Abstract
Background: Signet ring cell adenocarcinoma (SRCC) of the bladder is a rare and aggressive histological subtype of bladder cancer. Due to its infrequency, the understanding of its clinical behaviour, treatment strategies, and outcomes remains limited, being primarily derived from isolated case reports and series. Objective: To systematically review and analyse the available literature on SRCC of the bladder, emphasizing its clinical characteristics, diagnostic approaches, treatment modalities, and outcomes. Material and Methods: A comprehensive search was conducted across PubMed, Embase, and Medline following the PRISMA guidelines, including case reports, case series, observational studies, and clinical trials reporting on bladder SRCC. Results: We included 38 articles reporting on 77 patients, primarily males (79.2%), with a median age of 64 years. The most common presenting symptoms were haematuria (64.8%) and lower urinary tract symptoms (46.3%). All the diagnoses were based on histopathological examination of bladder tissue samples and immunohistochemistry. Mixed histological types of bladder cancer were found in 20.7% of cases, most commonly urothelial carcinoma (61.1%). The treatments varied, with 53.2% of patients undergoing radical cystectomy, 24.7% receiving radiotherapy, and 16.9% receiving chemotherapy. The five-year survival rates were 9.4%. Conclusion: Bladder SRCC presents aggressively, with varied treatment strategies; however, radical cystectomy appears to be the optimal means of surgical management for organ-confined disease. The overall survival rate is low, highlighting the need for further research to understand and manage this rare bladder cancer variant. All patients should undergo evaluation to exclude extravesical primaries. This systematic review contributes to a better understanding of this disease and may guide clinical management strategies.
1. Introduction
Bladder cancer is one of the most common malignancies of the urinary system, with urothelial carcinoma being the predominant histological subtype [1]. However, various other histological types of bladder cancer exist, including squamous cell carcinoma, adenocarcinoma, small cell carcinoma, and more. Adenocarcinoma of the bladder is often divided into urachal origin and non-urachal origin.
Signet ring cell adenocarcinoma (SRCC) of the bladder refers to those of non-urachal origin and is characterized by the presence of cells with abundant intracytoplasmic mucin that displaces the nucleus to the cell periphery, giving it a signet ring appearance [2]. While SRCC is more commonly associated with gastrointestinal malignancies, especially colorectal or gastric cancer, prostate cancer and breast cancer, its occurrence in the urinary bladder is infrequent. The presence of adenocarcinoma in the bladder warrants an extensive metastatic workup to rule out an extra-vesical primary.
Due to its rarity, knowledge about SRCC of the bladder is primarily derived from a limited number of case reports and case series, leading to challenges in understanding its clinical characteristics, behaviour, treatment strategies, and prognosis. The existing literature suggests that SRCC of the bladder is aggressive, with the majority of patients presenting with muscle-invasive disease with a propensity for early metastasis and a poor prognosis [3]. However, the scarcity and fragmented nature of the available evidence limit the understanding and management of this rare bladder cancer variant.
Given the above, it is essential to aggregate the existing evidence to provide a more comprehensive understanding of SRCC of the bladder. Therefore, this systematic review aims to collate and analyse the available literature on SRCC of the bladder to describe its clinical characteristics, diagnostic procedures, treatment strategies, and outcomes. The findings of this review will aid clinicians in the early recognition, appropriate management, and counselling of patients with this rare malignancy.
2. Methodology
A comprehensive search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines using the following databases: PubMed, Embase, and Medline. We searched these databases from inception until February 2023. The reference lists of the included studies and relevant reviews were manually checked to identify additional potential studies (Supplementary Data S1).
The search strategy combined key terms related to bladder cancer and signet ring cell carcinoma. The terms used were “signet ring cell carcinoma” AND “bladder carcinoma”. An English language restriction was imposed.
2.1. Eligibility Criteria
Studies were eligible for inclusion if they met the following criteria:
- Original articles reporting on patients diagnosed with signet ring cell carcinoma of the bladder.
- Studies providing data on at least one of the following outcomes: overall survival, disease-free survival, progression-free survival, treatment options and their outcomes, pathological characteristics, and prognostic factors.
- Case reports, case series, observational studies (cohort and case-control), and clinical trials were included.
Articles were excluded if they met the following criteria:
- Reviews, commentaries, editorials, letters, conference abstracts, and expert opinions.
- Studies not providing specific data on the outcomes for patients with signet ring cell carcinoma of the bladder.
- Studies on paediatric patients (aged <18 years).
- Studies that did not rule out a primary gastrointestinal malignancy.
2.2. Data Extraction and Quality Assessment
Data were extracted using a pre-specified data extraction form. The following information was obtained from each study: first author’s name, year of publication, study design, patients’ baseline characteristics, clinical findings, diagnostic methods, treatment methods and outcomes.
The methodological quality of the included studies was assessed by two independent authors (K.C. and M.B.). Any disagreements between the reviewers were resolved through discussion or consultation with a third reviewer if necessary.
2.3. Data Synthesis and Analysis
Given the nature of the included studies, being primarily case reports and case series, a meta-analysis was not feasible. Instead, data were synthesized qualitatively. Patient characteristics, such as age, gender, and presenting symptoms, were described. In addition, details about the diagnostic procedures, pathologic findings, treatments, and outcomes were collated. Descriptive statistics were used to summarize the data.
2.4. Risk of Bias across the Studies
The risk of bias in the case reports and case series was evaluated using the Oxford Centre for Evidence-Based Medicine: Levels of Evidence (CEBM) document. All the articles were of level 4 evidence (Supplementary Data S2).
Given that case reports and case series are inherently high in bias and low in evidence level, the overall evidence generated by this review should be interpreted with caution.
2.5. Ethics Approval and Consent to Participate
As this study was a systematic review, it did not involve direct contact with patients or alterations to patient care, and thus, it did not require ethics committee approval.
2.6. Availability of Data and Material
All the data generated or analysed during this study are included in this published article or are available from the corresponding author on request.
3. Results
3.1. Study Selection and Characteristics
The initial search yielded a total of 182 studies, which were screened for eligibility. Of these, 144 were excluded due to various reasons, such as irrelevant topics, not reporting specific data on patients with signet ring cell carcinoma of the bladder or not being original articles. A total of 38 articles, all case reports and case series, met our inclusion criteria and were included in the final qualitative synthesis [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46]. The PRISMA flow diagram of the study selection process is shown in Figure 1.
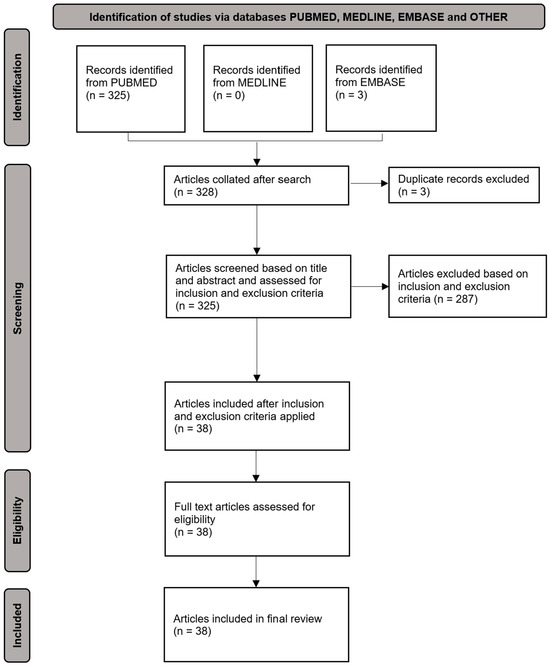
Figure 1.
PRISMA flow diagram for systematic reviews concerning signet ring cell adenocarcinoma of the bladder.
3.2. Patient Characteristics and Clinical Presentation
The 38 articles included a total of 77 patients with signet ring cell carcinoma of the bladder, with ages ranging from 18 to 85 years (median age: 64 years). Of these, 61 (79.2%) were males and 16 were females (20.8%). Of these, there were missing data (n = 24) on the most common presenting complaint. Factoring this in, the most common presenting symptoms were haematuria (n = 35, 64.8%), followed by lower urinary tract symptoms (n = 25, 46.3%) and lower abdominal pain (n = 8, 14.8%).
3.3. Diagnostic Procedures and Pathologic Findings
All the patients were diagnosed based on histopathological examination of bladder tissue samples obtained via cystoscopy and bladder biopsy, cystectomy, or post-mortem. Immunohistochemistry was performed in all cases to confirm the diagnosis. In 18 cases (20.7%), signet ring cell carcinoma was found mixed with other histological types of bladder cancer, most commonly urothelial carcinoma (n = 11, 61.1%) and carcinoma in situ (n = 6, 33.3%) [5,13,17,18,24,29,31,39,42].
Immunohistochemical analyses were conducted in several patients. The most common positive immunohistochemical markers were the Periodic acid–Schiff (PAS) (n = 18), Carcinoembryonic antigen (CEA) (n = 13), Epithelial membrane antigen (EMA) (n = 13) and Cytokeratin Cam 5.2 (n = 13) [13,15,16,17,21,25,26,28,29,31,36,38,40,41,42]. A summary of the immunohistochemical analyses can be found in Table 1.

Table 1.
Summary of the immunohistochemical analyses.
Imaging techniques were widely used to aid in the identification of a bladder mass and to assess for evidence of metastatic disease. In 59 cases (76.6%), a bladder mass was identified via ultrasound of the renal tract or computed tomography of the pelvis. Data on cystoscopy were available in 59 patients, and in all the patients, a bladder mass was detected via cystoscopy.
Data on staging were available in 51 patients (66.2%) and coded as per the American Joint Committee on Cancer (AJCC) Tumour, Node, Metastasis (TNM) staging system [47]. The TNM staging was reported as Stage I 13.5%, Stage II 23.1%, Stage III 25.0%, and Stage IV 36.5%, as represented in Table 2. The prognosis was similar across all the stages.
Table 2.
Patient demographics and characteristics.
Importantly, all 77 patients underwent diagnostic workup to exclude a gastrointestinal malignancy. The modalities included a combination of barium studies, gastroscopy, colonoscopy, and computed tomography imaging.
3.4. Treatment and Outcomes
The treatment strategies varied among the patients. A total of 41 patients (53.2%) underwent radical cystectomy, 19 (24.7%) received radiotherapy and 13 (16.9%) received chemotherapy. In some cases, a combination of these treatments was employed.
The median survival of all the patients who underwent radical cystectomy was 13 months. The one-year, three-year and five-year survival rates were 37.8%, 14.7% and 9.4%, respectively. Nine patients had a local recurrence or distant metastasis following radical cystectomy, with a median time to recurrence/metastatic disease of 16 months.
Patients with non-metastatic disease who underwent radical cystectomy had a median survival of 11.5 months. Accounting for both censoring and the individuals who died, the one-year, three-year, and five-year survival rates were 41.2%, 22.2%, and 16.7%, respectively. Perioperative outcomes were not routinely documented in the papers reviewed.
The chemotherapy regimens deployed were heterogenous. The most common agent used was a platinum-based chemotherapy agent, with three patients in this group. The second most common agent was 5-fluorouracil, with two patients in this group. Given the low numbers, a survival benefit analysis was not feasible.
At the time of reporting, 18 patients (23.4%) were alive with no evidence of disease, 6 (7.8%) were alive with disease, and 48 patients (62.3%) had died of the disease or disease-related complications. The median survival time was 12 months (range: 1–100 months). The most common sites of recurrence and metastases were the spine, liver, and bowel. The median time to recurrence of all the patients was 13.5 months. The one-year, three-year and five-year survival rates were 43.9%, 13.3% and 8.6%, respectively, accounting for censoring.
3.5. Quality of the Included Studies
As per the Joanna Briggs Institute (JBI) Critical Appraisal tools, the quality of the included studies was varied. Many case reports and series lacked details about patient demographics, specific interventions, or precise clinical outcomes, contributing to the risk of bias. It is important to interpret the results keeping this limitation in mind.
4. Discussion
Signet ring cell carcinoma (SRCC) of the bladder is an exceedingly rare and aggressive malignancy with a propensity for early metastasis and an overall poor prognosis. The nature of the disease and its rarity have posed significant challenges to clinicians in its recognition, management, and patient counselling. This systematic review aims to collate the available literature on SRCC of the bladder to provide a more comprehensive understanding of its clinical characteristics, diagnostic procedures, treatment strategies, and outcomes.
Given the scarcity of large-scale studies or clinical trials, our understanding of SRCC largely depends on experience with high-grade transitional cell bladder carcinoma and on case reports and case series, which are inherently high in bias and low in evidence level. Nevertheless, this systematic review attempts to provide an aggregated perspective and serves as the most comprehensive source of information to date regarding SRCC of the bladder. Importantly, although there have been multiple papers in the literature on bladder cancer analysing the outcomes of bladder cancer with variant histology, they do not focus specifically on signet ring cell adenocarcinoma of the bladder [48,49]. They do highlight the importance of awareness of variant histology and their specific management.
The results show that SRCC of the bladder predominantly affects older males, consistent with the demographic typically associated with bladder cancer [1]. Haematuria emerged as the most common presenting symptom, aligning with the typical clinical presentation of bladder cancers [50]. This finding is significant, as it emphasises the importance of considering SRCC in differential diagnoses when treating male patients presenting with haematuria.
The diagnostic procedures involve histopathological examination of bladder tissue samples to identify the presence of signet ring cells to confirm the diagnosis. The use of immunohistochemical markers such as PAS, CEA, EMA, and Cytokeratin Cam 5.2 could be useful to confirm the diagnosis if signet ring cells are not present on microscopy. PAS can be especially useful due to its high sensitivity in detecting mucin-secreting tumours such as adenocarcinomas [51].
All patients diagnosed with signet ring cell adenocarcinoma of the bladder should undergo radiographic exclusion of an extravesical primary, given the propensity for signet ring cell histology to metastasize. This workup should include computed tomography of the chest, abdomen and pelvis, and complete endoscopic examination of the gastrointestinal tract.
In terms of therapeutic strategies, our review discerned considerable heterogeneity in the treatment modalities among patients with SRCC of the bladder, reflecting a lack of consensus regarding optimal management. Recognizing the aggressive nature of SRCC, underscored by its propensity for early metastatic spread, it appears prudent to consider multi-modal treatments encompassing radical cystectomy, chemotherapy, and radiotherapy. It is imperative to acknowledge that the prevailing management guidelines for bladder cancer are derived from the EUA/AUA international protocols tailored for transitional cell carcinoma [52,53]. These protocols stratify patients based on the disease stage and align the treatment recommendations accordingly. Given that a significant proportion of SRCC patients present at advanced stages and acknowledging the intrinsic aggressiveness of this non-urachal adenocarcinoma variant, an immediate cystectomy might be imperative in the presence of non-metastatic disease. This urgency is accentuated by the poor prognostic implications associated with signet ring cell histology.
The survival rates were sobering, with the one-year, three-year and five-year survival rates being 43.9%, 13.3% and 8.6%, respectively. However, these figures are derived from inherently biased sources and must be interpreted with caution. Nevertheless, they underscore the aggressive nature of SRCC and the need for early recognition and aggressive management. Radical cystectomy appears to confer the highest survival benefit.
This systematic review, while insightful, is not without its limitations. Firstly, the evidence generated is based on case reports and case series, which are low-level evidence and high in bias. Secondly, the significant heterogeneity in patient characteristics, treatment protocols, and outcome measures limits the ability to draw firm conclusions. Thirdly, the exclusion of non-English studies may have led to language bias.
Despite these limitations, this review contributes to the urological field by consolidating the available knowledge on SRCC of the bladder. Future research in SRCC of the bladder should focus on creating an international registry for this rare entity to foster multi-centre collaborations and generate more robust evidence. This will hopefully pave the way for future research to further elucidate the nature of this aggressive disease, thereby improving patient outcomes.
Although our systematic review has collated the available evidence on signet ring cell carcinoma of the bladder, due to the nature of the included studies, the evidence generated should be interpreted with caution. However, further research is needed to improve our understanding of this disease and to establish standardized protocols for diagnosis and management.
In conclusion, SRCC of the bladder is a rare and aggressive disease variant presenting diagnostic and therapeutic challenges, with the mortality rates being similar across the TNM stages. Our findings highlight the clinical presentation, diagnostic procedures, and treatment strategies currently employed in managing this rare bladder cancer variant. Gastrointestinal and gynaecological primaries should be excluded by performing the appropriate investigations. Due to the aggressive nature of signet ring cell histology, early radical cystectomy should be considered in non-metastatic disease.
Supplementary Materials
The following supporting information can be downloaded at https://www.mdpi.com/article/10.3390/siuj5020022/s1, Supplementary Data S1: Seventy-seven cases of primary signet ring cell adenocarcinoma of the bladder, identified from a systematic review of PubMed, EMBASE, and Medline databases; Supplementary Data S2: Critical analysis of the papers.
Author Contributions
As per the CRediT (Contributor Roles Taxonomy) Author Statement, the author contributions for each author are listed below: K.K.Y.C.—Conceptualization, methodology, writing—original draft, writing—review and editing; M.B.—Conceptualization, methodology, data curation; K.W.—Data curation; C.S.—Data curation; W.X.—Formal analysis; R.S.—Supervision, writing—review and editing; P.B.—Supervision, writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data supporting the findings of this study are available within the article and/or its Supplementary Materials.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviation
SRCC—Signet ring cell adenocarcinoma.
References
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urology. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours. Urinary and Male Genital Tumours; WHO: Geneva, Switzerland, 2022; Volume 8, pp. 193–233. [Google Scholar]
- Lopez-Beltran, A.; Henriques, V.; Montironi, R.; Cimadamore, A.; Raspollini, M.R.; Cheng, L. Variants and new entities of bladder cancer. Histopathology 2019, 74, 77–96. [Google Scholar] [CrossRef] [PubMed]
- Allameh, F.; Fallah Karkan, M.; Nilipour, Y.; Rakhshan, A. Primary Signet-Ring Cell Carcinoma of the Urinary Bladder Successfully Managed with Radical Cystectomy in a Young Patient. Case Rep. Urol. 2017, 2017, 9121078. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.A.; Bumpers, H.L.; Kennedy, A.P.; Parsh, S.; Mobley, D.L.; Hoover, E.L. Primary adenocarcinoma, signet-ring, and transitional cell carcinoma of the bladder with penile metastasis. J. Natl. Med. Assoc. 1997, 89, 253–256. [Google Scholar] [PubMed]
- Chin, N.W.; Marinescu, A.M.; Fani, K. Composite adenocarcinoma and carcinoid tumor of urinary bladder. Urology 1992, 40, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Lamb, S.; Pintar, K.; Jacobs, S.C. Primary Signet-Ring Cell Carcinoma of the Urinary Bladder. Cuncer 1984, 53, 1985–1990. [Google Scholar] [CrossRef]
- Corwin, S.H.; Tassy, F.; Malament, M.; Grady, H.G. Rare signet ring cell variant of mucinous adenocarcinoma of the bladder. J. Urol. 1971, 106, 697–700. [Google Scholar] [CrossRef] [PubMed]
- Defillipo, N.; Blute, R.; Klein, L.A. Signet-ring cell carcinoma of bladder. Evaluation of three cases with review of literature. Urology 1987, 29, 479–483. [Google Scholar] [CrossRef] [PubMed]
- DeMay, R.M.; Grathwohl, M.A. Signet-ring-cell (colloid) carcinoma of the urinary bladder: Cytologic, histologic and ultrastructural findings in one case. Acta Cytol. 1985, 29, 132–136. [Google Scholar]
- De Ture, F.A.; Dein, R.; Hackett, R.L.; Drylie, D.M. Primary signet ring cell carcinoma of bladder exemplifying vesical epithelial multipotentiality. Urology 1975, 6, 240–244. [Google Scholar] [CrossRef]
- El Ammari, J.E.; Ahsaini, M.; Riyach, O.; El Fassi, M.J.; Farih, M.H.; Hammas, N.; Elfatmi, H.; Amarti, A. Primary signet-ring cell carcinoma of the urinary bladder successfully managed with cisplatin and gemcitabine: A case report. J. Med. Case Rep. 2013, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Erdoğru, T.; Kihçaslan, I.; Esen, T.; Ander, H.; Ziylan, O.; Uysal, V. Primary signet ring cell carcinoma of the urinary bladder. Review of the literature and report of two cases. Urol. Int. 1995, 55, 34–37. [Google Scholar] [CrossRef]
- Fiter, L.; Gimeno, F.; Martin, L.; Gomez Tejeda, L. Signet-ring cell adenocarcinoma of bladder. Urology 1993, 41, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Goble, N.M.; Clarke, T.J.; Teasdale, C. Signet ring cell adenocarcinoma of bladder secondary to long-term catheterization. Urology 1990, 35, 279–281. [Google Scholar] [CrossRef]
- Azadeh, B.; Vijayan, P.; Chejfec, G. Linitis Plastica-like Carcinoma of the Urinary Bladder. Br. J. Urol. 1989, 63, 479–482. [Google Scholar] [CrossRef] [PubMed]
- Hirano, Y.; Suzuki, K.; Fujita, K.; Furuse, H.; Fukuta, K.; Kitagawa, M.; Aso, Y. Primary signet ring cell carcinoma of the urinary bladder successfully treated with intra-arterial chemotherapy alone. Urology 2002, 59, 601. [Google Scholar] [CrossRef]
- Horne, D.W.; Fauver, H.E. Primary signet ring cell carcinoma of bladder. Urology 1987, 30, 574–578. [Google Scholar] [CrossRef]
- Ivanov, A.; Antonov, P.; Zapryanov, M.; Uchikov, P.; Belovezhdov, V. Primary signet-ring cell adenocarcinoma of the bladder-A case report and review of literature. Urol. Case Rep. 2022, 42, 102022. [Google Scholar] [CrossRef]
- Jayarajah, U.; Fernando, D.M.H.; Herath, K.B.; de Silva, M.V.C.; Goonewardena, S.A.S. Primary Signet-Ring Cell Adenocarcinoma of the Urinary Bladder Treated with Partial Cystectomy: A Case Report and Review of the Literature. Case Rep. Urol. 2017, 2017, 6829692. [Google Scholar] [CrossRef]
- Kim, S.S.; Choi, Y.D.; Nam, J.H.; Kwon, D.D.; Juhng, S.W.; Choi, C. Cytologic features of primary signet ring cell carcinoma of the bladder: A case report. Acta Cytol. 2009, 53, 309–312. [Google Scholar] [CrossRef]
- Kinra, P.; Rashmi, S.P.; Alam, A.; Singh, H.; Dash, S.C. Primary signet cell adenocarcinoma of bladder. Indian J. Pathol. Microbiol. 2017, 60, 584–586. [Google Scholar] [CrossRef] [PubMed]
- Kondo, A.; Mitsuya, H. Signet-ring cell carcinoma involving the urinary bladder: Report of a case and review of 21 cases. Urol. Int. 1981, 36, 373–379. [Google Scholar] [CrossRef]
- Kume, H.; Kanai, Y.; Tobisu, K.I.; Fujimoto, H.; Tomita, K.; Kakizoe, T. Signet-ring cell carcinoma of the urinary bladder associated with transitional cell carcinoma of the right ureter. Scand. J. Urol. Nephrol. 2000, 34, 278–279. [Google Scholar] [CrossRef]
- Manassero, F.; Giannarini, G.; Paperini, D.; Mogorovich, A.; Alì, G.; Boggi, U.; Selli, C. Simultaneous Penile and Signet Ring Cell Bladder Carcinoma in Renal Transplant Recipient: A First Case. Sci. World J. 2009, 9, 920. [Google Scholar] [CrossRef]
- Marino, G.; Motta, E.; Mosso, L.; Bocca, C.; Ravarino, N.; Torchio, B. Primary signet ring cell adenocarcinoma of the bladder. Minerva Urol. Nefrol. 2005, 57, 125–127. [Google Scholar]
- Bernstein, S.A.; Reuter, V.E.; Carroll, P.R.; Whitmore, W.F. Primary signet ring cell carcinoma of urinary bladder. Urology 1988, 31, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Morelli, O.; Castellani, D.; Asciutti, S.; Baldoni, M.; Familiari, L.; Nardi, E.; Clerici, C. Colon and gastric metastases from a primary signet-ring cell carcinoma of the urinary bladder. Dig. Liver Dis. 2006, 38, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Naeim, F.; Schlezinger, R.M.; de la Maza, L.M. Primary signet ring cell carcinoma of the bladder: Report of a case and review of the literature. J. Urol. 1972, 108, 274–276. [Google Scholar] [CrossRef]
- Ohnita, T.; Sakai, H.; Matsuo, M.; Hisamatsu, H.; Shimokawa, I.; Saito, Y. Primary signet ring cell adenocarcinoma of the bladder with elevated serum carbohydrate antigens 19–9 and 50. J. Urol. 1998, 159, 1641. [Google Scholar] [CrossRef]
- Ohtsuki, Y.; Fukumoto, T.; Okada, Y.; Teratani, Y.; Hayashi, Y.; Lee, G.H. Immunohistochemical and ultrastructural characterization of the signet-ring cell carcinoma component in a case of urothelial carcinoma of the urinary bladder. Med. Mol. Morphol. 2010, 43, 96–101. [Google Scholar] [CrossRef]
- Ponz, M.; Luzuriaga, J.; Robles, J.E.; Guillén, F.; Urmeneta, J.M.; Salvá, A.; Zudaire, J.J.; Berián, J.B. Primary signet-ring cell carcinoma of the urinary bladder (Linitis plastica). Eur. Urol. 1985, 11, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Pugashetti, N.; Stanley, A.; Primo, N.; Regina, G.E.; Marc, A. Metastatic signet-ring cell carcinoma of the urinary bladder: A novel management approach to a rare tumour. J. Can. Urol. Assoc. 2015, 9, E204–E207. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Romics, I.; Székely, E.; Szendroi, A. Signet-ring cell carcinoma arising from the urinary bladder. Can. J. Urol. 2008, 15, 4266–4268. [Google Scholar]
- Rosas-Uribe, A.; Luna, M. Primary signet ring cell carcinoma of the urinary bladder. Report of two cases. Arch. Pathol. 1969, 88, 294–297. [Google Scholar] [PubMed]
- Tanaka, T.; Kanai, N.; Sugie, S.; Nakamura, A.; Hayashi, H.; Fujimoto, Y.; Takeuchi, T. Primary signet-ring cell carcinoma of the urinary bladder. Pathol. Res. Pract. 1987, 182, 130–132. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.A.; Stephenson, A.J.; Campbell, S.C.; Jones, J.S.; Hansel, D.E. Clinicopathologic features and utility of immunohistochemical markers in signet-ring cell adenocarcinoma of the bladder. Hum. Pathol. 2009, 40, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Blute, M.L.; Engen, D.E.; Travis, W.D.; Kvols, L.K.; Prout, G.R. Primary signet ring cell adenocarcinoma of the bladder. J. Urol. 1989, 141, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Torenbeek, R.; Koot, R.A.C.; Blomjous, C.E.M.; De Bruin, P.C.; Newling, D.W.W.; Meijer, C.J.L.M. Primary signet-ring cell carcinoma of the urinary bladder. Histopathology 1996, 28, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Bégin, L.R.; Reid, M.; Brock, G.B. Oliguria, an unusual presentation of primary signet ring-cell adenocarcinoma of the urinary bladder: A case report and review of the literature. J. Surg. Oncol. 1999, 70, 64–67. [Google Scholar] [CrossRef]
- Yamamoto, S.; Ito, T.; Akiyama, A.; Miki, M.; Tachibana, M.; Takase, M.; Mochizuki, M. Primary signet-ring cell carcinoma of the urinary bladder inducing renal failure. Int. J. Urol. 2001, 8, 190–193. [Google Scholar] [CrossRef]
- Bodi, I.; Andrews, T.C.; Howard, R.S.; Al-Sarraj, S. Carcinomatous meningitis from primary signet ring cell carcinoma of bladder. Histopathology 2004, 44, 394–396. [Google Scholar] [CrossRef] [PubMed]
- Bouhajja, L.; Farah, F.; Garbouj, N.; Rammeh, S. Primary signet-ring cell carcinoma of the urinary bladder: A report of two cases. Tunis. Medicale 2019, 97, 167–169. [Google Scholar]
- Boukettaya, W.; Feki, J.; Charfi, S.; Toumi, N.; Khanfir, A.; Boudawara, T.; Daoud, J.; Frikha, M. Primary signet ring cell adenocarcinoma of the urinary bladder: A report of 2 cases. Urol. Case Rep. 2014, 2, 85–87. [Google Scholar] [CrossRef]
- Braun, E.V.; Ali, M.; Olusegun Fayemi, A.; Beaugard, E. Primary signet-ring cell carcinoma of the urinary bladder: Review of the literature and report of a case. Cancer 1981, 47, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Burnett, A.L.; Epstein, J.I.; Marshall, F.F. Adenocarcinoma of urinary bladder: Classification and management. Urology 1991, 37, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Schilsky, R.L.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual; ACS: Washington, DC, USA, 2017; pp. 211–212. Available online: https://link.springer.com/book/9783319406176 (accessed on 22 May 2022).
- Martin, J.W.; Jefferson, F.A.; Huang, M.; Sung, J.M.; Chang, J.; Piranviseh, K.; Ziogas, A.; Anton-Culver, H.; Youssef, R.F. A California Cancer Registry Analysis of Urothelial and Non-urothelial Bladder Cancer Subtypes: Epidemiology, Treatment, and Survival. Clin. Genitourin. Cancer 2020, 18, e330–e336. [Google Scholar] [CrossRef] [PubMed]
- Hajiran, A.; Azizi, M.; Aydin, A.M.; Zemp, L.; Peyton, C.C.; Dhillon, J.; Nealon, S.; Reich, R.R.; Cao, B.; Li, R.; et al. Pathological and Survival Outcomes Associated with Variant Histology Bladder Cancers Managed by Cystectomy with or without Neoadjuvant Chemotherapy. J. Urol. 2021, 205, 100–106. [Google Scholar] [CrossRef]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef]
- Vyas, M.; Zuckerman, J.; Andeen, N.; Tsang, P. Pathology Outlines—PAS (Periodic Acid-Schiff). Pathol. Outl. 2022, 79, 82–104. [Google Scholar]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Espinós, E.L.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef]
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J. Urol. 2017, 198, 552–559. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).