Predictors for Retrograde Ureteral Stenting Failure as an Initial Drainage Method for Emergent Complicated Acute Calculus Obstructive Uropathy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Methods
2.3. Analysis
3. Results
4. Discussion
5. Conclusion
Conflicts of Interest
Abbreviations
| PCN | percutaneous nephrostomy |
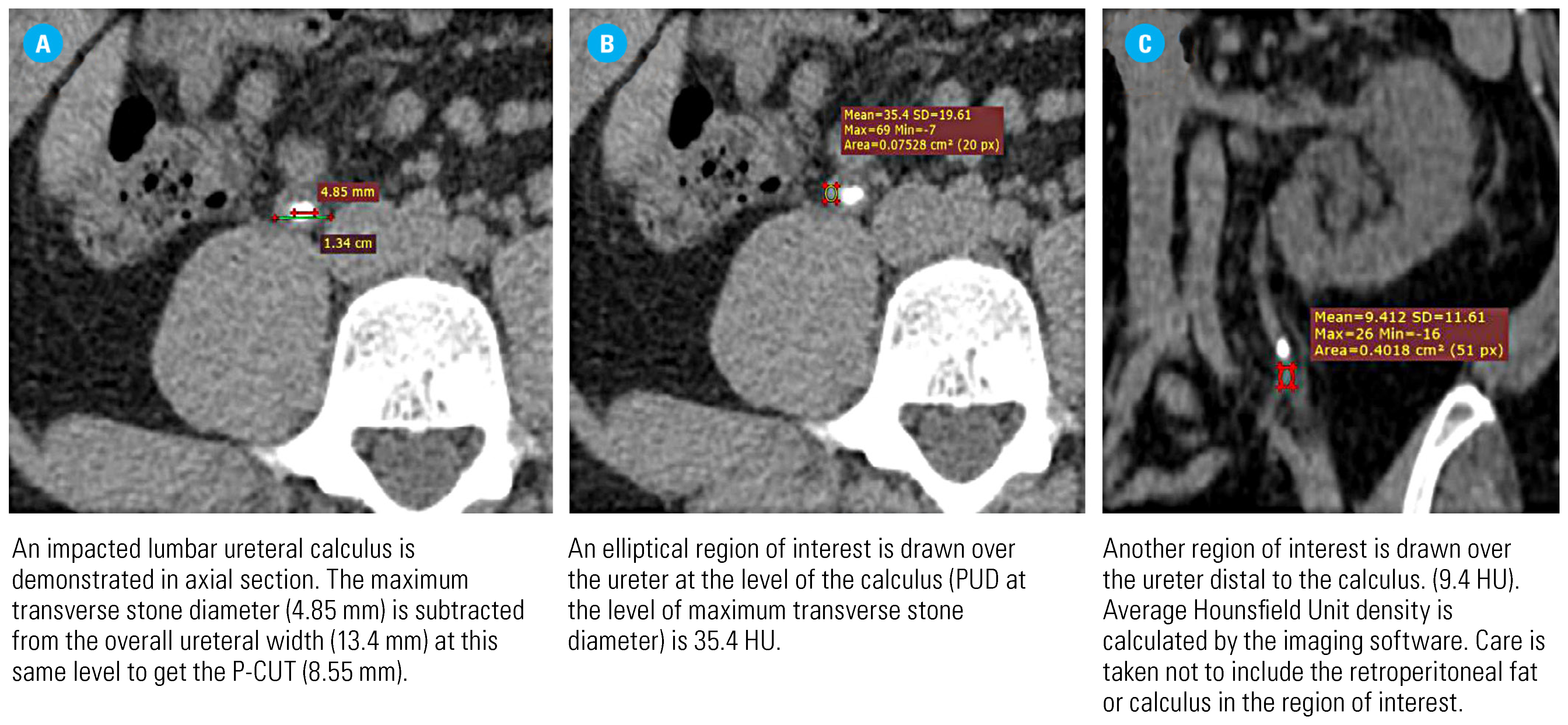
| P-CUT | pericalcular ureteric thickness |
| PUD | periureteral density |
| RUS | retrograde ureteral stenting |
| URS | ureteroscopy |
References
- Campbell, S.; Lane, B. Malignant renal tumors In Campbell-Walsh Urology; Wein, A.J., Kavoussi, L.R., Partin, A.W., Peters, C.A., Eds.; Elsevier: Philadelphia, PA, USA, 2016. [Google Scholar]
- Assimos, D.; Krambeck, A.; Miller, N.L.; Monga, M.; Murad, M.H.; Nelson, C.P.; et al. Surgical management of stones: American urological association/endourological society guideline, PART I. J Urol. 2016, 196, 1153–1160. [Google Scholar] [CrossRef]
- Turk, C.N.A.; Petrik, A.; Seitz, C.; et al. Guidelines on urolithiasis. 2020. Available online: https://uroweb.org/guideline/urolithiasis/.
- Masood, J.; Ismail, M.; El-Husseiny, T.; Moraitis, K.; Albanis, S.; Papatsoris, A.; et al. ‘An interventional urology list’–a novel concept for UK urological services. Ann R Coll Surg Engl. 2011, 93, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Weltings, S.; Schout, B.M.; Roshani, H.; Kamphuis, G.M.; Pelger, R.C. Lessons from Literature: Nephrostomy Versus Double J Ureteral Catheterization in Patients with Obstructive Urolithiasis—Which Method Is Superior? J Endourol. 2019, 33, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Skolarikos, A.; Alivizatos, G.; Papatsoris, A.; Constantinides, K.; Zerbas, A.; Deliveliotis, C. Ultrasound-guided percutaneous nephrostomy performed by urologists: 10-year experience. Urology. 2006, 68, 495–499. [Google Scholar] [CrossRef]
- Türk, C.; Petr˘ík, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; et al. EAU guidelines on interventional treatment for urolithiasis. Eur Urol. 2016, 69, 475–482. [Google Scholar] [CrossRef] [PubMed]
- de Sousa Morais, N.; Pereira, J.P.; Mota, P.; Carvalho-Dias, E.; Torres, J.N.; Lima, E. Percutaneous nephrostomy vs ureteral stent for hydronephrosis secondary to ureteric calculi: impact on spontaneous stone passage and health-related quality of life—a prospective study. Urolithiasis. 2019, 47, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, Z.G.; Oredein-McCoy, O.; Gerber, L.; Bañez, L.L.; Sopko, D.R.; Miller, M.J.; et al. Emergent ureteric stent vs percutaneous nephrostomy for obstructive urolithiasis with sepsis: patterns of use and outcomes from a 15 -year experience. BJU Int. 2013, 112, E122–E8. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, K.; Utsunomiya, N.; Ichioka, K.; Ueda, N.; Matsui, Y.; Terai, A. Emergency drainage for urosepsis associated with upper urinary tract calculi. J Urol. 2005, 173, 458–462. [Google Scholar] [CrossRef] [PubMed]
- Lynch, M.F.; Anson, K.M.; Patel, U. Current opinion amongst radiologists and urologists in the UK on percutaneous nephrostomy and ureteric stent insertion for acute renal unobstruction: Results of a postal survey. BJU Int. 2006, 98, 1143–1144. [Google Scholar] [CrossRef]
- Yossepowitch, O.; Lifshitz, D.A.; Dekel, Y.; Gross, M.; Keidar, D.M.; Neuman, M.; et al. Predicting the success of retrograde stenting for managing ureteral obstruction. J Urol. 2001, 166, 1746–1749. [Google Scholar] [CrossRef] [PubMed]
- Elbaset, M.; Ezzat, O.; Elgamal, M.; Sharaf, M.; Elmeniar, A.; Abdelhamid, A.; et al. Supranormal differential renal function in adults with ureteropelvic junction obstruction: does it really exist? Indian J Urol. 2020, 36, 205. [Google Scholar] [CrossRef] [PubMed]
- Elbaset, M.A.; Osman, Y.; Elgamal, M.; Sharaf, M.A.; Ezzat, O.; Elmeniar, A.M.; et al. Long-term outcomes after pyeloplasty for pelvi-ureteric junction obstruction in adults associated with renal congenital anomalies: age, sex and renal function matched analysis. Arab J Urol. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.Y.; Bamberger, J.N.; Blum, K.A.; Parkhomenko, E.; Thai, J.; Chandhoke, R.A.; et al. Predicting the impacted ureteral stone with computed tomography. Urology. 2019, 130, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Chandhoke, R.; Bamberger, J.N.; Gallante, B.; Atallah, W.; Gupta, M. Peri-calculus ureteral thickness on computed tomography predicts stone impaction at time of surgery: a prospective study. J Endourol. 2020, 34, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Cevik, I.; Dillioglugil, O.; Akdas, A.; Siegel, Y. Is stent placement necessary after uncomplicated ureteroscopy for removal of impacted ureteral stones? J Endourol. 2010, 24, 1263–1267. [Google Scholar] [CrossRef] [PubMed]
- Sammon, J.D.; Ghani, K.R.; Karakiewicz, P.I.; Bhojani, N.; Ravi, P.; Sun, M.; et al. Temporal trends, practice patterns, and treatment outcomes for infected upper urinary tract stones in the United States. Eur Urol. 2013, 64, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Pearle, M.S.; Pierce, H.L.; Miller, G.L.; Summa, J.A.; Mutz, J.M.; Petty, B.A.; et al. Optimal method of urgent decompression of the collecting system for obstruction and infection due to ureteral calculi. J Urol. 1998, 160, 1260–1264. [Google Scholar] [CrossRef] [PubMed]
- Elbaset, M.; Elkarta, A.; Eraky, A.; Badawy, M.; Sheir, K.; Shokeir, A. Role of pretreatment Doppler ultrasound in the prediction of factors affecting stone-clearance post-shockwave lithotripsy for ureteral stones: a prospective study. Int Urol Nephrol. 2020, 52, 1643–1649. [Google Scholar] [CrossRef]
- Brito, A.H.; Mitre, A.I.; Srougi, M. Ureteroscopic pneumatic lithotripsy of impacted ureteral calculi. Int Braz J Urol. 2006, 32, 295–299. [Google Scholar] [CrossRef]
- Oliver, R.; Wells, H.; Traxer, O.; Knoll, T.; Aboumarzouk, O.; Biyani, C.S.; et al. Ureteric stents on extraction strings: a systematic review of literature. Urolithiasis. 2018, 46, 129–136. [Google Scholar] [CrossRef]
- Legemate, J.D.; Wijnstok, N.J.; Matsuda, T.; Strijbos, W.; Erdogru, T.; Roth, B.; et al. Characteristics and outcomes of ureteroscopic treatment in 2650 patients with impacted ureteral stones. World J Urol. 2017, 35, 1497–1506. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.Y.; Hernandez Bustos, N.; Kambadakone, A.; Eisner, B.; Pareek, G. Emergency ureteral stone treatment score predicts outcomes of ureteroscopic intervention in acute obstructive uropathy secondary to urolithiasis. J Endourol. 2017, 31, 829–834. [Google Scholar] [CrossRef]
- Sarica, K.; Eryildirim, B.; Sahin, C.; Sabuncu, K.; Cetinel, C.; Narter, F. Impaction of ureteral stones into the ureteral wall: Is it possible to predict? Urolithiasis. 2016, 44, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Wenzler, D.L.; Kim, S.P.; Rosevear, H.M.; Faerber, G.J.; Roberts, W.W.; Wolf, J.; Stuart, J. Success of ureteral stents for intrinsic ureteral obstruction. J Endourol. 2008, 22, 295–300. [Google Scholar] [CrossRef]
- Yoshida, T.; Inoue, T.; Taguchi, M.; Omura, N.; Kinoshita, H.; Matsuda, T. Ureteral wall thickness as a significant factor in predicting spontaneous passage of ureteral stones of≤ 10 mm: a preliminary report. World J Urol. 2019, 37, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Morgentaler, A.; Bridge, S.S.; Dretler, S.P. Management of the impacted ureteral calculus. J Urol. 1990, 143, 263–266. [Google Scholar] [CrossRef]
- Alsaikhan, B.; Koziarz, A.; Lee, J.Y.; Pace, K.T. Preoperative alpha- blockers for ureteroscopy for ureteral stones: a systematic review and meta-analysis of randomized controlled trials. J Endourol. 2020, 34, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Koo, K.C.; Yoon, J.-H.; Park, N.-C.; Lee, H.S.; Ahn, H.K.; Lee, K.S.; et al. The impact of preoperative α-adrenergic antagonists on ureteral access sheath insertion force and the upper limit of force required to avoid ureteral mucosal injury: a randomized controlled study. J Urol. 2018, 199, 1622–1630. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
  |
 |
 |
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2021 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.
Share and Cite
Elbaset, M.A.; Edwan, M.; Abouelkheir, R.T.; Ashour, R.; Ramez, M.; Abdelhamid, A.; Osman, Y. Predictors for Retrograde Ureteral Stenting Failure as an Initial Drainage Method for Emergent Complicated Acute Calculus Obstructive Uropathy. Soc. Int. Urol. J. 2021, 2, 229-238. https://doi.org/10.48083/OZUL6913
Elbaset MA, Edwan M, Abouelkheir RT, Ashour R, Ramez M, Abdelhamid A, Osman Y. Predictors for Retrograde Ureteral Stenting Failure as an Initial Drainage Method for Emergent Complicated Acute Calculus Obstructive Uropathy. Société Internationale d’Urologie Journal. 2021; 2(4):229-238. https://doi.org/10.48083/OZUL6913
Chicago/Turabian StyleElbaset, M. A., Mohamed Edwan, Rasha T. Abouelkheir, Rawdy Ashour, Mohamed Ramez, Abdalla Abdelhamid, and Yasser Osman. 2021. "Predictors for Retrograde Ureteral Stenting Failure as an Initial Drainage Method for Emergent Complicated Acute Calculus Obstructive Uropathy" Société Internationale d’Urologie Journal 2, no. 4: 229-238. https://doi.org/10.48083/OZUL6913
APA StyleElbaset, M. A., Edwan, M., Abouelkheir, R. T., Ashour, R., Ramez, M., Abdelhamid, A., & Osman, Y. (2021). Predictors for Retrograde Ureteral Stenting Failure as an Initial Drainage Method for Emergent Complicated Acute Calculus Obstructive Uropathy. Société Internationale d’Urologie Journal, 2(4), 229-238. https://doi.org/10.48083/OZUL6913