Abstract
Objectives: Our objective was to assess the rate of complications and gastrointestinal adverse effects of rectal spacer insertion for salvage post prostatectomy radiation therapy. Methods: A retrospective observational study was performed. Between September 2018 and March 2022, 64 post-radical prostatectomy patients who were planned for salvage radiation therapy received a rectal spacer. The selected patients were those who had nerve-sparing prostatectomy with intrafascial or interfascial dissections (where Denonvillier’s fascia is retained). Radiation dose to the rectal wall and gastrointestinal symptoms were assessed. Symptoms were graded using the National Cancer Center Institute Common Terminology Criteria for Adverse Events v4.0 grading scheme. A total of 39 patients had pre-spacer planning computer tomography (CT) scans, and the rectal dose before and after the spacer insertion was calculated. Comparisons were made using the Student’s t-test, with a p-value < 0.05 representing statistical significance. Finally, clinicians were surveyed to rate the ease of the procedure using a 5-point Likert scale of 1 to 5 (1: very difficult, 2: difficult, 3: moderate, 4: easy, 5: very easy). Results: A total of 64 patients successfully underwent rectal spacer insertion. The mean age was 64.4 years (standard deviation: 5.7 years). After a median of 14 months’ (range 6 to 35) follow up, acute grade 1 and above gastrointestinal (GI) toxicities were seen in 28% of patients (grade 2 in 1.5%), and late grade 1 and above GI toxicities were seen in 12% of patients (grade 2 in 1.5%). Amongst the 39 patients with pre-spacer planning CT images, the volume of the rectum receiving 60%, 70%, 80%, 90%, and 100% of the prescribed radiation dose was reduced by 25.9%, 34.2%, 35.4%, 43.7%, and 61.7%, respectively. All dose reductions were statistically significant. The procedure was rated as “easy” or “very easy” to perform in 56% of cases. Conclusions: The insertion of a rectal spacer in selected patients undergoing PPRT is feasible and safe and significantly improves rectal wall radiation dosimetry in salvage post prostatectomy radiation therapy. It was accomplished in >95% of patients, increasing vesico-rectal separation from ‘immediate vicinity’ to 11 mm without any post-operative complications in experienced hands. In addition, it achieved significant reduction in rectal radiation doses, leading to low rates of acute and late grade 2 toxicity.
1. Introduction
Biochemical recurrence after radical prostatectomy is estimated to occur in 20% to 40% of patients with prostate cancer [1]. Salvage post prostatectomy radiation therapy (PPRT) is a potentially curative treatment in this patient cohort [1]. However, significant gastrointestinal (GI) side effects from high-dose radiation to the rectal wall is a dose limiting factor [2]. The risk of significant late grade 2 GI toxicity varies from 8% to 14% [3,4,5]. The SAKK09/10 study reported a combined 11.5% risk of late grade 2–3 GI toxicity at 64Gy with a doubling of toxicity when the dose was escalated to 70 Gy [6]. The rates of grade 2–3 GI toxicity were higher than what we would expect for intact prostates despite a lower dose of radiation. This is not surprising as the posterior border of the area for radiation therapy or clinical target volume (CTV) is placed at the mesorectal fascia (usually anterior rectal wall) superiorly above the pelvic floor. To safely deliver radiation and reduce the radiation dose to the rectum, the placement of a spacer between the target anatomy (prostate bed) and the rectum may be considered [7].
There are several changes in bladder and rectal anatomy following a prostatectomy that require consideration before the insertion of a rectal spacer [8]. Spacer placement in the treatment naïve patient consists of identifying the perirectal fat situated posterior to Denonvillier’s fascia and anterior to the fascia propria of the rectum. After a prostatectomy, however, there are several changes to the anatomy in this area. Firstly, the prostate is no longer present, and the Denonvillier’s fascia may be resected in the setting where there is concern about T3 disease posteriorly. Secondly, consideration needs to be given to the location of recurrence. The anastomotic site represents the most common area of recurrence, followed by the bladder neck and rectovesical regions [9]. Given the potential difficulties in the insertion of a rectal spacer in the post-prostatectomy setting, there are minimal data reporting on the technique, the success of this procedure, the procedural complication rates, and its effectiveness in reducing the rectal dose.
There are limited data in the current literature regarding rectal spacer insertion in the post-prostatectomy setting. Despite this, the scant evidence suggests significant improvements in GI symptoms with spacer insertion [10]. As such, we perform a retrospective analysis to report on a cohort of patients who received rectal spacing prior to salvage radiation therapy with the aim of assessing the rates of complications and GI adverse effects.
2. Methods
2.1. Study Population
After institutional ethics approval (GenesisCare Office of Research approval number 2022/ETH00247), a retrospective analysis of patients undergoing salvage PPRT and rectal spacer insertion between September 2018 and March 2022 was performed. Indications for post-prostatectomy radiation therapy (PPRT) included biochemical recurrence with a rising PSA in patients with known extracapsular extension, seminal vesicle involvement, or positive margins. Patients considered for rectal spacer insertion also had prior nerve-sparing prostatectomy with intrafascial or interfascial dissections. This is important as Denonvillier’s fascia will be retained along with the perirectal fat. Patients who had extrafascial dissections were not considered for rectal spacing. In addition, this cohort of patients also did not have metastatic or macroscopic local recurrence detected on their prostate-specific membrane antigen positron emission tomography (PSMA-PET) imaging, and as such, the prostate bed was targeted.
2.2. Rectal Spacer and Technique
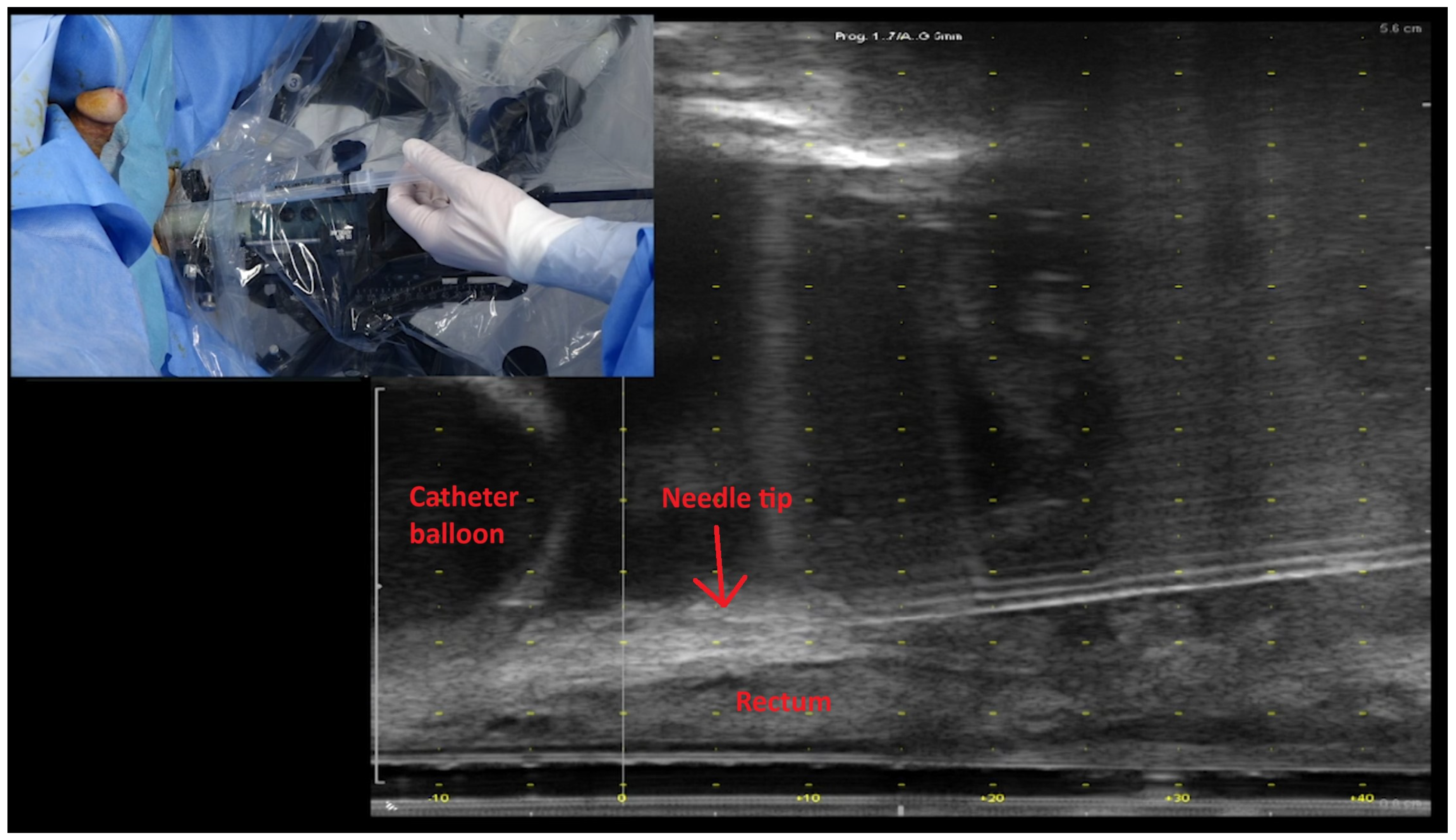
Patients underwent rectal spacing with either hyaluronic acid (Barrigel®, Palette Life Sciences, Santa Barbara, CA, USA) or hydrogel (SpaceOAR®, Boston Scientific, Massachusetts, Marlborough, MA, USA). The insertion technique is demonstrated in Figure 1. The rectal spacer was inserted into the perirectal fat posterior to the retained Denonvillier’s fascia between the bladder and anterior rectal wall using a transperineal approach under TRUS guidance. An indwelling urinary catheter was inserted to help delineate the vesico-urethral anastomosis (VUA). The perirectal fat was identified between the bladder and anterior rectum. An 18G spinal needle (Quincke Type Point® Spinal Needle, BD, Stockholm, Sweden) was inserted using a freehand technique targeting the midline of the prostate bed under sagittal TRUS guidance. Hydrodissection of the perirectal fat in the sagittal midline with 3 to 5 mL of sterile saline was attempted and, if successful, followed by insertion of 6 to 9 mL of hyaluronic acid (66% of cases) or hydrogel. After insertion, the vesico-rectal separation was calculated by measurement at the midline of spacer’s sagittal length. Pre- and post-spacer insertion images can be seen in Figure 2.
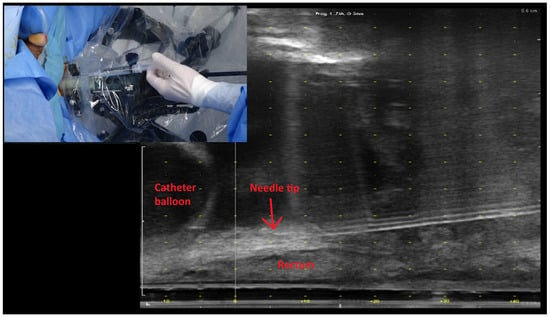
Figure 1.
Ultrasound image demonstrating the insertion of needle to the level of the vesico-ureteric anastomosis and just prior to hydrodissection and its relationship to the rectum and bladder neck (as outlined by the catheter balloon). Inset: transperineal approach for insertion of rectal spacer; here, the syringe contains normal saline ready for hydrodissection.
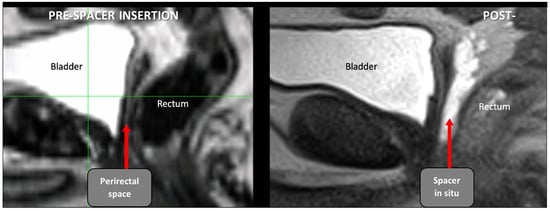
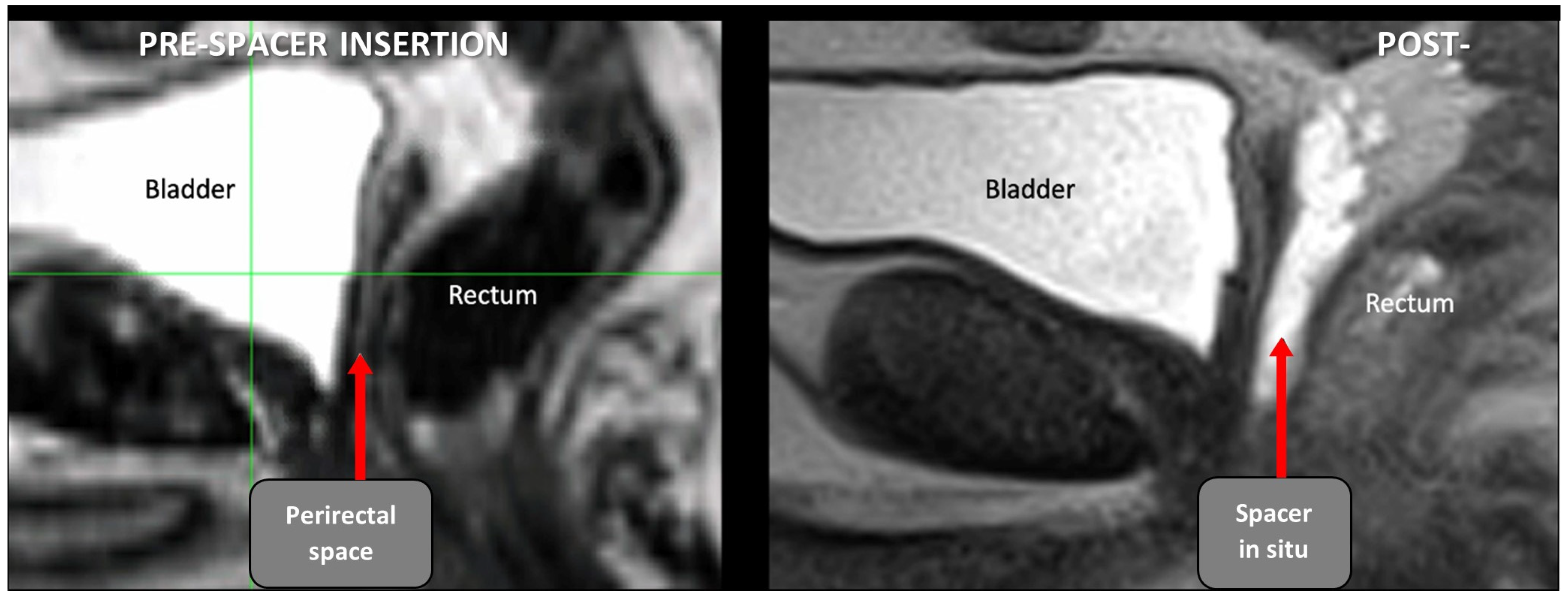
Figure 2.
Pre- and post-spacer insertion MRI images (sagittal) with hyaluronic acid in perirectal space extending just above pelvic floor.
2.3. Radiation Therapy
A total of 39 patients had a pre-spacer computerized tomography (CT) scans available for assessment. These are not routine but conducted as planning CT scans prior to a patient-led decision change regarding rectal spacer insertion. Pre- (when available) and post-perirectal spacer CT planning scans, together with post-perirectal spacer MRI scans, were acquired for dosimetric comparison (see Figure 3). The prostate bed CTV was delineated according to standard Australian guidelines [11], and the CTV was uniformly expanded by 7 mm [12] to create the planning target volume (PTV). The prescribed dose to the prostate bed was 70.2 Gy in 1.8 Gy fractions using volumetric arc radiation therapy [12]. Given PSMA-PET scans were negative in these patients, pelvic lymph nodes were not included in the radiation. The PTV and rectal dosimetry for the two sets of CT planning scans (PTV 7 mm/pre spacer and PTV 7 mm/post spacer) were compared.
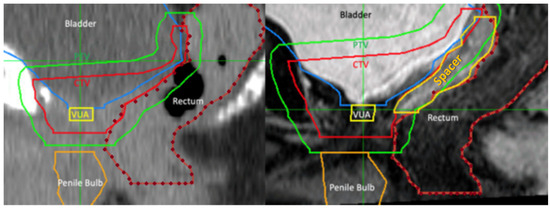
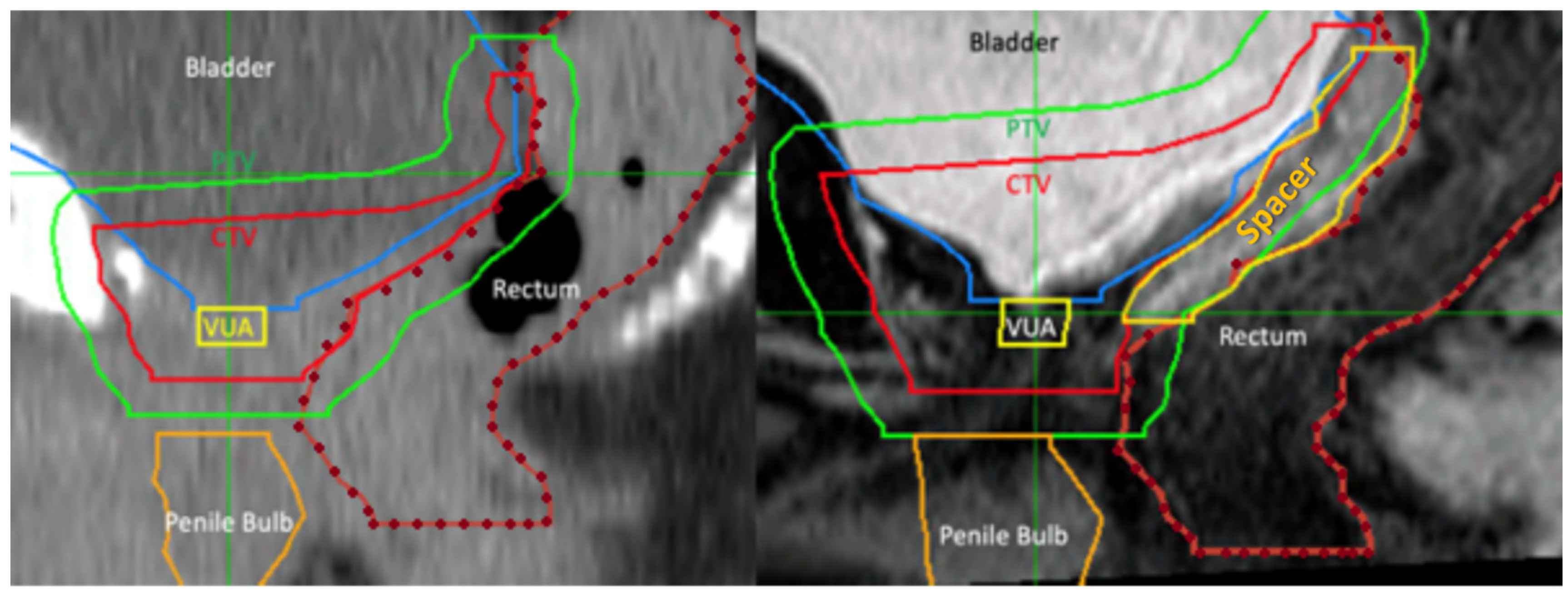
Figure 3.
Comparison of planned radiation area (green line) in the same patient pre- and post-rectal spacer insertion. Prior to spacer insertion, a long length of rectal wall (delineated by dotted orange line) was exposed to high dose radiation. This decreased by the use of hyaluronic acid spacer (yellow line). Abbreviations: CTV—clinical tumour volume, PTV—planning tumour volume, VUA—vesicoureteric anastomosis.
2.4. Radiation Toxicities
Baseline symptoms relating to the GI tract were assessed. After radiation therapy, the patients were assessed for acute toxicity at two weeks and three months (≤3 months of radiation) and late toxicity at six months, and then every six months of their follow up (>3 months of radiation). The severity of each GI toxicity was graded based on the National Cancer Center Institute Common Terminology Criteria for Adverse Events v4.03 grading scheme [13].
2.5. Study Endpoints
The primary endpoint was the incidence of peri-operative complications and acute and chronic GI toxicity with rectal spacer in the post-prostatectomy radiation setting. Secondary endpoints included rectal dosimetry reduction, separation created by rectal spacer, change or interruption to radiation therapy, and ease of procedure as rated by the clinician. Rectal dosimetry reductions are reported at rV100%, rV90%, rV80%, rV70%, and rV60% in concordance with previous large, randomised control trials [14,15].
2.6. Data Collection and Analysis
Retrospective data were collected, including patient demographics, pre-prostatectomy serum PSA, pre-prostatectomy MRI findings, clinical staging, pathological staging, histology, and margin positivity. Once the rectal spacer was inserted, each case was rated by the operator on ease of spacer application based on a Likert scale of 1 to 5 (1: very difficult, 2: difficult, 3: moderate, 4: easy, 5: very easy).
For patients who had pre-spacer planning scans, rectal dosimetric comparisons were performed, and percentage reduction was assessed. The Student’s t-test was used for comparison, and statistical significance was defined as a p-value of <0.05. Patients were reviewed at two weeks, three months, six months, and then at intervals of six months post-PPRT.
3. Results
Between September 2018 and March 2022, a total of 67 patients underwent attempted rectal spacer insertion before their PPRT. Sixty-four patients underwent successful insertions of rectal spacers under general anaesthesia. Three patients did not receive a rectal spacer as the hydrodissection of the perirectal plane was unsuccessful. There were no post-operative complications reported. Thirty-nine patients had undergone pre-spacer insertion planning scans and were available for radiation dosimetry comparisons pre- and post-spacer insertion.
The patient cohort characteristics are summarised in Table 1. The mean age of the cohort was 64.4 years (SD: 5.7 years). All underwent radical prostatectomies and had experienced biochemical recurrence with a median PSA of 0.2 nmol/mL. A PSMA-PET/CT was performed, and there were no areas of avidity; thus, the prostate bed was targeted for radiation therapy. Neoadjuvant androgen deprivation therapy was initiated in 75% of patients.

Table 1.
Patient characteristics and perioperative factors.
The pre- and post-spacer insertion characteristics are summarised in Table 2. The distance between the bladder and rectal wall increased from ≤2 mm to a median of 11mm [9,10,11,12,13] at its greatest extent. Grade 1 rectal wall infiltration, as defined by Fisher-Valuck et al., was seen in 3% (2/67) [16]. These cases were asymptomatic and were monitored. Following rectal spacing, the rectal volume for all patients (N = 67) receiving 42.2 Gy (rV60%), 49.1 Gy (rV70%), 56.2 Gy (rV80%), 63.2 Gy (rV90%), and 70.2 Gy (rV100%) were 28.1%, 23%, 17.9%, 12.5%, and 3.8% respectively. A statistically significant reduction was seen on all rectal volume end points from rV60% to rV100% in the 39 patients with both pre- and post-rectal spacer CT planning scans (see Table 3).
Table 2.
Pre- and post-spacer insertion characteristics.
Table 3.
Volume of patients’ rectum exposed to radiation based on a planning treatment volume of 7 mm margin for the 39 patients with pre- and post-spacer CT scans. Student’s t-test was used for comparison of the p-values quoted.
All patients completed their planned PPRT. The median follow up was 14 months (range 6 to 35). Acute GI toxicity was reported in 28% of patients (G1 27% and G2 1%). Late GI toxicity was reported in 12% of patients (G1 10% and G2 1%). Acute GU toxicity was reported in 78% of patients (G1 72% and G2 6%). Late GU toxicity was reported in 25% of patients (G1 18% and G2 7%) (see Table 4). Recurrence was seen in five patients, with four being at a pelvic lymph node and one being a distant bony metastasis.
Table 4.
Functional toxicities and outcomes post radiation therapy with rectal spacer in situ.
4. Discussion
Radiotherapy is widely used as a treatment option for prostate cancer. However, the rectum, due to its close proximity, is a dose-limiting structure [17]. If the rectum receives a high dose of radiation, this can lead to complications such as bleeding, frequency, urgency or mucus discharge, and even mucosal ulceration and fistula. As a result, various injectable agents have been placed in the perirectal fat to provide physical distancing between the prostate and rectum, leading to a reduction in the volume of patients’ rectum receiving high doses of radiation and a significant reduction in acute and late GI toxicity [14,15,18,19,20]. PPRT can also be associated with significant rectal toxicity [4,5]. Thus, we postulate that the effects of rectal spacing can be extrapolated to benefit this group of patients.
Limited studies have examined the use of rectal spacers in the post-prostatectomy setting. A literature review has only identified a case report [21], a conference presentation [22], and a small study of 21 patients [10]. There were no reported comparisons of the volume of the rectum receiving radiation with or without a rectal spacer. However, there are two randomised studies in the intact prostate setting that have shown a significant reduction in volume of rectum receiving high-dose radiation. The hyaluronic acid spacer trial showed an 85% reduction in volume of rectum receiving 90% of the prescription dose (rV90%) [15]. Our PPRT rectal spacing results also showed a significant reduction in the rV90% by 43.7%. This variance in the absolute percentage of reduction in rV90% can be explained by two factors. Firstly, the difference in the radiation field margins set for PPRT versus patients with intact prostates (a bigger 7 mm planning target volume margin posteriorly in PPRT vs. 5 mm for intact prostate). Secondly, due to the anatomical changes following a radical prostatectomy, it was not possible to space the entire length of the radiation field for PPRT. A spacer can only be inserted above the pelvic floor at the level of the VUA and superiorly, whereas the radiation fields extended below this. Despite these challenges, the use of a rectal spacer for PPRT still resulted in a significant reduction in rV90%, well above the 25% mark achieved for intensity modulated radiation therapy. This reduction in the volume of rectum receiving high-dose radiation is thought to reduce GI toxicity in our cohort.
Whilst the radiation dose used on the rectum serves as a marker of potential side effects, patient-reported side effects are also a reflection of toxicity and could better represent quality of life. Without rectal spacing, salvage radiation therapy can be associated with both acute and late gastrointestinal toxicities. Acute grade 2 or higher toxicities have been reported at 4% [4], while late grade 2 or higher toxicities have been reported at 8%–10% [4,5]. All of these studies had reported patients with grade 3 adverse events. There are a limited number of studies on salvage radiation with rectal spacing. Pinkawa et al. reported on a patient who underwent successful insertion of a rectal spacer between the recurrence and the anterior rectal wall [21]. This patient experienced frequency of stools (grade 1 GI toxicity) in the acute setting, and no gastrointestinal toxicity at 8 months of follow up. Similarly, Yeh et al. reported 9 of 32 (28%) patients who developed grade 1 GI toxicity in the acute setting, with complete resolution in all but three patients (9%) at six months’ follow up [22]. Similarly, Lehrich et al. found 43% patients had experienced acute grade 1 GI toxicity during the radiation treatment. Late toxicity was defined as those present at 6 months after radiation treatment, and 14% and 5% of patients experienced grade 1 and grade 2 toxicity, respectively. The present study provides the largest dataset to date, and our results concur with the currently available data. Significant acute grade 2 or more GI toxicity was reported in 1% (1/67) of patients. Late grade 1 GI toxicity was reported in 10% (7/67) of patients ableit with a short median follow up. Furthermore, the worst GI toxicity experienced is grade 2 in severity, in comparison to the grade 3 or higher in previous reports [4,5]. As such, significant acute and late GI toxicity appears to be less common and less severe after rectal spacer insertion compared to PPRT patients without the use of rectal spacers [3,4,5,6].
Discussion regarding the process of spacer insertion in the post-prostatectomy setting is warranted, particularly given the concerns about feasibility [23]. Only patients who underwent a nerve sparing radical prostatectomy were considered for rectal spacing. A known intrafascial or interfascial dissection was a pre-requisite as this means Denonvillier’s fascia is retained and, with it, the perirectal fat behind it. It is this retained perirectal fat that we are inserting the rectal spacer into. If an extrafascial dissection is performed, by definition, this means Denonvillier’s fascia is removed and, with it, the perirectal fat behind it. Pinkawa et al. described the procedure as requiring “about 15 min” [21]; otherwise, there are currently no reports on the ease of rectal spacer placement in the post-prostatectomy setting. In the present study, we show that the majority of procedures (56%) were rated as “very easy” or “easy” on a 5-point Likert scale. Regardless of rating, all cases that were successfully hydrodissected also underwent successful insertions of rectal spacers with no immediate peri-procedural complications. The resultant vesico-rectal separation increased from immediate vicinity to a median distance of 11 mm. It should be noted that there were three cases where rectal spacer was not inserted as hydrodissection was unable to be achieved, and these were rated as “very difficult”. A further four cases were rated as “difficult” due to either thin perirectal fat or prominent rectal hump, resulting in a challenging needle entry and targeting of the perirectal fat layer. The above highlighted two points. Firstly, hydrodissection contributed to the safety of this procedure and should be an essential step. Secondly, despite post-operative changes and “difficult” ratings, an adequate separation of the rectum from the bladder above the pelvic floor can be achieved. These data reassure that with the correct training, this procedure can not only be used by widespread clinicians but also in a safe manner.
The present study had five (7%) patients with treatment failure at a median of 14 months follow up. This included four with nodal recurrence and one with distant bony metastatic disease. No patients had prostate bed recurrence. Current literature reports on the survival and progression of the disease often after three or five years of follow up, with 5-year progression-free survivals of 50.8% [24] and 68.4% [25] and a 6-year progression-free rate of 32% [26]. Our rate of progression is much lower. However, given our follow up period is considerably shorter, comparisons and conclusions of progression-free durations are difficult to draw. However, what can be compared is the location of disease progression. Lymph nodes are identified as a common site of treatment failure, which is followed by distant bony metastasis [27]. This is in concordance with our observed results.
Our study is not without limitations, with the main one being the lack of head-to-head comparisons of patient cohorts with and without a rectal spacer inserted. Notwithstanding this limitation, we provide the first analysis of the largest cohort of patients to undergo rectal spacer insertion for salvage radiation therapy in the post-prostatectomy setting.
5. Conclusions
Perirectal spacing in selected patients undergoing PPRT is feasible and safe and has the potential to reduce both acute and late GI toxicity. Successful perirectal spacing was completed in >95% of patients (64/67), increasing vesico-rectal separation from ‘immediate vicinity’ to 11 mm without any postoperative complications in experienced hands. In addition, it achieves significant reduction in rectal radiation doses. Both acute and late G2 toxicity is low, albeit with a short follow-up period.
Author Contributions
Conceptualization, D.A., M.C. (Michael Chao) and P.O.; methodology, M.C. (Michael Chao); formal analysis, M.C. (Michael Chao); investigation, T.P., D.A., D.P., D.L.J., A.T., K.M., Y.C., P.M., J.T., H.H., E.H., M.C. (Margaret Cokelek), N.L. and F.F.; resources, M.C. (Michael Chao) and P.O.; data curation, M.C. (Michael Chao); writing—original draft preparation, A.H.; writing—review and editing, A.H., M.C. (Michael Chao) and D.B.; visualization, M.C. (Michael Chao), A.H. and D.B.; supervision, M.C. (Michael Chao), D.B. and N.L.; project administration, M.C. (Michael Chao) and P.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of GenesisCare (approval number: 2022/ETH00247).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author (MC). The data are not publicly available to safeguard privacy of research participants.
Conflicts of Interest
Michael Chao and Peter Orio are consultants for Palette Life Sciences Pty Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Zaorsky, N.G.; Calais, J.; Fanti, S.; Tilki, D.; Dorff, T.; Spratt, D.E.; Kishan, A.U. Salvage therapy for prostate cancer after radical prostatectomy. Nat. Rev. Urol. 2021, 18, 643–668. [Google Scholar] [CrossRef] [PubMed]
- Leiker, A.J.; Desai, N.B.; Folkert, M.R. Rectal radiation dose-reduction techniques in prostate cancer: A focus on the rectal spacer. Future Oncol. 2018, 14, 2773–2788. [Google Scholar] [CrossRef] [PubMed]
- Parker, C.C.; Clarke, N.W.; Cook, A.D.; Kynaston, H.G.; Petersen, P.M.; Catton, C.; Cross, W.; Logue, J.; Parulekar, W.; Payne, H.; et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomised, controlled phase 3 trial. Lancet 2020, 396, 1413–1421. [Google Scholar] [CrossRef] [PubMed]
- Sargos, P.; Chabaud, S.; Latorzeff, I.; Magné, N.; Benyoucef, A.; Supiot, S.; Pasquier, D.; Abdiche, M.S.; Gilliot, O.; Graff-Cailleaud, P.; et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localised prostate cancer after radical prostatectomy (GETUG-AFU 17): A randomised, phase 3 trial. Lancet Oncol. 2020, 21, 1341–1352. [Google Scholar] [CrossRef] [PubMed]
- Kneebone, A.; Fraser-Browne, C.; Duchesne, G.M.; Fisher, R.; Frydenberg, M.; Herschtal, A.; Williams, S.G.; Brown, C.; Delprado, W.; Haworth, A.; et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomised, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020, 21, 1331–1340. [Google Scholar] [CrossRef] [PubMed]
- Ghadjar, P.; Hayoz, S.; Bernhard, J.; Zwahlen, D.R.; Hölscher, T.; Gut, P.; Polat, B.; Hildebrandt, G.; Müller, A.C.; Plasswilm, L.; et al. Dose-intensified Versus Conventional-dose Salvage Radiotherapy for Biochemically Recurrent Prostate Cancer after Prostatectomy: The SAKK 09/10 Randomized Phase 3 Trial. Eur. Urol. 2021, 80, 306–315. [Google Scholar] [CrossRef]
- Pinkawa, M. Spacer application for prostate cancer radiation therapy. Future Oncol. 2014, 10, 851–864. [Google Scholar] [CrossRef]
- Rocco, B.; Cozzi, G. Denonvilliers’ Fascia: Anatomy, Surgical Planes, Use in Reconstruction. In Robot-Assisted Radical Prostatectomy: Beyond the Learning Curve; Davis, J.W., Ed.; Springer International Publishing: Cham, Switzerland, 2016; pp. 113–118. [Google Scholar]
- Connolly, J.A.; Shinohara, K.; Presti, J.C., Jr.; Carroll, P.R. Local recurrence after radical prostatectomy: Characteristics in size, location, and relationship to prostate-specific antigen and surgical margins. Urology 1996, 47, 225–231. [Google Scholar] [CrossRef]
- Lehrich, B.; Moyses, H.; Ravera, J.; Yoshida, J.; Torrey, R.; Baghdassarian, R.; Gazzaniga, M.; Weinberg, A.; Phan, C.; Chalfin, S.; et al. Five-year results of post-prostatectomy patients administered a hydrogel rectal spacer implant in conjunction with dose escalated external beam radiation therapy. J. Radiat. Oncol. 2019, 8, 31–38. [Google Scholar] [CrossRef]
- Sidhom, M.A.; Kneebone, A.B.; Lehman, M.; Wiltshire, K.L.; Millar, J.L.; Mukherjee, R.K.; Shakespeare, T.P.; Tai, K.-H. Post-prostatectomy radiation therapy: Consensus guidelines of the Australian and New Zealand Radiation Oncology Genito-Urinary Group. Radiother. Oncol. 2008, 88, 10–19. [Google Scholar] [CrossRef]
- Chao, M.; Ho, H.; Joon, D.L.; Chan, Y.; Spencer, S.; Ng, M.; Wasiak, J.; Lawrentschuk, N.; McMillan, K.; Sengupta, S.; et al. The use of tissue fiducial markers in improving the accuracy of post-prostatectomy radiotherapy. Radiat. Oncol. J. 2019, 37, 43–50. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services NIoH, National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE), v4.03; EORTC: Brussels, Belgium, 2010.
- Mariados, N.; Sylvester, J.; Shah, D.; Karsh, L.; Hudes, R.; Beyer, D.; Kurtzman, S.; Bogart, J.; Hsi, R.A.; Kos, M.; et al. Hydrogel Spacer Prospective Multicenter Randomized Controlled Pivotal Trial: Dosimetric and Clinical Effects of Perirectal Spacer Application in Men Undergoing Prostate Image Guided Intensity Modulated Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 971–977. [Google Scholar] [CrossRef]
- Mariados, N.F.; Orio, P.F., 3rd; Schiffman, Z.; Van, T.J.; Engelman, A.; Nurani, R.; Kurtzman, S.M.; Lopez, E.; Chao, M.; Boike, T.P.; et al. Hyaluronic Acid Spacer for Hypofractionated Prostate Radiation Therapy: A Randomized Clinical Trial. JAMA Oncol. 2023, 9, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Valuck, B.W.; Chundury, A.; Gay, H.; Bosch, W.; Michalski, J. Hydrogel spacer distribution within the perirectal space in patients undergoing radiotherapy for prostate cancer: Impact of spacer symmetry on rectal dose reduction and the clinical consequences of hydrogel infiltration into the rectal wall. Pract. Radiat. Oncol. 2017, 7, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Karsh, L.I.; Gross, E.T.; Pieczonka, C.M.; Aliotta, P.J.; Skomra, C.J.; Ponsky, L.E.; Nieh, P.T.; Han, M.; Hamstra, D.A.; Shore, N.D. Absorbable Hydrogel Spacer Use in Prostate Radiotherapy: A Comprehensive Review of Phase 3 Clinical Trial Published Data. Urology 2018, 115, 39–44. [Google Scholar] [CrossRef]
- Miller, L.E.; Efstathiou, J.A.; Bhattacharyya, S.K.; Payne, H.A.; Woodward, E.; Pinkawa, M. Association of the Placement of a Perirectal Hydrogel Spacer with the Clinical Outcomes of Men Receiving Radiotherapy for Prostate Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e208221. [Google Scholar] [CrossRef] [PubMed]
- Hamstra, D.A.; Mariados, N.; Sylvester, J.; Shah, D.; Karsh, L.; Hudes, R.; Beyer, D.; Kurtzman, S.; Bogart, J.; Hsi, R.A.; et al. Continued Benefit to Rectal Separation for Prostate Radiation Therapy: Final Results of a Phase III Trial. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 976–985. [Google Scholar] [CrossRef] [PubMed]
- Hamstra, D.A.; Mariados, N.; Sylvester, J.; Shah, D.; Gross, E.; Hudes, R.; Beyer, D.; Kurtzman, S.; Bogart, J.; Hsi, R.A.; et al. Sexual quality of life following prostate intensity modulated radiation therapy (IMRT) with a rectal/prostate spacer: Secondary analysis of a phase 3 trial. Pract. Radiat. Oncol. 2018, 8, e7–e15. [Google Scholar] [CrossRef] [PubMed]
- Pinkawa, M.; Schubert, C.; Escobar-Corral, N.; Holy, R.; Eble, M.J. Application of a hydrogel spacer for postoperative salvage radiotherapy of prostate cancer. Strahlenther. Onkol. 2015, 191, 375–379. [Google Scholar] [CrossRef]
- Yeh, J.; Tokita, K.; Chien, J.; Ravera, J. (P141) rectal spacer injection in postprostatectomy patients undergoing high-dose salvage external beam radiation. Oncology 2015, 29 (Suppl. S1). [Google Scholar]
- Yang, D.X.; Verma, V.; An, Y.; Yu, J.B.; Sprenkle, P.C.; Leapman, M.S.; Park, H.S. Radiation Dose to the Rectum with Definitive Radiation Therapy and Hydrogel Spacer Versus Postprostatectomy Radiation Therapy. Adv. Radiat. Oncol. 2020, 5, 1225–1231. [Google Scholar] [CrossRef]
- Zaine, H.; Vandendorpe, B.; Bataille, B.; Lacornerie, T.; Wallet, J.; Mirabel, X.; Lartigau, E.; Pasquier, D. Salvage Radiotherapy for Macroscopic Local Recurrence Following Radical Prostatectomy. Front. Oncol. 2021, 11, 1258. [Google Scholar] [CrossRef]
- Wu, W.-C.; Lai, Y.-L.; Liang, J.-A. Salvage radiotherapy for biochemical recurrence after radical prostatectomy: Experience of a single center. Ther. Radiol. Oncol. 2018, 2, 3. [Google Scholar] [CrossRef]
- Stephenson, A.J.; Scardino, P.T.; Kattan, M.W.; Pisansky, T.M.; Slawin, K.M.; Klein, E.A.; Anscher, M.S.; Michalski, J.M.; Sandler, H.M.; Lin, D.W.; et al. Predicting the Outcome of Salvage Radiation Therapy for Recurrent Prostate Cancer after Radical Prostatectomy. J. Clin. Oncol. 2007, 25, 2035–2041. [Google Scholar] [CrossRef]
- De Bruycker, A.; Lambert, B.; Claeys, T.; Delrue, L.; Mbah, C.; De Meerleer, G.; Villeirs, G.; De Vos, F.; De Man, K.; Decaestecker, K.; et al. Prevalence and prognosis of low-volume, oligorecurrent, hormone-sensitive prostate cancer amenable to lesion ablative therapy. BJU Int. 2017, 120, 815–821. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).