Abstract
Introduction: Mild traumatic brain injury (mTBI) in older adults (≥65 years) is often underestimated, despite being associated with significant morbidity. Age-related vulnerability, comorbidities, and medication use may exacerbate outcomes. This study aimed to identify predictors of brain health and functional recovery in older adults following mTBI, focusing on acute symptoms, CT imaging findings, and sociodemographic factors. Methods: We analyzed a cohort of 93 older adult patients with mTBI (GCS 13–15) who were prospectively enrolled at a tertiary neurosurgical center. All patients underwent baseline CT, structured clinical assessment, and follow-up at six months with standardized instruments (Glasgow Outcome Scale–Extended-GOSE, 12-Item Short Form Health Survey (quality-of-life measure)-SF-12, Rivermead Post-Concussion Symptoms Questionnaire-RPQ, Patient Health Questionnaire-9 (depression measure)-PHQ-9, PTSD (Post Traumatics Stress Disorder) Checklist for DSM (Diagnostic and Statistical Manual for Mental Disorders)-PCL-5, Timed up and Go Test (mobility measure-TUG test). Multivariate regression was performed to identify independent predictors of recovery. Results: At six months, 94.9% of older adults achieved functional independence (GOSE ≥ 5), though only 43% attained complete recovery (GOSE = 8). Patients with acute intracranial lesions on CT had worse physical outcomes, including slower mobility (mean TUG 17.6 vs. 16.3 s, p = 0.012). Severe acute headache independently predicted poorer recovery (lower GOSE and SF-12 PCS). Lower educational attainment correlated with worse functional and quality-of-life outcomes, consistent with reduced cognitive reserve. Psychological outcomes (PTSD and depression rates) were not associated with CT findings but were influenced by social support and sex. Prompt anticoagulation reversal in patients on anticoagulants markedly reduced hemorrhagic complications. Discussion: Older adults with mTBI generally maintain independence but experience reduced physical health and mobility compared to younger patients. Predictors of poorer outcomes include severe acute symptoms, CT-detected lesions, advanced age, and lower educational levels. Psychosocial support mitigated mental health complications. Conclusions: mTBI in older adults is not benign. Clinical, imaging, and sociodemographic factors collectively shape recovery. Early identification of high-risk patients and targeted interventions are essential to preserve brain health and independence in this growing population.
1. Introduction
Mild traumatic brain injury (mTBI) is a significant clinical and public health issue, which is often underestimated despite its potential long-term neurological and psychosocial consequences. It is traditionally defined by a Glasgow Coma Scale (GCS) score of 13–15, brief loss of consciousness or confusion (less than 30 min), and post-traumatic amnesia lasting under 24 h. Despite being labeled “mild,” this injury can lead to enduring neurological deficits and reduced quality of life in a subset of patients. Older adults with mTBI are of particular concern. Due to age-related neurobiological changes—such as reduced neuroplasticity, cerebral atrophy, and a higher prevalence of medical comorbidities—older individuals may experience a more difficult recovery even after relatively minor head trauma. Epidemiologically, falls are a leading cause of mTBI in the elderly, and age over 65 is a known risk factor for intracranial hemorrhage even with mild injury. Furthermore, many older patients are on antithrombotic medications (anticoagulants or antiplatelet agents) which can exacerbate bleeding risk and complicate the acute management of brain injuries [1,2,3].
Prior research and clinical observations indicate that advanced age is associated with worse functional outcomes after TBI. Older patients have a higher likelihood of prolonged hospitalization, post-injury disability, and development of post-concussion syndrome compared to younger adults. They also tend to take longer to recover their baseline functional status. However, the specific predictors of outcome within the older adult mTBI population remain less well characterized. Identifying which factors—from acute clinical symptoms to brain imaging abnormalities and patient demographic characteristics—most strongly influence recovery in older mild TBI patients is important for guiding treatment and rehabilitation strategies [1,4].
Neuroimaging, particularly computed tomography (CT), plays a crucial role in the evaluation of mTBI. Cranial CT scans can rapidly detect acute intracranial lesions (such as subdural hematomas, contusions, or traumatic subarachnoid hemorrhage) that classify an injury as “complicated” mTBI. Such findings may portend worse outcomes, especially in older patients who have less physiological reserves to compensate for brain injuries. On the other hand, a normal CT does not guarantee a benign course, as diffuse axonal injury or microstructural damage (often not visible on CT) can still produce significant symptoms. Therefore, it is essential to consider imaging results in conjunction with clinical factors when prognosticating outcomes [5,6].
Sociodemographic factors and baseline patient characteristics might also modulate recovery. Variables such as age (as a continuous variable even among seniors), sex, educational level, marital status, living situation, and employment/retirement status could influence both the likelihood of complications and the trajectory of rehabilitation. For instance, lower educational attainment has been associated with poorer cognitive outcomes after brain injury, potentially reflecting lower cognitive reserve. Social support (e.g., having a spouse or caregiver at home) might mitigate psychological stress and facilitate adherence to recovery recommendations, whereas social isolation could worsen outcomes. In the context of older patients, factors such as living alone or being widowed might correlate with slower or less complete recoveries due to reduced assistance and engagement in daily activities [7,8].
Acute clinical presentation is another critical piece of the puzzle: the severity and nature of symptoms in the immediate aftermath of the injury may reflect the extent of brain dysfunction and predict long-term outcomes. Symptoms such as severe headache, vomiting, loss of consciousness, or focal neurological deficits in the emergency setting might indicate a more significant injury (even if classified as “mild” by GCS) and could herald a more complicated recovery course. In contrast, an older patient with an ostensibly mild injury but who remains relatively asymptomatic during acute evaluation may be more likely to recover swiftly [3,9].
Given these considerations, we undertook a detailed analysis of older adults with mTBI, leveraging data from a prospective cohort study. Our aim was to determine which factors best predict six-month outcomes in older patients, specifically examining (1) acute injury characteristics and symptoms, (2) CT neuroimaging findings, and (3) sociodemographic and background factors. We hypothesized that older patients with more severe acute symptoms and with intracranial injuries on CT would have poorer functional and quality-of-life outcomes. We also anticipated that markers of vulnerability (such as very advanced age, lower education, or lack of social support) would correlate with worse recovery. By focusing exclusively on the older subset, our analysis aimed to inform a more tailored approach to managing mild TBI in the elderly—an increasingly important issue as the population ages and the number of older individuals sustaining head injuries continues to rise. Notably, Serbia has one of the highest proportions of elderly people in the world (over 17% aged 65+), underscoring the local importance of understanding geriatric mTBI outcomes. This study is among the first prospective analyses of older mTBI patients in our region, helping to fill a gap in data and offering insights distinct from prior studies in other countries [1,10].
2. Materials and Methods
2.1. Study Design and Participants
This research was designed as a combined prospective–retrospective cohort study, conducted at a single tertiary care center (Department of Neurosurgery, University Clinical Center of Vojvodina, Novi Sad, Serbia) between June 2022 and May 2023. The study included adult patients with mild traumatic brain injury who were admitted to the neurosurgery service. For the present analysis, we focused exclusively on older adult patients, defined as those aged 65 years or above. Out of the 350 patients in the overall cohort, 93 met this age criterion and form the study sample described here.
All patients had mild TBI as defined by clinical criteria (GCS score of 13–15 upon initial evaluation). Additional inclusion criteria included having undergone a head CT scan at admission (which was indicated for all patients due to their presenting symptoms or high-risk mechanisms) and the ability to participate in follow-up assessments. Patients with significant pre-existing neurological conditions (e.g., dementia, Parkinson’s disease, prior stroke with deficits) or severe psychiatric disorders were excluded to avoid confounding influences on outcomes; specifically, five such older patients were excluded, ensuring that follow-up measures predominantly reflected the impact of the index TBI rather than other progressive illnesses. This ensured that follow-up measures predominantly reflected the impact of the index TBI rather than other progressive illnesses.
2.2. Acute Clinical Assessment and Management
Upon admission (typically through the emergency department), each patient underwent a standardized acute evaluation. This included a thorough clinical neurological examination and detailed documentation of acute injury-related symptoms. The specific acute symptoms recorded were: presence and severity of headache (patients were asked to rate their headache intensity, if any, on a numeric scale), occurrence of nausea and/or vomiting, any reported or witnessed loss of consciousness (and its duration if applicable), the presence of confusion or disorientation, and any focal neurological deficits noted (such as limb weakness, sensory loss, speech difficulties, or gait abnormalities). Vital signs were monitored, and GCS was reassessed periodically during the observation period.
All patients received initial management according to established mild TBI protocols. This included close neurological observation (hourly checks of orientation, pupils, limb strength, etc., during the first 6–24 h, as indicated), pain control, and antiemetic therapy if needed for nausea. Importantly, special attention was given to patients who were on anticoagulant therapy prior to injury. In our cohort of older patients, approximately 4% were taking an oral anticoagulant (such as warfarin or a direct oral anticoagulant) for unrelated medical conditions (e.g., atrial fibrillation). For those individuals, if any intracranial hemorrhage was detected on CT or strongly suspected clinically, prompt reversal of anticoagulation was undertaken. Reversal agents (vitamin K, prothrombin complex concentrates or fresh frozen plasma, and/or specific antidotes if available) were administered as per hospital protocol in order to mitigate the risk of hemorrhage expansion.
2.3. Neuroimaging and Injury Classification
All participants underwent non-contrast head CT imaging soon after arrival, typically within the first hour of evaluation. CT scans were interpreted by board-certified radiologists and neurosurgeons. We recorded the findings of each scan. For the purpose of the analysis, patients were categorized based on CT results into two groups:
- Uncomplicated mTBI: no acute intracranial pathology visible on CT.
- Complicated mTBI: presence of acute traumatic intracranial lesions on CT.
The types of CT abnormalities observed in the complicated cases included acute subdural hematomas, cerebral contusions, traumatic subarachnoid hemorrhage, and a few instances of small epidural hematomas. None of the patients had injuries severe enough to warrant immediate neurosurgical intervention at presentation (by definition, those would typically be considered more than mild TBI). However, patients with lesions were kept under careful observation and repeat neuroimaging was performed as needed (for example, a follow-up CT after 24 h for larger but nonsurgical hemorrhages, per our department’s usual care). This categorization of “uncomplicated” vs. “complicated” mTBI follows standard definitions, where a mild TBI is considered complicated if neuroimaging reveals an acute intracranial abnormality.
We also noted extracranial injuries or factors that might influence recovery (for instance, some patients had minor orthopedic injuries from their falls, which could affect mobility during follow-up, but these were generally mild).
2.4. Sociodemographic and Clinical Data Collection
Baseline sociodemographic data were collected through patient interviews and medical record reviews. These data included age (recorded in years), sex, highest educational level attained, marital status (with a particular note of whether the patient lived alone or with family/a partner), and employment status at the time of injury. Given the age group, the vast majority of these patients were retired from full-time employment; we noted whether they were engaged in any part-time work or active volunteer roles, as an indicator of their lifestyle prior to injury.
We also documented relevant medical histories, including major comorbidities (such as hypertension, diabetes, cardiac disease), and prior psychiatric history (e.g., depression or anxiety disorders), since these could potentially affect post-TBI recovery or symptom reporting. The use of alcohol at the time of injury was recorded (e.g., whether the injury was alcohol-related or not), as intoxication can influence both injury severity and acute symptomatology.
2.5. Outcome Measures at Six Months
Patients were scheduled for follow-up evaluations at 1 month and 6 months post-injury. The primary endpoint was the 6-month outcome. Follow-up was conducted in clinic or by phone when necessary.
We employed standardized instruments: GOSE (global functional recovery; independence defined as GOSE ≥ 5), SF-12 (Physical and Mental Component Summary scores), RPQ (post-concussion symptoms), PCL-5 (probable PTSD if ≥33), PHQ-9 (depression severity), and TUG plus 10 m walk (mobility/balance).
All evaluators were trained and encouraged patients (and family where present) to report ongoing issues candidly.
2.6. Statistical Analysis
We first performed descriptive analyses to summarize the characteristics of the older adult mTBI subgroup and their outcomes. Continuous variables (such as age, GOSE score, SF-12 scores) are presented as means ± standard deviations, and categorical variables (e.g., presence of CT lesion, or achieving independent status) as counts and percentages.
To explore predictors of outcomes, we conducted both univariate and multivariate analyses:
Univariate analysis: we used independent-samples t tests or Mann–Whitney U tests (as appropriate based on data distribution) to compare mean outcome scores between groups (e.g., CT lesion vs. no lesion; severe headache vs. no headache; higher vs. lower education). Chi-square tests were employed for categorical outcome comparisons (e.g., proportion independent in CT+ vs. CT− groups). Pearson or Spearman correlation coefficients were calculated to examine relationships between continuous predictors (such as age in years) and outcome measures.
Multivariate Analysis: To identify independent predictors, we built multiple linear regression models for continuous outcomes (GOSE treated as an interval score, SF-12 PCS, SF-12 MCS, RPQ score, etc.) and logistic regression models for binary outcomes (such as the presence of significant post-concussion syndrome, defined by RPQ above a threshold, or inability to return to independent community mobility). Predictor variables entered into these models included: age (continuous), sex, education level (dichotomized into higher vs. lower education for some analyses), living situation (not alone vs. alone), acute CT finding (lesion vs. none), and acute symptom severity markers (presence of severe headache, occurrence of vomiting, loss of consciousness). We also included anticoagulation status (yes/no) in outcome models related to complications.
Model selection followed a stepwise approach, retaining factors with p < 0.05. We checked assumptions of regression (linearity, homoscedasticity, normality of residuals) and goodness-of-fit (using R2 for linear models and Hosmer–Lemeshow test for logistic models). Due to the sample size, we were cautious about overfitting; thus, we limited the number of predictors in any given model to ensure a subject-to-variable ratio that maintains statistical power.
All statistical analyses were conducted using IBM SPSS (Statistical Package for the Social Sciences) version 26 (IBM Corp., Armonk, NY, USA). A two-tailed p < 0.05 was considered statistically significant for hypothesis testing.
Ethical approval for the study was obtained from the institutional ethics committee, and all participants (or their legal guardians) provided informed consent for inclusion in the research and for follow-up contact.
3. Results
3.1. Cohort Characteristics and Overall Outcomes
The older adult mTBI cohort (n = 93) had ages ranging from 65 to 89 years, with a mean age of 72.1 ± 6.8 years. Just over half of the patients were male (53.8%), reflecting a slightly more balanced sex ratio than typically seen in younger TBI cohorts (where males often predominate). The majority of these injuries resulted from low-level falls (approximately 68% were falls from standing height, e.g., slips in the bathroom or trips on uneven ground). The remainder were due to causes such as road traffic accidents (15%), accidental strikes to the head (e.g., objects falling, 10%), or assault (rare, 2%).
On initial CT imaging, 46% of patients had an acute intracranial lesion (complicated mTBI)—most frequently small subdural hematomas (n = 20) or contusions (n = 15)—while 54% had no acute findings (uncomplicated mTBI). No patient required neurosurgical intervention (Figure 1).
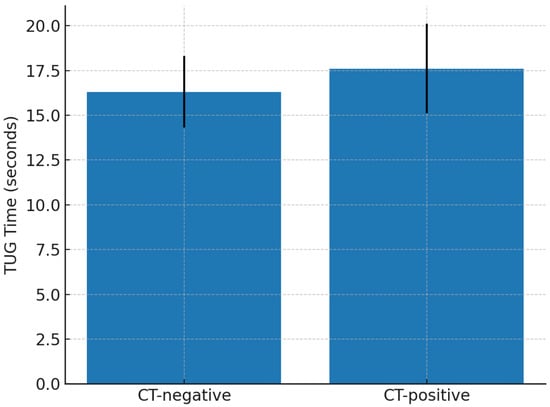
Figure 1.
Comparison of TUG performance at six months by CT findings in older adults with mTBI.
At the six-month follow-up, most older patients demonstrated good recovery, but some deficits persisted in certain domains. As shown in Figure 2, nearly all patients (94.9%) attained functional independence (GOSE ≥ 5) by six months. The median GOSE was 7 (IQR 6–8), with 43% reaching full recovery (GOSE = 8), while 5% remained at GOSE 4 (moderate disability); none had severe disability or had died.
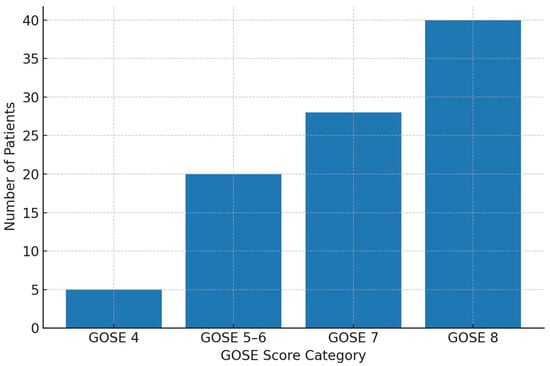
Figure 2.
GOSE distribution in older adults with mTBI.
Approximately 74% of patients had resumed their pre-injury social and leisure activities by 6 months, whereas ~26% reported persistent limitations (e.g., reduced outings or exercise) due to lingering symptoms. Notably, none of the older adults were expected to return to work in the traditional sense, as all were retired; thus, “return to work” rates (often reported in TBI outcomes) are not applicable here. Instead, we focused on social reintegration and independent living as key outcome indicators for this age group.
All basic descriptive data are given in Table 1.

Table 1.
Characteristics of older adult patients with mTBI (n = 93).
Older patients’ six-month health-related quality of life reflected residual physical deficits: the mean SF-12 Physical Component score was ~60 (well below the population mean of 50), whereas the mean Mental Component score was ~70 (above population norms). Post-concussion symptoms were generally mild (mean RPQ 5.4), with only 11% meeting the criteria for post-concussion syndrome; similarly, probable PTSD (8.6% of patients) and moderate depression (3.2%) were uncommon. Mobility testing still showed some impairment (mean TUG 17.8 s, slower than age-normative ~10 s).
In summary, by six months post-injury, most older adults with mTBI had a good outcomes in terms of independence and mental health, but they exhibited greater physical health deficits and functional slowing compared to a younger cohort. There was considerable individual variability, prompting a closer look at which factors accounted for who did well vs. who struggled.
3.2. Predictors of Outcome in Older Adults
We next analyzed how various acute factors and patient characteristics were associated with the range of outcomes observed in our older mTBI patients. The key findings regarding predictors of brain health and recovery are outlined below (Table 2).
Table 2.
Predictors of outcome in older adults with mTBI.
Acute clinical presentation: the severity of acute symptoms had a strong relationship with long-term outcomes. In particular, an intense acute headache was a significant predictor of poorer recovery. Older patients who reported a severe headache (for instance, rating it ≥7 on a 0–10 pain scale) in the emergency phase had, on average, a lower GOSE at six months (mean GOSE ~6.3) compared to those with no headache or mild headache (mean GOSE ~7.1). They also had worse physical health scores (SF-12 PCS lower by ~15 points). Other acute symptoms exhibited correlations in the univariate analysis: patients who experienced vomiting after the injury or had a brief loss of consciousness tended to have lower functional outcomes and more post-concussion symptoms at follow-up than those who did not. However, in our multivariate regression, which included multiple symptom variables simultaneously, headache remained the only independent symptom predictor of outcome (p < 0.01), whereas vomiting or LOC did not independently predict outcome once headache severity was accounted for. This is likely due to overlap among symptoms—for example, those who vomited often had a severe headache as well, implying a more intense overall injury event. Essentially, the presence of a more severe acute post-traumatic symptom complex (with headache being a convenient marker for it) portended a more complicated recovery in older patients. On the other hand, older patients who remained relatively symptom-free in the acute setting almost uniformly achieved excellent recovery, confirming that a benign early clinical presentation is a good sign even in the elderly.
Neuroimaging findings: CT scan results were associated with differences in physical outcomes. Older patients with an acute intracranial lesion on CT (complicated mTBI) had worse outcomes on several measures than those with normal CT scans. To illustrate this, the mean GOSE score was 6.9 for CT-positive patients vs. 7.4 for CT-negative patients (p = 0.025), indicating that CT-positive patients were more likely to have residual functional limitations. Additionally, CT-positive patients had significantly slower mobility: their average TUG time was 17.6 s compared to 16.3 s in CT-negative patients (p = 0.012). Similarly, 10 m walk times were slower (7.86 s vs. 7.22 s, p = 0.010). These objective differences suggest that intracranial injuries seen on CT (even if small) translated into tangible physical impairments such as reduced balance or gait speed in many older individuals. Importantly, CT findings did not predict psychological outcomes. The proportion of patients meeting criteria for PTSD or depression did not differ depending on whether a CT lesion was present (for example, PTSD incidence ~9% in CT+ vs. ~8% in CT−, p = 0.57; depression incidence ~12% in CT+ vs. ~10% in CT−, p = 0.60). Additionally, the SF-12 Mental Component scores were nearly identical between CT-positive and CT-negative groups (~70 vs. 69, p = 0.97). In other words, an older patient’s risk for developing psychological distress after mTBI appeared unrelated to the presence of a visible brain injury on the initial CT. This finding underscores that structural brain damage (as detected by CT) primarily affected physical and neurological function, whereas mental health outcomes were driven by other factors (perhaps individual susceptibility, coping mechanisms, or social environment).
Sociodemographic factors: the analysis revealed that certain patient characteristics significantly influenced recovery among older adults:
Age (within the older group): even within our 65+ cohort, increasing age was associated with slightly worse outcomes. In a regression model, each additional year of age had a small negative effect on functional recovery (β ≈ −0.012 per year for GOSE, p = 0.026) and on mobility (older patients needed more time on TUG, correlation r ≈ +0.20, p < 0.05). In practical terms, an 85-year-old patient tended to have slightly more difficulty recovering than a 65-year-old patient, likely due to frailty and other age-related factors. Thus, “older old” patients may merit special attention, even if all are technically seniors.
Educational attainment: lower education was clearly linked with worse outcomes. Older patients who had not completed high school had a significantly lower mean SF-12 PCS (55.4 vs. 79.9 for those with higher education, p < 0.001) and lower SF-12 MCS (62.8 vs. 71.7, p = 0.002). They also had lower GOSE scores (mean 6.65 vs. 7.18, p = 0.001). Moreover, on objective tests, those with lower education performed worse (TUG 18.96 s vs. 16.47 s, p < 0.001). These differences remained significant even after adjusting for age and CT findings in multivariate analysis. The results support the concept of cognitive reserve: more educated individuals may better compensate for brain injury deficits, or they might engage in more active rehabilitation strategies, leading to improved outcomes. Conversely, patients with limited education (possibly reflecting cognitive baseline differences or health literacy issues) might struggle more and require additional support to achieve the same recovery.
Sex: in the full sample (younger + older), female sex was associated with reporting higher levels of post-traumatic symptoms (like depression and PTSD). Within the older group, we observed a similar trend: older female patients had slightly higher PCL-5 and PHQ-9 scores on average than older males, and they reported post-concussion symptoms (RPQ) more frequently. For example, 12% of older women vs. 6% of older men met the criteria for probable PTSD (a non-significant difference given sample size, but trend-wise higher), and women had a slightly higher mean RPQ (by ~2 points). Female patients also had lower SF-12 physical scores (perhaps due in part to baseline health differences). These patterns suggest that female sex may be a risk factor for experiencing more psychological or symptomatic burden after mTBI, which is consistent with some literature on TBI outcomes. While the exact reasons are not fully clear, hypotheses include hormonal differences, differences in reporting, or psychosocial factors.
Social support and living situation: having a partner or not living alone was associated with better mental health outcomes. Older adults who were married or cohabiting had higher SF-12 MCS scores (by ~5 points on average) and tended to have lower depression scores than those who were single, widowed, or living alone, though these differences did not always reach statistical significance. For instance, only 8% of those with a partner had PHQ-9 ≥ 5 (mild depression or more) vs. 15% of those living alone (this difference in proportions was not large enough to be conclusive in our sample, p = 0.18). We also found that unemployment status was universally high (100%) in the 65+ group since they were essentially all retired, so employment could not be analyzed as a discriminator within this older cohort. However, engagement in community activities (anecdotal data from patient interviews) appeared helpful; patients who continued to have hobbies or engage in social visits tended to report a better sense of well-being. Overall, these observations align with the idea that socially vulnerable patients (i.e., those who are isolated or lack support) may face a more difficult recovery. They might be more prone to feelings of anxiety or have less assistance in overcoming physical challenges, compared to those with strong family support.
Anticoagulation and complication prevention: although only a small subset of our older patients was on anticoagulant therapy at injury (4% of the sample), the management of these cases was instructive. Among the four anticoagulated patients, two had delayed or incomplete anticoagulation reversal (due to late presentation or initially unrecognized medication use); both of those patients developed intracranial hemorrhagic complications (one expanding subdural hematoma requiring later surgical drainage, and one hemorrhagic contusion that led to neurological worsening). In contrast, the other two patients received immediate anticoagulation reversal on admission and avoided any significant hemorrhage progression. They recovered similarly to non-anticoagulated patients, with no notable differences in six-month outcomes. While numbers are too small for statistical analysis, this stark comparison illustrates the critical importance of rapid anticoagulation reversal in older mTBI patients to protect brain health. It suggests that proactive acute management can directly influence outcomes by preventing secondary brain injury. None of the promptly reversed patients had any decline in GOSE due to hemorrhagic complications, whereas the patient who required surgery had the lowest GOSE (5) in the cohort. These findings underscore a practical point: identifying those on blood thinners and acting swiftly can be a life- and function-saving action.
Finally, we synthesized these findings in a multivariate context. In a multiple linear regression predicting the GOSE score at six months for older patients (with GOSE treated as a continuous outcome 1–8), we included age, sex, education, CT lesion presence, and acute headache severity as predictors. The model was significant (F(5,87) ≈ 3.6, p = 0.005) and explained roughly 15% of the variance in GOSE outcomes (adjusted R2 = 0.13). Within this model, the two variables that retained independent significance were education (β = +0.267, p = 0.010)—indicating higher education predicted better GOSE—and age (β = −0.012 per year, p = 0.026)—indicating that, even for 65+ ages, older age predicted slightly worse GOSE. Presence of a CT lesion showed a negative effect (point-biserial r = −0.21 with GOSE) but did not reach statistical significance in the multivariate model (possibly due to overlap with headache or age effects), and headache severity similarly had a negative coefficient that fell short of significance when other factors were accounted for. This suggests that, in older adults, no single factor overwhelmingly determines outcome; rather, it is the combination of factors that shapes recovery. A patient with multiple risk factors (for example, an 80-year-old with low education, a severe initial headache, and a contusion on CT) is likely to have a considerably harder recovery than a 66-year-old highly educated patient with none of those risk factors. This multifactorial nature of outcome aligns with the clinical reality that mild TBI recovery in older people is influenced by an interplay of injury severity, brain reserve, and support systems.
4. Discussion
Our study provides a clinically focused analysis of older adults with mild traumatic brain injury, highlighting the predictors of brain health and functional recovery in this population. Our findings reinforce that even so-called “mild” TBIs can have meaningful consequences for older patients, and they shed light on which factors clinicians should consider when stratifying risk and planning follow-up. These observations are broadly consistent with prior research on TBI prognostic factors. Notably, our study is the first to examine geriatric mTBI outcomes in Serbia; in the absence of national health registry data on long-term TBI outcomes, this work provides unique local evidence to inform healthcare planning for older adults.
Overall, the prognosis for older mild TBI patients was positive in terms of survival and basic independence, but many experienced residual effects. Nearly all patients in our cohort were living independently at six months, which is reassuring. However, only about half achieved a full recovery with no complaints, and a substantial minority had ongoing symptoms or activity limitations. Notably, physical functioning was an area of deficit for several older patients—evidenced by lower SF-12 physical scores and slower mobility tests relative to their younger counterparts. This suggests that, while older individuals often “get by” after mTBI, they may do so at a lower level of physical ability (perhaps avoiding certain activities or accepting a new baseline of fatigue or unsteadiness) [1,11,12].
The predictor analysis offers insights into why some older patients do worse and how we might intervene.
Acute injury severity (clinical): we found that the initial clinical picture carries prognostic weight. In particular, an older patient who presents with severe headache and related symptoms is signaling a higher risk case. This aligns with clinical intuition and other studies that link acute symptom load to outcomes. For clinicians, this means that, even if an elderly patient’s CT scan is normal, persisting intense symptoms in the ED (such as uncontrolled headache or repeated vomiting) are a red flag. Our results support advising such a patient (and family) that additional rest and gradual return to activity will likely be needed, and arranging early follow-up (e.g., at a dedicated concussion clinic) to monitor for post-concussive syndrome. It may also inform decisions on initial disposition—for example, admitting an older mTBI patient for observation if they have worrisome symptoms, even if imaging is normal, could be beneficial. Conversely, an older patient with very mild acute symptoms can likely be managed more conservatively [1,13].
Neuroimaging (CT): the presence of an acute intracranial lesion in an older mTBI patient is not to be taken lightly. Our data show that these patients had measurably worse functional outcomes. This emphasizes that “complicated mTBI” in the elderly might need to be approached more like a moderate TBI in terms of vigilance and rehabilitation. That said, it was illuminating that CT lesions did not predict psychological sequelae. This highlights an important point: structural injury and emotional trauma are somewhat independent aspects of mTBI outcomes. An older person can be quite shaken or depressed even if their scan is clean, or, conversely, they can have a brain bleed but maintain good spirits and cognition. Therefore, comprehensive care for these patients should encompass both medical management of the physical injury and attention to psychological health, regardless of CT findings. Patients with CT lesions should ideally seek physical therapy (for balance/gait) and perhaps more frequent neurological check-ups, whereas all patients (CT lesion or not) should be screened for mood or anxiety issues in follow-up [14,15].
Education and cognitive reserve: one striking result was the impact of education on recovery. Those with higher education did better overall, consistent with the idea that cognitive reserve mitigates the effects of brain insults. Practically, this suggests that older patients with limited formal education might benefit from more proactive cognitive rehabilitation and support. For example, occupational therapy focusing on memory strategies or cognitive exercises could be offered if they report cognitive difficulties. It also underscores the importance of clear communication and education about injury to patients: those with lower health literacy may need more guidance on what to do post-discharge (e.g., activity pacing, danger signs to watch for, etc.). We should not assume that all patients understand or know how to manage post-concussion symptoms; tailored counseling is particularly vital for those who might otherwise be less equipped to navigate recovery on their own [16,17].
Social support: our findings, though not all statistically significant, hinted that older adults with strong social support networks tend to fare better, especially in mental health. This is in line with broad TBI research where social support correlates with better outcomes. For clinicians, an implication is to assess the social situation: does the patient have someone at home? Are they engaged in social activities? If an older patient is socially isolated, referrals to social services or community programs (such as senior centers, fall prevention classes, or head injury support groups) could be beneficial. Family education is also key; family members should be informed about the potential for subtle personality or cognitive changes and how to be supportive (for example, encouraging routine, providing transportation, helping with remembering medical appointments or medications). Our results show that isolation can worsen subjective recovery, meaning that part of the treatment for these patients might extend beyond traditional medicine into the realm of community and family interventions [18,19].
Gender differences: although our study was not able to analyze sex differences in real depth, we observed a trend that older women reported more emotional and post-concussive symptoms. This is consistent with some literature suggesting women (including older women) might experience PCS more or be more likely to report symptoms. The reasons for this could be biological (e.g., hormonal factors) or psychosocial (women may be more forthcoming about symptoms). Regardless, awareness of this trend means practitioners should ensure female patients are carefully screened and that their symptoms are validated and managed (and not dismissed as “just stress”, for instance). At the same time, lower symptom reporting in men does not necessarily mean an absence of issues; men might under-report due to stoicism. Thus, both groups require open-ended questioning at follow-ups to draw out any ongoing difficulties [20,21,22,23].
Practically, these findings support a more tailored, proactive approach to managing older adults after a mild TBI. Clinicians should maintain a high index of suspicion and follow-up for those older patients who exhibit any red flags—be it significant acute symptoms or a positive head CT. Early referral to rehabilitation services (physical, occupational, and vestibular therapy) should be considered for high-risk patients to address balance, mobility, and cognitive complaints before they lead to long-term disability. Simultaneously, attention must be given to the psychosocial context: engaging family members in the recovery process, educating patients and caregivers about what to expect, and connecting those who are isolated with community resources could mitigate some of the negative outcomes associated with social vulnerability [24].
From a healthcare systems perspective, the study underscores the need for integrated care pathways for geriatric TBI. Such pathways might include routine cognitive and depression screening for older TBI patients, scheduled follow-ups, and a multidisciplinary team (including geriatric specialists, rehabilitation therapists, and social workers) to address the myriad factors influencing recovery.
In summary, while most older adults with mild TBI do recover to a large extent, a significant subset experiences persistent difficulties. By identifying who those patients are early—using the predictors identified in this study—we have the opportunity to intervene and potentially improve their outcomes. Ensuring that “mild” does not equate to “neglected” in this population will help improve brain health and functional independence for the growing number of older individuals who sustain head injuries. The ultimate goal is to enable older patients not just to survive a mild TBI, but to regain their pre-injury level of function and quality of life as fully as possible, through vigilant and personalized clinical care [1,13,25,26,27].
Future directions: our findings highlight the need for more focused research on geriatric mild TBI. Future studies could explore interventions targeted at the identified risk factors—for example, a trial of a structured balance training program for older mTBI patients with CT lesions to see if it improves outcomes, or an investigation of whether cognitive rehabilitation can particularly help those with lower education. Additionally, studying longer-term outcomes (one to two years post-injury) in older patients would be valuable to see whether mild TBI accelerates functional decline or cognitive aging. There is also interest in whether repetitive mild TBIs or a mild TBI in older age contributes to neurodegenerative processes (such as an increased risk of dementia); our dataset cannot address that issue, but larger longitudinal cohorts could [28].
In summary, although the majority of older mild TBI patients regain independence, a notable subset experiences lingering deficits. Early identification of high-risk cases—based on the predictors we identified—offers an opportunity to intervene and improve outcomes. Mild TBI in older people should not be considered benign: proactive, individualized care is needed to preserve brain health and functional independence in this growing population.
Limitations
While our study provides valuable insights, it is important to consider its limitations. The sample is limited to patients from a single institution, which may limit the generalizability of the findings to other settings or populations. The size of the older adult subgroup (93 patients) offers moderate statistical power, but smaller effects may have gone undetected. Additionally, follow-up was restricted to the six-month post-injury mark; we did not capture longer-term outcomes or late-emerging issues, which could be relevant for an older population. We also relied largely on patient-reported outcomes and relatively brief clinical measures (such as SF-12 and questionnaires) rather than in-depth neuropsychological testing, which could miss subtle cognitive deficits. Finally, treatment during the follow-up period (such as how many patients received rehabilitation therapy, counseling, etc.) was not standardized or rigorously tracked in our study, which could influence outcomes.
Despite these limitations, the study’s strengths include a well-characterized prospective cohort with a comprehensive outcome assessment across multiple domains, and a focus on an underserved research area (geriatric mild TBI). The consistency of several findings with theoretical expectations (e.g., cognitive reserve, importance of acute symptoms) lends credibility to the results.
5. Conclusions
Mild traumatic brain injury in older adults is not trivial; it can leave lasting functional and quality-of-life deficits. In this cohort, worse outcomes were linked to greater acute injury severity (notably, severe headache), intracranial lesions on CT, and lower physiological/cognitive reserve (advanced age, lower education). Conversely, strong social support and timely care (e.g., anticoagulation reversal when indicated) were associated with better recovery.
Clinically, we recommend adopting a proactive, tailored approach, maintaining a high index of suspicion in seniors with red flags (significant symptoms or positive CT), ensuring early referral to rehabilitation (physical, occupational, vestibular), and addressing the psychosocial context through caregiver engagement, education, and linkage to community resources. At the systems level, integrated geriatric TBI pathways should be established, with routine cognitive/depression screening, scheduled follow-ups, and a multidisciplinary team.
Bottom line: most older adults recover substantially, but a meaningful subset does not. Early identification of high-risk patients using these predictors enables interventions that protect brain health and preserve independence.
Author Contributions
Conceptualization, J.G. and I.H.; methodology, J.G. and I.H.; software, J.G. and I.H.; validation, D.D. and B.J.; formal analysis, B.J.; investigation, D.D.; resources, J.G. and I.H.; data curation, J.G. and I.H.; writing—original draft preparation, J.G. and I.H.; writing—review and editing, P.V.; visualization, J.G.; supervision, P.V.; project administration, I.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of University Clinical Centre of Vojvodina (01-39/216/1, approved on 12 July 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| mTBI | Mild traumatic brain injury |
| CT | Computed tomography |
| GCS | Glasgow Coma Scale |
| GOSE | Glasgow Outcome Scale–Extended |
| SF-12 | 12-Item Short Form Health Survey |
| RPQ | Rivermead Post-Concussion Symptoms Questionnaire |
| PCL-5 | PTSD Checklist for DSM-5 |
| PTSD | Post-traumatic stress disorder |
| DSM-5 | Diagnostic and Statistical Manual for Mental Disorders |
| PHQ-9 | Patient Health Questionnaire-9 |
| TUG | Timed Up and Go test |
References
- Corriero, A.; Fornaciari, A.; Terrazzino, S.; Zangari, R.; Izzi, A.; Peluso, L.; Savi, M.; Faso, C.; Cavallini, L.; Polato, M.; et al. The impact of age and intensity of treatment on the outcome of traumatic brain injury. Front. Neurol. 2024, 15, 1471209. [Google Scholar] [CrossRef]
- Mao, A.; Su, J.; Ren, M.; Chen, S.; Zhang, H. Risk prediction models for falls in hospitalized older patients: A systematic review and meta-analysis. BMC Geriatr. 2025, 25, 29. [Google Scholar] [CrossRef] [PubMed]
- Gürü, S.; Özensoy, H.S.; Ertürk, N.; Örün, S.; Ceyhan, M.A. Analyses of the characteristics and prognosis of elderly patients visiting a high-capacity Turkish emergency department due to an occupational accident: A cross-sectional study. BMC Geriatr. 2025, 25, 610. [Google Scholar] [CrossRef] [PubMed]
- Von Steinbüechel, N.; Hahm, S.; Muehlan, H.; Arango-Lasprilla, J.C.; Bockhop, F.; Čović, A.; Schmidt, S.; Steyerberg, E.W.; Maas, A.I.R.; Menon, D.; et al. Impact of Sociodemographic, Premorbid, and Injury-Related Factors on Patient-Reported Outcome Trajectories after Traumatic Brain Injury (TBI). J. Clin. Med. 2023, 12, 2246. [Google Scholar] [CrossRef] [PubMed]
- Perumpalath, N.; Jineesh, T.; Rajendran, V.R.; Devarajan, E.; Rajan, P.; Subramnian, G.; Juvaina, P.; Pillai, S.S. Traumatic Intra Cranial Injury—Computed Tomography, per Operative and Post Mortem Find Ings: A Prognostic Correlation. J. Evol. Med. Dent. Sci. 2015, 4, 11043–11058. [Google Scholar] [CrossRef]
- Jha, D.K.; Chauhan, R.N. Diagnosis and Management of Computed Tomography in Head Injury. Int. J. Med. Biomed. Stud. 2019, 3, 284–289. [Google Scholar] [CrossRef]
- Lo, T.W.; Chan, G.H. Understanding the life experiences of elderly in social isolation from the social systems perspective: Using Hong Kong as an illustrating example. Front. Psychiatry 2023, 14, 1114135. [Google Scholar] [CrossRef]
- Söderman, M.; Bondesson, A.; Pettersson, T.; Gustafsson, L. “Intensive-Home-Rehabilitation” Intervention for Older Persons: A Follow-Up Study of Team Members’ Perceptions. J. Multidiscip. Health 2023, 16, 2207–2216. [Google Scholar] [CrossRef]
- Erwander, K.; Agvall, B.; Ivarsson, K. The role of vital signs in predicting mortality risk in elderly patients visiting the emergency department. BMC Emerg. Med. 2025, 25, 144. [Google Scholar] [CrossRef]
- Kim, D.Y.; Kim, M.H.; Pyun, S.B. Comparison of Functional Outcomes Between Elderly and Young. 2024. Available online: https://journals.lww.com/topicsingeriatricrehabilitation/abstract/2019/04000/comparison_of_functional_outcomes_between_elderly.10.aspx (accessed on 22 August 2025).
- Marešová, P.; Krejcar, O.; Maskuriy, R.; Bakar, N.A.A.; Selamat, A.; Truhlářová, Z.; Horak, J.; Joukl, M.; Vítkova, L. Challenges and opportunity in mobility among older adults—Key determinant identification. BMC Geriatr. 2023, 23, 447. [Google Scholar] [CrossRef]
- Cossio-Bolaños, M.; Vidal-Espinoza, R.; Villar-Cifuentes, I.; de Campos, L.F.C.C.; de Lázari, M.S.R.; Urra-Albornoz, C.; Sulla-Torres, J.; Gomez-Campos, R. Functional fitness benchmark values for older adults: A systematic review. Front. Public Health 2024, 12, 1335311. [Google Scholar] [CrossRef]
- Barrett, C.A.; Goetting, M.G.; Lyerla, R.; Fogarty, K.J. Subsequent Emergency Department Visits in Geriatric Mild Traumatic Brain Injury: Relationship with Fall, Payor, and Discharge Outcome. Healthcare 2025, 13, 1236. [Google Scholar] [CrossRef]
- Kwon, H.; Kim, Y.; Lee, J.; Kim, S.; Kim, Y.; Kim, W.Y. Incidence and outcomes of delayed intracranial hemorrhage: A population-based cohort study. Sci. Rep. 2024, 14, 19502. [Google Scholar] [CrossRef]
- Sergeyenko, Y.; Andreae, M.E.; Segal, M. Diagnosis and Management of Mild Traumatic Brain Injury (mTBI): A Comprehensive, Patient-centered Approach. Curr. Pain Headache Rep. 2025, 29, 19. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, S.; Corderman, S.; Berlinberg, E.J.; Schoenthaler, A.; Horwitz, L.I. Assessment of Patient Education Delivered at Time of Hospital Discharge. JAMA Intern. Med. 2023, 183, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Austad, K.; Lee, J.H.; Lanney, H.; Rapoport, V.O.; Wornhoff, R.; McDaniel, K.L.; Li-Garrison, L.; Jack, B.W. Evaluating the quality and equity of patient hospital discharge instructions. BMC Health Serv. Res. 2025, 25, 291. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Mandado, O.; Periáñez, J.A. An effective psychological intervention in reducing internalized stigma and improving recovery outcomes in people with severe mental illness. Psychiatry Res. 2020, 295, 113635. [Google Scholar] [CrossRef]
- Salas, C.E.; Rojas-Líbano, D.; de Castro, O.A.; Cruces, R.; Evans, J.J.; Radovic, D.; Arévalo-Romero, C.; Torres, J.; Aliaga, Á. Social isolation after acquired brain injury: Exploring the relationship between network size, functional support, loneliness and mental health. Neuropsychol. Rehabil. 2021, 32, 2294–2318. [Google Scholar] [CrossRef]
- Fisher, K.; Seidler, Z.E.; King, K.; Oliffe, J.L.; Rice, S. Men’s anxiety: A systematic review. J. Affect. Disord. 2021, 295, 688–702. [Google Scholar] [CrossRef]
- Herreen, D.; Rice, S.; Zajac, I. Brief assessment of male depression in clinical care: Validation of the Male Depression Risk Scale short form in a cross-sectional study of Australian men. BMJ Open 2022, 12, e053650. [Google Scholar] [CrossRef]
- Palmer, R.M.; Smith, B.J.; Kite, J.; Phongsavan, P. The socio-ecological determinants of help-seeking practices and healthcare access among young men: A systematic review. Health Promot. Int. 2024, 39, daae024. [Google Scholar] [CrossRef]
- Wågberg, S.; Stålnacke, B.-M.; Magnusson, B.M. Gender and Age Differences in Outcomes after Mild Traumatic Brain Injury. J. Clin. Med. 2023, 12, 4883. [Google Scholar] [CrossRef]
- Mitchell, A.; Elmasry, Y.E.T.; Poelgeest, E.P.; van Welsh, T. Anticoagulant use in older persons at risk for falls: Therapeutic dilemmas—A clinical review. Eur. Geriatr. Med. 2023, 14, 683–696. [Google Scholar] [CrossRef]
- Lim, J.Y.; Jee, Y.; Choi, S.G.; Torbati, S.; Berdahl, C.T.; Lee, S.H. Redefining Trauma Triage for Elderly Adults: Development of Age-Specific Guidelines for Improved Patient Outcomes Based on a Machine-Learning Algorithm. Medicina 2025, 61, 784. [Google Scholar] [CrossRef] [PubMed]
- Thompson, H.J.; McCormick, W.C.; Kagan, S.H. Traumatic Brain Injury in Older Adults: Epidemiology, Outcomes, and Future Implications. J. Am. Geriatr. Soc. 2006, 54, 1590–1595. [Google Scholar] [CrossRef]
- Tyler, C.M.; Dini, M.E.; Perrin, P.B. Group-Based Patterns of Life Satisfaction and Functional Independence over the 10 Years after Traumatic Brain Injury in Older Adults: A Model Systems Study. Int. J. Environ. Res. Public Health 2023, 20, 5643. [Google Scholar] [CrossRef]
- Coffeng, S.M.; Abdulle, A.E.; van der Horn, H.J.; de Koning, M.E.; ter Maaten, J.C.; Spikman, J.M.; van der Naalt, J. Good Health-Related Quality of Life in Older Patients One Year after mTBI despite Incomplete Recovery: An Indication of the Disability Paradox? J. Clin. Med. 2024, 13, 2655. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Swiss Federation of Clinical Neuro-Societies. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).