]. Mobile devices can be used for the ambulatory assessment of self-reported data (i.e., symptom distress), performance data (i.e., cognitive skills), phone-based senor data (i.e., physical activity), and wearable sensor data (i.e., sleep behavior) [8]. This form of data collection is particularly suitable where traditional questionnaire surveys reach their limits due to different forms of bias. One of these is the so-called recall bias—an error in answer accuracy regarding experiences from the past [9]. By using mobile devices for ambulatory assessment, it is possible to collect data in real time without a recall bias [10]. This is a huge advantage for data assessment, especially for collecting data between sessions of psychotherapy. These processes are called intersession experiences [11,12] of psychotherapy.
“Intersession experiences” (ISE) or “intersession processes” describe the processing and internalization of therapy and their contents between therapy sessions [12] and include all spontaneous and intentional thoughts, feelings, memories, and fantasies about the therapy and the therapist [13]. According to Orlinsky and Geller [11,12], the theoretical concept of intersession experiences can be explained with different psychoanalytic and developmental psychological theories, especially theories that are dealing with the concept of internalization and representation. Orlinsky and Geller describe representation as “[…] all forms of cognitive or ideational experience other than immediate sensory data and innate response patterns. The concept of representation encompasses memories and expectations, habits and skills, images and fantasies, thoughts and symbols. Representations may be concrete or abstract, realistic or unrealistic, and may refer to things past, present, or future. They may also vary in both their degree of energy and their emotional valence” [12], p. 425. According to Orlinsky and colleagues [11], internalization, on the other hand, includes: “[…] all the processes whereby individuals transform current felt perceptions into emotionally charged schemata and elaborate them into organized elements of personality” [11], p. 497. They describe intersession experiences as the internalized representations of therapy and therapists which can have a significant impact on the therapeutic process and outcome. In [14], one can find a suggestion for the integration of intersession experiences in the generic model of psychotherapy [15,16], a comprehensive transtheoretical model that integrates different results of psychotherapy research.
The concept of intersession experiences has been hardly investigated in the field of psychotherapy research since most psychotherapy studies are focusing on processes within the therapy session (intra-session experiences such as the therapeutic alliance). However, the amount of time that a patient is in the face-to-face setting is rather small in comparison to the rest of lifetime. This leads to the assumption that this kind of between-session processes are directly related to relevant psychotherapy concepts and outcome. Nevertheless, since the conceptualization, there have been only a few studies on intersession experiences [17]. Previous studies, in turn, have shown that most patients in psychotherapy are thinking about the therapy or the therapist between the sessions [18,19], especially right before or after a session, or in stressful situations, respectively [20]. Furthermore, previous research indicates a high correlation between intersession experiences and therapeutic alliance [13,21,22,23] as well as between intersession experiences and outcome [20,21,24,25,26]. A study with patients with bulimia nervosa showed that intersession experiences were a better predictor for outcome than, for example, the global therapeutic alliance [22]. Studies have found disorder-specific differences (i.e., patients with anxiety disorder vs. patient with personality disorder) in intersession experiences of patients [27,28,29] as well as differences between different therapy settings (i.e., individual therapy vs. group therapy) [21,30,31]. Hartmann and colleagues [30] showed that patients from cognitive-behavioral psychotherapy (CBT) had higher intersession experiences at the beginning of therapy in comparison to patients from a psychodynamic psychotherapy. The reason for that are homework assignments, a characteristic of CBT. It is possible that the homework assignments promote intersession experiences. Nevertheless, intersession experiences have been studied and found in all different forms of psychotherapy like, for example, CBT, psychodynamic psychotherapy, or psychoanalytic psychotherapy and could be seen as a common factor of psychotherapy. An overview of previous intersession research can be found in Stewart and Schröder (2015) [17]. In summary, previous results lead to the conclusion that intersession experiences are very specific and individual processes have an important impact on the psychotherapeutic process and outcome.
However, hitherto, intersession experiences are not systematically assessed in psychotherapeutic practice, which could be associated with the current methodological approach. In particular, the gold standard for the assessment of intersession experiences is the Intersession Experience Questionnaire (IEQ) [32,33]. The IEQ is a self-report questionnaire with 52-items and records (a) intensity of intersession experiences; (b) context of intersession experiences; (c) content of intersession experiences; (d) emotional quality of intersession experiences; and (e) significant others, sharing intersession experiences (see Table 1). Patients are asked to fill out the questionnaire immediately before a psychotherapy session and the questions are related to the period between the last session and the current point of time. However, in practice, therapists have not enough time resources to deliver and evaluate the questionnaire of the patients and to use the systematic information about their intersession experiences for the psychotherapeutic process. Furthermore, in psychotherapy with weekly sessions, the questions of the questionnaire refer to a time period of seven days and thus to a higher risk of recall bias.

Table 1.
The Intersession Experiences Questionnaire [33] with five scales and nine factors.
In order to remedy the aforementioned drawbacks, we have worked on a digital solution to support psychotherapists in their day-to-day practice. In the following, we are presenting a new smartphone application for iOS and Android smartphones for the economic and systematic assessment of intersession experiences.
2. Materials and Methods
The development of the smartphone application is part of an intersession project from the University of Klagenfurt, funded by the Österreichische Nationalbank (OeNB), grant number: 17485. The project started in June 2017 and consists of three overall partial studies:
- Investigating the relationship between in-session and intersession experiences from a psychodynamic perspective [34].
- Development of a smartphone application for economic and systematic assessment of intersession experiences.
- Randomized-control trial to investigate the efficacy of the smartphone application.
The Ethics Committee of Carinthia (Austria) has approved this study with all partial studies. Thus, the approval comprises preliminary studies, the development of the smartphone application framework, as well as the final randomized-controlled trial. The study is registered with the number A 01/16. Written informed consent to participate was/will be obtained from all participants.
In this paper, we are focusing on the second part of the study—the development of the smartphone application.
Aims
Currently, there is no appropriate method to assess intersession experiences systematically in psychotherapeutic practice. Thus, the primary aim of Study 2 was the development of a practical option for the systematic assessment of intersession experiences. A priori, we have defined the central features of the smartphone application:
- Economic and systematic ambulatory assessment of intersession experiences.
- Automated evaluation and summary of results for psychotherapists.
- Interventions to promote positive intersession experiences.
For this purpose, we have developed native iOS- and Android smartphone applications as well as a web application for the administration and overview of results for psychotherapists and researchers, which is denoted as “Intersession-Online”. Intersession-Online is available on App Store and Google Play Store.
3. Results
The kick-off meeting for the development of Intersession-Online was held in May 2018 with the cooperation partner at the Institute of Databases and Information Systems (DBIS, University of Ulm) in Ulm (Germany). The team consists of psychotherapy researchers and well-experienced programmers in the field of mHealth. First, the user requirements specification was discussed. Based on the requirements, the programmers started to develop the framework, consisting of (a) a RESTful application programming interface (API), (b) a web application, (c) a relational database, (d) native iOS-, and (e) Android applications. Regular meetings were held to clarify open questions and to discuss problems as well as to accompany the process. Note that it was also initially decided to implement the framework in a way that the mobile applications are able to provide the entire feature set when the used smartphones are in offline mode.
3.1. Functions
3.1.1. Users
Intersession-Online provides three different user types: “Researcher”, “Therapist”, and “Patient”. (1) Researchers can activate registered therapist accounts and have access to data of those patients who have allowed data access for research purposes (please see, for more information, “Data collection”). They act as administrators and can adjust settings (i.e., an account management is provided). In addition, a data export feature was implemented for researchers. (2) Therapists can create an account on the website www.intersession-online.de. After successful account activation by the researcher, therapists can generate a pairing code to match with their patients. If allowed by the patient, they have data access and can check for different results. The results, in turn, are graphically presented (i.e., intersession experiences, symptom burden, therapeutic alliance). Furthermore, they can check received interventions of their patients and whether they have accomplished them. Researchers and therapists work on the website, while the application is intended to be used exclusively by patients. (3) Patients can download the app in the App Store or Google Play Store and create a new account. After successful registration, including an e-mail validation, the app can be used with limited functionality. As soon as they are paired with the therapist, all functions are activated, and the patients can receive questionnaires and interventions.
3.1.2. Procedure
First of all, patients need to download the smartphone application Intersession-Online in the Apple App Store or Google Play Store and must create a new account. For this purpose, the privacy policy must be accepted, an unregistered, valid e-mail address specified, and a password set. During this step, patients are asked for permission to data access for researchers. This permission can be transparently withdrawn and granted again at any time. In a second step, the patient gets a validation email and needs to confirm the provided email address. After a successful validation, the patient will be automatically forwarded to the login screen and can enter the app with the validated account information. After the registration, the patient can start the pairing process. For this, an individual patient code that was personally received from the therapist is necessary. If the patient does not yet have the code, he/she can skip this step and accomplish it later on. A complete activation of all functions is only possible after a successful pairing process with the therapist was accomplished. This is a safety precaution to ensure that the patients are in psychotherapeutic treatment and that they use the app only under professional supervision. The app is not intended to replace a therapy and should only be used in addition to it. After successful pairing, patients get the baseline questionnaires (please see “Data”), which are available for seven days. Subsequently, patients need to add their therapy appointments to receive questionnaires and interventions in accordance with their therapy procedure and duration. After finishing the therapy, patients will receive questionnaires for follow-up observations after 1 month, 6 months, and 1 year (see also Figure 1).
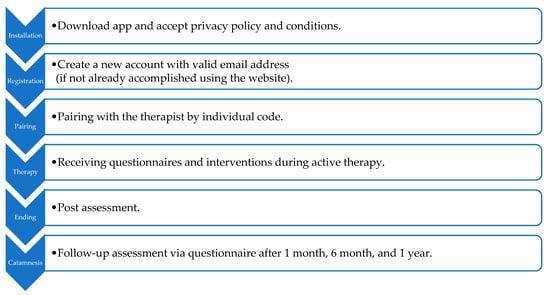
Figure 1.
General procedure of Intersession-Online from installing to finishing.
3.1.3. Features
Intersession-Online offers three platforms within the implemented framework: (1) a web application (i.e., the website), (2) a native iOS-, and (3) a native Android application. The website (see Figure 2) contains all relevant information for researchers and therapists. For researchers and therapists, the start screen shows a time line with all current activities of paired patients (i.e., new patients, new contributions, etc.). The menu navigation directs to the profiles of paired patients as well as their results if access has been allowed. In the profile, the therapist can terminate the therapy; i.e., the termination includes the stop of sending push notifications to the smartphone of the patient. Furthermore, it is possible to edit the personal profile (i.e., therapist contact data, relevant information) and to generate new pairing codes. An overview shows all active pairing codes. The menu item “Questionnaires” displays all available questionnaires and their items. This allows therapists to take a closer look at applied questionnaires.
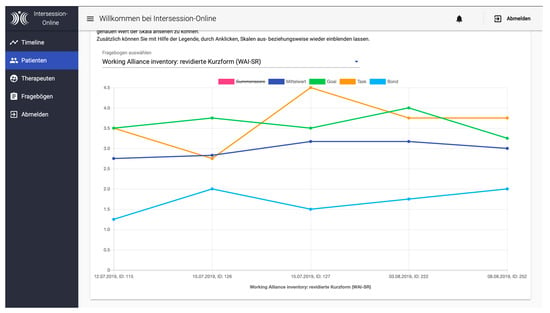
Figure 2.
An example of an evaluated Working-Alliance-Inventory (WAI) [35] for the therapist.
From the start screen of the applications, patients can navigate to open questionnaires and interventions (see Figure 3). Furthermore, they can enter and edit therapy appointments in the calendar and visit the therapist profile. An important menu is the settings section, in which patients can edit their own profile, switching push notifications to on or off, and decide if the therapist and/or researcher can see their data. Almost all features of the mobile applications are available, even without an active internet connection. Data sets are synchronized with the server component as soon as the connection is reestablished. Finally, Table 2 shows an overview of all relevant functions.
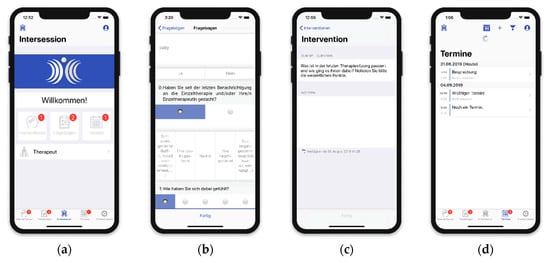
Figure 3.
Screenshots of the iOS-version of Intersession-Online: (a) shows the home screen indicating open interventions, questionnaires, and appointments; (b) is the daily intersession-assessment with two questions; (c) is an example for an intervention with the opportunity to make private notes, which are solely saved on the mobile phone; and (d) shows an overview of appointments with personal notes.
Table 2.
Overview of functions of Intersession-Online.
Finally, Figure 4 summarizes the technical setting of the implemented framework.
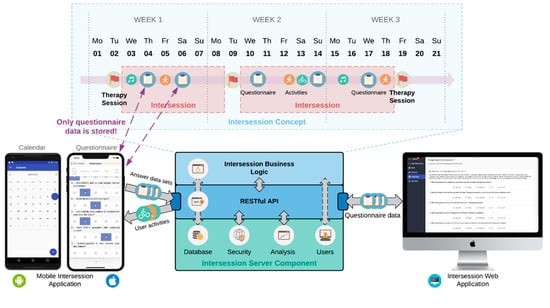
Figure 4.
Intersession-Online technical framework at a glance.
Based on the components shown in Figure 4, we shortly summarize the development of the app and the entire framework. Essentially, the framework encompasses three fundamental technical pillars. First, as already mentioned, two native mobile applications were developed. Specifically, an Android app was developed with Android Studio and using Java as the programming language. Due to the lack of space, the used external libraries were omitted. Then, to complement the mobile side, an iOS mobile application was developed using Xcode and Swift. Again, the libraries that were used beyond the native functions of the mobile operating system were omitted, however, for both apps, they can be obtained in the settings sections of the apps. Second, the two mobile apps communicate with a RESTful-API (i.e., the API follows the REST architecture style) that was particularly developed for the intersession project, for more information see [36]. The API follows guidelines that we presented in [37]. As a particular function of the API, it enables the mobile apps to operate completely in offline mode. This includes the provision of notifications that were applied on the smart mobile devices. Therefore, the locally provided native notification functions provided by the mobile operating systems are utilized. As the drawbacks of this approach are only of minor importance, the local notification system could be powerfully utilized for this project, for more information see [10]. Third, a web application based on Angular was developed, which offers numerous features for the therapist and the patients as well. The web application was developed in tight collaboration with the psychological experts to meet the requirements for the analyzation of the data (e.g., anonymized download of results for statistical evaluation purposes, visualization of data over time, etc.). Also, the mobile apps were developed in tight collaboration with the psychologists. Therefore, an agile development approach was followed by working in sprints, in accordance with the scrum development paradigm.
3.1.4. Data Collection/Monitoring
One of the primary goals of Intersession-Online is collecting data on intersession experiences of patients in an economic and systematic way, as well as to provide the evaluated information in a clear manner to therapists. For this purpose, Intersession-Online uses different questionnaires at different timepoints. In general, there are five different assessment timepoints:
- Pre- and post-treatment assessment at the beginning and end of therapy.
- Daily ambulatory assessment.
- Post-session assessment.
- Weekend assessment.
- Follow-up assessment.
Pre- and Post-Treatment Assessment
The first assessment is carried out after successful pairing with the therapist—the baseline assessment. According to [38], Intersession experiences are affected by the patients’ basic personality structure, which is essentially shaped in early relationship experiences, the current in-session process between patient and therapist, as well as the intensity of the therapeutic process and the patients’ emotional involvement. Based on this, we have decided to use the following instruments for the assessment of potential moderator- and mediator-variables. The baseline and post assessment comprise a standard set of psychodynamic questionnaires:
Childhood Trauma Questionnaire (CTQ) [39]: The CTQ is a self-report questionnaire for the assessment of abuse and neglect with 28 items. It differentiates between five types of maltreatment.
List of pathogenic beliefs (LPB) [40]: The LPB deals with maladaptive expectations (pathogenic beliefs) of patients and comprise of 23 items.
Mentalization Questionnaire (MZQ) [41]: The MZQ is the first published self-report questionnaire for the assessment of mentalizing. Mentalizing is the ability to understand own and other behavior in terms of mental states [42]. Meanwhile, mentalizing is associated with the development and maintenance of several mental disorders [43].
Relationship Questionnaire (RQ) [44]: The RQ is a simple 4-item screening questionnaire to assess attachment. The attachment theory postulates different attachment styles with healthier and less healthier types of attachment.
Inventory of Personality Organization (IPO-2001) [45]: The IPO-2001 is a self-report measure with 83 items that examines specific personality traits of a person.
Personality Inventory for DSM-5 and ICD-11 (PID-5-BF+) [46]: The PID-5-BF+ is a questionnaire for the assessment of six personality domains based on DSM-5 [47] and ICD-11 [48].
Health-49 [49]: The Health-49 questionnaires allows the assessment of different aspects of psychosocial health with overall 49 items.
The baseline assessment is available within the first seven days after pairing. The post-treatment assessment is sent out as soon as the therapy is completed and is also available for seven days.
Daily Ambulatory Assessment
Furthermore, patients get every day three push notifications on a random basis that are accompanied with a questionnaire including one or two questions (please see Figure 3b). The questions are sent out randomly between 08:00 am to 12:00 am, 12:00 am to 04:00 pm, and 04:00 pm to 08:00 pm. The first question of Intersession-Online asks whether the patient had intersession experiences since the last push notification. If the patient answers with “yes”, a second question is triggered asking about the emotional quality of intersession experiences on a five-point Likert scale. This form of ambulatory assessment allows to get a full picture of intersession experiences in real time without any bias and may leverage intersession research as well as psychotherapeutic practice.
Post-Session Assessment
Intersession-Online also provides a calendar feature. Patients can add their appointments with the therapist into the app, which is a central feature of the app. Two hours after finishing a session, patients are asked to fill out two short questionnaires. First, the short version of the Symptom-Checklist with overall 9 items (SCL-K9) [50] has to be filled out. It is a questionnaire to assess psychopathology and distress. Furthermore, patients get the Working Alliance Inventory short revised [35], a questionnaire for the assessment of therapeutic alliance. This post-session assessment is primarily intended as a result indicator of the last session.
Weekend Assessment
Since the responses in the SCL-K9 can be affected by the last session, Intersession-Online is once again randomly asked during the weekend, between Friday 06:00 pm and Sunday 06:00 pm, about the psychopathology and distress with the use of the SCL-K9. In addition, patients are asked to fill out a short version of the Intersession Experience Questionnaire—the IEQ short. The IEQ consists of those eight items from the long version with the highest factor loadings on each factor.
In summary, Intersession-Online has a pre- and posttreatment assessment, three daily measures on intersession experiences each time with one or two questions (based on the answer in the first question), a post-session assessment on distress and therapeutic alliance, and a final weekend assessment asking about symptom distress and intersession experiences.
3.1.5. Interventions
Another major aim of Intersession-Online is to promote positive intersession experiences. This is to be achieved by different interventions based on an algorithm that checks the combination of intensity and quality of intersession experiences and symptom distress. The algorithm uses the scores from the weekend assessment and classifies the symptom distress in three categories: low, medium, and high symptom distress. Intersession experiences are categorized in seven different categories: low intersession experiences, medium intersession experiences primarily negative, medium intersession experiences primarily positive, medium intersession experiences neutral, high intersession experiences primarily negative, high intersession experiences primarily positive, and high intersession experiences neutral. This categorization leads to a 7 × 3 matrix with 21 interventions. Interventions were generated based on the first part of the study of the intersession project. In this study [31], we have investigated successful and unsuccessful therapies and patient-therapist dyads and tried to identify helpful interventions.
Intersession-Online is equipped with different interventions, which are divided into commendations, questions, and tasks. For example: The combination between high symptom distress and low intersession experiences triggers a question to promote intersession experiences: “What happened in the last therapy session and how did you feel? Please note down the essential points and consider discussing them with your therapist.” Here, an answer field is presented, however, the entries are just saved locally on the phone and not transferred to the server. Another example could be a patient with high symptom distress and high level of intersession experiences with mainly negative emotions. In some circumstances, this could be a depressive patient with a high level of rumination. In this case, it would be important to interrupt the negative intersession process and the patient would get a mindfulness exercise. Another task could be to take a break and do something the patient likes to do (i.e., to watch a favorite movie). An example for a comment would be presented in the case of low symptom distress and positive intersession experiences: “You are on the right track – keep it up!”
We see the greatest need for action in the case of at least medium or high symptom distress. Here, patients get mainly questions and tasks to promote positive intersession experiences and to start to reflect on the therapeutic process. Interventions are randomly sent out between the weekend assessment and the first psychotherapy appointment in the next week.
3.1.6. Introduction and Implementation of Intersession-Online in Psychotherapeutic Practice
The acceptance of Intersession-Online depends on different factors. Above all, the compliance of therapists and patients is crucial. In order to increase the compliance, Intersession-Online includes different approaches. First of all, the website provides general information on intersession experiences and their relevance to the psychotherapeutic process. This information is for all therapists and patients or interested parties who are unfamiliar with the concept of intersession experiences. If a therapist is interested in using Intersession-Online, a one-time 30-min personal conversation or phone call provided by a researcher will take place to introduce Intersession-Online. This introduction includes, again, general information on the concept of intersession experiences, the rational, as well as a brief overview about Intersession-Online as a new possibility for the economic assessment of intersession experiences in psychotherapeutic practice.
If the therapist is still interested in using the application, the therapist account is activated by the researcher. After successful activation, a second talk follows. The aim of this second talk is to familiarize the therapist with the use of Intersession-Online as good as possible. During this presentation, the therapist learns to handle the smartphone application framework from both patient and therapists’ perspectives. This procedure ensures that the therapists can also competently advise and introduce his/her own patients. This second introduction takes about 30 min. As a last step, we provide a digital user manual with all relevant information and FAQ. Technical support is also available to all users.
If a patient wants to use Intersession-Online, he/she receives an automatically generated document from the therapist with a personal pairing code and step-by-step instructions on how to set up the app. We recommend a personal introduction for the patient provided by the therapist to discuss all central points of Intersession-Online (i.e., frequency of push notifications; explanation for the frequency of push notifications, data security; which data will be transferred; which data will be only stored locally on the device?). This personal introduction can increase the patient’s compliance. In our first alpha tests, we found that the willingness of patients to complete frequent assessments was higher when they received a personal and comprehensive introduction. This introduction takes about 20 to 25 min. In addition, the patients also receive a user manual with all important aspects and functions of Intersession-Online and FAQ. Technical support is also available for all patients.
In summary, therapists invest about 60 to 90 min (one time) to get to know and handle Intersession-Online competently as well as 20 to 25 min to introduce patients to the app. Based on previous experiences and pre-tests, the daily usage time per patient is estimated to be about one to two minutes. Within this time, all summarized and graphically presented results of the patient can be viewed, i.e., before a session. The psychotherapeutic practice is characterized by a tight schedule. Therefore, it is necessary to have a simple and clear app structure and user-friendly presented graphical results in order to allow app usage between two sessions.
3.1.7. Privacy Issues
Intersession-Online collects sensitive data. Therefore, data security is a central issue for Intersession-Online. In order to protect the patient’s data, different safety precautions were implemented. First, patients can share their data with researchers and their therapists. Data-sharing only happens with the permission of the patient. The patient can change the permission at any time. That means, the patient can withdraw or grant the permission in a flexible and transparent manner by easily using the settings section of the apps.
Privacy Protection on the Phone
The most confidential data that are stored in the app are the user credentials. They grant access to all sensitive user-related records. Therefore, they are solely stored encrypted.
Privacy Protection on the Server
The data exchange with the server component is realized with a secure hypertext transfer protocol (HTTPS) connection. Confidential data on the server can only be retrieved externally by authorized persons with a proper authentication.
Server Requirements
The server comprises the web application, the RESTful API, and the relational database. The web application was implemented using Angular. For the RESTful API, the Laravel framework was utilized. For the data storage, a MariaDB relational database was used. More information about the server can be found at [36]. For the entire communication within the framework, only encrypted data channels are used (i.e., HTTPS). In addition, for the installation of the framework components, it was taken care of all commonly security measures (e.g., for MariaDB mysql_secure_installation).
3.1.8. Research with Intersession-Online
The development of Intersession-Online is part of a larger intersession project with different partial studies. At the moment, we are doing the alpha testing. Based on other studies that have reviewed new smartphone applications [51], a total of N = 20 patients will be recruited for testing and evaluating the app. For the evaluation, we are using App Quality Assessment (AQUA), a multidimensional questionnaire for the assessment of the quality of smartphone applications. The app will be evaluated regarding usability, user engagement, content, visualization, therapeutic quality, and security. After the evaluation, Intersession-Online will be revised based on patient feedback. The patients are recruited at the psychotherapeutic research and study center from the Institute for Psychology at the University of Klagenfurt. This is an outpatient center, mainly for patients with anxiety or mood disorders. They receive weekly psychoanalytic, psychodynamic, or mentalized-based treatment for 50 min.
Patient participation is voluntary and written informed consent to participate will be obtained from all participants. The data of the patients are protected by the measures described in 3.1.6. If the patients have any questions, they can ask their therapists or the principal investigator. Patients have the right to withdraw from the study at any time without any consequences for their therapy.
The main study will be a randomized-controlled trial (RCT) to investigate the efficacy of Intersession-Online. Primary outcomes are quality of intersession experiences, outcome, and therapeutic alliance. Our hypothesis is that patients with Intersession-Online will have more positive intersession experiences, a better outcome, and therapeutic alliance. With reference to preliminary studies, in which differences in intersession activities showed small to medium effect sizes, we have calculated a power analysis with f = 0.25, an alpha error probability of p < 0.05, and a sufficiently high power of w = 0.80. The power analysis showed an a priori total sample size (both groups) of N = 158 patients, which will be the planned sample size for the RCT.
4. Limitations
For such a complex framework that was presented here, there exist technical limitations on one hand as well as domain-specific limitations on the other. Technically, it is always an issue whether the iOS and Android application are really similar. Based on the study shown in [52], it can be assumed that there might be also differences for this project. However, the apps have been thoroughly tested, including the perceived subjective feeling whether the apps are equally experienced. In addition, after Study 3 (see Section 2) has been finished, and based on the gathered real-life date, we plan a study to investigate whether the two mobile operating systems have caused a bias on the data collection procedure or their usage for the intersession in general. Furthermore, the provision of notifications, especially in offline mode, is always challenging to provide in a reliable manner on the two mobile operating systems. Experiences from other projects have been therefore exploited, e.g., [10]. Furthermore, the mobile operating systems are often updated, these update cycle might interrupt functions and must be therefore carefully monitored. In this context, also important, not all mobile operating system versions can be satisfactorily considered. Consequently, older mobile operating versions are excluded, what might influence the overall satisfaction of users. From the domain-specific side, also limitations might be the case. First, as the procedure which has to be accomplished necessitates many steps to be done, users might get quickly bothered. Furthermore, it must be assumed that using Intersession-Online will already lead to higher intersession experiences, solely due to the repeated enquiries every day. Therefore, we must expect a slight bias when assessing intersession experiences of patients with Intersession-Online. Another limitation refers to the intervention algorithm of Intersession-Online. Currently, we are using scores of symptom distress and intersession activity based on the weekend assessment. It is conceivable that the generated and conveyed intervention is not corresponding to the current state of the patient. Reasons for that could be, for example, a change in symptom distress and intersession activity in the time between the weekend assessment and delivered intervention.
5. Discussion
Mobile health devices have become more and more important in psychotherapy. The market is flooded by all kinds of apps and online interventions and today’s technical options open new possibilities, especially for unconventional topics. Interestingly, currently less research on digital solutions exists. For example, recent works [53,54,55] have proposed a framework for remote therapeutic interventions. However, they do not explicitly consider the intersession phase in relation to therapeutic sessions. Since these works stem from the same authors, it is indicated that a digital and mobile-driven intersession management is still in its infancy. However, intersession experiences are a promising topic in psychotherapy research and practice. Nocross and Lambert [56] summarized that about 40% of variances of therapeutic variables are unexplained. Intersession experiences could be an auspicious approach to explain a part of these 40% unexplained variances. Hitherto, there is no possibility to assess intersession experiences in a systematic and economic way. The gold standard for the assessment of intersession experiences is too long for regular assessments. Furthermore, the questionnaire should be filled out immediately before a therapy session, which, in turn, leads to time difficulties and is associated with a recall bias. Here, new technologies could remedy this situation. Intersession-Online, a smartphone-based framework, addresses these problems and offers an opportunity to assess intersession experiences systematically and economically as well as to provide the summarized results to researchers and therapists in a comprehensive way. Moreover, it is planned that the framework is being used as an intervention to promote positive intersession experiences.
However, it remains to be seen whether therapists and patients will accept Intersession-Online. Our aim is to provide an app and website as user-friendly as possible, so that there is no considerable additional effort for therapists and patients. Nevertheless, we have to assume that the acceptance can be influenced by certain variables. Since almost every person in Europe has a smartphone nowadays, the basic prerequisite for using the app is given. However, we assume that the degree of technical affinity and age will influence the user behavior. Patients and therapists with low technical qualifications as well as older people are likely to show less interest on mobile health technologies. This problem could possibly be solved with intensive technical advice and support. Therefore, all therapists who want to use Intersession-Online will receive a personal introduction as described above. For the future, we also want to have video instructions. It can also be assumed that patients with serious mental illness (i.e., patients with schizophrenia or severe major depressive disorder) will also use the app less frequently than healthier patients.
The use of Intersession-Online might initially seem like a further effort for therapists, but in contrast, there is an enormous, systematic gain of real-time information for the psychotherapeutic process. By using Intersession-Online, therapists can track in real-time how patients are post-processing their sessions. Based on this information, the psychotherapeutic process and outcome can be optimized. However, this gain is associated with little time investment by the therapists. We need to check if it will be possible to implement Intersession-Online in the time-constrained workflows of psychotherapists. To date, it is unclear whether it will be possible for therapists in practice to provide their patients with an introduction to the app. It is also unclear whether therapists really have time to check the results of the next patient immediately before a session to use this information in this new psychotherapy session.
6. Summary and Outlook
To the best of our knowledge, Intersession-Online is the first possibility to assess intersession-experiences easily in real time and to provide summarized and evaluated results to therapists and researcher comprehensively. The evidence-based development of Intersession-Online is a future-oriented approach that can enhance both psychotherapy research and practice. However, the functionality and efficacy must first be proven. A randomized-controlled trial will be conducted to investigate the efficacy of Intersession-Online. Previous studies have shown that there is a correlation between intersession experiences and outcome as well as between intersession experiences and therapeutic alliance. The causality, however, is unclear. Future studies need to find an answer to this open question. Intersession-Online could make its contribution.
The future of psychotherapy research and practice lies in new technologies. The latter will be increasingly used in the future. However, it is important to rely on evidence-based possibilities. Following this, mobile health technologies may constitute proper supplements for research and practice. On the other hand, these technologies may never overcome the necessity of personal contact with a therapist.
Author Contributions
Conceptualization, T.-C.G. and S.A.; software, R.P., C.V.; resources, S.A. and R.P.; writing—original draft preparation, T.-C.G.; writing—review and editing, T.-C.G., R.P., C.V., T.P., S.A.; supervision, R.P., T.P. and S.A.; project administration, T.-C.G., R.P. and S.A.; funding acquisition, S.A., T.-C.G.
Funding
The development of the smartphone application is part of an intersession project from the University of Klagenfurt funded by the Österreichische Nationalbank (OeNB), grant number: 17485. The funder has no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results. The protocol was not peer-reviewed by this funding body.
Acknowledgments
The authors want to thank the Österreichische Nationalbank (OeNB) for funding this project. Furthermore, we want to thank (in alphabetical order) our programmer Miriam Gessler (Android-App), Julian Huber (API, database), Verena Pfaff (website), Reka Rejtoe (website), Carsten Vogel (iOS-App) for their tireless efforts and many hours of work.
Ethics Approval
The Ethics Committee of Carinthia (Austria) has approved this study. The study is registered with the number A 01/16. Written informed consent to participate will be obtained from all participants.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lui, J.H.L.; Marcus, D.K.; Barry, C.T. Evidence-based apps? A review of mental health mobile applications in a psychotherapy context. Prof. Psychol. Res. Pract. 2017, 48, 199–210. [Google Scholar] [CrossRef]
- Ruwaard, J.; Kristjansdottir, O.; Donker, T.; Petrie, K.; Proudfoot, J.; Clarke, J.; Birch, M.-R.; Christensen, H. Smartphones for smarter delivery of mental health programs: A systematic review. J. Med Internet Res. 2013, 15, e247. [Google Scholar]
- World Health Organization. MHealth: New Horizons for Health Through Mobile Technologies; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Menon, V.; Rajan, T.M.; Sarkar, S. Psychotherapeutic Applications of Mobile Phone-based Technologies: A Systematic Review of Current Research and Trends. Indian J. Psychol. Med. 2017, 39, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Prentice, J.L.; Dobson, K.S. A review of the risks and benefits associated with mobile phone applications for psychological interventions. Can. Psychol. Can. 2014, 55, 282–290. [Google Scholar] [CrossRef]
- Pryss, R.; Reichert, M.; John, D.; Frank, J.; Schlee, W.; Probst, T. A personalized sensor support tool for the training of mindful walking. In Proceedings of the IEEE 15th International Conference on Wearable and Implantable Body Sensor Networks (BSN), Las Vegas, NV, USA, 4–7 March 2018; pp. 114–117. [Google Scholar]
- Pryss, R.; John, D.; Schlee, W.; Schlotz, W.; Schobel, J.; Kraft, R.; Spiliopoulou, M.; Langguth, B.; Reichert, M.; O’Rourke, T.; et al. Exploring the time trend of stress-levels while using the crowdsensing mHealth platform TrackYourStress and the influence of stress reactivity. JMIR mHealth 2019, 7, e13978. [Google Scholar]
- Bush, N.E.; Armstrong, C.M.; Hoyt, T.V. Smartphone apps for psychological health: A brief state of the science review. Psychol. Serv. 2019, 16, 188–195. [Google Scholar] [CrossRef]
- Last John, M. A Dictionary of Epidemiology, 4th ed.; Oxford University Press: New York, NY, USA, 2001. [Google Scholar]
- Pryss, R.; Probst, T.; Schlee, W.; Schobel, J.; Langguth, B.; Neff, P.; Spiliopoulou, M.; Reichert, M. Prospective crowdsensing versus retrospective ratings of tinnitus variability and tinnitus–stress associations based on the TrackYourTinnitus mobile platform. Int. J. Data Sci. Anal. 2018, 43, 88. [Google Scholar] [CrossRef]
- Orlinsky, D.E.; Geller, J.D.; Tarragona, M.; Farber, B. Patient’s representations of psychotherapy: A new focus for psychodynamic research. J. Consult. Clin. Psychol. 1993, 61, 596–610. [Google Scholar] [CrossRef]
- Orlinsky, D.E.; Geller, J.D. Patient’s Representations of Their Therapists and Therapy: New Measures; Miller, N.E., Ed.; Psychodynamic treatment research. A handbook for clinical practice; BasicBooks: New York, NY, USA, 1993; pp. 423–466. [Google Scholar]
- Hartmann, A.; Orlinsky, D.; Zeeck, A. The structure of intersession experience in psychotherapy and its relation to the therapeutic alliance. J. Clin. Psychol. 2011, 67, 1044–1063. [Google Scholar] [CrossRef]
- Hartmann, A. Therapie Zwischen den Stunden: Explorationen von Intersession-Prozessen [Therapy Between Therapy Sessions: Exploration of Intersession Experiences]; P. Lang: Frankfurt, Germany, 1997. [Google Scholar]
- Orlinsky, D.E. The generic model of psychotherapy after 25 years: Evolution of a research-based metatheory. J. Psychother. Integr. 2009, 19, 319–339. [Google Scholar] [CrossRef]
- Sol, G.L.; Bergin, E.A. (Eds.) Handbook of Psychotherapy and Behavior Change, 3rd ed.; Wiley: New York, NY, USA, 1986. [Google Scholar]
- Stewart, S.; Schröder, T. Emotional homework: A systematic literature review of patients’ intersession experiences. J. Psychother. Integr. 2015, 25, 236–252. [Google Scholar] [CrossRef]
- Tarragona, M.; Orlinsky, D.E. Patient’s experience of therapy between sessions. In Proceedings of the 18th Annual Meeting of the Society for Psychotherapy Research, Ulm, Germany, 16–20 June 1987. [Google Scholar]
- Orlinsky, D.E.; Tarragona, M. Patient’s representations of the therapist and experiences in therapy sessions: Further findings. In Proceedings of the 20th Annual Meeting of the Society for Psychotherapy Research, Toronto, ON, Canada, 21–24 June 1989. [Google Scholar]
- Geller, J.; Farber, B. Factors influencing the process of internalization in psychotherapy. Psychother. Res. 1993, 3, 166–180. [Google Scholar] [CrossRef]
- Andreas, S.; Gablonski, T.-C.; Hiesberger, S.; Senft, B.; Koller, I.; Schulz, H. Intersession-Prozesse in stationärer psychotherapeutischer Behandlung: Ist die Einzel-oder die Gruppentherapie entscheidender für die therapeutische Beziehung und das Therapieergebnis? [Intersession-Processes in inpatient therapy: Are the individual or group therapy important for the therapeutic relationship and the outcome?]. Psychodyn. Psychother. 2016, 15, 206–218. [Google Scholar]
- Knox, S.; Goldberg, J.L.; Woodhouse, S.S.; Hill, C.E. Client’s internal representations of their therapists. J. Couns. Psychol. 1999, 46, 244–256. [Google Scholar] [CrossRef][Green Version]
- Owen, J.; Quirk, K.; Hilsenroth, M.J.; Rodolfa, E. Working through: In-session processes that promote between-session thoughts and activities. J. Couns. Psychol. 2012, 59, 161–167. [Google Scholar] [CrossRef]
- Geller, J.D.; Cooley, R.S.; Hartley, D. Images of psychotherapist: A theoretical and methodological perspective. Imagin. Cogn. Personal. 1981, 1, 123–146. [Google Scholar] [CrossRef]
- Hartmann, A.; Orlinsky, D.; Weber, S.; Sandholz, A.; Zeeck, A. Session and intersession experience related to treatment outcome in bulimia nervosa. Psychother. Theory Res. Pract. Train. 2010, 47, 355–370. [Google Scholar] [CrossRef]
- Zeeck, A.; Hartmann, A. Relating therapeutic process to outcome: Are there predictors for the short-term course in anorexic patients? Eur. Eat. Disord. Rev. 2005, 13, 245–254. [Google Scholar] [CrossRef]
- Bender, D.S.; Farber, B.A.; Sanislow, C.A.; Dyck, I.R.; Geller, J.D.; Skodol, A.E. Representations of therapists by patiens with personality disorder. Am. J. Psychother. 2003, 57, 219–236. [Google Scholar] [CrossRef]
- Gablonski, T.-C.; Hiesberger, S.; Senft, B.; Andreas, S. The relationship between intersession processes and level of personality functioning in patients with mental disorders. In Proceedings of the 46th International Annual Meeting of the Society for Psychotherapy Research (SPR), Philadelphia, PA, USA, 24–27 June 2015. [Google Scholar]
- Almut, Z.; Hartmann, A.; Herzog, W.; Wild, B.; deZwaan, M.; Zipfel, S.; Sahin, Z. Outpatient psychotherapy for anorexia nervosa: exploring the Inter-Session-Process in the ANTOP-study. In Proceedings of the 46th International Annual Meeting of the Society for Psychotherapy Research (SPR), Philadelphia, PA, USA, 24–27 June 2015. [Google Scholar]
- Hartmann, A.; Almut, Z.; Herzog, W.; Wild, B.; deZwaan, M.; Zipfel, S.; Sahin, Z. The inter-session-process in psychodynamic and cognitive-behavioral psychotherapy for anorexia nervosa and its relation to outcome. In Proceedings of the 46th International Annual Meeting of the Society for Psychotherapy Research (SPR), Philadelphia, PA, USA, 24–27 June 2015. [Google Scholar]
- Pomnitz Fabiane, B.; Schattenburg, S.L.; Wünsch-Leiteritz, W.; Leiteritz, A.; Schreiber-Willnow, K.; Dobersch, J.; Moffenter, J.; Nickel, R.; Huber, T.; Braks, K. Was erleben Patienten in stationärer Psychotherapie zwischen den Gruppentherapie-Sitzungen? Eine Erprobung des Inter-Session-Fragebogens in der Klinik. Psychother. Psych. Med. 2016, 66, 21–30. [Google Scholar] [CrossRef]
- Orlinsky, D.E.; Tarragona, M. Intersession Experience Questionnaire (Patient Form); University of Chicago Committee on Human Development: Chicago, IL, USA, 1986. [Google Scholar]
- Hartmann, A.; Orlinsky, D.E.; Geller, J.D.; Zeeck, A. Der Inter-Session-Fragebogen (ISF) [The Intersession Experience Questionnaire]. Psychother. Psych. Med. 2003, 53, T67–T75. [Google Scholar]
- Gablonski, T.-C.; Kadur, J.; Lüdemann, J.; Wirth, L.; Lutz, G.; Andreas, S. Intersession experiences and its association with in-session-processes and outcome. In Proceedings of the 50th International Annual Meeting of the Society for Psychotherapy Research (SPR), Buenos Aires, Argentina, 3–6 July 2019. [Google Scholar]
- Fabian, W.; Munder, T.; Leonhart, R.; Herzog, T.; Plassmann, R.; Barth, J.; Wolfgang Linster, H. Die deutschsprachige Version des Working Alliance Inventory-short revised (WAI-SR)-Ein schulenübergreifendes, ökonomisches und empirisch validiertes Instrument zur Erfassung der therapeutischen Allianz. Klin. Diagn. Eval. 2008, 1, 343–358. [Google Scholar]
- Huber, J. Conception and Realization of a REST-based Application Programming Interface for Intersession-Management in Psychology. Bachelor’s Thesis, Ulm University, Ulm, Germany, 2019. [Google Scholar]
- Pryss, R.; Schobel, J.; Reichert, M. Requirements for a flexible and generic API enabling mobile crowdsensing mhealth applications. In Proceedings of the 4th International Workshop on Requirements Engineering for Self-Adaptive, Collaborative, and Cyber Physical Systems (RESACS), Bannf, AB, Canada, 20 August 2018; pp. 24–31. [Google Scholar]
- Almut, Z.; Hartmann, A.; Orlinsky, D.E. Inter-Session-Prozesse: Ein vernachlässigtes Thema der Psychotherapieforschung. Psychother. Psych. Med. 2004, 54, 236–242. [Google Scholar]
- Klinitzke, G.; Romppel, M.; Häuser, W.; Brähler, E.; Glaesmer, H. Die deutsche Version des Childhood Trauma Questionnaire (CTQ)-psychometrische Eigenschaften in einer bevölkerungsrepräsentativen Stichprobe. Psychother. Psychosom. Med. Psychol. 2012, 62, 47–51. [Google Scholar] [CrossRef]
- Sammet, I.; Leichsenring, F.; Schauenburg, H.; Andreas, S. Self-ratings of pathogenic beliefs: A study based on the psychodynamic control-mastery theory. Psychotherapy research. J. Soc. Psychother. Res. 2007, 17, 494–503. [Google Scholar] [CrossRef]
- Hausberg, M.C.; Schulz, H.; Piegler, T.; Happach, C.G.; Klöpper, M.; Brütt, A.L.; Sammet, I.; Andreas, S. Is a self-rated instrument appropriate to assess mentalization in patients with mental disorders? Development and first validation of the mentalization questionnaire (MZQ). Psychotherapy Research. 2012, 22, 699–709. [Google Scholar]
- Fonagy, P.; Gergely, G.; Jurist, E.L.; Target, M. Affect Regulation, Mentalization, and the Development of the Self; Other Press: New York, NY, USA, 2002. [Google Scholar]
- Bateman, A.; Fonagy, P. (Eds.) Handbook of Mentalizing in Mental Health Practice; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2012. [Google Scholar]
- Bartholomew, K.; Horowitz, L.M. Attachment styles among young adults: A test of a four-category model. J. Pers. Soc. Psychol. 1991, 61, 226–244. [Google Scholar] [CrossRef]
- Dammann, G.; Smole, S.; Kraus, C.; Buchheim, P. IPO-2001: Inventory of Personality Organization; Psychosomatische Poliklinik: Munich, Germany, 2002. [Google Scholar]
- Kerber, A.; Schultze, M.; Knaevelsrud, C.; Wright, A.G.C.; Spitzer, C.; Zimmermann, J. Persönlichkeitsinventar für DSM-5 und ICD-11—Kurzform (PID5BF+); American Psychiatric Association: Philadelphia, PA, USA, 2019. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. DSM-5; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- World Health Organization. ICD-11-MMS: International Classification of Diseases for Mortality and Morbidity Statistics; W.H.O.: Geneva, Switzerland, 2019. [Google Scholar]
- Rabung, S.; Harfst, T.; Koch, U.; Schulz, H. Hamburger Module zur Erfassung allgemeiner Aspekte psychosozialer Gesundheit für die therapeutische Praxis (Health-49); Universitätsklinikum Hamburg Eppendorf: Hamburg, Germany, 2007. [Google Scholar]
- Klaghofer, R.; Brähler, E. Konstruktion und teststatistische Prüfung einer Kurzform der SCL-90-R. Zeitschrift für Klinische Psychologie. Psychiatr. Psychother. 2001, 49, 115–124. [Google Scholar]
- Wolf, M.; Kraft, S.; Tschauner, K.; Bauer, S.; Becker, T.; Puschner, B. User activity in a mobile phone intervention to assist mindfulness exercises in people with depressive symptoms. Ment. Health Prev. 2016, 4, 57–62. [Google Scholar] [CrossRef]
- Pryss, R.; Schlee, W.; Hoppenstedt, B.; Reichert, M.; Spiliopoulou, M.; Langguth, B.; Probst, T. Applying Machine Learning on the Daily Life Data of the TrackYourTinnitus mHealth Crowdsensing Platform Predicts the Mobile Operating System with High Accuracy. JMIR 2019. preprints. [Google Scholar]
- Schickler, M.; Pryss, R.; Schlee, W.; Probst, T.; Langguth, B.; Schobel, J.; Reichert, M. Usability Study on Mobile Processes Enabling Remote Therapeutic Interventions. In Proceedings of the IEEE 31st International Symposium on Computer-Based Medical Systems (CBMS), Karlstad, Sweden, 18–21 June 2018; pp. 146–151. [Google Scholar]
- Schickler, M.; Pryss, R.; Schobel, J.; Reichert, M. Supporting Remote Therapeutic Interventions with Mobile Processes. In Proceedings of the IEEE International Conference on AI & Mobile Services (AIMS), Honolulu, HI, USA, 25–30 June 2017; pp. 30–37. [Google Scholar]
- Schickler, M.; Pryss, R.; Stach, M.; Schobel, J.; Schlee, W.; Probst, T.; Reichert, M. An IT Platform Enabling Remote Therapeutic Interventions. In Proceedings of the IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS), Thessaloniki, Greece, 22–24 June 2017; pp. 111–116. [Google Scholar]
- Nocross, J.C.; Lambert, M.J. Evidence-based therapy relationships. In Psychotherapy Relationships That Work. Evidence-Based Responsiveness; Norcross, J.C., Ed.; Oxford University Press: New York, NY, USA, 2011; pp. 3–21. [Google Scholar]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).