Epidemiology and Clinical Characteristics of Urogenital Tuberculosis in Sabah, Malaysia

Abstract
:1. Introduction
2. Materials and Methods
3. Results
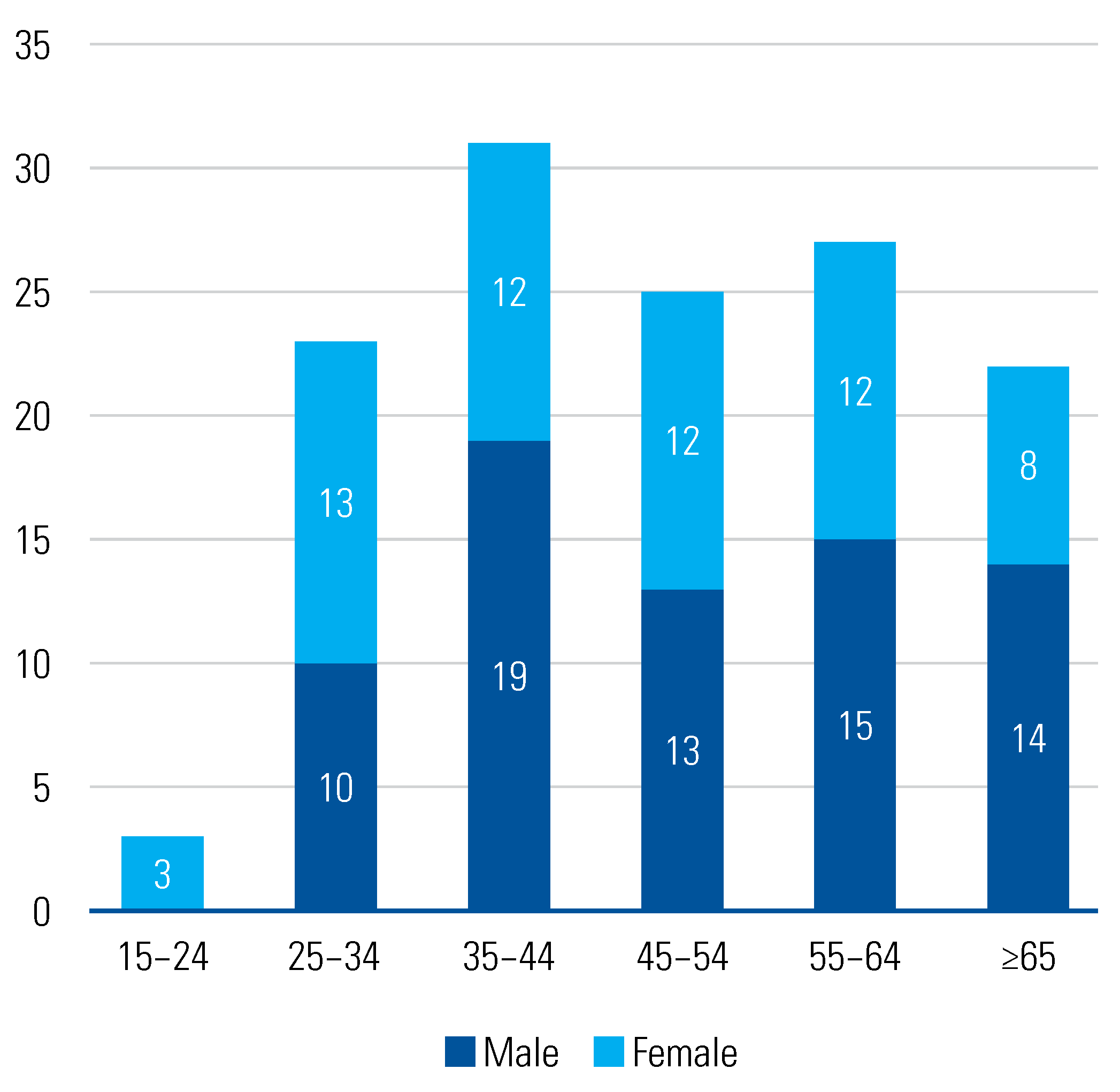
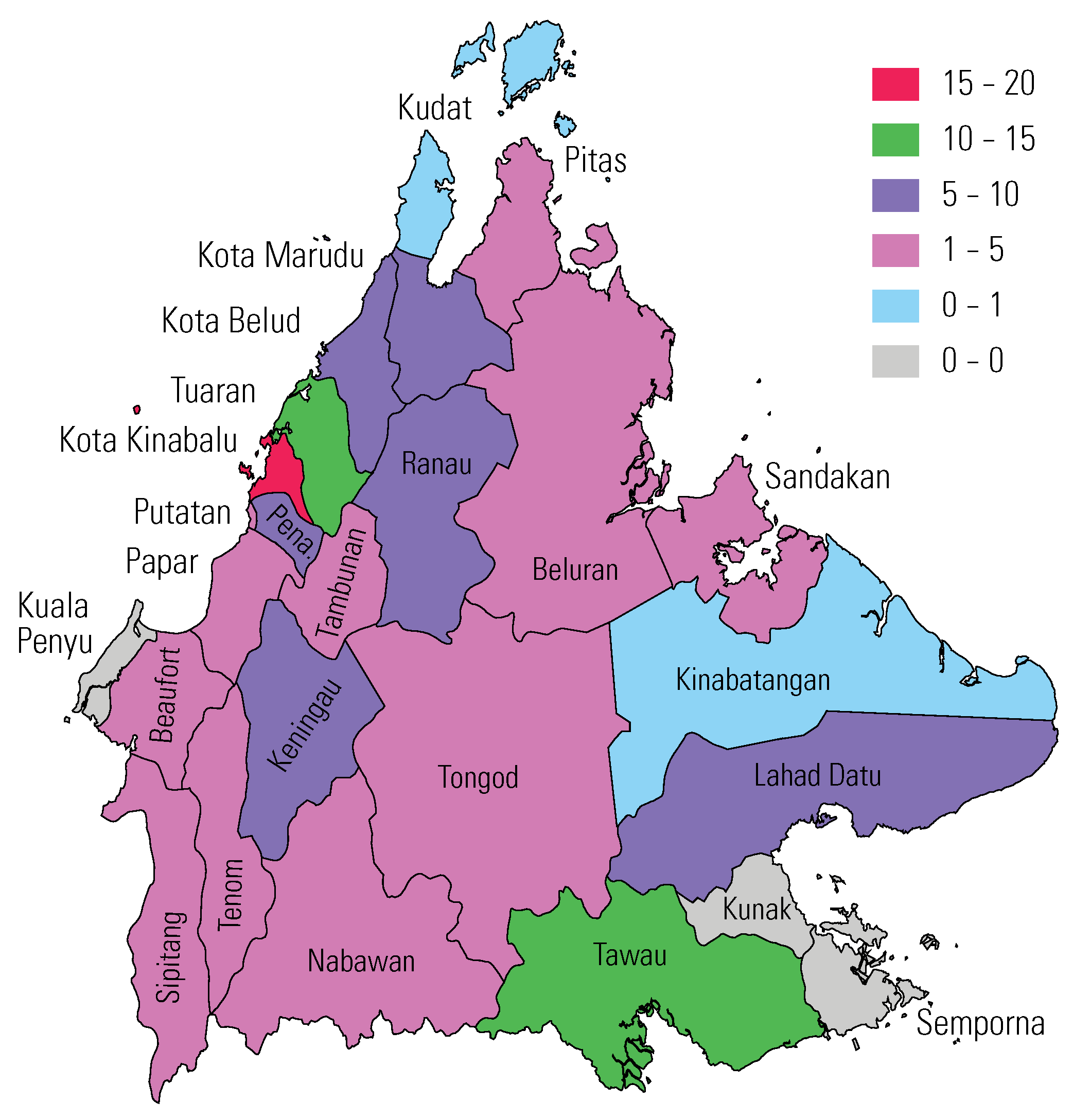
3.1. Patient Demographics
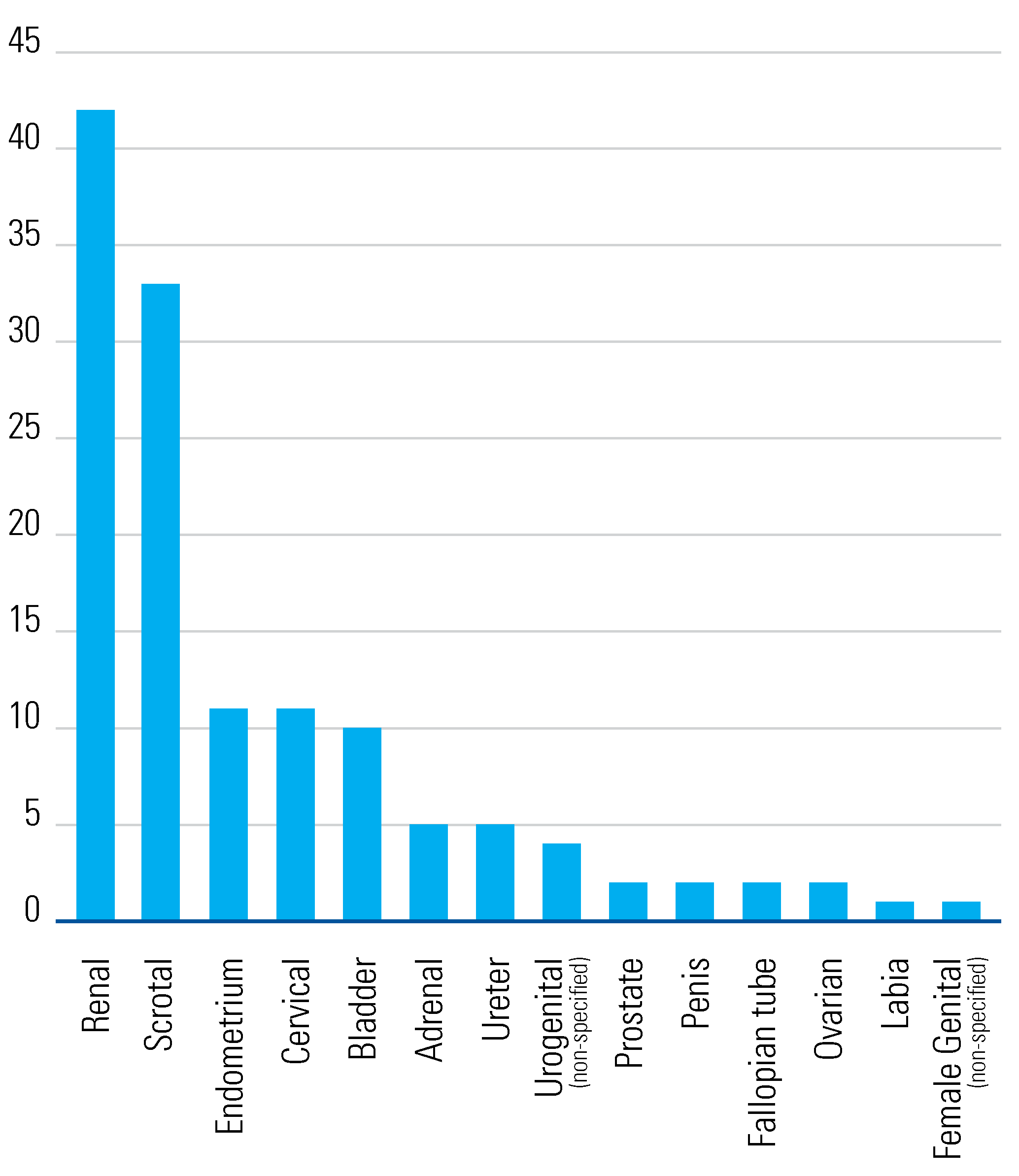
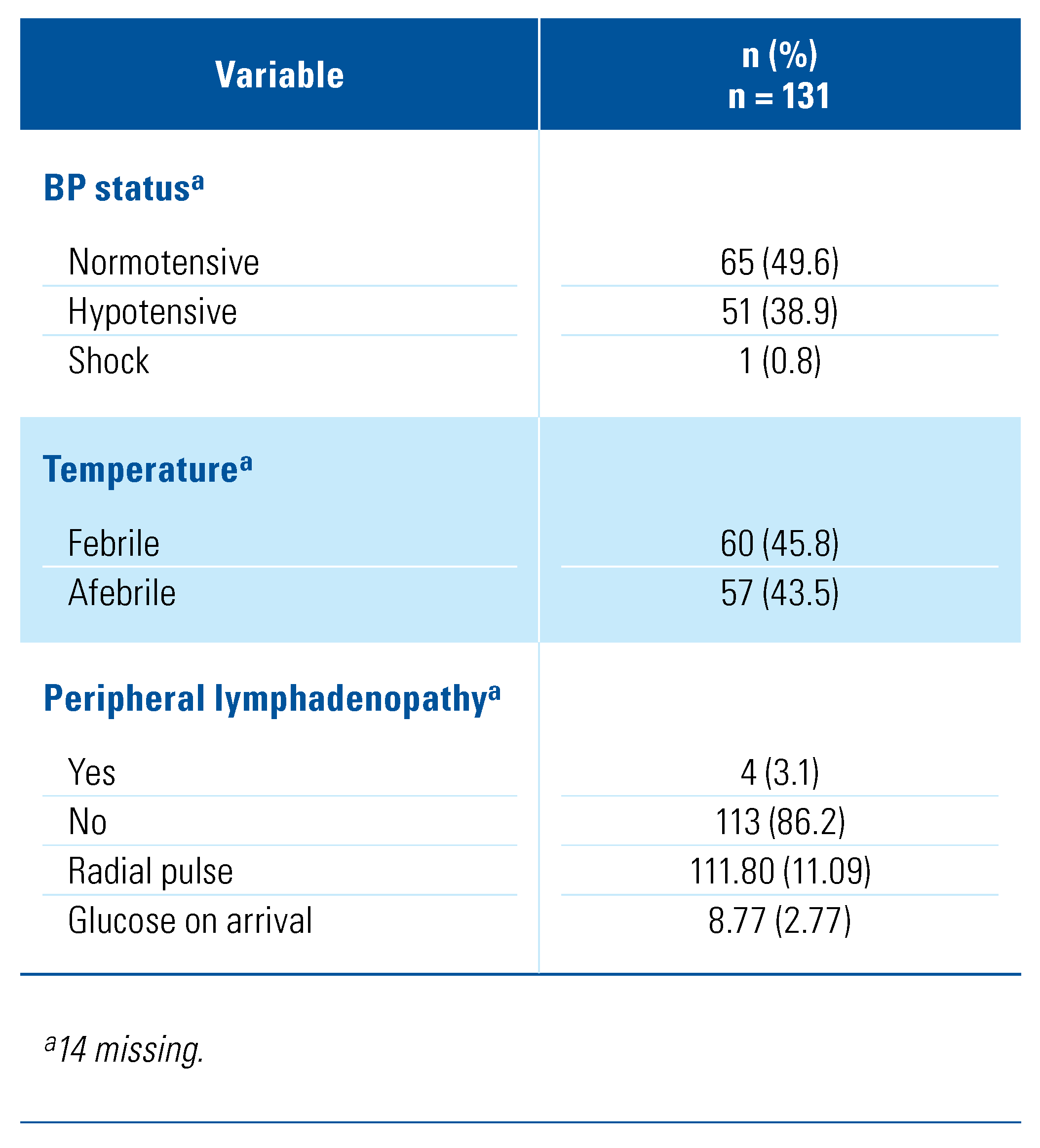
3.2. Clinical Characteristics of Patients
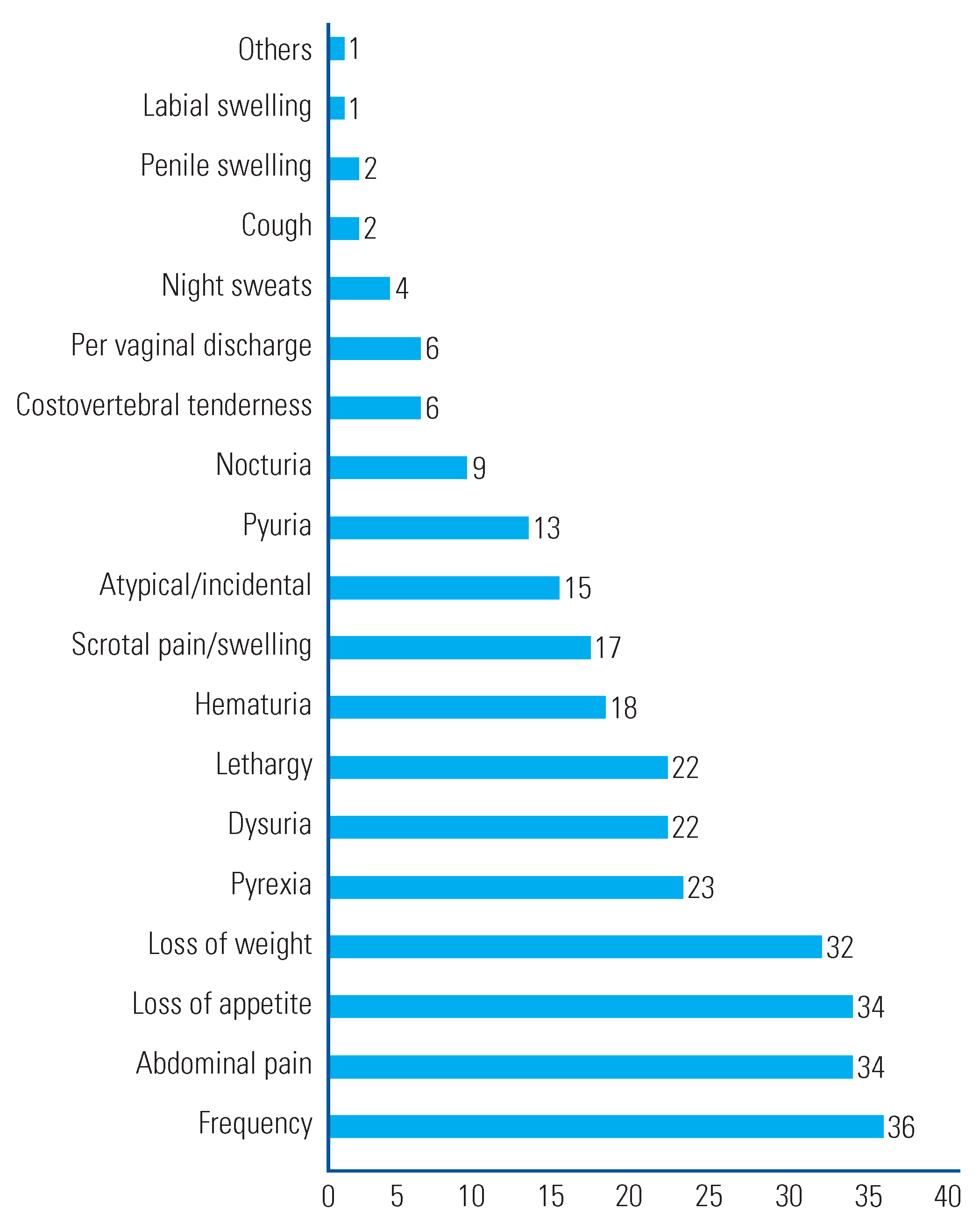
3.3. Clinical Presentation
3.4. Method of Diagnosis
3.5. Treatment Outcomes
5. Discussion
4. Conclusions
Acknowledgments
Conflicts of Interest
Abbreviations
| DOTS | directly observed treatment short course |
| EPTB | extrapulmonary TB |
| FDC | fixed-dosanation |
| TB | tuberculosis |
| UGTB | urogenital tuberculosis |
References
- Gutierrez, M.C.; Brisse, S.; Brosch, R.; Fabre, M.; Omaïs, B.; Marmiesse, M.; et al. Ancient origin and gene mosaicism of the progenitor of Mycobacterium tuberculosis. PLoS Pathogens 2005, 1, e5. [Google Scholar] [CrossRef] [PubMed]
- Hershkovitz, I.; Donoghue, H.D.; Minnikin, D.E.; May, H.; Lee, O.Y.C.; Feldman, M.; et al. Tuberculosis origin: The Neolithic scenario. Tuberculosis. 2015, 95 (Suppl. 1), S122–S126. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO. Global tuberculosis report 2019. In World Health Organization. 2020.
- Iyawoo, K. Tuberculosis in Malaysia: Problems and prospect of treatment and control. Tuberculosis 2004, 84, 4–7. [Google Scholar] [CrossRef] [PubMed]
- Visweswaran, R.K.; Bhat, S. Tuberculosis of the urinary tract. In: Floege J, Johnson RJ, Feehally, J., eds. Comprehensive Clinical Nephrology. Science Direct 2010, 641–648. [Google Scholar] [CrossRef]
- Figueiredo, A.; Lucon, A.; Srougi, M. Urogenital tuberculosis. In Tuberculosis and Nontuberculous Mycobacterial Infections, 7th ed.; Schlossberg, D., Ed.; ASM Press: Washington, DC, USA, 2017. [Google Scholar] [CrossRef]
- Abbara, A.; Davidson, R.N. Etiology and management of genitourinary tuberculosis. Nat. Rev. Urol. 2011, 8, 678–688. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, R.; Ansari, M.S.; Mandhani, A.; Gulia, A. Clinical presentation and diagnostic approach in cases of genitourinary tuberculosis. Indian. J. Urol. 2008, 24, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Department of Statistics, Malaysia. Available online: https://www.dosm.gov.my.
- Dollah, R.; Wan Hassan, W.S.; Peters, D.; Othman, Z. Old threats, new approach and national security in Malaysia: Issues and challenges in dealing with cross-border crime in East Coast of Sabah. Mediterr. J. Soc. Sciences 2016, 7, 178. [Google Scholar] [CrossRef]
- Kulchavenya, E.; Kholtobin, D. Diseases masking and delaying the diagnosis of urogenital tuberculosis. Ther. Adv. Urol. 2015, 7, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Merchant, S.; Bharati, A.; Merchant, N. Tuberculosis of the genitourinary system-urinary tract tuberculosis: Renal tuberculosis-part I. Indian. J. Radiol. Imaging. 2013, 23, 46–63. [Google Scholar] [CrossRef] [PubMed]
- Kulchavenya, E.; Zhukova, I.; Kholtobin, D. Spectrum of urogenital tuberculosis. J. Infect. Chemother. 2013, 19, 880–883. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, S.; Palaniyandi, V.; Kumaresan, N.; Govindaraju, S.; Rajasekaran, J.; Murugappan, I.; et al. Aspects of evolving genito urinary tuberculosis-a profile of genito urinary tuberculosis (GUTB) in 110 patients. J. Clin. Diagn. Res. 2017, 11, PC01–PC05. [Google Scholar] [CrossRef] [PubMed]
- Zajaczkowski, T. Genitourinary tuberculosis: Historical and basic science review: Past and present. Cent. European J. Urol. 2012, 65, 182–187. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n (%) n = 131 |
|---|---|
| Incidence of GUTB/year | |
| 2014 | 20 (15.3) |
| 2015 | 20 (15.3) |
| 2016 | 14 (10.7) |
| 2017 | 19 (14.5) |
| 2018 | 17 (13.0) |
| 2019 | 28 (21.4) |
| 2020 | 13 (9.9) |
| Source of notification | |
| Government hospital | 107 (81.7) |
| Local health clinic | 14 (10.7) |
| Health office | 5 (3.8) |
| Private sector | 5 (3.8) |
| Age (mean±SD) | 48.64 (14.99) |
| Gender | |
| Male | 71 (54.2) |
| Female | 60 (45.8) |
| kg/m2 (mean±SD) | 22.52 (5.32) |
| Nationality | |
| Citizen | 118 (90.1) |
| Peribumi Sabah | 108 (91.5) |
| Chinese | 6 (5.1) |
| Others | 3 (2.5) |
| Peribumi Sarawak | 1 (0.8) |
| Non-Citizen | 13 (9.9) |
| Indonesia | 8 (6.1) |
| Philippines | 4 (3.1) |
| Pakistan | 1 (0.8) |
| Years in Malaysia | |
| 0–5 years | 2 (15.4) |
| 6–15 years | 3 (23.1) |
| 16–20 years | 3 (23.1) |
| 21–25 years | 3 (23.1) |
| >25 years | 2 (15.4) |
| Number of dependents | |
| 0 | 16 (12.2) |
| 1–3 | 48 (36.6) |
| >3 | 54 (41.2) |
| Location | |
| Urban | 37 (28.2) |
| Rural | 94 (71.8) |
| Highest level of patient education a | |
| Illiterate/ No formal education | 37 (28.2) |
| Higher secondary (Form 4/5) | 37 (28.2) |
| Lower secondary (up to Form 3) | 24 (18.3) |
| Primary school | 11 (8.4) |
| Form 6/ Certificate/ Diploma course | 6 (4.6) |
| Tertiary education | 2 (1.5) |
| Employment and income b | |
| Employed/Income | 48 (36.6) |
| Unemployed | 77 (58.8) |
| Occupation c | |
| Professionals (including health care) | 4 (3.1) |
| Skilled | 1 (0.8) |
| Semi-skilled | 17 (13.0) |
| Unskilled/ Labourers | 15 (11.5) |
| Self-employed (unstated) | 6 (4.6) |
| Retired | 5 (3.8) |


| Variable | n (%) n = 131 |
|---|---|
| Treatment length months (mean ± SD) | 8.60 (3.97) |
| Length of stay months (mean ± SD) | 1.00 (1.65) |
| Intensive phase regimen a | |
| 2 EHRZ | 58 (44.2) |
| 2 HRZ | 1 (0.8) |
| FDC | 54 (41.2) |
| Others | 12 (9.2) |
| Intensive phase adverse events | |
| Deaths | 5 (3.8) |
| MDR-TB | 0 |
| None | 126 (96.2) |
| Maintenance phase regimen a | |
| 4H 2R 2E | 3 (2.3) |
| 4 HR | 102 (77.9) |
| FDC | 1 (0.8) |
| Others | 19 (14.5) |
| Current status b | |
| Still under treatment | 5 (3.8) |
| Completed treatment | 106 (81.0) |
| Lost to follow-up/ defaulted | 8 (6.1) |
| Death | 7 (5.3) |
| Change of diagnosis | 2 (1.5) |
| Underwent | |
| DOTS intensive phase c | 117 (89.3) |
| DOTS maintenance phase d | 100 (76.3) |
| Main observer for intensive phase DOTS b | |
| Family | 84 (63.6) |
| Health care worker | 43 (32.8) |
| Unobserved | 1 (0.8) |
| Surgical intervention e | |
| I&D | 14 (10.7) |
| Cystoscopy | 13 (9.9) |
| Orchidectomy | 9 (6.9) |
| Colposcopy | 8 (6.1) |
| Pipelle | 4 (3.1) |
| Stenting | 4 (3.1) |
| Nephrostomy | 3 (2.3) |
| Ovarian cystectomy | 3 (2.3) |
| TRUS biopsy | 2 (1.5) |
| Salpingectomy | 2 (1.5) |
| Ureteroscopy | 1 (0.8) |
| Nephrectomy | 1 (0.8) |
| Renal biopsy | 1 (0.8) |
| FNAC | 1 (0.8) |
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.
Share and Cite
Ramasamy, K.; Thevarajah, S. Epidemiology and Clinical Characteristics of Urogenital Tuberculosis in Sabah, Malaysia. Soc. Int. Urol. J. 2022, 3, 69-76. https://doi.org/10.48083/WHLL5336
Ramasamy K, Thevarajah S. Epidemiology and Clinical Characteristics of Urogenital Tuberculosis in Sabah, Malaysia. Société Internationale d’Urologie Journal. 2022; 3(2):69-76. https://doi.org/10.48083/WHLL5336
Chicago/Turabian StyleRamasamy, Karthikayenee, and Shankaran Thevarajah. 2022. "Epidemiology and Clinical Characteristics of Urogenital Tuberculosis in Sabah, Malaysia" Société Internationale d’Urologie Journal 3, no. 2: 69-76. https://doi.org/10.48083/WHLL5336
APA StyleRamasamy, K., & Thevarajah, S. (2022). Epidemiology and Clinical Characteristics of Urogenital Tuberculosis in Sabah, Malaysia. Société Internationale d’Urologie Journal, 3(2), 69-76. https://doi.org/10.48083/WHLL5336