1. Introduction
It is well known that long-term exposure to hand-arm vibration (HAV) leads to chronic complaints or diseases. In Germany, approximately 1600 occupational diseases related to HAV are reported annually; approximately 350 are recognized as occupational diseases [
1]. While working with vibrating tools, occupants are forced to adopt various postures, such as working overhead or bending forwards. However, to evaluate the workload for most occupational diseases caused by vibrating tools, only the magnitude of the HAV exposure according to ISO 5349-1 [
2] is considered. Consequently, adverse health effects of HAV while adopting an awkward posture can be underestimated by investigating the exposure of the device only. For example, the elevated prevalence of musculoskeletal diseases observed by workers with vibrating tools can be caused by combined effects of many risk factors, such as hard physical effort, constrained postures and strong grip force [
3,
4]. Recent studies [
5] have also shown that operators suffer from HAV syndrome as well as neck and back pain when exposed to prolonged vibration and constantly adopting an awkward posture. In contrast to the combined effects of whole-body and awkward posture, which have been quantified in several studies [
6,
7,
8] and even presented in a Technical report ISO/TR 10687 [
9], nothing quantifiable has yet been investigated in case of the combined effects of HAV and awkward hand-arm posture.
To show the influence of posture during hand-arm vibration exposure, different approaches such as magnitude of the vibration and feed and gripping forces for different working directions are applied [
10,
11,
12,
13]. While significant lower vibration magnitude was measured for working horizontally compared to vertical directions [
12], significant influence of the body posture on the acceleration of the main handle was shown by means of feed and gripping forces [
13].
Another approach to investigate the impact of posture during HAV exposure is considering power absorption. Thus, awkward wrist and elbow posture can yield higher power absorption into the hand-arm system compared to neutral posture [
14,
15]. For example, under an extended arm posture, the magnitudes of transmitted vibration were observed to be nearly twice as many as those for the bent-arm posture in the low-frequency region [
10].
Also, physiological investigations such as electromyographic measurements have been used to show the effect of combined exposures of vibration and posture on the human body [
16]. While the reaction of the flexor carpi ulnaris is primarily determined by the grip pressure, electrical activity of the biceps and triceps brachii muscles is increased during exposure to vibration. The authors suggest that segmental vibration can give rise to intense musculoskeletal strain in the upper extremities of the exposed workers. Thus, pathological changes in the musculoskeletal structures of the hand-arm system are caused by long-term use of portable vibrating tools, followed by musculoskeletal disorders such as upper limb pain, joint stiffness, and movement limitation. These musculoskeletal disorders could also be caused by awkward posture [
17], which is not considered quantitively yet.
Finally, the hypothesis here is that only measuring the HAV on the vibrating tool does not describe the impact on the body of the operating people. Thus, there is an underestimation of risk assessment if there is no consideration of the posture. As it is still unknown to what extent awkward posture can modulate the impact of vibrations on the hand-arm system, other investigations, such as muscle activity, can provide an overview about the impacts on the body, accompanying standard vibration measurements on the device. Thus, the aim of this project was to investigate the impact on the muscle load in the shoulder, upper arm, and forearm by using electromyographic data and subjective perception of the subjects using a hand-held power tool in three different positions.
2. Materials and Methods
2.1. Trial Population
Eleven (11) healthy, right-handed volunteers (seven males and four females, mean age ± standard deviation (SD) = 36 ± 11 year; mean height ± SD = 178 ± 8 cm; mean weight ± SD = 76 ± 15 kg) participated in this project. All subjects were not professional users. However, they were well-trained in using the tool.
At the time of the experiment, all subjects were in good health and were not suffering from noteworthy physical complaints. Also, participants should not have had any musculoskeletal problems or disease in the last twelve months. Written informed consent was obtained from the participants to participate in the experiments and allow for data analysis and the publication of results. The Ethics Committee of Luebeck University, Medical Faculty, approved of the study design with a positive vote.
2.2. Experimental Procedure
To investigate the influence of the working direction while using an impact wrench, three directions were chosen: upwards, forwards and downwards. Considering anthropometric differences, a height-adjustable experimental setup was designed to enable starting conditions that were as equal as possible in each working direction for each test person. The test persons were asked to adopt a standing posture with a 90-degree forearm angle perpendicular to the wooden plank of the test rack.
Figure 1 shows an example of the test setup with a test person and the examined impact wrench.
As a specimen for the tests, oak planks with a thickness of at least 100 mm and a size of approximately 800 mm300 mm were used. To enable a long screw-in time, 100 mm-long wood screws were used.
These screws were screwed in 12 times for each direction. A pilot hole was provided for each of the 12 screwing tasks. The power tool chosen for these tests was the Bosch Professional GDX 18V-LI impact wrench (Robert Bosch, Gerlingen, Germany), since this impact wrench delivers a high torque and is also safe and easy to use, even for inexperienced individuals. The working order (e.g., up/front/down) was randomly allocated, thus, six permutations were executed for three directions. After working in each working direction, 10 min pauses were executed.
2.3. Hand-Arm Vibration Measurements
In accordance with ISO 5349 [
2,
18], the tool handle vibration was measured for a period of 12 screwdriving operations. Accelerometers were glued on the tool handle (
Figure 1) in accordance with ISO 28927-5 [
19]. Accelerometer mounting and the application of necessary frequency weightings were undertaken in compliance with ISO 5349-1 and ISO 5349-2 standards [
2,
18].
The vibration magnitudes were expressed as root-mean-square (r.m.s.) acceleration, which was frequency-weighted and band-limited using the Wh filter in accordance with ISO 5349-1. The root-sum-of-squares (vibration total value,
) of the frequency-weighted acceleration values for the
x,
y and
z axes were calculated using:
Only the screwing-in processes with no pauses were included for the evaluations. When the screwing-in process was not completed in a single step, these instances were not included in the calculation of the mean value.
2.4. Body Posture
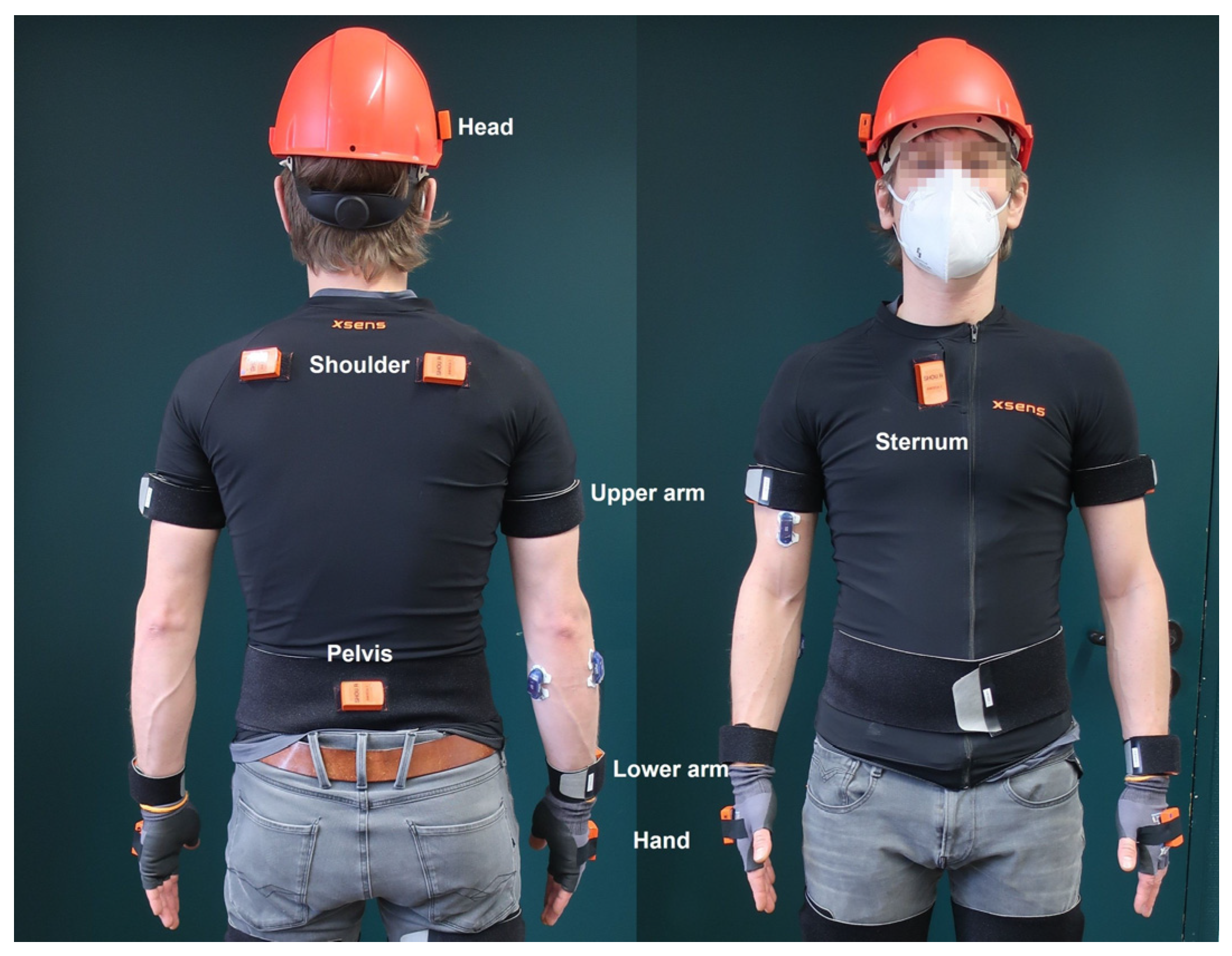
A Xsens Awinda (Movella Holdings Inc, Henderson, NV, USA) wireless measurement system (18 inertial measurement units) with 60 Hz measurement frequency was used to assess body posture (
Figure 2).
These measurement units comprise accelerometers, gyroscopes, magnetometers and a barometer. Recording of body posture data takes place in combination with the associated MVN 2022.0 Analyze software from Xsens. After the data was recorded, it was imported into CUELA (‘computer-assisted recording and long-term analysis of musculoskeletal loads’), an analyzing software developed by the Institute for Occupational Safety and Health of the German Social Accident Insurance [
20]. Hereby, the angle of the body is analyzed in accordance with ISO TR 10687 [
9]. Positive values denote flexion and radial deviation, while negative values denote extension and ulnar deviation.
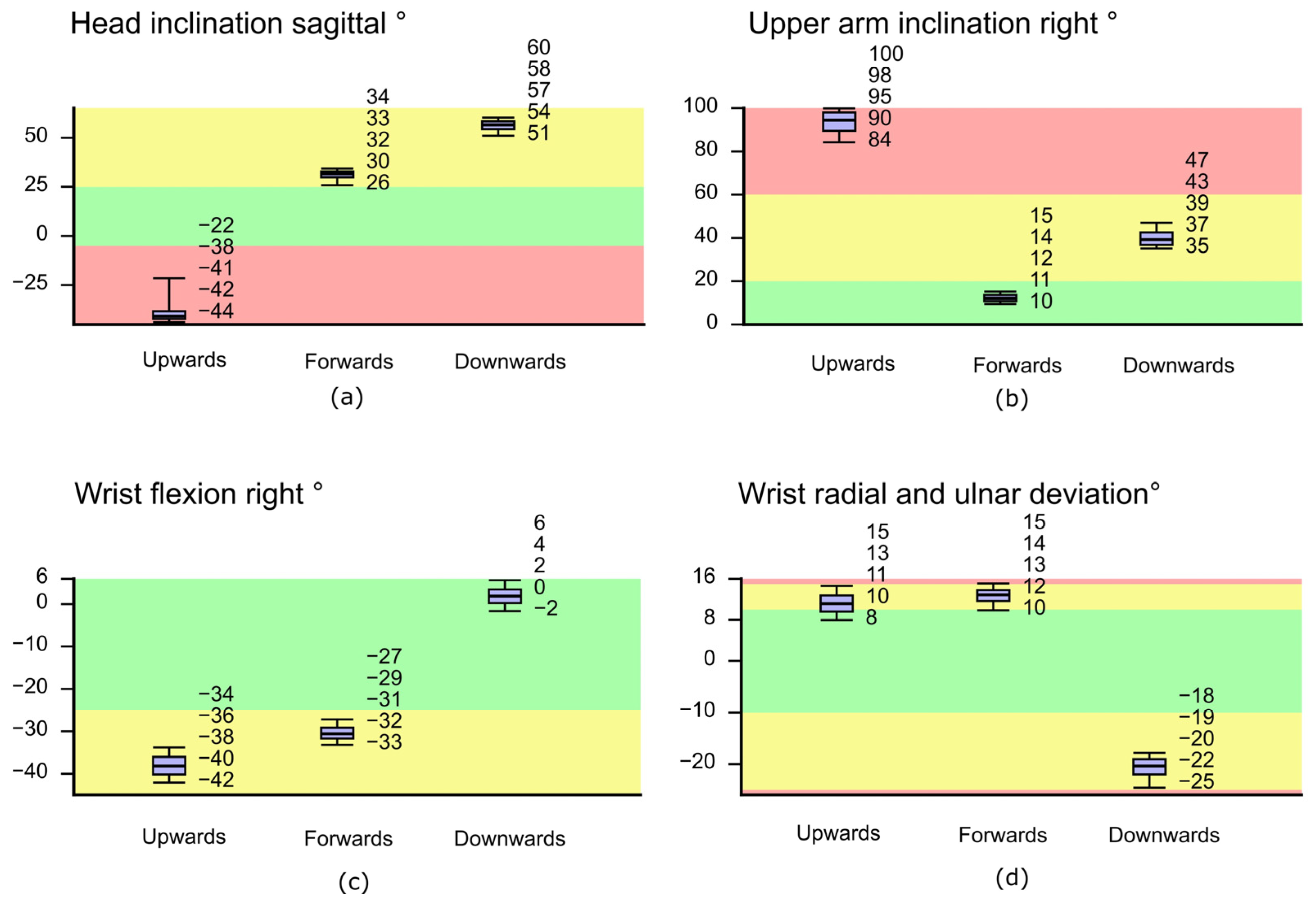
Table 1 depicts the angles which will be presented in this paper along with the associated categories for neutral, moderate, and awkward movement ranges. The results are shown as a boxplot distribution of all detected data with respect to these color-coded risk categories (5th, 25th, 50th, 75th and 95th percentile).
2.5. Electromyography
A wireless bipolar surface Electromyography (sEMG) measuring system, Cometa Wave Plus was used to analyze muscle activity. Surface electrode placement (Ambu
®, BlueSensor, Ballerup, Denmark) and skin preparation followed the SENIAM guidelines [
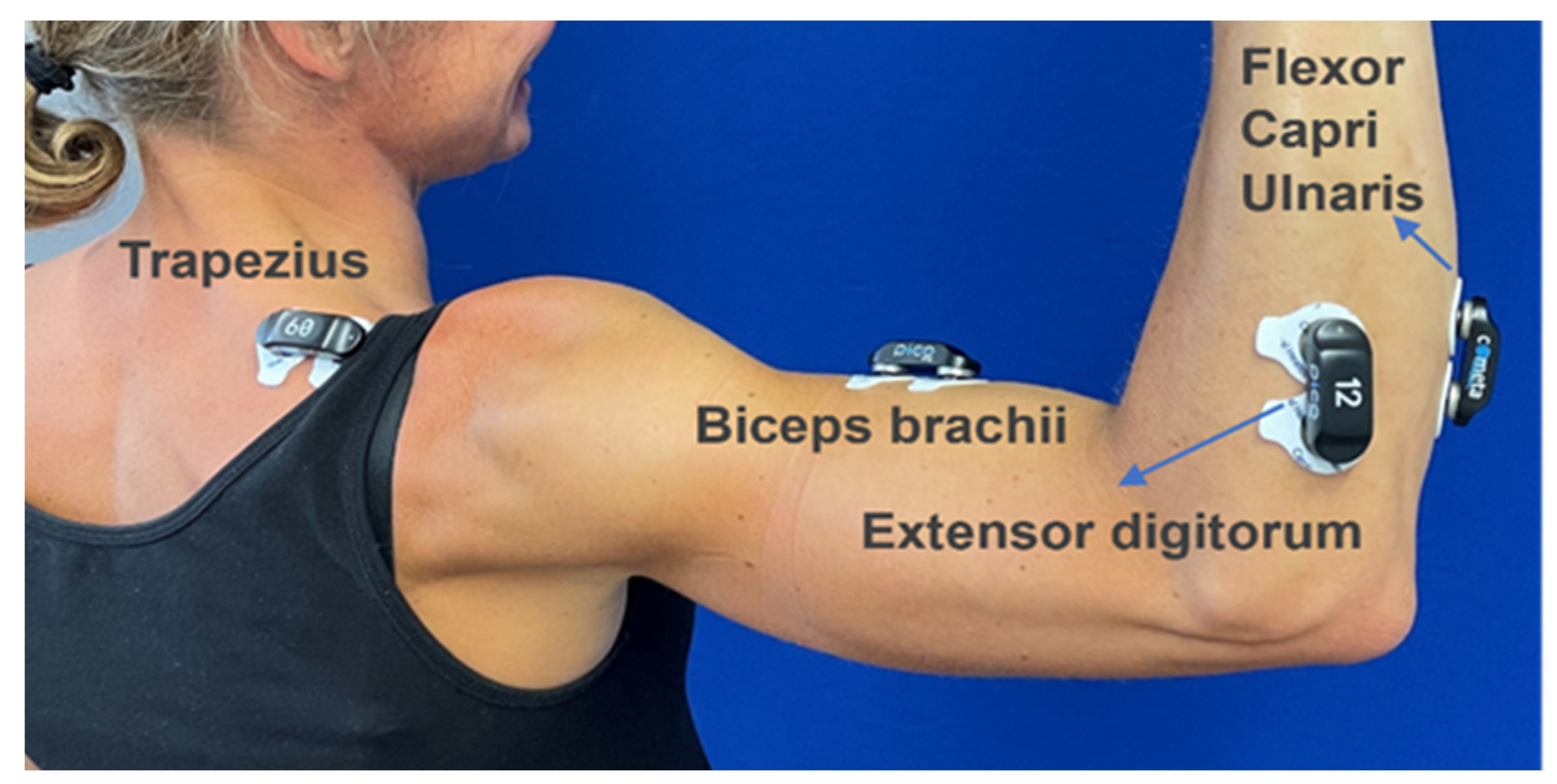
21]. The measurements were performed with Ag/AgCL electrodes (Kendall H 124 SG, Dublin, OH, USA). Since all subjects were right-handed, four transducers were placed on the right-hand side of the hand-arm system. Two pairs of adhesive circular surface electrodes were applied with a diameter of 24 mm (
Figure 3).
For M. trapezius descendens, electrodes were placed at 50% on the line from the acromion to the spine on vertebra C7. For M. biceps brachii, electrodes were placed on the line between the medial acromion and the fossa cubit at 1/3 from the fossa cubit [
21].
M. flexor carpi ulnaris and M. extensor digitorum were chosen as indicators for muscle activity during the chosen task. The electrodes for forearm muscles were applied to the most prominent part of the muscles, approximately one-third of the distance from the lateral epicondyle to the ulnar styloid [
17].
All sEMG signals were sampled at a frequency of 2000 Hz. Following the recommendations for the processing of the EMG data of Hansson et al. 1997 [
22], a bandpass filtering of 30–400 Hz and a RMS calculation was carried out with a rectangular window (window width of 0.125 s).
The percentage value (MVCP) was calculated from the RMS channels based on the maximum voluntary contraction (MVC values) of the individual muscles.
2.6. Subjective Perception of the Exposures
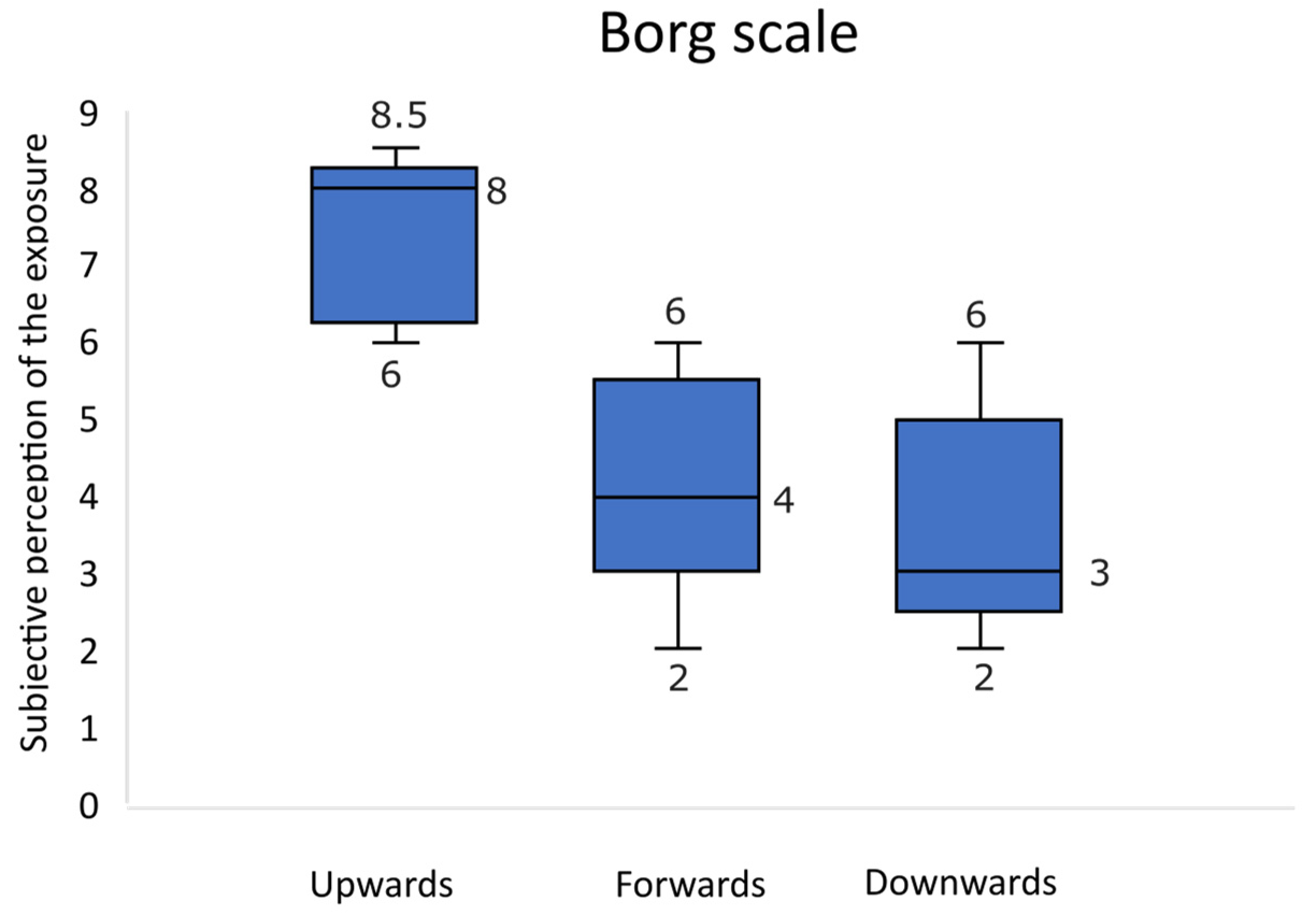
To assess the perceived exertion for the individual test sections, the modified Borg CR10 scale was used [
23]. In
Figure 4, the classification of the perception after being questioned: “how was the effort felt” is depicted, ranging from 0 for “absolutely nothing” to 10 for “extremely strong” is demonstrated.
2.7. Data Analysis and Statistics
Both, EMG and HAV measurement data were exported to the CUELA software (2022/V8) for the evaluation of vibration exposure and assessment of body posture following synchronization with body angles and video data [
20]. The statistical analysis of the data was performed with IBM SPSS Statistics 26 software.
This experiment was designed as a counter -balanced trial. A priori case calculations were not conducted.
As a measure of the central tendency, mean values were calculated for continuous variables and the SD as a measure of dispersion. Boxplots are used to describe the dispersion of the data. The Shapiro-Wilk test and additional histogram tests were used for all data to analyze the normal distribution. For normally distributed data, the influences of the posture on the vibration, EMG data and subjective perception are tested via one-way analysis of variance. A subsequent Tukey post hoc test is used for finding significant differences between groups with equal variance, while the Games-Howell post hoc test is used for groups with no equal variance. In the case of no normal distribution, the Kruskall-Wallis test is used for finding stochastic differences between groups, followed by a Dunn-Bonferroni post hoc test.
4. Discussion
With an average exposure duration of 5.8 to 6.3 s for each experimental screwing task, there was also no statistically significant difference between HAV exposures along the measurement axis (x, y and z).
According to the manufacturer technical specifications, the vibration exposure of the wrench for tightening of bolts and nuts of maximum allowable size is about 11.5 m/s2. In comparison to this information, the measured total vibration exposures for the used power tool were much lower, while driving screws into wood (4.4–4.8 m/s2), which is probably due to the material (wood instead of metal).
In contrast to the study by Taylor et. al. [
12] in which tool vibrations differed significantly for the various working directions, no significant difference was seen for vibration exposure while working in three directions in this trial. This could also be due to the different type of substrate provided in the experiments. In this study, we used a pre-cast wood plank, whereas the screwing tasks were mainly conducted by rotatory drive. In the study by Taylor et al. [
12], a pre-cast concrete paving slab was used to analyze drilling tasks which might mainly require hammer action. The aspects of substrate and the mode of the operation such as rotating, hammering, or oscillating need to be considered in more detail in future studies. Thus, a greater range of tools with different specifications are needed to analyze the impact of the posture on the HAV. In a similar designed experiment however, Liljelind et al. 2011 [
4] found that different working posture during grinding operations does not appear to affect the level of HAV. In a subsequent study, significant determinants for HAV were defined by anthropometric measures, such as volume of the hands, maximum grip force and weight of the operator [
24]. These findings are consistent with our data in which HAV remained the same at different muscle loads.
For the posture data, there is generally a very small distribution of data within the measurements, which is probably due to the individual adjustment of the test setup in relation to body height of test subjects.
When looking at the risk categories, it is evident that the test subjects frequently adopted an awkward posture when working in the upwards direction. The observed body angles show that the upwards working direction particularly impacts head inclination, due to extension of the neck resulting from the need to look up, and the shoulders, due to the high level of shoulder flexion.
When looking at wrist flexion, the results show that the angles of flexion when working in the forwards and upwards directions are similar and lie in the moderate (yellow) range of motion. This hand position is adopted automatically when gripping the handle of the power tool. When using the tool to drive in screws, this leads to extension of the forearm in the direction of the back of the hand. When working in the downwards direction, the level of wrist flexion is improved, while a high level of ulnar deviation is seen, since the wrist needs to be in a highly angled position for the downwards screwdriving motion. These results are in good agreement with those of the studies by Besa et al. [
14], who also emphasized that the transfer of energy to the hand-arm system is dependent on the position of the wrist.
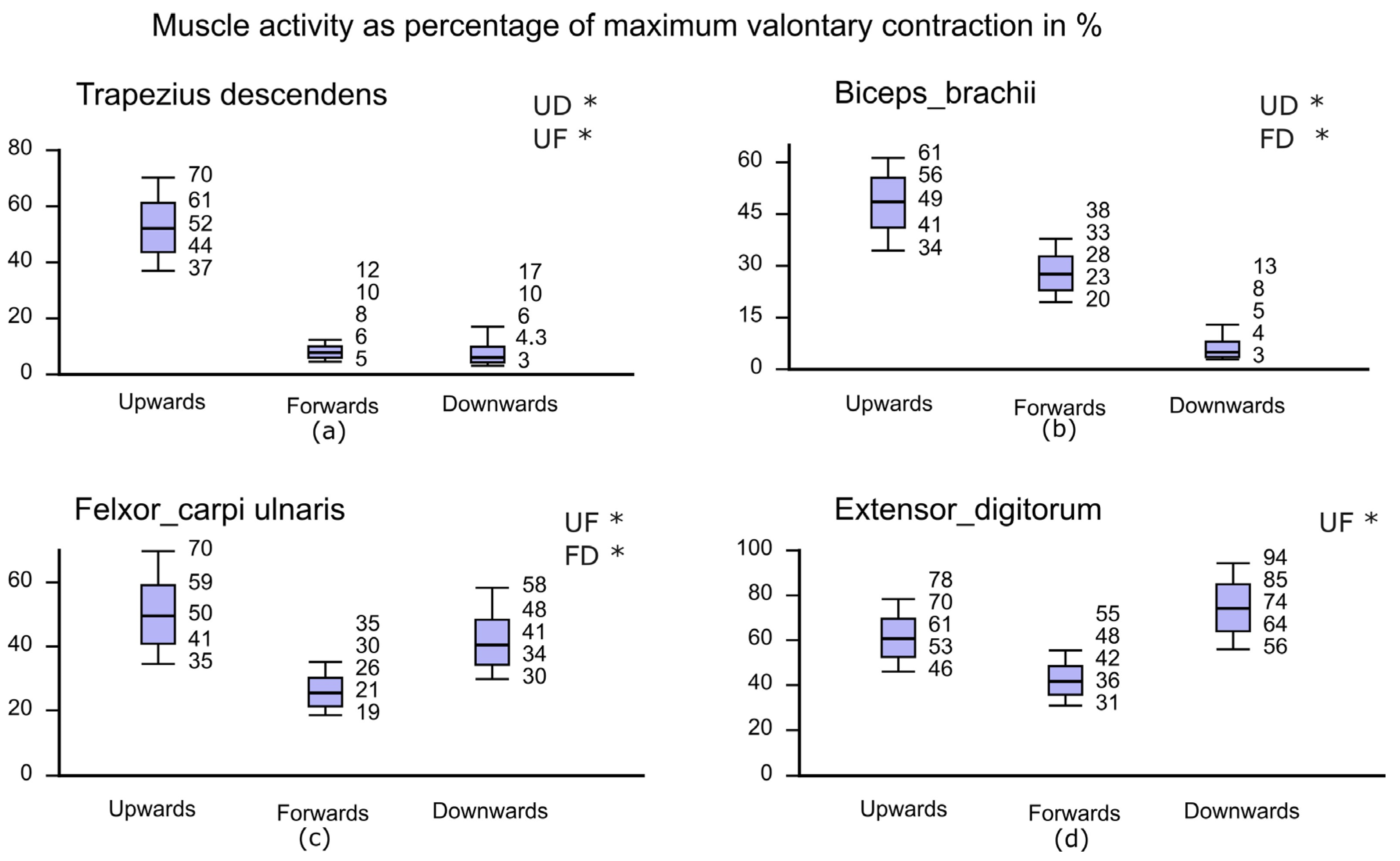
In relation to the MVCP values, the upwards working direction showed the highest level of muscle activity for the M. trapezius descendens, by far. This is due to the fact that the M. trapezius descendens plays a very important role in lifting the arms, since it must compensate for the weight of the arm and the machine and must provide a proportion of the feed force. When working in the forwards direction and downwards direction, the muscle activity in the M. trapezius descendens is very low, since lifting of the arms is not required, particularly in the case of downwards tests. When considering the data for upper arm inclination, a similar pattern can be seen. Therefore, in connection with the posture, a high level of work load for muscles of the shoulder girdle can be assumed when working in the upwards direction in particular.
For the M. biceps brachii, the results show that working in the upwards direction requires the highest level of muscle activity and that the level of muscle activity decreases in the forwards and downwards working directions. As a result, it can be assumed that, particularly when working in the upwards directions, the highest level of muscular force is provided by the M. biceps. The muscle activity in this muscle is lowest when working in the downwards direction, which corresponds to a lower level of muscular force provided.
Both the M. extensor digitorum and M. flexor carpi ulnaris show lower levels of activity in the forwards working direction compared to the upwards and downwards directions. This pattern was also observed for upper arm inclination.
With the M. flexor carpi ulnaris, the highest level of muscle activity was seen in the downwards working directions. This could be caused by the high level of radial deviation. These findings line up with the data from Besa et al. [
14] in that the resonance frequencies obtained for extreme wrist positions are higher than for the neutral position. Also, Dupuis et al. 1976 [
16] found that the reaction of the flexor carpi ulnaris is primarily determined by the grip pressure. Due to the lack of grip force measurements, it is not possible to interpret these forces in relation to EMG data and wrist postures. This should be considered in future studies.
In contrast to vibration data, the subjective data from the test participants regarding the levels of vibration exposure in three working directions showed high variance. While the levels of perceived vibration exposure were rated as medium for the forwards and downwards working directions, the vibration exposure when working in the upwards direction was rated as very strong. These findings align very well with the measured impacts especially of posture and muscular activity.
When thinking about workplace exposure assessments of combined exposures (as in our case, HAV and posture) by questioning employees, one should keep in mind that these efforts probably are more apt to assess awkward postures than exposures to vibration.
A good example for that is carpal tunnel syndrome, which is thought to arise from a combination of factors, such as vibration, mechanical stresses to tissues from forceful gripping, awkward postures, and repetitive movements [
25]. Therefore, to assess the risk of HAV exposure, musculoskeletal disorders of upper extremities among others, quantitative investigations of accompanying factors such as posture and coupling forces are needed [
26].





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}