
Direct-to-Implant Prepectoral Breast Reconstruction with a Novel Collagen Matrix Following Nipple-Sparing Mastectomy: A Case Report


 and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction and Clinical Significance
2. Case Presentation
2.1. Clinical Findings and Treatment Plan
2.2. Surgical Procedure
2.2.1. Preoperative Assessment
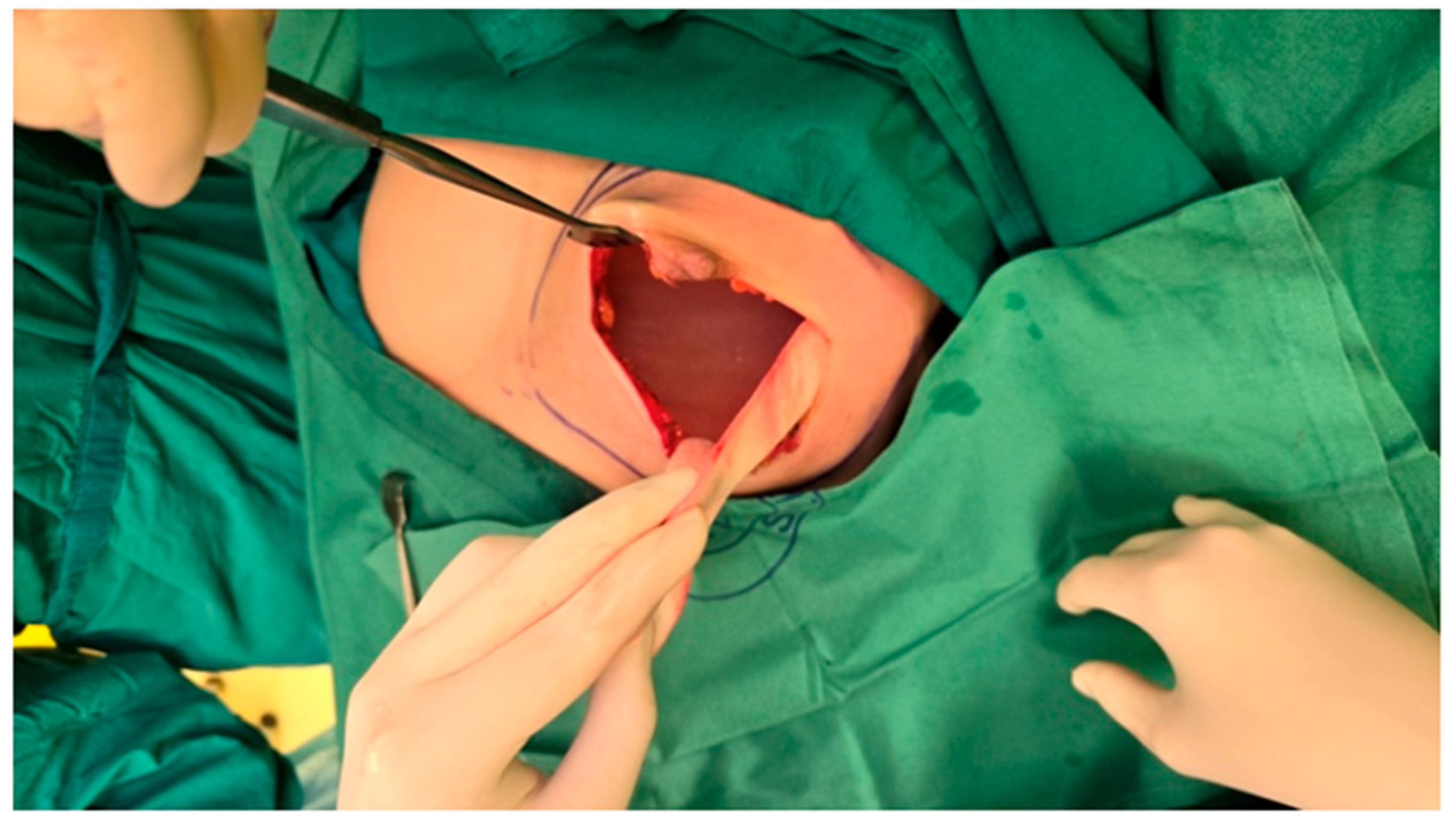
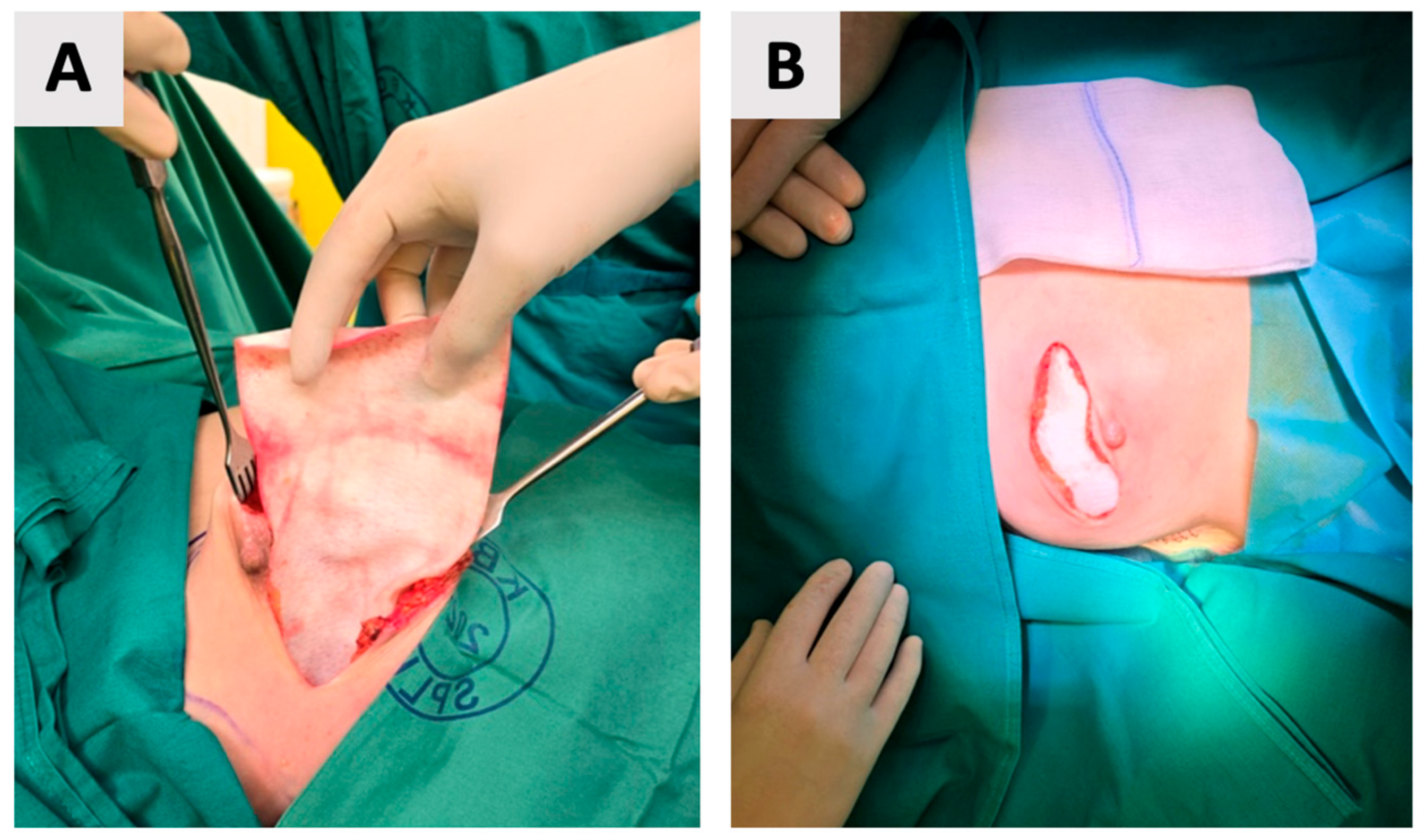
2.2.2. Mastectomy
2.2.3. Implant Placement and Wound Closure
2.2.4. Postoperative Course and Healing
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giaquinto, A.N.; Sung, H.; Newman, L.A.; Freedman, R.A.; Smith, R.A.; Star, J.; Jemal, A.; Siegel, R.L. Breast Cancer Statistics 2024. CA Cancer J. Clin. 2024, 74, 477–495. [Google Scholar] [CrossRef] [PubMed]
- Rahman, G.A. Breast Conserving Therapy: A Surgical Technique Where Little Can Mean More. J. Surg. Tech. Case Rep. 2011, 3, 1–4. [Google Scholar] [CrossRef]
- Santanelli di Pompeo, F.; Firmani, G.; Paolini, G.; Clemens, M.W.; Argento, G.; Barelli, G.M.; Rosati, E.; Zanovello, C.; D’Orsi, G.; Sorotos, M. Determining Breast Implant Prevalence: A Population Study of Italian Chest Radiographs. Aesthetic Plast. Surg. 2023, 47, 957–965. [Google Scholar] [CrossRef]
- Santanelli di Pompeo, F.; Sorotos, M.; Clemens, M.W.; Paolini, G.; Anibaldi, P.; Davoli, M.; Baglio, G.; Pinnarelli, L.; Ferranti, M.; Cerza, F.; et al. Mortality Rate in Breast Implant Surgery: Is an Additional Procedure Worthwhile to Mitigate BIA-ALCL Risk? Aesthetic Plast. Surg. 2023, 47, 914–926. [Google Scholar] [CrossRef] [PubMed]
- Quintero Sierra, L.A.; Busato, A.; Zingaretti, N.; Conti, A.; Biswas, R.; Governa, M.; Vigato, E.; Parodi, P.C.; Bernardi, P.; Sbarbati, A.; et al. Tissue-Material Integration and Biostimulation Study of Collagen Acellular Matrices. Tissue Eng. Regen. Med. 2022, 19, 477–490. [Google Scholar] [CrossRef] [PubMed]
- Barbeck, M.; Lorenz, J.; Kubesch, A.; Böhm, N.; Booms, P.; Choukroun, J.; Sader, R.; Kirkpatrick, C.J.; Ghanaati, S. Porcine Dermis-Derived Collagen Membranes Induce Implantation Bed Vascularization Via Multinucleated Giant Cells: A Physiological Reaction? J. Oral Implantol. 2015, 41, e238–e251. [Google Scholar] [CrossRef] [PubMed]
- Rothamel, D.; Benner, M.; Fienitz, T.; Happe, A.; Kreppel, M.; Nickenig, H.-J.; Zöller, J.E. Biodegradation Pattern and Tissue Integration of Native and Cross-Linked Porcine Collagen Soft Tissue Augmentation Matrices—An Experimental Study in the Rat. Head. Face Med. 2014, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Pabst, A.M.; Happe, A.; Callaway, A.; Ziebart, T.; Stratul, S.I.; Ackermann, M.; Konerding, M.A.; Willershausen, B.; Kasaj, A. In Vitro and in Vivo Characterization of Porcine Acellular Dermal Matrix for Gingival Augmentation Procedures. J. Periodontal Res. 2014, 49, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Alkildani, S.; Burckhardt, K.; Köwitsch, A.; Radenkovic, M.; Stojanovic, S.; Najman, S.; Jung, O.; Liu, L.; Barbeck, M. The Influence of Different Crosslinking Agents onto the Physical Properties, Integration Behavior and Immune Response of Collagen-Based Barrier Membranes. Front. Bioeng. Biotechnol. 2024, 12, 1506433. [Google Scholar] [CrossRef] [PubMed]
- Macadam, S.A.; Lennox, P.A. Acellular Dermal Matrices: Use in Reconstructive and Aesthetic Breast Surgery. Can. J. Plast. Surg. 2012, 20, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Wan, H.; Sandor, M.; Qi, S.; Ervin, F.; Harper, J.R.; Silverman, R.P.; McQuillan, D.J. Host Response to Human Acellular Dermal Matrix Transplantation in a Primate Model of Abdominal Wall Repair. Tissue Eng. Part A 2008, 14, 2009–2019. [Google Scholar] [CrossRef] [PubMed]
- Mohammadyari, F.; Parvin, S.; Khorvash, M.; Amini, A.; Behzadi, A.; HajEbrahimi, R.; Kasaei, F.; Olangian-Tehrani, S. Acellular Dermal Matrix in Reconstructive Surgery: Applications, Benefits, and Cost. Front. Transplant. 2023, 2, 1133806. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.E.; Burns, N.K.; Campbell, K.T.; Mathur, A.B.; Jaffari, M.V.; Rios, C.N. Comparison of Cross-Linked and Non-Cross-Linked Porcine Acellular Dermal Matrices for Ventral Hernia Repair. J. Am. Coll. Surg. 2010, 211, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Zeng, J.; Tian, X.; Zheng, H.; Wu, X. A Review of Different Breast Reconstruction Methods. Am. J. Transl. Res. 2023, 15, 3846–3855. [Google Scholar] [PubMed]
- Malekpour, M.; Malekpour, F.; Wang, H.T.-H. Breast Reconstruction: Review of Current Autologous and Implant-Based Techniques and Long-Term Oncologic Outcome. World J. Clin. Cases 2023, 11, 2201–2212. [Google Scholar] [CrossRef] [PubMed]
- Nagura, N.; Hayashi, N.; Takei, J.; Yoshida, A.; Ochi, T.; Iwahira, Y.; Yamauchi, H. Breast Reconstruction after Risk-Reducing Mastectomy in BRCA Mutation Carriers. Breast Cancer 2020, 27, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Saldanha, I.J.; Broyles, J.M.; Adam, G.P.; Cao, W.; Bhuma, M.R.; Mehta, S.; Pusic, A.L.; Dominici, L.S.; Balk, E.M. Implant-Based Breast Reconstruction after Mastectomy for Breast Cancer: A Systematic Review and Meta-Analysis. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4179. [Google Scholar] [CrossRef] [PubMed]
- Malata, C.M.; McIntosh, S.A.; Purushotham, A.D. Immediate Breast Reconstruction after Mastectomy for Cancer. Br. J. Surg. 2000, 87, 1455–1472. [Google Scholar] [CrossRef] [PubMed]
- Berna, G.; De Grazia, A.; Antoniazzi, E.; Romeo, M.; Dell’Antonia, F.; Lovero, S.; Marchica, P.; Rizzetto, C.; Burelli, P. Novel Three-Dimensional Acellular Dermal Matrix for Prepectoral Breast Reconstruction: First Year in Review with BRAXON®Fast. Front. Surg. 2022, 9, 970053. [Google Scholar] [CrossRef] [PubMed]
- di Pompeo, F.S.; Firmani, G.; Paolini, G.; Amorosi, V.; Briganti, F.; Sorotos, M. Immediate Prepectoral Breast Reconstruction Using an ADM with Smooth Round Implants: A Prospective Observational Cohort Study. J. Plast. Reconstr. Aesthet. Surg. 2023, 80, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Fischer, J.P.; Nelson, J.A.; Cleveland, E.; Sieber, B.; Rohrbach, J.I.; Serletti, J.M.; Kanchwala, S. Breast Reconstruction Modality Outcome Study: A Comparison of Expander/Implants and Free Flaps in Select Patients. Plast. Reconstr. Surg. 2013, 131, 928. [Google Scholar] [CrossRef] [PubMed]
- Zhong, T.; McCarthy, C.; Min, S.; Zhang, J.; Beber, B.; Pusic, A.L.; Hofer, S.O.P. Patient Satisfaction and Health-Related Quality of Life after Autologous Tissue Breast Reconstruction: A Prospective Analysis of Early Postoperative Outcomes. Cancer 2012, 118, 1701–1709. [Google Scholar] [CrossRef] [PubMed]
- Colakoglu, S.; Khansa, I.; Curtis, M.S.; Yueh, J.H.; Ogunleye, A.; Haewyon, C.; Tobias, A.M.; Lee, B.T. Impact of Complications on Patient Satisfaction in Breast Reconstruction. Plast. Reconstr. Surg. 2011, 127, 1428–1436. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, P.G.; Jazayeri, L. Two-Stage Implant-Based Breast Reconstruction: An Evolution of the Conceptual and Technical Approach over a Two-Decade Period. Plast. Reconstr. Surg. 2016, 138, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dueñas-Rodríguez, B.; Navarro-Cecilia, J.; Luque-López, C.; Sánchez-Andujar, B.; Garcelán-Trigo, J.A.; Ramírez-Expósito, M.J.; Martínez-Martos, J.M. Single-Stage Immediate Breast Reconstruction with Acellular Dermal Matrix after Breast Cancer: Comparative Study and Evaluation of Breast Reconstruction Outcomes. Cancers 2023, 15, 5349. [Google Scholar] [CrossRef] [PubMed]
- Manyam, B.V.; Shah, C.; Woody, N.M.; Reddy, C.A.; Weller, M.A.; Juloori, A.; Naik, M.; Valente, S.; Grobmyer, S.; Durand, P.; et al. Long-Term Complications and Reconstruction Failures in Previously Radiated Breast Cancer Patients Receiving Salvage Mastectomy with Autologous Reconstruction or Tissue Expander/Implant-Based Reconstruction. Breast J. 2019, 25, 1071–1078. [Google Scholar] [CrossRef] [PubMed]
- Taj, S.; Chandavarkar, R.; Vidya, R. Current Global Trends in Prepectoral Breast Reconstruction. Medicina 2024, 60, 431. [Google Scholar] [CrossRef] [PubMed]
- Polotto, S.; Bergamini, M.L.; Pedrazzi, G.; Arcuri, M.F.; Gussago, F.; Cattelani, L. One-Step Prepectoral Breast Reconstruction with Porcine Dermal Matrix-Covered Implant: A Protective Technique Improving the Outcome in Post-Mastectomy Radiation Therapy Setting. Gland. Surg. 2020, 9, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Bertozzi, N.; Pesce, M.; Santi, P.; Raposio, E. One-Stage Immediate Breast Reconstruction: A Concise Review. Biomed. Res. Int. 2017, 2017, 6486859. [Google Scholar] [CrossRef] [PubMed]
- Topol, B.M.; Dalton, E.F.; Ponn, T.; Campbell, C.J. Immediate Single-Stage Breast Reconstruction Using Implants and Human Acellular Dermal Tissue Matrix with Adjustment of the Lower Pole of the Breast to Reduce Unwanted Lift. Ann. Plast. Surg. 2008, 61, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Bassetto, F.; Pandis, L. Clinical Experience with Surgimend in Breast Reconstruction: An Overview. Br. J. Hosp. Med. 2020, 81, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Gui, G.; Gui, M.; Gui, A.; Tasoulis, M.K. Physical Characteristics of SurgiMend Meshed Biological ADM in Immediate Prepectoral Implant Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2022, 10, e4369. [Google Scholar] [CrossRef] [PubMed]
- Berger, L.E.; Spoer, D.L.; Huffman, S.S.; Haffner, Z.K.; Tom, L.K.; Parkih, R.P.; Song, D.H.; Fan, K.L. Acellular Dermal Matrix-Assisted, Prosthesis-Based Breast Reconstruction: A Comparison of SurgiMend PRS, AlloDerm, and DermACELL. Ann. Plast. Surg. 2024, 93, 34–42. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banović, J.; Pribudić, Z.; Madir, M.B.; Beara, V.; Perić, L.; Čandrlić, M.; Kačarević, Ž.P. Direct-to-Implant Prepectoral Breast Reconstruction with a Novel Collagen Matrix Following Nipple-Sparing Mastectomy: A Case Report. Reports 2025, 8, 120. https://doi.org/10.3390/reports8030120
Banović J, Pribudić Z, Madir MB, Beara V, Perić L, Čandrlić M, Kačarević ŽP. Direct-to-Implant Prepectoral Breast Reconstruction with a Novel Collagen Matrix Following Nipple-Sparing Mastectomy: A Case Report. Reports. 2025; 8(3):120. https://doi.org/10.3390/reports8030120
Chicago/Turabian StyleBanović, Josip, Zrinka Pribudić, Mia Buljubašić Madir, Vedran Beara, Luka Perić, Marija Čandrlić, and Željka Perić Kačarević. 2025. "Direct-to-Implant Prepectoral Breast Reconstruction with a Novel Collagen Matrix Following Nipple-Sparing Mastectomy: A Case Report" Reports 8, no. 3: 120. https://doi.org/10.3390/reports8030120
APA StyleBanović, J., Pribudić, Z., Madir, M. B., Beara, V., Perić, L., Čandrlić, M., & Kačarević, Ž. P. (2025). Direct-to-Implant Prepectoral Breast Reconstruction with a Novel Collagen Matrix Following Nipple-Sparing Mastectomy: A Case Report. Reports, 8(3), 120. https://doi.org/10.3390/reports8030120