Role of Multiparametric Magnetic Resonance Imaging and Targeted Biopsy in the Detection of Clinically Significant Prostate Cancer in Patients with Suspicious Digital Rectal Examination



 and
and
Abstract
1. Introduction
2. Methods
2.1. Patients
2.2. Prostate MRI
2.3. Prostate Biopsy
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Poppel, H.; Hogenhout, R.; Albers, P.; van den Bergh, R.C.; Barentsz, J.O.; Roobol, M.J. A European Model for an Organised Risk-stratified Early Detection Programme for Prostate Cancer. Eur. Urol. Oncol. 2021, 4, 731–739. [Google Scholar] [CrossRef]
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Eberli, D.; De Meerleer, G.; De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; et al. EAU Guidelines on Prostate Cancer 2023. Available online: www.uroweb.org (accessed on 27 August 2023).
- Mazzone, E.; Stabile, A.; Pellegrino, F.; Basile, G.; Cignoli, D.; Cirulli, G.O.; Sorce, G.; Barletta, F.; Scuderi, S.; Bravi, C.A.; et al. Positive predictive value of prostate imaging reporting and data system version 2 for the detection of clinically significant prostate cancer: A systematic review and meta-analysis. Eur. Urol. Oncol. 2021, 4, 697–713. [Google Scholar] [CrossRef]
- Morote, J.; Borque-Fernando, A.; Triquell, M.; Campistol, M.; Celma, A.; Regis, L.; Abascal, J.M.; Servian, P.; Planas, J.; Mendez, O.; et al. A clinically significant prostate cancer predictive model using digital rectal examination prostate volume category to stratify initial prostate cancer suspicious and reduce magnetic resonance imaging demand. Cancers 2022, 14, 5100. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef]
- Porpiglia, F.; Manfredi, M.; Mele, F.; Cossu, M.; Bollito, E.; Veltri, A.; Cirillo, S.; Regge, D.; Faletti, R.; Passera, R.; et al. Diagnostic pathway with multiparametric magnetic resonance imaging versus standard pathway: Results from a randomized prospective study in biopsy-naïve patients with suspected prostate cancer. Eur. Urol. 2017, 72, 282–288. [Google Scholar] [CrossRef]
- Morote, J.; Celma, A.; Roche, S.; de Torres, I.M.; Mast, R.; Semedey, M.E.; Regis, L.; Planas, J. Who benefits from multiparametric magnetic resonance imaging after suspicion of prostate cancer? Eur. Urol. Oncol. 2019, 2, 664–669. [Google Scholar] [CrossRef]
- Omri, N.; Alex, S.; Jacob, B.; Ofer, N. The additive value of mpMRI on prostate cancer detection: Comparison between patients with and without a suspicious digital rectal examination. Urol. Oncol. 2021, 39, 728.e7–728.e11. [Google Scholar] [CrossRef]
- Turkbey, B.; Brown, A.M.; Sankineni, S.; Wood, B.J.; Pinto, P.A.; Choyke, P.L. Multiparametric prostate magnetic resonance imaging in the evaluation of prostate cancer. CA Cancer J. Clin. 2016, 66, 326–636. [Google Scholar] [CrossRef]
- Ficarra, V.; Novella, G.; Novara, G.; Galfano, A.; Pea, M.; Martignoni, G.; Artibani, W. The potential impact of prostate volume in the planning of optimal number of cores in the systematic transperineal prostate biopsy. Eur. Urol. 2005, 48, 932–937. [Google Scholar] [CrossRef]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; ISUP Grading Committee. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostate Cancrinoma: Definition of grading patients and proposal for a new grading system. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Carroll, P.; Coley, C.; McLeod, D.; Schellhammer, P.; Sweat, G.; Wasson, J.; Zietman, A.; Thompson, I. Prostate-specific antigen best practice policy-part 1: Early detection and diagnosis of prostate cancer. Urology 2001, 57, 217–224. [Google Scholar] [CrossRef]
- Carvalhal, G.F.; Smith, D.S.; Mager, D.E.; Ramos, C.; Catalona, W.J. Digital rectal examination for detecting prostate cancer at prostate specific antigen levels of 4 ng/ml or less. J. Urol. 1999, 161, 835–839. [Google Scholar] [CrossRef]
- Okotie, O.T.; Roehl, K.A.; Han, M.; Loeb, S.; Gashti, S.N.; Catalona, W.J. Characteristics of prostate cancer detected by digital rectal examination only. Urology 2007, 70, 1117–1120. [Google Scholar] [CrossRef]
- Gosselaar, C.; Roobol, M.J.; Roemeling, S.; Schröder, F.H. The role of digital rectal examination in subsequent visits in the European randomized study of screening for prostate cancer (ERSPC). Eur. Urol. 2008, 54, 581–588. [Google Scholar] [CrossRef]
- Borden, L.S.; Wright, J.L.; Kim, J.; Latchamsetty, K.; Porter, C.R. An abnormal digital rectal examination is an independent predictor of Gleason 7 prostate cancer in men undergoing initial prostate biopsy: A prospective study of 790 men. BJU Int. 2007, 99, 559–563. [Google Scholar] [CrossRef]
- Thompson, I.M.; Ankerst, D.P.; Chi, C.; Goodman, P.J.; Tangen, C.M.; Lucia, M.S.; Feng, Z.; Parnes, H.L.; Coltman, C.A., Jr. Assessing prostate cancer risk: Results from the Prostate Cancer Prevention Trial. J. Natl. Cancer Inst. 2006, 98, 529–534. [Google Scholar] [CrossRef]
- Naji, L.; Randhawa, H.; Sohani, Z.; Dennis, B.; Lautenbach, D.; Kavanagh, O.; Bawor, M.; Banfield, L.; Profetto, J. Digital rectal examination for prostate cancer screening in primary care: A systematic review and meta-analysis. Ann. Fam. Med. 2018, 16, 149–154. [Google Scholar] [CrossRef]
- Andersson, J.; Palsdottir, T.; Lantz, A.; Aly, M.; Grönberg, H.; Egevad, L.; Eklund, M.; Nordström, T. Digital rectal examination in Stockholm3 biomarker-based prostate cancer screening. Eur. Urol. Open Sci. 2022, 44, 69–75. [Google Scholar] [CrossRef]
- Wegelin, O.; van Melick, H.H.E.; Hooft, L.; Bosch, J.R.; Reitsma, H.B.; Barentsz, J.O.; Somford, D.M. Comparing Three Different Techniques for Magnetic Resonance Imaging-targeted Prostate Biopsies: A Systematic Review of In-bore versus Magnetic Resonance Imaging-transrectal Ultrasound fusion versus Cognitive Registration. Is There a Preferred Technique? Eur. Urol. 2017, 71, 517–531. [Google Scholar] [CrossRef]
- Monda, S.M.; Vetter, J.M.; Andriole, G.L.; Fowler, K.J.; Shetty, A.S.; Weese, J.R.; Kim, E.H. Cognitive Versus Software Fusion for MRI-targeted Biopsy: Experience Before and After Implementation of Fusion. Urology 2018, 119, 115–120. [Google Scholar] [CrossRef]
- Turkay, R.; Inci, E.; Yildiz, O.; Ozgur, E.; Taşci, A. Cognitive Versus Magnetic Resonance-Ultrasound Fusion Prostate Biopsy: Which One Is Worthier to Perform? Ultrasound Q 2020, 36, 345–349. [Google Scholar] [CrossRef]
- Hayes, M.; Bassale, S.; Chakiryan, N.H.; Boileau, L.; Grassauer, J.; Wagner, M.; Foster, B.; Coakley, F.; Isharwal, S.; Amling, C.L.; et al. Selecting patients for magnetic resonance imaging cognitive versus ultrasound fusion biopsy of the prostate: A within-patient comparison. BJU Compass 2022, 3, 443–449. [Google Scholar] [CrossRef]
- Yamada, Y.; Shiraishi, T.; Ueno, A.; Ueda, T.; Fujihara, A.; Naitoh, Y.; Hongo, F.; Ukimura, O. Magnetic resonance imaging-guided targeted prostate biopsy: Comparison between computer-software-based fusion versus cognitive fusion technique in biopsy-naïve patients. Int. J. Urol. 2020, 27, 67–71. [Google Scholar] [CrossRef]
- Marra, G.; Ploussard, G.; Futterer, J.; Valerio, M.; EAU-YAU Prostate Cancer Working Party. Controversies in MR targeted biopsy: Alone or combined, cognitive versus software-based fusion, transrectal versus transperineal approach? World J. Urol. 2019, 37, 277–287. [Google Scholar] [CrossRef]



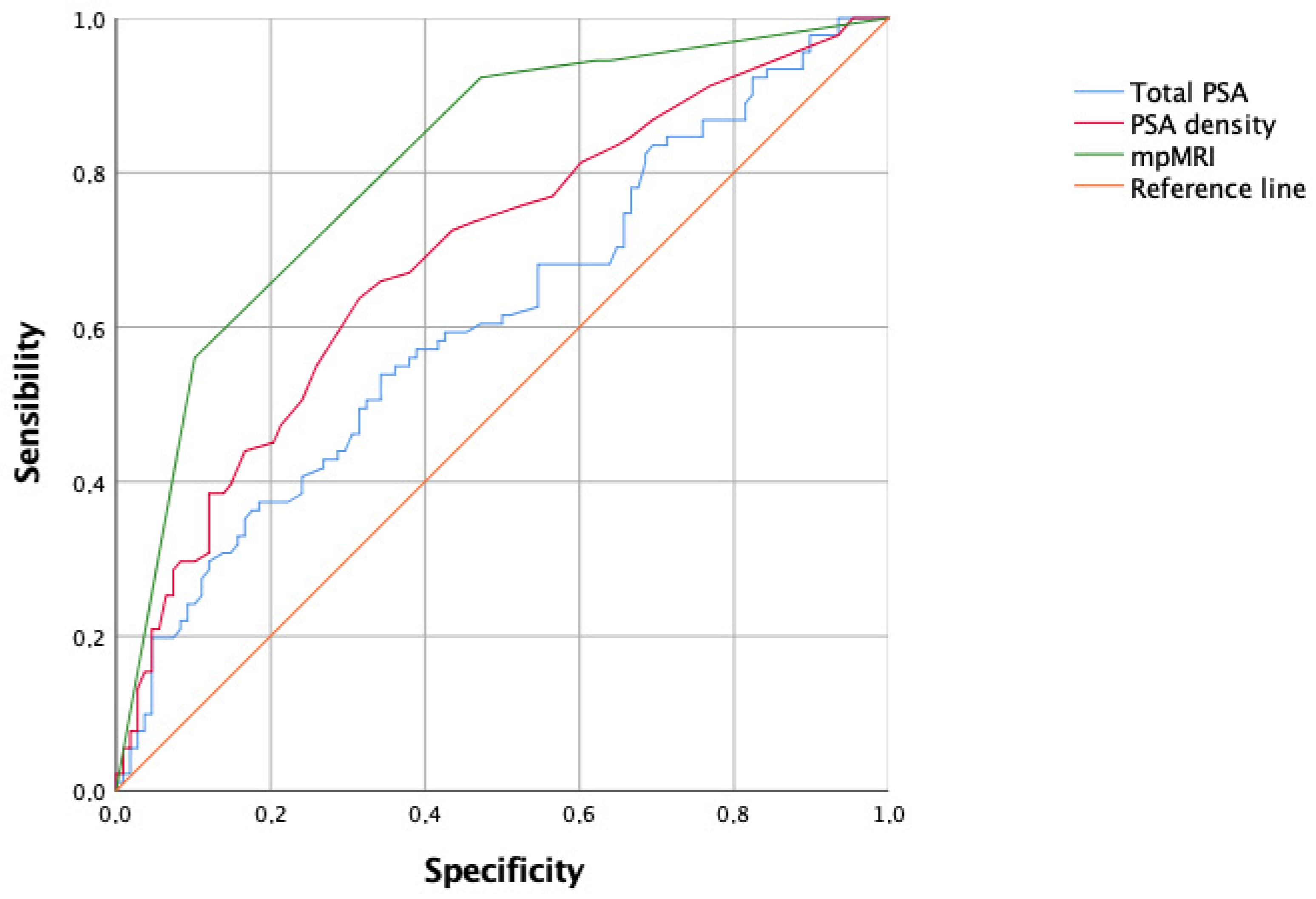{kind=link}
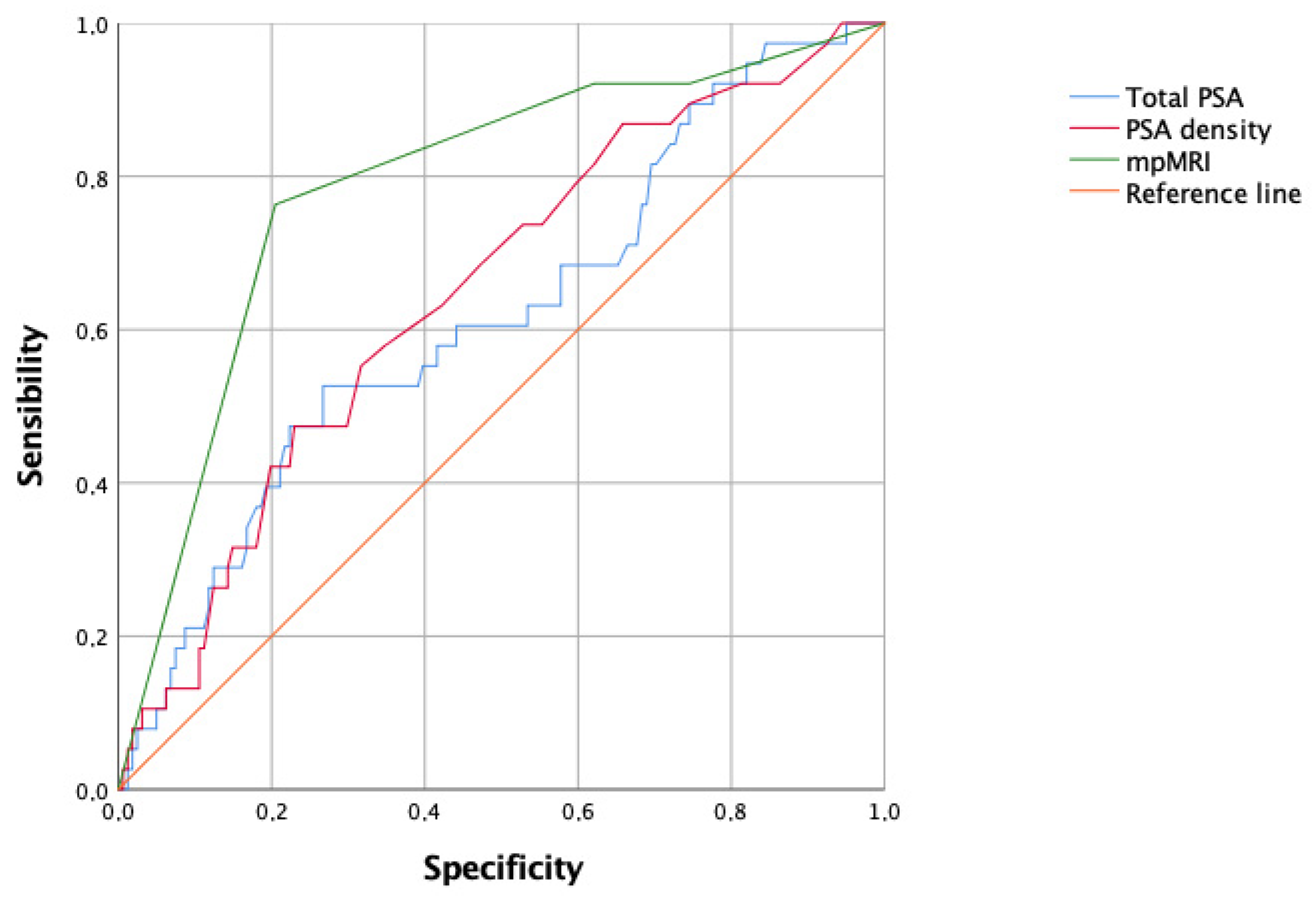{kind=link}
| Variable | Value |
|---|---|
| Median (IQR) age (years) | 68 (63–74) |
| Median (IQR) serum PSA level (ng/mL) | 7.9 (5.3–13.5) |
PSA categories, n (%)
| 127 (63.8%) 46 (23.1%) 26 (13.1%) |
| Median (IQR) prostate volume (cc) | 50 (40–67) |
| Median (IQR) PSAD (ng/mL/cc) | 0.16 (0.08–0.28) |
PSAD categories, n (%)
| 96 (48.2%) 103 (51.8%) |
PI-RADS v2.1 categories, n (%)
| 46 (23.1%) 18 (9%) 73 (36.7%) 62 (31.2%) |
| PSA (ng/mL) | PSAD (ng/mL/cc) | Size of the Index Lesion (mm) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| PI-RADS v2.1 categories | ≤10 | 10.1–20 | >20 | p value | ≤0.15 | >0.15 | p value | Median (IQR) | p value |
| 1–2 (n = 46) | 33 (71.7%) | 9 (19.6%) | 4 (8.7%) | <0.001 | 29 (63%) | 17 (37%) | 0.002 | N.A. | <0.001 |
| 3 (n = 18) | 11 (61.1%) | 6 (33.3%) | 1 (5.6%) | 11 (61.1%) | 7 (38.9%) | 8 (7–12) | |||
| 4 (n = 73) | 55 (75.3%) | 14 (19.2%) | 4 (5.5%) | 38 (52.1%) | 35 (47.9%) | 12 (10–15) | |||
| 5 (n = 62) | 28 (45.2%) | 17 (27.4%) | 17 (27.4%) | 18 (29%) | 44 (71%) | 17 (14–24) | |||
| Total (n = 199) | 127 | 46 | 26 | 96 | 103 | 14 (12–18) | |||
| PI-RADS v2.1 Categories | Prostate Biopsy Outcomes | |||
|---|---|---|---|---|
| Negative (%) | Positive (Any Cancer) (%) | csPCa (%) | Aggressive PCa (%) | |
| 1–2 (n = 46) | 36 (78.2%) | 10 (21.7%) | 5 (10.9%) | 3 (6.5%) |
| 3 (n = 18) | 14 (77.8%) | 4 (22.2%) | 2 (11.1%) | 0 |
| 4 (n = 73) | 25 (34.2%) | 48 (65.8%) | 33 (45.2%) | 6 (8.2%) |
| 5 (n = 62) | 4 (6%) | 58 (93.5%) | 51 (82.3%) | 29 (46.8%) |
| Total (n = 199) | 79 (39.7%) | 120 (60.3%) | 91 (45.7%) | 38 (19.1%) |
| p value | <0.001 | <0.001 | <0.001 | |
| Variables | Categories | OR | 95%CI | p Value |
|---|---|---|---|---|
| Age | continuous | 1.016 | 0.975–1.059 | 0.45 |
| PSA | continuous | 0.999 | 0.992–1.007 | 0.87 |
| PSAD | <0.15 ng/mL/cc ≥0.15 ng/mL/cc | Referent 2.173 | 1.068–4.423 | 0.03 |
| PI-RADS v2.1 categories | 1–2 3 4 5 | Referent 0.861 6.288 29.515 | 0.148–5.009 2.154–18.354 9.158–95.128 | <0.001 |
| SBx | Total | |||
|---|---|---|---|---|
| All cases (n = 153) | TBx | Negative or insignificant PCa | Clinically significant PCa | Total |
| Negative or insignificant PCa | 67 (91.8%) | 17 (21.3%) | 84 (54.9%) | |
| Clinically significant PCa | 6 (8.2%) | 63 (78.7%) | 69 (45.1%) | |
| Total | 73 (100%) | 80 (100%) | 153 | |
| SBx | Total | |||
| Patients with PSA ≤ 10 ng/mL (n = 94) | TBx | Negative or insignificant PCa | Clinically significant PCa | Total |
| Negative or insignificant PCa | 46 (90.2%) | 13 (30.2%) | 59 (62.8%) | |
| Clinically significant PCa | 5 (9.8%) | 30 (69.8%) | 35 (37.2%) | |
| Total | 25 (100%) | 43 (100%) | 94 | |
| SBx | Total | |||
| Patients with PSA > 10 ng/mL (n = 59) | TBx | Negative or insignificant PCa | Clinically significant PCa | Total |
| Negative or insignificant PCa | 21 (95.5%) | 4 (10.8%) | 25 (42.4%) | |
| Clinically significant PCa | 1 (4.5%) | 33 (91.2%) | 34 (57.4%) | |
| Total | 22 (100%) | 37 (100%) | 59 | |
| SBx | Total | |||
|---|---|---|---|---|
| All cases (n = 153) | TBx | Negative or non-aggressive PCa | Aggressive PCa | Total |
| Negative or non-aggressive PCa | 118 (98.3%) | 5 (15.2%) | 123 (80.4%) | |
| Aggressive PCa | 2 (1.7%) | 28 (84.8%) | 30 (19.6%) | |
| Total | 120 (100%) | 33 (100%) | 153 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ficarra, V.; Buttitta, A.; Rossanese, M.; Alibrandi, A.; Anastasi, G.; Blandino, A.; Ieni, A.; Martini, M.; Giannarini, G. Role of Multiparametric Magnetic Resonance Imaging and Targeted Biopsy in the Detection of Clinically Significant Prostate Cancer in Patients with Suspicious Digital Rectal Examination. Soc. Int. Urol. J. 2024, 5, 122-132. https://doi.org/10.3390/siuj5020021
Ficarra V, Buttitta A, Rossanese M, Alibrandi A, Anastasi G, Blandino A, Ieni A, Martini M, Giannarini G. Role of Multiparametric Magnetic Resonance Imaging and Targeted Biopsy in the Detection of Clinically Significant Prostate Cancer in Patients with Suspicious Digital Rectal Examination. Société Internationale d’Urologie Journal. 2024; 5(2):122-132. https://doi.org/10.3390/siuj5020021
Chicago/Turabian StyleFicarra, Vincenzo, Alessandro Buttitta, Marta Rossanese, Angela Alibrandi, Giuseppina Anastasi, Alfredo Blandino, Antonio Ieni, Maurizio Martini, and Gianluca Giannarini. 2024. "Role of Multiparametric Magnetic Resonance Imaging and Targeted Biopsy in the Detection of Clinically Significant Prostate Cancer in Patients with Suspicious Digital Rectal Examination" Société Internationale d’Urologie Journal 5, no. 2: 122-132. https://doi.org/10.3390/siuj5020021
APA StyleFicarra, V., Buttitta, A., Rossanese, M., Alibrandi, A., Anastasi, G., Blandino, A., Ieni, A., Martini, M., & Giannarini, G. (2024). Role of Multiparametric Magnetic Resonance Imaging and Targeted Biopsy in the Detection of Clinically Significant Prostate Cancer in Patients with Suspicious Digital Rectal Examination. Société Internationale d’Urologie Journal, 5(2), 122-132. https://doi.org/10.3390/siuj5020021