

Pulmonary Embolism (PE) to Chronic Thromboembolic Pulmonary Disease (CTEPD): Findings from a Survey of UK Physicians

Abstract
Highlights
- Considerable variability was reported in the follow-up of patients presenting with acute PE and in the awareness and investigation of suspected CTEPD;
- Despite most participants having local guidelines for PE management, less than two-thirds reported that a dedicated PE follow-up clinic was available.
- These data suggest that a national audit should be performed to gain an understanding of the barriers to the timely detection of CTEPD among UK physicians.
Abstract
1. Introduction
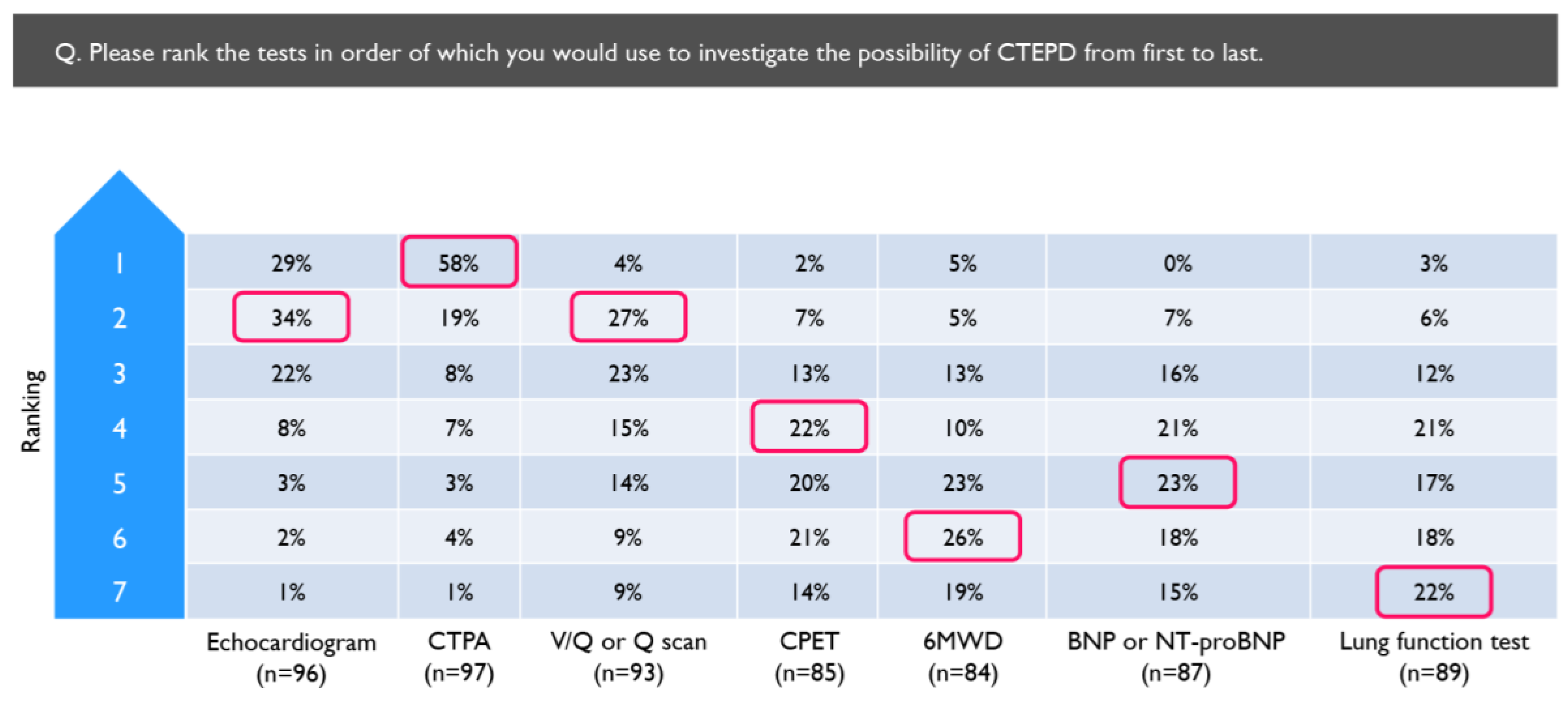
- CTPA is most often used as the first-line of investigation for CTEPD fol-lowing PE despite cardiac echocardiography and V/Q scintigraphy being recommended;
- CTEPH was ranked as the most common cause for persistent breathless-ness post-PE despite it being relatively rare compared to other issues such as deconditioning. This may lead to onward referrals without the appro-priate investigations being conducted;
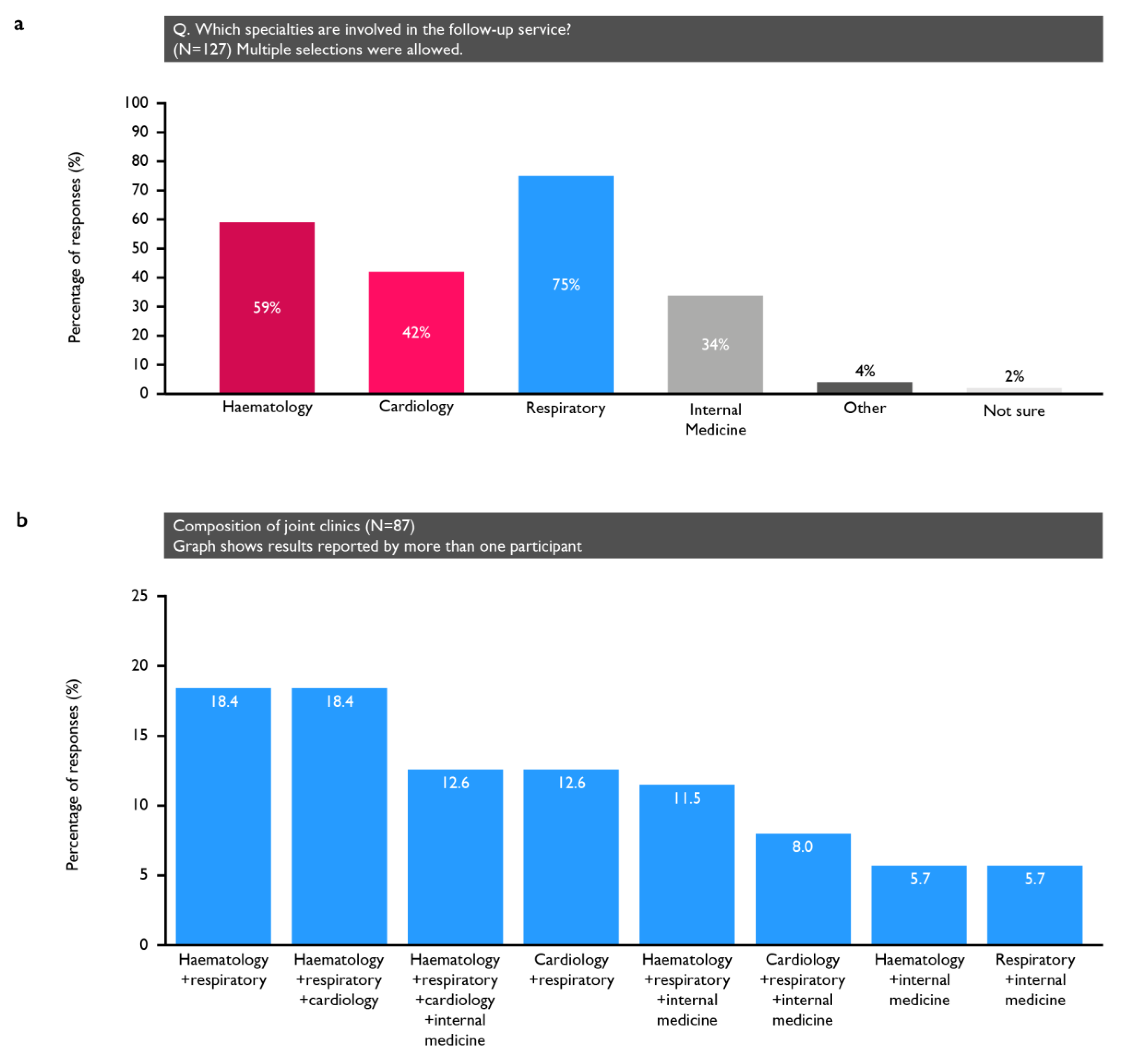
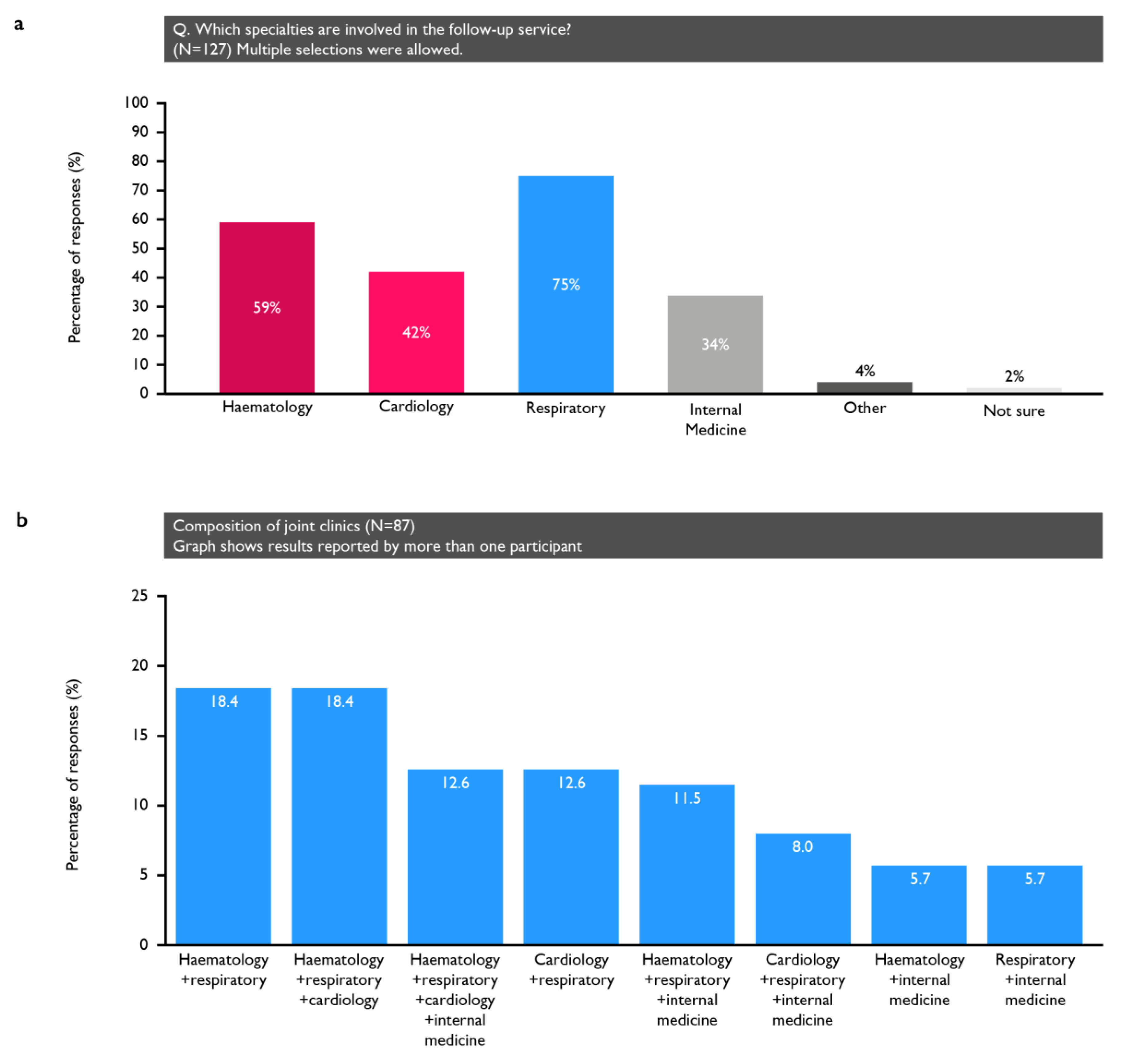
- Haematologists with an interest in thrombosis should be involved in the PE follow-up pathway;
- Protocols for PE follow-up should highlight the need for a retrospective review of the CTPA from the initial PE assessment;
- Hospital protocols should ensure smooth integration of their PE care pathways and ensure that physicians are aware of their nearest specialist PH centre.
2. Materials and Methods
2.1. Data Analysis
2.2. Ethical Statement
3. Results
3.1. Participants
3.2. General Management of PE in the Centres in Which the Respondents Practice
3.3. Experience in Evaluating Suspected CTEPD
4. Discussion
4.1. PE Management
4.2. Use of Imaging Modalities
4.3. Other Tools to Support Post-PE Follow-Up
4.4. Aspects of Post-PE Follow-Up Needing Improvement
4.5. Multidisciplinary Follow-Up of PE
4.6. Referral to PH Centre
4.7. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef] [PubMed]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2022, 61, 2200879. [Google Scholar] [CrossRef] [PubMed]
- Capone, C.; Valentini, A.; Spinillo, S.L.; Klersy, C.; Celentano, A.; Pin, M.; Monterosso, C.; Dore, R.; Bassi, E.M.; Zacchino, M.; et al. Radiological differences between chronic thromboembolic pulmonary disease (CTEPD) and chronic thromboembolic pulmonary hypertension (CTEPH). Eur. Radiol. 2021, 31, 6230–6238. [Google Scholar] [CrossRef]
- Valerio, L.; Mavromanoli, A.C.; Barco, S.; Abele, C.; Becker, D.; Bruch, L.; Ewert, R.; Faehling, M.; Fistera, D.; Gerhardt, F.; et al. Chronic thromboembolic pulmonary hypertension and impairment after pulmonary embolism: The FOCUS study. Eur. Heart J. 2022, 43, 3387–3398. [Google Scholar] [CrossRef] [PubMed]
- Riedel, M.; Stanek, V.; Widimsky, J.; Prerovsky, I. Longterm follow-up of patients with pulmonary thromboembolism. Late prognosis and evolution of hemodynamic and respiratory data. Chest 1982, 81, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Delcroix, M.; Lang, I.; Pepke-Zaba, J.; Jansa, P.; D’Armini, A.M.; Snijder, R.; Bresser, P.; Torbicki, A.; Mellemkjaer, S.; Lewczuk, J.; et al. Long-term outcome of patients with chronic thromboembolic pulmonary hypertension. Circulation 2016, 133, 859–871. [Google Scholar] [CrossRef]
- Quadery, S.R.; Swift, A.J.; Billings, C.G.; Thompson, A.A.R.; Elliot, C.A.; Hurdman, J.; Charalampopoulos, A.; Sabroe, I.; Armstrong, I.J.; Hamilton, N.; et al. The impact of patient choice on survival in chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2018, 52, 1800589. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.-J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 543–603. [Google Scholar]
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2015, 46, 903–975. [Google Scholar]
- Klok, F.A.; Ageno, W.; Ay, C.; Bäck, M.; Barco, S.; Bertoletti, L.; Becattini, C.; Carlsen, J.; Delcroix, M.; van Es, N.; et al. Optimal follow-up after acute pulmonary embolism: A position paper of the European Society of Cardiology Working Group on Pulmonary Circulation and Right Ventricular Function, in collaboration with the European Society of Cardiology Working Group on Atherosclerosis and Vascular Biology, endorsed by the European Respiratory Society. Eur. Heart J. 2021, 43, 183–189. [Google Scholar]
- Ruan, W.; Yap, J.J.; Quah, K.K.; Cheah, F.K.; Phua, G.C.; Sewa, D.W.; Ismail, A.B.; Chia, A.X.; Jenkins, D.; Tan, J.L.; et al. Clinical updates on the diagnosis and management of chronic thromboembolic pulmonary hypertension. Ann. Acad. Med. Singap. 2020, 49, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Ende-Verhaar, Y.M.; van den Hout, W.B.; Bogaard, H.J.; Meijboom, L.J.; Huisman, M.V.; Symersky, P.; Vonk-Noordegraaf, A.; Klok, F.A. Healthcare utilization in chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. J. Thromb. Haemost. JTH 2018, 16, 2168–2174. [Google Scholar] [CrossRef]
- Klok, F.A.; Couturaud, F.; Delcroix, M.; Humbert, M. Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Eur. Respir. J. 2020, 55, 2000189. [Google Scholar] [CrossRef] [PubMed]
- Pepke-Zaba, J.; Delcroix, M.; Lang, I.; Mayer, E.; Jansa, P.; Ambroz, D.; Treacy, C.; D’Armini, A.M.; Morsolini, M.; Snijder, R.; et al. Chronic thromboembolic pulmonary hypertension (CTEPH): Results from an international prospective registry. Circulation 2011, 124, 1973–1981. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Barco, S.; Konstantinides, S.V.; Dartevelle, P.; Fadel, E.; Jenkins, D.; Kim, N.H.; Madani, M.; Matsubara, H.; Mayer, E.; et al. Determinants of diagnostic delay in chronic thromboembolic pulmonary hypertension: Results from the European CTEPH Registry. Eur. Respir. J. 2018, 52, 1801687. [Google Scholar] [CrossRef] [PubMed]
- Delcroix, M.; Torbicki, A.; Gopalan, D.; Sitbon, O.; Klok, F.A.; Lang, I.; Jenkins, D.; Kim, N.H.; Humbert, M.; Jais, X.; et al. ERS statement on chronic thromboembolic pulmonary hypertension. Eur. Respir. J. 2021, 57, 2002828. [Google Scholar] [CrossRef]
- Jing, Z.-C.; Parikh, K.; Pulido, T.; Jerjes-Sanchez, C.; White, R.J.; Allen, R.; Torbicki, A.; Xu, K.-F.; Yehle, D.; Laliberte, K.; et al. Efficacy and Safety of Oral Treprostinil Monotherapy for the Treatment of Pulmonary Arterial Hypertension. Circulation 2013, 127, 624–633. [Google Scholar] [CrossRef]
- Remy-Jardin, M.; Ryerson, C.J.; Schiebler, M.L.; Leung, A.N.C.; Wild, J.M.; Hoeper, M.M.; Alderson, P.O.; Goodman, L.R.; Mayo, J.; Haramati, L.B.; et al. Imaging of pulmonary hypertension in adults: A position paper from the Fleischner Society. Eur. Respir. J. 2021, 57, 531–549. [Google Scholar] [CrossRef]
- Klok, F.A.; Dzikowska-Diduch, O.; Kostrubiec, M.; Vliegen, H.W.; Pruszczyk, P.; Hasenfuß, G.; Huisman, M.V.; Konstantinides, S.; Lankeit, M. Derivation of a clinical prediction score for chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. J. Thromb. Haemost. JTH 2016, 14, 121–128. [Google Scholar] [CrossRef]
- Boon, G.; Ende-Verhaar, Y.M.; Bavalia, R.; El Bouazzaoui, L.H.; Delcroix, M.; Dzikowska-Diduch, O.; Huisman, M.V.; Kurnicka, K.; Mairuhu, A.T.A.; Middeldorp, S.; et al. Non-invasive early exclusion of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: The InShape II study. Thorax 2021, 76, 1002–1009. [Google Scholar] [CrossRef]
- Otero, R.; Bertoletti, L.; Muriel, A.; Siniscalchi, C.; Jimenez, C.; Luis Lobo, J.; Kigitovica, D.; Quintavalla, R.; Rocci, A.; Jara-Palomares, L.; et al. Role of a clinical prediction score in a chronic thromboembolic pulmonary hypertension rule-out strategy. Eur. Respir. J. 2018, 51, 1702576. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Cohn, D.M.; Middeldorp, S.; Scharloo, M.; Büller, H.R.; van Kralingen, K.W.; Kaptein, A.A.; Huisman, M.V. Quality of life after pulmonary embolism: Validation of the PEmb-QoL Questionnaire. J. Thromb. Haemost. JTH 2010, 8, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Asady, E.; Ghanima, W.; Jelsness-Jorgensen, L.P.; Klok, F.A.; Kahn, S.R.; Stromme, H.; Wik, H.S. Health-related quality-of-life questionnaires for deep vein thrombosis and pulmonary embolism: A systematic review on questionnaire development and methodology. Res. Pr. Thromb. Haemost. 2021, 5, e12556. [Google Scholar] [CrossRef] [PubMed]
- Oakden, V.; Cooper, R.; Lim, S.; Inani, M.; Jameel, R.; Waseem, T.; Zahran, M.; Isiaka, Z.; Ganaie, M. Follow-up of acute pulmonary embolism (PE): Need for dedicated PE clinics and multidisciplinary team (MDT) meetings? Eur. Respir. J. 2021, 58, PA507. [Google Scholar]
- Chang, K.Y.; Duval, S.; Badesch, D.B.; Bull, T.M.; Chakinala, M.M.; De Marco, T.; Frantz, R.P.; Hemnes, A.; Mathai, S.C.; Rosenzweig, E.B.; et al. Mortality in Pulmonary Arterial Hypertension in the Modern Era: Early Insights From the Pulmonary Hypertension Association Registry. J. Am. Heart Assoc. 2022, 11, e024969. [Google Scholar] [CrossRef]
- Skoro-Sajer, N.; Kopec, G.; Abe, K.; Forfia, P.; Heresi, G.; Jevnikar, M.; Sheares, K.; Terra-Filho, M.; Whitford, H.; Zhai, Z.; et al. Chronic thromboembolic pulmonary hypertension global cross-sectional scientific survey (CLARITY)—Interim results on the adoption and perception of guidelines. Eur. Heart J. 2022, 43, 1867. [Google Scholar] [CrossRef]
- Boon, G.J.A.M.; Jairam, P.M.; Groot, G.M.C.; van Rooden, C.J.; Ende-Verhaar, Y.M.; Beenen, L.F.M.; Kroft, L.J.M.; Bogaard, H.J.; Huisman, M.V.; Symersky, P.; et al. Identification of chronic thromboembolic pulmonary hypertension on CTPAs performed for diagnosing acute pulmonary embolism depending on level of expertise. Eur. J. Intern. Med. 2021, 93, 64–70. [Google Scholar] [CrossRef]
- Boon, G.J.A.M.; Ende-Verhaar, Y.M.; Beenen, L.F.M.; Coolen, J.; Delcroix, M.; Golebiowski, M.; Huisman, M.V.; Mairuhu, A.T.A.; Meijboom, L.J.; Middeldorp, S.; et al. Prediction of chronic thromboembolic pulmonary hypertension with standardised evaluation of initial computed tomography pulmonary angiography performed for suspected acute pulmonary embolism. Eur. Radiol. 2022, 32, 2178–2187. [Google Scholar] [CrossRef]
- Rousseau, H.; Del Giudice, C.; Sanchez, O.; Ferrari, E.; Sapoval, M.; Marek, P.; Delmas, C.; Zadro, C.; Revel-Mouroz, P. Endovascular therapies for pulmonary embolism. Heliyon 2021, 7, e06574. [Google Scholar] [CrossRef]
- Araszkiewicz, A.; Jankiewicz, S.; Sławek-Szmyt, S.; Klotzka, A.; Grygier, M.; Mularek-Kubzdela, T.; Lesiak, M. Rapid clinical and haemodynamic improvement in a patient with intermediate-high risk pulmonary embolism treated with transcatheter aspiration thrombectomy. Postep. W Kardiol. Interwencyjnej = Adv. Interv. Cardiol. 2019, 15, 497–498. [Google Scholar] [CrossRef]
- Condliffe, R.; Albert, P.; Alikhan, R.; Gee, E.; Horner, D.; Hunter, L.; Jacobs, P.; Limbrey, R.; Newnham, M.; Preston, W.; et al. British Thoracic Society Quality Standards for outpatient management of pulmonary embolism. BMJ Open Respir. Res. 2020, 7, e000636. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Cardiology (n = 50) | Respiratory Medicine (n = 50) | Haematology (n = 25) | Internal Medicine (n = 50) | Overall (N = 175) | |
|---|---|---|---|---|---|
| Title, n (%) | |||||
| Specialty Registrar | 10 (20) | 6 (12) | 0 | 5 (10) | 21 (12) |
| Consultant | 40 (80) | 44 (88) | 25 (100) | 45 (90) | 154 (88) |
| Mean duration of experience in the specialty, years | 16.0 | 15.1 | 14.7 | 16.7 | 15.7 |
| Mean number of patients with PE seen in a year | 53.5 | 74.6 | 55.0 | 52.8 | 59.5 |
| Primary work setting, n (%) | |||||
| District general hospital/teaching hospital | (66) | (82) | (92) | (94) | (82) |
| PH shared care centre | (12) | (14) | (4) | (4) | (9) |
| PH centre | (22) | (4) | (4) | (2) | (9) |
| Hospital setting, n (%) | |||||
| Public | 46 (92) | 47 (94) | 19 (76) | 45 (90) | 157 (90) |
| Private | 0 | 0 | 3 (12) | 1 (2) | 4 (2) |
| Both | 4 (8) | 3 (6) | 3 (12) | 4 (8) | 14 (8) |
| UK region of practice (%) | |||||
| Northeast England | 2 | 4 | 4 | 6 | 4 |
| Northwest England | 12 | 16 | 8 | 8 | 11 |
| East Midlands | 8 | 8 | 12 | 12 | 10 |
| West Midlands | 8 | 12 | 12 | 10 | 10 |
| Yorkshire and the Humber | 2 | 14 | 4 | 4 | 6 |
| Southeast England | 8 | 2 | 4 | 18 | 9 |
| Southwest England | 6 | 10 | 8 | 4 | 7 |
| East of England | 8 | 4 | 12 | 10 | 8 |
| London | 32 | 26 | 32 | 20 | 27 |
| Scotland | 10 | 2 | 4 | 4 | 5 |
| Wales | 2 | 2 | 0 | 4 | 2 |
| Northern Ireland | 2 | 0 | 0 | 0 | 1 |
| Cardiology (n = 50) | Respiratory Medicine (n = 50) | Haematology (n = 25) | Internal Medicine (n = 50) | Overall (N = 175) | |
|---|---|---|---|---|---|
| Respondents who routinely investigate the possibility of suspected CTEPD in patients following acute PE, n (%) | 34 (68) | 35 (70) | 12 (48) | 16 (32) | 97 (55) |
| Patients in which these physicians routinely investigate the possibility of suspected CTEPD | n = 34 | n = 35 | n = 12 | n = 16 | n = 97 |
| In all patients, including asymptomatic patients, n (%) | 6 (18) | 11 (31) | 1 (8) | 3 (19) | 21 (22) |
| In patients who are symptomatic at the 3-month follow-up visit, n (%) | 24 (71) | 27 (77) | 11 (92) | 12 (75) | 74 (76) |
| In patients with a large clot burden at acute presentation, n (%) | 20 (59) | 23 (66) | 9 (75) | 9 (56) | 61 (63) |
| In thrombolysed patients, n (%) | 8 (24) | 20 (57) | 7 (58) | 6 (38) | 41 (42) |
| In patients with thrombophilias, n (%) | 12 (35) | 14 (40) | 1 (8) | 5 (31) | 32 (33) |
| In patients with recurrent VTE, n (%) | 21 (62) | 23 (66) | 7 (58) | 9 (56) | 60 (62) |
| In patients with sPAP >60 mmHg at acute presentation, n (%) | 14 (41) | 18 (51) | 5 (42) | 8 (50) | 45 (46) |
| Other, n (%) | 1 (3) | 2 (6) | 0 | 0 | 3 (3) |
| Tests used to investigate the possibility of CTEPD | n = 34 | n = 35 | n = 12 | n = 16 | n = 97 |
| Echocardiogram (%) | |||||
| Always/sometimes | 91/9 | 83/9 | 83/17 | 56/38 | 81/14 |
| Occasionally/never | 0/0 | 9/0 | 0/0 | 6/0 | 4/0 |
| CTPA (%) | |||||
| Always/sometimes | 79/21 | 60/37 | 25/67 | 69/19 | 64/32 |
| Occasionally/never | 0/0 | 3/0 | 8/0 | 13/0 | 4/0 |
| V/Q or Q scan (%) | |||||
| Always/sometimes | 21/56 | 43/51 | 25/58 | 6/56 | 27/55 |
| Occasionally/never | 21/3 | 6/0 | 17/0 | 38/0 | 18/1 |
| CPET (%) | |||||
| Always/sometimes | 18/38 | 23/43 | 8/50 | 6/44 | 16/42 |
| Occasionally/never | 32/12 | 31/3 | 33/8 | 31/19 | 32/9 |
| 6MWD (%) | |||||
| Always/sometimes | 26/38 | 23/46 | 17/50 | 13/50 | 22/44 |
| Occasionally/never | 21/15 | 26/6 | 33/0 | 19/19 | 24/10 |
| BNP or NT-proBNP (%) | |||||
| Always/sometimes | 53/35 | 34/37 | 17/58 | 25/38 | 37/39 |
| Occasionally/never | 6/6 | 14/14 | 25/0 | 31/6 | 15/8 |
| Lung function test (%) | |||||
| Always/sometimes | 47/35 | 49/34 | 50/33 | 25/44 | 44/36 |
| Occasionally/never | 15/3 | 11/6 | 17/0 | 25/6 | 15/4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pepke-Zaba, J.; Howard, L.; Kiely, D.G.; Sweeney, S.; Johnson, M. Pulmonary Embolism (PE) to Chronic Thromboembolic Pulmonary Disease (CTEPD): Findings from a Survey of UK Physicians. Adv. Respir. Med. 2024, 92, 45-57. https://doi.org/10.3390/arm92010007
Pepke-Zaba J, Howard L, Kiely DG, Sweeney S, Johnson M. Pulmonary Embolism (PE) to Chronic Thromboembolic Pulmonary Disease (CTEPD): Findings from a Survey of UK Physicians. Advances in Respiratory Medicine. 2024; 92(1):45-57. https://doi.org/10.3390/arm92010007
Chicago/Turabian StylePepke-Zaba, Joanna, Luke Howard, David G. Kiely, Shruti Sweeney, and Martin Johnson. 2024. "Pulmonary Embolism (PE) to Chronic Thromboembolic Pulmonary Disease (CTEPD): Findings from a Survey of UK Physicians" Advances in Respiratory Medicine 92, no. 1: 45-57. https://doi.org/10.3390/arm92010007
APA StylePepke-Zaba, J., Howard, L., Kiely, D. G., Sweeney, S., & Johnson, M. (2024). Pulmonary Embolism (PE) to Chronic Thromboembolic Pulmonary Disease (CTEPD): Findings from a Survey of UK Physicians. Advances in Respiratory Medicine, 92(1), 45-57. https://doi.org/10.3390/arm92010007