
Primary Reconstruction of Extended Multifragmented Skull Fracture: Case Report and Technical Note

 , and
, and {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction and Clinical Significance
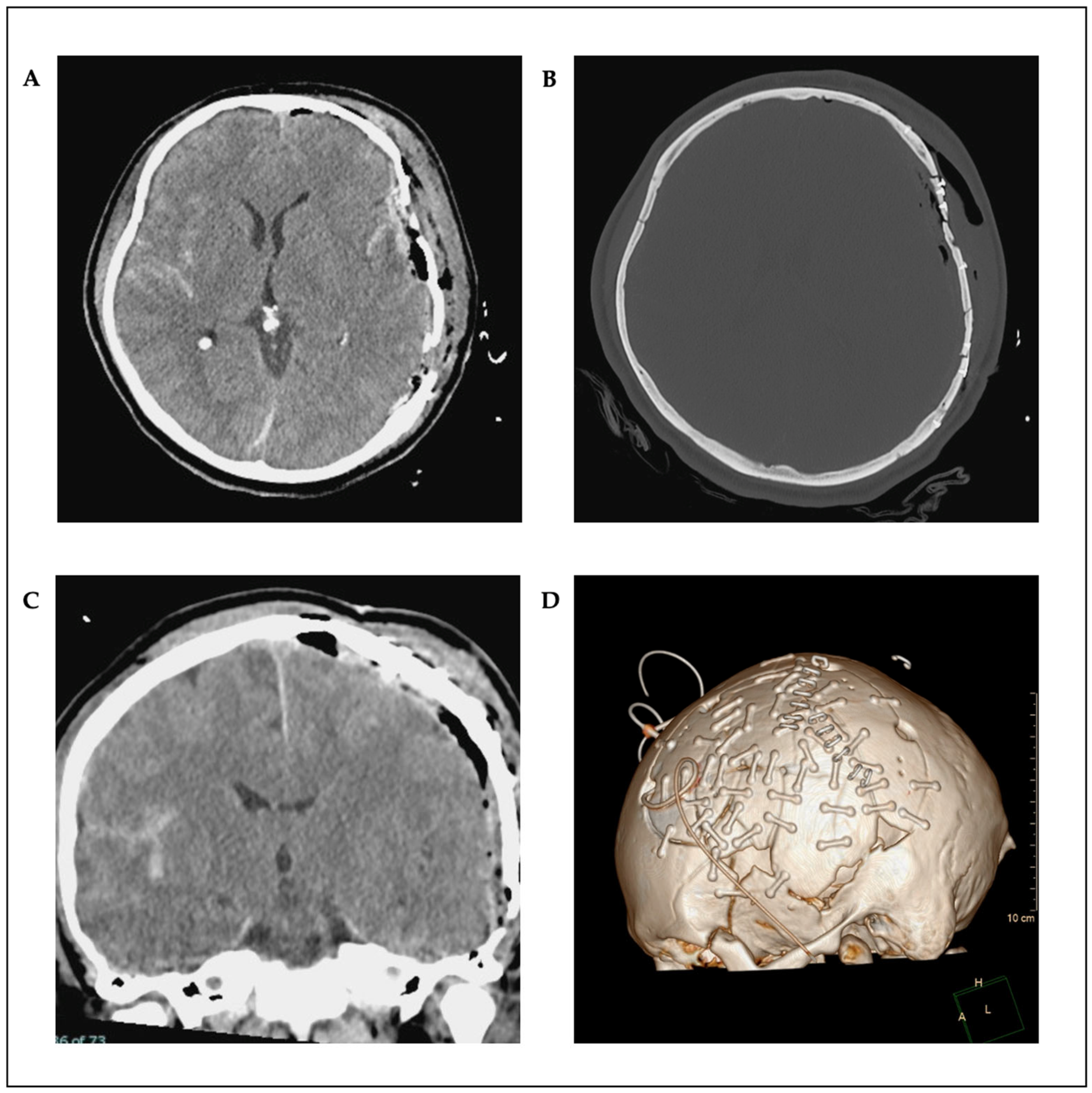
2. Case Presentation
Surgical Technique
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TBI | Traumatic brain injuries |
| DC | Decompresive craniectomy |
| DECRA | Decompresive craniectomy in diffuse traumatic brain injury |
| RCT | Randomized controlled trial |
| ICP | Intracranial pressure |
| RESCUEicp | Randomized Evaluation of Surgery with Craniectomy for Uncontrollable Elevation of Intracranial Pressure |
| CSF | Cerebrospinal fluid |
| CT | Computed tomography |
| SAH | Subarachnoid hemorrhage |
| MRI | Magnetic resonance imaging |
| ENT | Ear-Nose-Throat |
References
- Rosenfeld, J.V.; Maas, A.I.; Bragge, P.; Morganti-Kossmann, M.C.; Manley, G.T.; Gruen, R.L. Early Management of Severe Traumatic Brain Injury. Lancet 2012, 380, 1088–1098. [Google Scholar] [CrossRef] [PubMed]
- Coronado, V.G.; McGuire, L.C.; Sarmiento, K.; Bell, J.; Lionbarger, M.R.; Jones, C.D.; Geller, A.I.; Khoury, N.; Xu, L. Trends in Traumatic Brain Injury in the U.S. and the Public Health Response: 1995–2009. J. Saf. Res. 2012, 43, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Theadom, A.; Barker-Collo, S.; Starkey, N.J.; McPherson, K.; Kahan, M.; Dowell, A.; Brown, P.; Parag, V.; Kydd, R.; et al. Incidence of Traumatic Brain Injury in New Zealand: A Population-Based Study. Lancet Neurol. 2013, 12, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.F.; Wen, L.; Shen, F.; Li, G.; Lou, R.; Liu, W.G.; Zhan, R.Y. Surgical Complications Secondary to Decompressive Craniectomy in Patients with a Head Injury: A Series of 108 Consecutive Cases. Acta Neurochir. 2008, 150, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Servadei, F.; Compagnone, C.; Sahuquillo, J. The Role of Surgery in Traumatic Brain Injury. Curr. Opin. Crit. Care 2007, 13, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Honeybul, S.; Janzen, C.; Kruger, K.; Ho, K.M. Decompressive Craniectomy for Severe Traumatic Brain Injury: Is Life Worth Living? Clinical Article. J. Neurosurg. 2013, 119, 1566–1575. [Google Scholar] [CrossRef] [PubMed]
- Guerra, W.K.-W.; Gaab, M.R.; Dietz, H.; Mueller, J.-U.; Piek, J.; Fritsch, M.J. Surgical Decompression for Traumatic Brain Swelling: Indications and Results. J. Neurosurg. 1999, 90, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.J.; Rosenfeld, J.V.; Murray, L.; Arabi, Y.M.; Davies, A.R.; D’Urso, P.; Kossmann, T.; Ponsford, J.; Seppelt, I.; Reilly, P.; et al. Decompressive Craniectomy in Diffuse Traumatic Brain Injury. N. Engl. J. Med. 2011, 364, 1493–1502. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, P.J.; Kolias, A.G.; Timofeev, I.S.; Corteen, E.A.; Czosnyka, M.; Timothy, J.; Anderson, I.; Bulters, D.O.; Belli, A.; Eynon, C.A.; et al. Trial of Decompressive Craniectomy for Traumatic Intracranial Hypertension. N. Engl. J. Med. 2016, 375, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Camal Ruggieri, I.N.; Cícero, A.M.; Issa, J.P.M.; Feldman, S. Bone Fracture Healing: Perspectives According to Molecular Basis. J. Bone Miner. Metab. 2021, 39, 311–331. [Google Scholar] [CrossRef] [PubMed]
- Goiato, M.C.; Anchieta, R.B.; Pita, M.S.; Dos Santos, D.M. Reconstruction of Skull Defects: Currently Available Materials. J. Craniofacial Surg. 2009, 20, 1512–1518. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S.; Kucukyuruk, B.; Abuzayed, B.; Aydin, S.; Sanus, G.Z. Cranioplasty: Review of Materials and Techniques. J. Neurosci. Rural. Pract. 2011, 2, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Spetzger, U.; Vougioukas, V.; Schipper, J. Materials and Techniques for Osseous Skull Reconstruction. Minim. Invasive Ther. Allied Technol. 2010, 19, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Staffa, G.; Barbanera, A.; Faiola, A.; Fricia, M.; Limoni, P.; Mottaran, R.; Zanotti, B.; Stefini, R. Custom Made Bioceramic Implants in Complex and Large Cranial Reconstruction: A Two-Year Follow-Up. J. Cranio-Maxillofac. Surg. 2012, 40, e65–e70. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, A.; Austerberry, R.; Morrison, D.; Ho, K.M.; Honeybul, S. Cranioplasty with Custom-Made Titanium Plates-14 Years Experience. Neurosurgery 2013, 72, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.M.; Jung, H.; Skirboll, S. Materials Used in Cranioplasty: A History and Analysis. Neurosurg. Focus 2014, 36, E19. [Google Scholar] [CrossRef] [PubMed]
- Capitelli-McMahon, H.; Kahlar, N.; Rahman, S. Titanium Versus Autologous Bone-Based Cranioplasty: A Systematic Review and Meta-Analysis. Cureus 2023, 15, e39516. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camal Ruggieri, I.N.; Feigl, G.C.; Britz, G.W.; Kuzmin, D.; Staribacher, D. Primary Reconstruction of Extended Multifragmented Skull Fracture: Case Report and Technical Note. Reports 2025, 8, 102. https://doi.org/10.3390/reports8030102
Camal Ruggieri IN, Feigl GC, Britz GW, Kuzmin D, Staribacher D. Primary Reconstruction of Extended Multifragmented Skull Fracture: Case Report and Technical Note. Reports. 2025; 8(3):102. https://doi.org/10.3390/reports8030102
Chicago/Turabian StyleCamal Ruggieri, Iván N., Guenther C. Feigl, Gavin W. Britz, Dzmitry Kuzmin, and Daniel Staribacher. 2025. "Primary Reconstruction of Extended Multifragmented Skull Fracture: Case Report and Technical Note" Reports 8, no. 3: 102. https://doi.org/10.3390/reports8030102
APA StyleCamal Ruggieri, I. N., Feigl, G. C., Britz, G. W., Kuzmin, D., & Staribacher, D. (2025). Primary Reconstruction of Extended Multifragmented Skull Fracture: Case Report and Technical Note. Reports, 8(3), 102. https://doi.org/10.3390/reports8030102