
Artificial Intelligence-Empowered Embryo Selection for IVF Applications: A Methodological Review

 ,
,  , , ,
, , ,  , , ,
, , ,  and
and 
Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
1.1. In Vitro Fertilization
1.2. Artificial Intelligence in ART
1.3. Motivation and Contributions
- The different DL architectures are briefly outlined first.
- Several tasks are reviewed that cover IVF applications which can be addressed using AI techniques.
- An emphasis is given to more recent works, from 2021 onward.
- Emphasis is also given to DL techniques, as they constitute the state of the art in AI and ML methodologies.
- Future research directions and challenges are discussed.
2. Review Methodology
- The work should be published in a peer-reviewed scientific journal, presented at an international conference and included in its proceedings, or published as a book chapter in a collected volume. So, the works have already been submitted to a peer-review process.
- The publications are in English.
- Publications should have a digital object identifier (DOI).
- The works should be listed on an indexing service like Google Scholar, Scopus, or Web of Science.
3. Overview of AI Methodologies
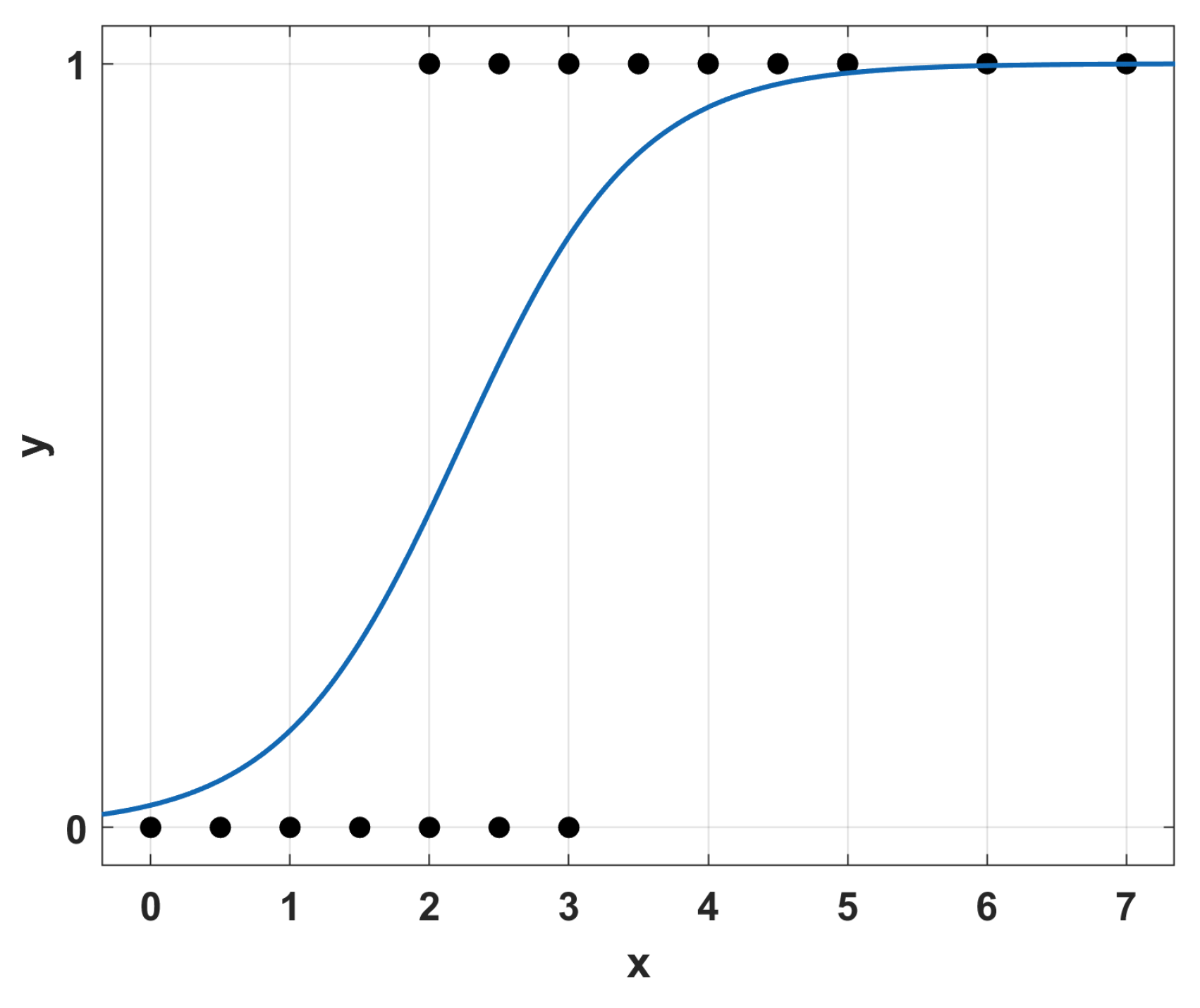
3.1. Regression Learning
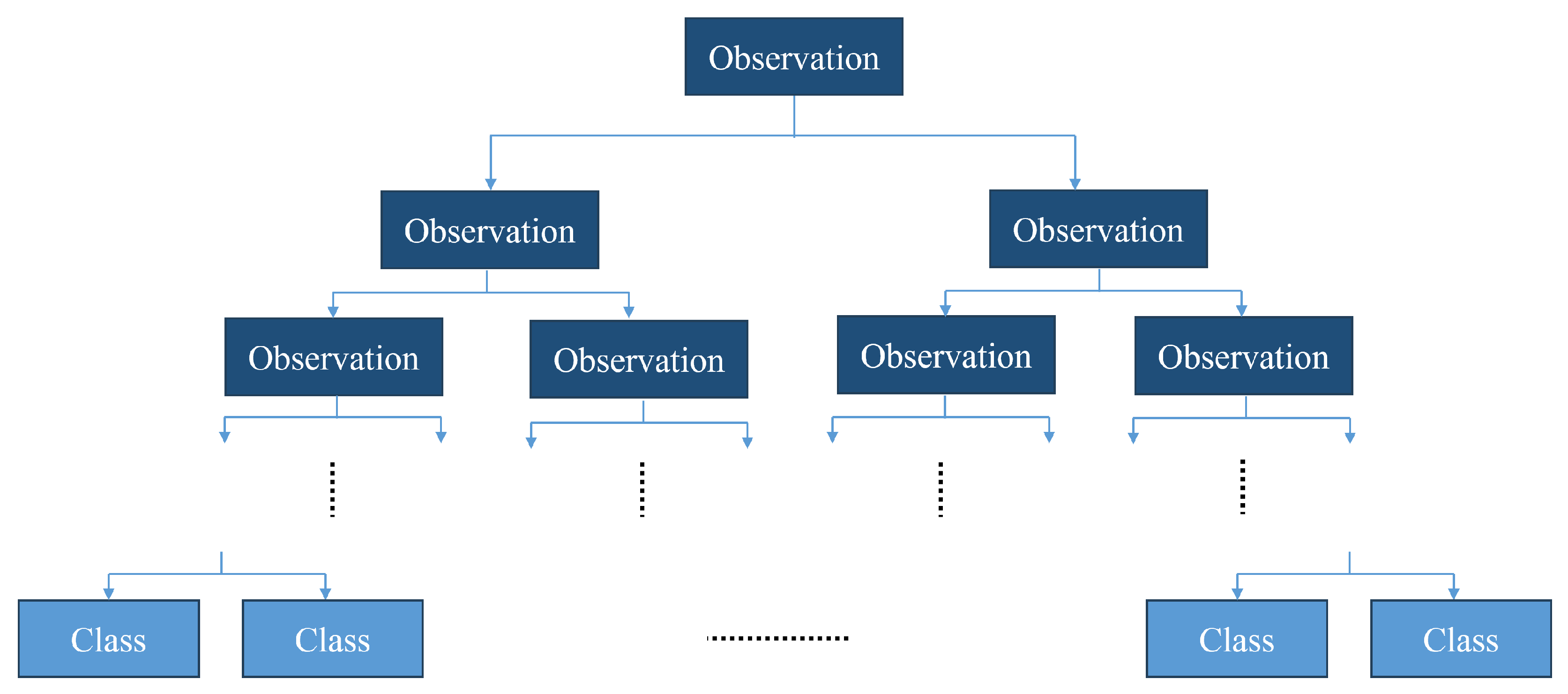
3.2. Decision Tree Learning
3.3. Artificial Neural Networks
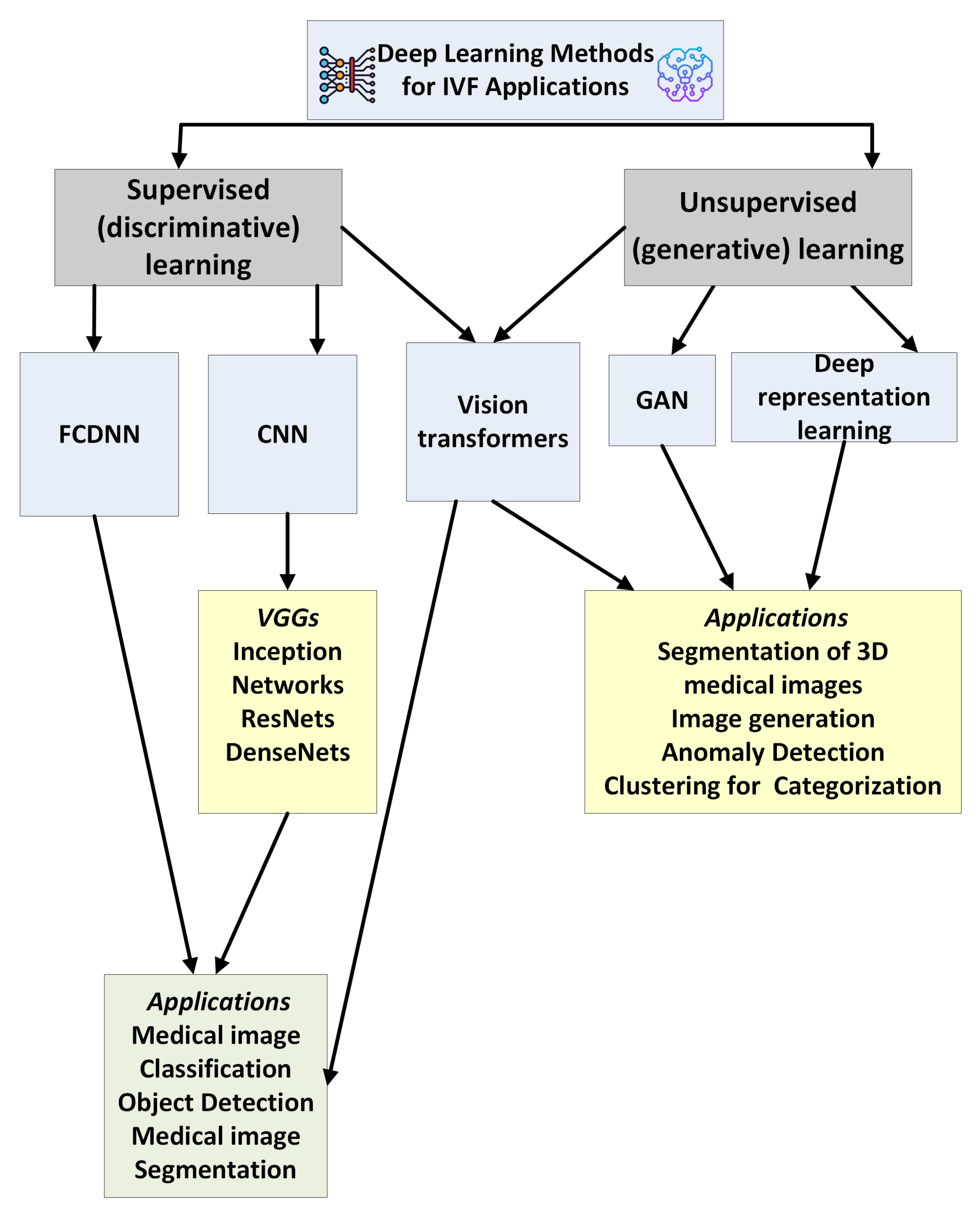
3.4. Deep Learning Methods
3.4.1. Fully Connected Deep Neural Networks
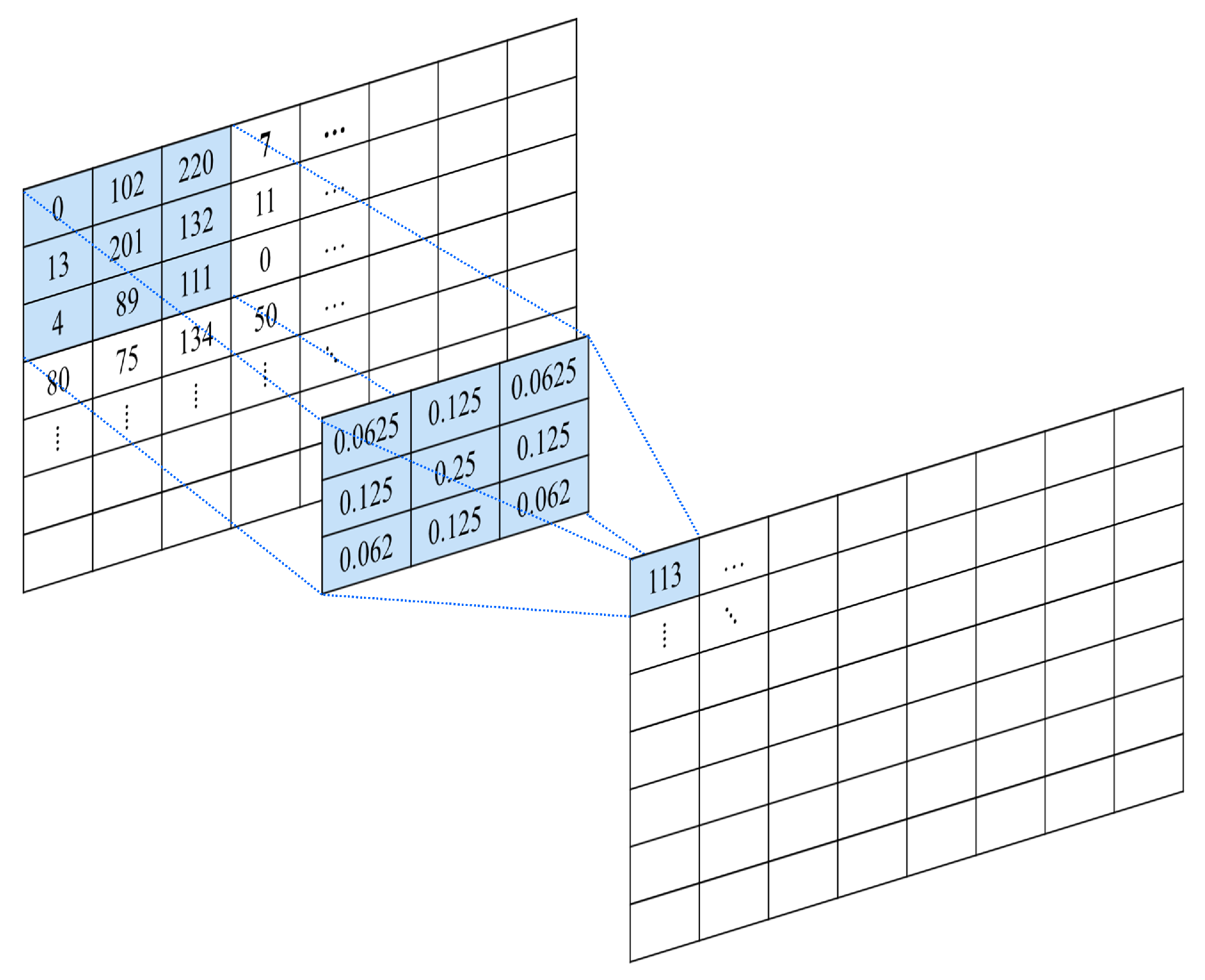
3.4.2. Convolutional Neural Networks
- Input layer: The first layer of the network accepts the input data and, if required, transforms them in a format suitable for further processing. For example, RGB image data can be rearranged into multi-dimensional arrays.
- Convolution layers: The convolution layers are the distinct blocks of the CNN. They are used for feature extraction. In contrast to a fully connected layer, where each neuron receives input from all neurons in the previous layer, the neurons in the convolutional layer have a smaller receptive field. The receptive field indicates that every neuron receives input from only a restricted subset of the previous layer.
- Activation function: Most CNNs in the literature consider either a Rectified Linear Unit (ReLU) function or a variant of it. ReLU is defined as [17]:A variant of ReLU that has been successfully considered in many CV problems is Leaky ReLU, defined as:The parameter is usually taken as 0.01.
- Pooling layers: They are used to reduce the size of the incoming data by summarizing small groups of features using a computationally efficient method. For example, a max pooling layer will extract the maximum element from a feature region, like an image subregion, effectively reducing the feature data for the next processing step.
- Flattening: This operation reshapes the data into a 1D vector.
- Output layer: This is the end layer, which provides the model’s prediction.
- Visual Geometry Group models (VGGs) have a network ranging from 11 to 19 layers. They were initially proposed in order to demonstrate that deeper networks can outperform networks with fewer layers. Using a smaller size of convolutional kernels (), they can have fewer parameters and increased accuracy [18].
- The problem of overfitting can be avoided by Inception Networks that use modules consisting of multiple filters of varying sizes on the same level, effectively making the network ‘wider’. Here, the problem of the vanishing gradient is mitigated by alternating between fully connected layers and average pooling instead and also by adding auxiliary classifiers to the intermediate layers. Several improvements have been developed, like InceptionV2, InceptionV3, and InceptionV4 [19].
- Xception is an architecture built on the InceptionV3 model. Specifically, it replaces the inception modules with depth-wise separable convolutions, that is, a 2D convolution that is independent for each channel, followed by a 1D point-wise convolution. This architecture outperforms InceptionV3 in several image recognition tasks. Its parameter set is also reduced, leading to a decrease in learning latency [20].
- Residual Networks (ResNets) resolve the problem of degradation that can appear in several deep CNN architectures. Their implementation allows deeper networks to be trained and perform better. This is possible through the residual learning technique. Here, instead of using parameter layers to learn the relation between inputs and outputs, similar to VGG, they are used to extract the residual between inputs and outputs [21].
- Densely Connected Convolutional Networks (DenseNets) are inspired by ResNets. They establish maximum flow of information between layers by connecting all of them directly with each other with matching feature-map sizes. Therefore, DenseNet resolves the vanishing-gradient problem and underlines feature propagation and reuse. They also have a reduced set of parameters [22].
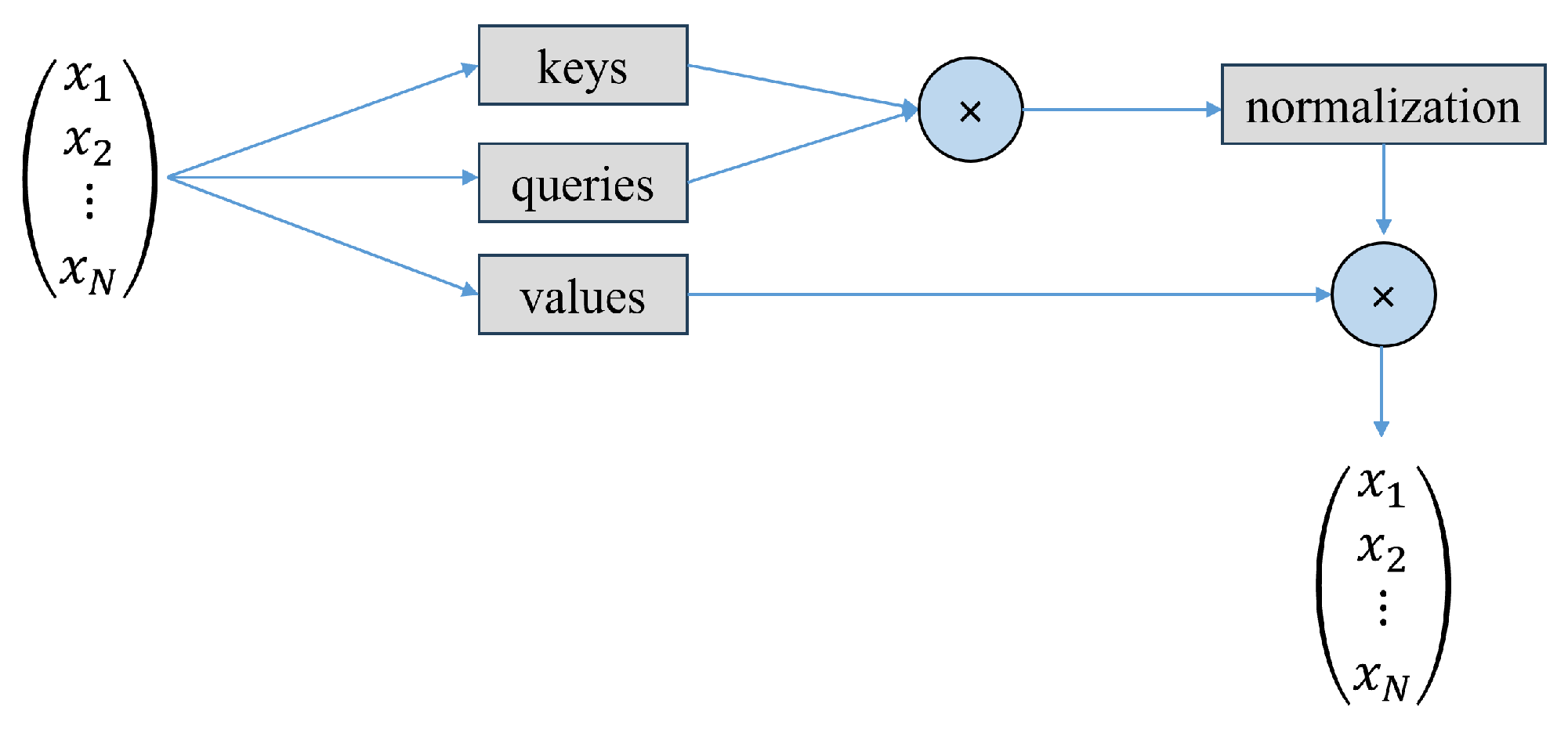
3.4.3. Attention-Based Models
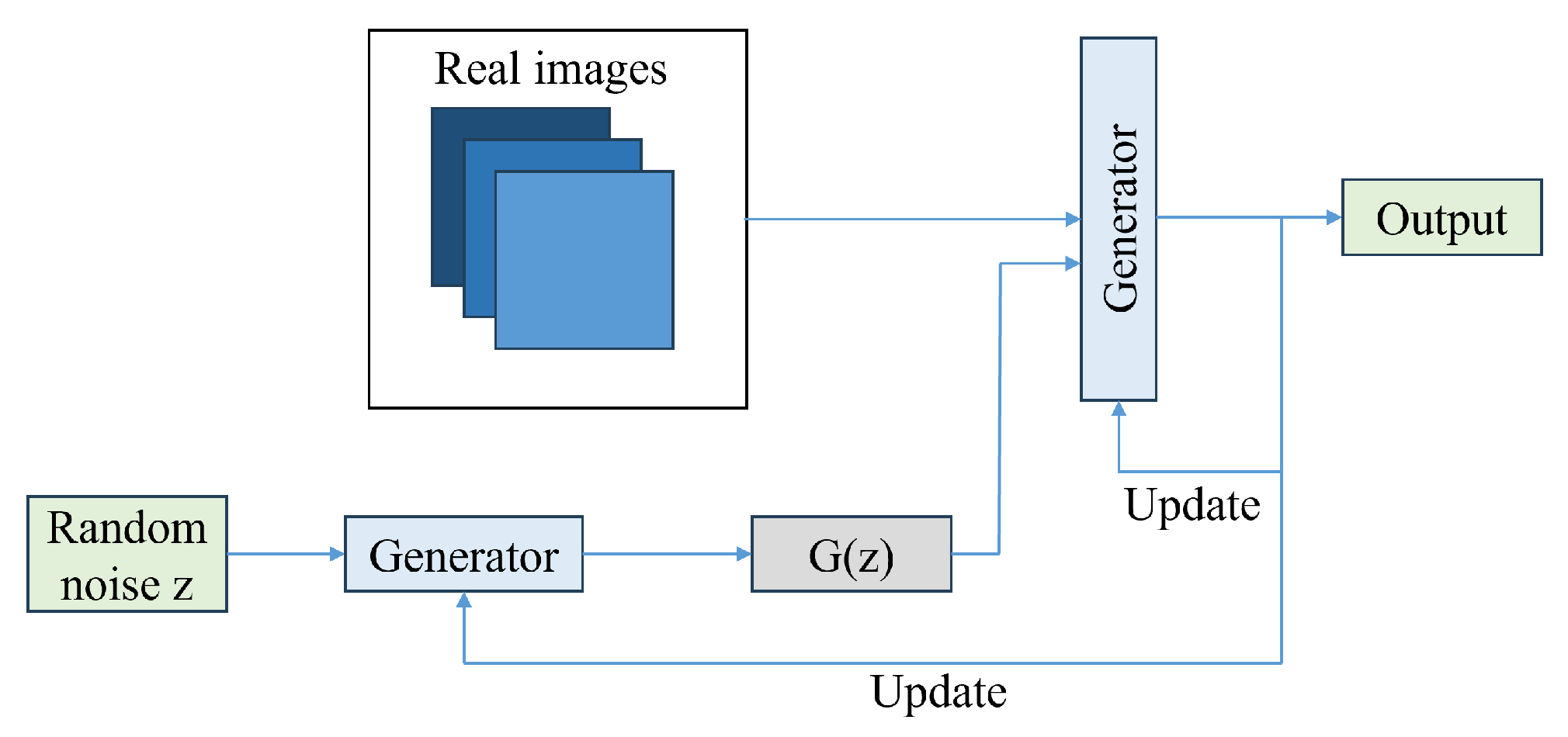
3.4.4. Generative Adversarial Networks
4. DL-Empowered Embryo Selection for IVF Application
- Strategy Selection: DL is used as a support tool in medical decision-making.
- Embryo Development Annotation: In this case, the researchers develop an automated annotation tool for human embryo development in time-lapse devices based on image analysis.
- Intracytoplasmic Sperm Injection: In this case, DL is being implemented in intracytoplasmic sperm injection (ICSI) procedures to improve the selection, analysis, and ultimately success rates of fertilization. This includes the creation of models that can be used to identify high-quality sperm, evaluate DNA fragmentation, and even monitor sperm movement during the procedure.
- Component Segmentation: Semantic segmentation of images in combination with an object detection technique can support the further processing of embryos for tasks like grading or outcome prediction.
- Embryo Grading: It involves a classification task in which embryo images are classified according to a specific grading system that evaluates the quality and developmental potential of embryos.
- Ovarian Stimulation: Ovarian stimulation is a critical stage in IVF technologies, requiring the formulation of numerous decisions regarding drug protocols, dosing, and timing that can be customized to the individual profile of each patient. DL has the potential to help fertility physicians recommend personalized treatment plans, optimize the number of retrieved oocytes, and improve patient outcomes by analyzing extensive datasets from previous IVF cycles.
- Predicting Retrieved Oocytes: It involves ML methods to predict the number of retrieved oocytes.
- Pregnancy and Live Birth Prediction: ML has been extensively employed to evaluate the prospective maternal risks during pregnancy and predict the mode of childbirth
- Intrauterine Insemination (IUI): In this case, ML methods are applied for predicting clinical pregnancy outcomes from intrauterine insemination (IUI) and identifying significant factors affecting pregnancy.
- Sperm Analysis: ML has the potential to improve intracytoplasmic sperm injection by assisting clinicians in the objective selection of sperm. This is a classfication task.
- Quality Assurance: DL is applied as an assistive quality assurance tool to identify perturbations in the embryo culture environment that may affect clinical outcomes.


4.1. Reviews on the Topic of AI in IVF
4.2. Strategy Selection
4.3. Embryo Development Annotation
4.4. Intracytoplasmic Sperm Injection
4.5. Component Segmentation
4.6. Embryo Grading
4.7. Ovarian Stimulation
4.8. Predicting Retrieval of Oocytes
4.9. Pregnancy and Live-Birth Prediction
4.10. Intrauterine Insemination (IUI)
4.11. Sperm Analysis
4.12. Quality Assurance
5. Open Challenges
5.1. Selecting the Best Architecture
5.2. Data Availability
5.3. Data Limitations
5.4. Transfer Learning
5.5. Model Interpretability
5.6. AI and Responsibility
5.7. The Role of Embryologists
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| nD (1D,…) | n-dimensional (one-dimensional etc.) |
| AFC | Antral Follicle Count |
| AI | Artificial Intelligence |
| ART | Assisted Reproductive Technology |
| BC | Blastocoel |
| BG | Background |
| CNN | Convolutional Neural Network |
| CV | Computer Vision |
| DL | Deep Learning |
| ET | Embryo Transfer |
| FCDNN | Fully Connected Deep Neural Network |
| FSH | Follicle-Stimulating Hormone |
| GAN | Generative Adversarial Network |
| GLOM | Grey Level Co-Occurrence Matrix |
| hpi | Hours Post Insemination |
| ICM | Inner Cell Mass |
| ICSI | Intra-Cytoplasmic Sperm Injection |
| IVF | In Vitro Fertilization |
| LSTM | Long Short-Term Memory |
| MII | Metaphase II |
| ML | Machine Learning |
| NLP | Natural Language Processing |
| NN | Neural Network |
| PGT | Preimplantation Genetic Testing |
| ResNet | Residual Network |
| RGB | Red–Green–Blue |
| SVM | Support Vector Machine |
| TE | Trophectoderm |
| TLI | Time-Lapse Imaging |
| ViT | Vision Transformer |
| VGG | Visual Geometry Group |
| ZP | Zona Pellucida |
References
- CDC. What is Assisted Reproductive Technology? Available online: https://www.cdc.gov/art/about/ (accessed on 31 January 2024).
- Bormann, C.L. ART: Laboratory Aspects. In Clinical Reproductive Medicine and Surgery: A Practical Guide; Springer: Berlin/Heidelberg, Germany, 2022; pp. 393–408. [Google Scholar]
- CDC. ART Success Rates. Available online: https://www.cdc.gov/art/success-rates/?CDC_AAref_Val=https://www.cdc.gov/art/artdata/index.html (accessed on 31 January 2024).
- CDCC. 2020 National ART Summary. Available online: https://www.cdc.gov/art/php/national-summary/ (accessed on 31 January 2024).
- Miyagi, Y.; Miyake, T. Potential of artificial intelligence for estimating Japanese fetal weights. Acta Medica Okayama 2020, 74, 483–493. [Google Scholar] [PubMed]
- Looney, P.; Stevenson, G.N.; Nicolaides, K.H.; Plasencia, W.; Molloholli, M.; Natsis, S.; Collins, S.L. Fully automated, real-time 3D ultrasound segmentation to estimate first trimester placental volume using deep learning. JCI Insight 2018, 3, e120178. [Google Scholar] [CrossRef] [PubMed]
- Petrozziello, A.; Jordanov, I.; Papageorghiou, T.A.; Redman, W.C.; Georgieva, A. Deep learning for continuous electronic fetal monitoring in labor. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; IEEE: New York, NY, USA, 2018; pp. 5866–5869. [Google Scholar]
- Yazdani, A.; Costa, S.; Kroon, B. Artificial intelligence: Friend or foe? Aust. New Zealand J. Obstet. Gynaecol. 2023, 63, 127–130. [Google Scholar] [CrossRef]
- Curchoe, C.L. For whom the artificial intelligence bell tolls: Preimplantation genetic testing for aneuploidy, does it toll for thee? Fertil. Steril. 2022, 117, 536–538. [Google Scholar] [CrossRef]
- Gardner, D.K.; Sakkas, D. Making and selecting the best embryo in the laboratory. Fertil. Steril. 2023, 120, 457–466. [Google Scholar] [CrossRef]
- Charnpinyo, N.; Suthicharoenpanich, K.; Onthuam, K.; Engphaiboon, S.; Chaichaowarat, R.; Suebthawinkul, C.; Siricharoen, P. Embryo Selection for IVF using Machine Learning Techniques Based on Light Microscopic Images of Embryo and Additional Factors. In Proceedings of the 2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Sydney, Australia, 24–27 July 2023; IEEE: New York, NY, USA, 2023; pp. 1–4. [Google Scholar]
- Basile, N.; Carbajosa, A.R.; Meseguer, M. Evaluation of embryo quality: Time-lapse imaging to assess embryo morphokinesis. In Textbook of Assisted Reproductive Techniques; CRC Press: Boca Raton, FL, USA, 2017; pp. 285–298. [Google Scholar]
- Fadon, P.; Gallegos, E.; Jalota, S.; Muriel, L.; Diaz-Garcia, C. Time-lapse systems: A comprehensive analysis on effectiveness. In Proceedings of the Seminars in Reproductive Medicine; Thieme Medical Publishers, Inc.: New York, NY, USA, 2021; Volume 39, pp. e12–e18. [Google Scholar]
- Yu, C.; Liu, J.; Nemati, S.; Yin, G. Reinforcement Learning in Healthcare: A Survey. ACM Comput. Surv. 2021, 55, 1–36. [Google Scholar] [CrossRef]
- Prayitno; Shyu, C.R.; Putra, K.T.; Chen, H.C.; Tsai, Y.Y.; Hossain, K.S.M.T.; Jiang, W.; Shae, Z.Y. A Systematic Review of Federated Learning in the Healthcare Area: From the Perspective of Data Properties and Applications. Appl. Sci. 2021, 11, 11191. [Google Scholar] [CrossRef]
- Krishnan, R.; Rajpurkar, P.; Topol, E. Self-supervised learning in medicine and healthcare. Nat. Biomed. Eng. 2022, 6, 1346–1352. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; Adaptive Computation and Machine Learning; MIT Press: Cambridge, MA, USA, 2016; p. 800. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. In Proceedings of the 3rd International Conference on Learning Representations, ICLR 2015, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A.A. Inception-v4, Inception-ResNet and the Impact of Residual Connections on Learning. In Proceedings of the Thirty-First AAAI Conference on Artificial Intelligence, AAAI’17, San Francisco, CA, USA, 4–9 February 2017; AAAI Press: San Francisco, CA, USA, 2017; pp. 4278–4284. [Google Scholar]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 2261–2269. [Google Scholar] [CrossRef]
- Vaswani, A.; Shazeer, N.; Parmar, N.; Uszkoreit, J.; Jones, L.; Gomez, A.N.; Lu, K.; Polosukhin, I. Attention is All you Need. In Proceedings of the Advances in Neural Information Processing Systems; Guyon, I., Luxburg, U.V., Bengio, S., Wallach, H., Fergus, R., Vishwanathan, S., Garnett, R., Eds.; Curran Associates, Inc.: Red Hook, NY, USA, 2017; Volume 30. [Google Scholar]
- Wolf, T.; Debut, L.; Sanh, V.; Chaumond, J.; Delangue, C.; Moi, A.; Cistac, P.; Rault, T.; Louf, R.; Funtowicz, M.; et al. Transformers: State-of-the-art natural language processing. In Proceedings of the 2020 Conference on Empirical Methods in Natural Language Processing: System Demonstrations, Online, 16–20 November 2020; pp. 38–45. [Google Scholar]
- Dosovitskiy, A.; Beyer, L.; Kolesnikov, A.; Weissenborn, D.; Zhai, X.; Unterthiner, T.; Dehghani, M.; Minderer, M.; Heigold, G.; Gelly, S.; et al. An Image is Worth 16 × 16 Words: Transformers for Image Recognition at Scale. In Proceedings of the International Conference on Learning Representations, Vienna, Austria, 4 May 2021. [Google Scholar]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. In Proceedings of the Advances in Neural Information Processing Systems, Montreal, QC, Canada, 8–13 December 2014; pp. 2672–2680. [Google Scholar]
- Moriya, T.; Roth, H.R.; Nakamura, S.; Oda, H.; Nagara, K.; Oda, M.; Mori, K. Unsupervised segmentation of 3D medical images based on clustering and deep representation learning. In Proceedings of the Medical Imaging, Houston, TX, USA, 11–13 February 2018. [Google Scholar]
- Hengstschläger, M. Artificial intelligence as a door opener for a new era of human reproduction. Hum. Reprod. Open 2023, 2023, hoad043. [Google Scholar] [CrossRef]
- Miloski, B. Opportunities for artificial intelligence in healthcare and in vitro fertilization. Fertil. Steril. 2023, 120, 3–7. [Google Scholar] [CrossRef]
- Gardner, D.K. The way to improve ART outcomes is to introduce more technologies in the laboratory. Reprod. Biomed. Online 2022, 44, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, K.A.L.; Atazhanova, T.; Chavez-Badiola, A.; Shivhare, S.B. Automation in ART: Paving the way for the future of infertility treatment. Reprod. Sci. 2023, 30, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Louis, C.M.; Erwin, A.; Handayani, N.; Polim, A.A.; Boediono, A.; Sini, I. Review of computer vision application in in vitro fertilization: The application of deep learning-based computer vision technology in the world of IVF. J. Assist. Reprod. Genet. 2021, 38, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Zaninovic, N.; Rosenwaks, Z. Artificial intelligence in human in vitro fertilization and embryology. Fertil. Steril. 2020, 114, 914–920. [Google Scholar] [CrossRef]
- Jiang, V.S. Artificial Intelligence in the IVF Laboratory: A Review of Advancements Over the Last Decade. Fertil. Steril. 2023, 120, S0015–S0282. [Google Scholar] [CrossRef]
- Letterie, G. Artificial Intelligence and assisted reproductive technologies: 2023. Ready for prime time? Or not. Fertil. Steril. 2023, 120, 32–37. [Google Scholar] [CrossRef]
- Luong, T.M.T.; Le, N.Q.K. Artificial intelligence in time-lapse system: Advances, applications, and future perspectives in reproductive medicine. J. Assist. Reprod. Genet. 2024, 41, 239–252. [Google Scholar] [CrossRef]
- Narmadha, K.; Varalakshmi, P. Federated Learning in Healthcare: A Privacy Preserving Approach. In Proceedings of the MIE, Nice, France, 27–30 May 2022; pp. 194–198. [Google Scholar]
- Hariton, E.; Pavlovic, Z.; Fanton, M.; Jiang, V.S. Applications of artificial intelligence in ovarian stimulation: A tool for improving efficiency and outcomes. Fertil. Steril. 2023, 120, 8–16. [Google Scholar] [CrossRef]
- Salih, M.; Austin, C.; Warty, R.; Tiktin, C.; Rolnik, D.; Momeni, M.; Rezatofighi, H.; Reddy, S.; Smith, V.; Vollenhoven, B.; et al. Embryo selection through artificial intelligence versus embryologists: A systematic review. Hum. Reprod. Open 2023, 2023, hoad031. [Google Scholar] [CrossRef]
- Wang, J.; Guo, Y.; Zhang, N.; Li, T. Research progress of time-lapse imaging technology and embryonic development potential: A review. Medicine 2023, 102, e35203. [Google Scholar] [CrossRef]
- Kim, J.; Lee, J.; Jun, J.H. Non-invasive evaluation of embryo quality for the selection of transferable embryos in human in vitro fertilization-embryo transfer. Clin. Exp. Reprod. Med. 2022, 49, 225. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.; Anteby, R.; Efros, O.; Klang, E.; Soffer, S. Deep Learning for Embryo Evaluation Using Time-Lapse: A Systematic Review of Diagnostic Test Accuracy. Am. J. Obstet. Gynecol. 2023, 229, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Isa, I.S.; Yusof, U.K.; Mohd Zain, M. Image Processing Approach for Grading IVF Blastocyst: A State-of-the-Art Review and Future Perspective of Deep Learning-Based Models. Appl. Sci. 2023, 13, 1195. [Google Scholar] [CrossRef]
- Jiang, V.S.; Bormann, C.L. Non-invasive genetic screening: Current advances in artificial intelligence for embryo ploidy prediction. Fertil. Steril. 2023, 120, 228–234. [Google Scholar] [CrossRef]
- Shobha, R.B.; Bharathi, S.; Pareek, P.K. Deep Learning Methods to Automate Embryo Classification and Evaluation. In Proceedings of the International Conference on Applied Machine Learning and Data Analytics, Reynosa, Mexico, 22–23 December 2022; Springer: Berlin/Heidelberg, Germany, 2022; pp. 1–12. [Google Scholar]
- Glatstein, I.; Chavez-Badiola, A.; Curchoe, C.L. New frontiers in embryo selection. J. Assist. Reprod. Genet. 2023, 40, 223–234. [Google Scholar] [CrossRef]
- Cimadomo, D.; Fernandez, L.S.; Soscia, D.; Fabozzi, G.; Benini, F.; Cesana, A.; Dal Canto, M.B.; Maggiulli, R.; Muzzì, S.; Scarica, C.; et al. Inter-centre reliability in embryo grading across several IVF clinics is limited: Implications for embryo selection. Reprod. BioMed. Online 2022, 44, 39–48. [Google Scholar] [CrossRef]
- Giménez-Rodríguez, C.; Meseguer, M. The patient or the blastocyst; which leads to the perfect outcome prediction? Fertil. Steril. 2023, 120, 811–812. [Google Scholar] [CrossRef]
- Sfakianoudis, K.; Maziotis, E.; Grigoriadis, S.; Pantou, A.; Kokkini, G.; Trypidi, A.; Giannelou, P.; Zikopoulos, A.; Angeli, I.; Vaxevanoglou, T.; et al. Reporting on the value of artificial intelligence in predicting the optimal embryo for transfer: A systematic review including data synthesis. Biomedicines 2022, 10, 697. [Google Scholar] [CrossRef]
- Dimitriadis, I.; Zaninovic, N.; Badiola, A.C.; Bormann, C.L. Artificial intelligence in the embryology laboratory: A review. Reprod. BioMed. Online 2022, 44, 435–448. [Google Scholar] [CrossRef]
- Brayboy, L.M.; Quaas, A.M. The DIY IVF cycle—harnessing the power of deeptech to bring ART to the masses. J. Assist. Reprod. Genet. 2023, 40, 259–263. [Google Scholar] [CrossRef]
- Cherouveim, P.; Velmahos, C.; Bormann, C.L. Artificial Intelligence (AI) for Sperm Selection–a Systematic Review. Fertil. Steril. 2023, 120, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Voliotis, M.; Hanassab, S.; Abbara, A.; Heinis, T.; Dhillo, W.S.; Tsaneva-Atanasova, K. Quantitative approaches in clinical reproductive endocrinology. Curr. Opin. Endocr. Metab. Res. 2022, 27, 100421. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Zhan, H.; Zhang, X.; Pang, Y.; Xu, H.; Zhang, B.; Lao, K.; Ding, P.; Wang, Y.; Han, L. Predictive models for starting dose of gonadotropin in controlled ovarian hyperstimulation: Review and progress update. Hum. Fertil. 2023, 26, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Wang, Z.; Du, M.; Liu, Z. Artificial intelligence in the assessment of female reproductive function using ultrasound: A review. J. Ultrasound Med. 2022, 41, 1343–1353. [Google Scholar] [CrossRef]
- Rolfes, V.; Bittner, U.; Gerhards, H.; Krüssel, J.S.; Fehm, T.; Ranisch, R.; Fangerau, H. Artificial intelligence in reproductive medicine—An ethical perspective. Geburtshilfe Frauenheilkd. 2023, 83, 106–115. [Google Scholar] [CrossRef]
- Go, K.J.; Hudson, C. Deep technology for the optimization of cryostorage. J. Assist. Reprod. Genet. 2023, 40, 1829–1834. [Google Scholar] [CrossRef]
- Wang, R.; Pan, W.; Yu, L.; Zhang, X.; Pan, W.; Hu, C.; Wen, L.; Jin, L.; Liao, S. AI-Based Optimal Treatment Strategy Selection for Female Infertility for First and Subsequent IVF-ET Cycles. J. Med. Syst. 2023, 47, 87. [Google Scholar] [CrossRef]
- Bauer, E.; Kohavi, R. An empirical comparison of voting classification algorithms: Bagging, boosting, and variants. Mach. Learn. 1999, 36, 105–139. [Google Scholar] [CrossRef]
- Ke, G.; Meng, Q.; Finley, T.; Wang, T.; Chen, W.; Ma, W.; Ye, Q.; Liu, T.Y. Lightgbm: A highly efficient gradient boosting decision tree. Adv. Neural Inf. Process. Syst. 2017, 30, 3149–3157. [Google Scholar]
- Liu, Z.; Huang, B.; Cui, Y.; Xu, Y.; Zhang, B.; Zhu, L.; Wang, Y.; Jin, L.; Wu, D. Multi-task deep learning with dynamic programming for embryo early development stage classification from time-lapse videos. IEEE Access 2019, 7, 122153–122163. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; IEEE: New York, NY, USA; pp. 248–255. [Google Scholar]
- Fjeldstad, J.; Qi, W.; Mercuri, N.; Siddique, N.; Meriano, J.; Krivoi, A.; Nayot, D. An artificial intelligence tool predicts blastocyst development from static images of fresh mature oocytes. Reprod. BioMed. Online 2024, 48, 103842. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, PMLR, Long Beach, CA, USA, 10–15 June 2019; pp. 6105–6114. [Google Scholar]
- Lee, C.I.; Su, Y.R.; Chen, C.H.; Chang, T.A.; Kuo, E.E.S.; Zheng, W.L.; Hsieh, W.T.; Huang, C.C.; Lee, M.S.; Liu, M. End-to-end deep learning for recognition of ploidy status using time-lapse videos. J. Assist. Reprod. Genet. 2021, 38, 1655–1663. [Google Scholar] [CrossRef] [PubMed]
- Carreira, J.; Zisserman, A. Quo vadis, action recognition? Anew model and the kinetics dataset. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 6299–6308. [Google Scholar]
- Kay, W.; Carreira, J.; Simonyan, K.; Zhang, B.; Hillier, C.; Vijayanarasimhan, S.; Viola, F.; Green, T.; Back, T.; Natsev, P.; et al. The kinetics human action video dataset. arXiv 2017, arXiv:1705.06950. [Google Scholar]
- Targosz, A.; Myszor, D.; Mrugacz, G. Human oocytes image classification method based on deep neural networks. BioMed. Eng. Online 2023, 22, 92. [Google Scholar] [CrossRef]
- Chen, L.C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoder-decoder with atrous separable convolution for semantic image segmentation. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 801–818. [Google Scholar]
- Iandola, F.N.; Han, S.; Moskewicz, M.W.; Ashraf, K.; Dally, W.J.; Keutzer, K. SqueezeNet: AlexNet-level accuracy with 50x fewer parameters and <0.5 MB model size. arXiv 2016, arXiv:1602.07360. [Google Scholar]
- Danardono, G.B.; Erwin, A.; Purnama, J.; Handayani, N.; Polim, A.A.; Boediono, A.; Sini, I. A Homogeneous Ensemble of Robust Pre-defined Neural Network Enables Automated Annotation of Human Embryo Morphokinetics. J. Reprod. Infertil. 2022, 23, 250. [Google Scholar] [CrossRef]
- Einy, S.; Sen, E.; Saygin, H.; Hivehchi, H.; Dorostkar Navaei, Y. Local Binary Convolutional Neural Networks’ Long Short-Term Memory Model for Human Embryos’ Anomaly Detection. Sci. Program. 2023, 2023. [Google Scholar] [CrossRef]
- Juefei-Xu, F.; Naresh Boddeti, V.; Savvides, M. Local binary convolutional neural networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 19–28. [Google Scholar]
- Jiang, V.S.; Kartik, D.; Thirumalaraju, P.; Kandula, H.; Kanakasabapathy, M.K.; Souter, I.; Dimitriadis, I.; Bormann, C.L.; Shafiee, H. Advancements in the future of automating micromanipulation techniques in the IVF laboratory using deep convolutional neural networks. J. Assist. Reprod. Genet. 2023, 40, 251–257. [Google Scholar] [CrossRef]
- Aguirre-Espericueta, G.; Mendizabal-Ruiz, G. CNNs for ISCI Stage Recognition on Video Sequences. In Proceedings of the XLV Mexican Conference on Biomedical Engineering; Springer: Berlin/Heidelberg, Germany, 2022; pp. 111–118. [Google Scholar]
- Saeedi, P.; Yee, D.; Au, J.; Havelock, J. Automatic identification of human blastocyst components via texture. IEEE Trans. Biomed. Eng. 2017, 64, 2968–2978. [Google Scholar]
- Rad, R.M.; Saeedi, P.; Au, J.; Havelock, J. Predicting human embryos’ implantation outcome from a single blastocyst image. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; IEEE: New York, NY, USA, 2019; pp. 920–924. [Google Scholar]
- Shi, W.; Caballero, J.; Huszár, F.; Totz, J.; Aitken, A.P.; Bishop, R.; Rueckert, D.; Wang, Z. Real-time single image and video super-resolution using an efficient sub-pixel convolutional neural network. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 1874–1883. [Google Scholar]
- Chen, L.C.; Papandreou, G.; Schroff, F.; Adam, H. Rethinking atrous convolution for semantic image segmentation. arXiv 2017, arXiv:1706.05587. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- Arsalan, M.; Haider, A.; Choi, J.; Park, K.R. Detecting blastocyst components by artificial intelligence for human embryological analysis to improve success rate of in vitro fertilization. J. Pers. Med. 2022, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention–MICCAI 2015: 18th International Conference, Munich, Germany, 5–9 October 2015; Proceedings, Part III 18. Springer: Berlin/Heidelberg, Germany, 2015; pp. 234–241. [Google Scholar]
- Iglovikov, V.; Shvets, A. Ternausnet: U-net with vgg11 encoder pre-trained on imagenet for image segmentation. arXiv 2018, arXiv:1801.05746. [Google Scholar]
- Zhao, H.; Shi, J.; Qi, X.; Wang, X.; Jia, J. Pyramid scene parsing network. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 2881–2890. [Google Scholar]
- Rad, R.M.; Saeedi, P.; Au, J.; Havelock, J. BLAST-NET: Semantic segmentation of human blastocyst components via cascaded atrous pyramid and dense progressive upsampling. In Proceedings of the 2019 IEEE International Conference on Image Processing (ICIP), Taipei, Taiwan, 22–25 September 2019; IEEE: New York, NY, USA, 2019; pp. 1865–1869. [Google Scholar]
- Mushtaq, A.; Mumtaz, M.; Raza, A.; Salem, N.; Yasir, M.N. Artificial Intelligence-Based Detection of Human Embryo Components for Assisted Reproduction by In Vitro Fertilization. Sensors 2022, 22, 7418. [Google Scholar] [CrossRef] [PubMed]
- Ishaq, M.; Raza, S.; Rehar, H.; Abadeen, S.E.Z.U.; Hussain, D.; Naqvi, R.A.; Lee, S.W. Assisting the Human Embryo Viability Assessment by Deep Learning for In Vitro Fertilization. Mathematics 2023, 11, 2023. [Google Scholar] [CrossRef]
- Jamal, A.; Dharmawan, A.P.; Septiandri, A.A.; Iffanolida, P.A.; Riayati, O.; Wiweko, B. Densely U-Net Models for Human Embryo Segmentation. In Proceedings of the 2023 4th International Conference on Artificial Intelligence and Data Sciences (AiDAS), Ipoh, Malaysia, 6–7 September 2023; IEEE: New York, NY, USA, 2023; pp. 17–22. [Google Scholar]
- Septiandri, A.A.; Jamal, A.; Iffanolida, P.A.; Riayati, O.; Wiweko, B. Human blastocyst classification after in vitro fertilization using deep learning. In Proceedings of the 2020 7th International Conference on Advance Informatics: Concepts, Theory and Applications (ICAICTA), Online, 8–9 September 2020; IEEE: New York, NY, USA, 2020; pp. 1–4. [Google Scholar]
- Khder, S.M.; Mohamed, E.A.; Yassine, I.A. A Clustering-Based Fusion System for Blastomere Localization. Biomed. Eng. Appl. Basis Commun. 2022, 34, 2250021. [Google Scholar] [CrossRef]
- Targosz, A.; Przystałka, P.; Wiaderkiewicz, R.; Mrugacz, G. Semantic segmentation of human oocyte images using deep neural networks. BioMed. Eng. OnLine 2021, 20, 40. [Google Scholar] [CrossRef]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. SegNet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef]
- Bori, L.; Meseguer, F.; Valera, M.A.; Galan, A.; Remohi, J.; Meseguer, M. The higher the score, the better the clinical outcome: Retrospective evaluation of automatic embryo grading as a support tool for embryo selection in IVF laboratories. Hum. Reprod. 2022, 37, 1148–1160. [Google Scholar] [CrossRef]
- Pierson, H.E.; Invik, J.; Meriano, J.; Pierson, R.A. A novel system for rapid conversion of Gardner embryo grades to linear scale numeric variables. Reprod. BioMed. Online 2023, 46, 808–818. [Google Scholar] [CrossRef]
- Alkindy, F.K.; Yusof, U.K.; Zain, M.M. An Automated Day 3 Embryo Grading Based On Morphological Characteristics Using CNN with Transfer Learning Techniques. In Proceedings of the 2023 IEEE 13th International Conference on Control System, Computing and Engineering (ICCSCE), Penang, Malaysia, 25–26 August 2023; IEEE: New York, NY, USA, 2023; pp. 214–219. [Google Scholar]
- Mohamed, Y.A.; Yusof, U.K.; Isa, I.S.; Zain, M.M. An Automated Blastocyst Grading System Using Convolutional Neural Network and Transfer Learning. In Proceedings of the 2023 IEEE 13th International Conference on Control System, Computing and Engineering (ICCSCE), Penang, Malaysia, 25–26 August 2023; IEEE: New York, NY, USA, 2023; pp. 202–207. [Google Scholar]
- Garg, K.; Dev, A.; Bansal, P.; Mittal, H. An Efficient Deep Learning Model for Embryo Classification. In Proceedings of the 2024 14th International Conference on Cloud Computing, Data Science & Engineering (Confluence), Noida, India, 18–19 January 2024; IEEE: New York, NY, USA, 2024; pp. 358–363. [Google Scholar]
- Thirumalaraju, P.; Kanakasabapathy, M.K.; Bormann, C.L.; Gupta, R.; Pooniwala, R.; Kandula, H.; Souter, I.; Dimitriadis, I.; Shafiee, H. Evaluation of deep convolutional neural networks in classifying human embryo images based on their morphological quality. Heliyon 2021, 7, e06298. [Google Scholar] [CrossRef]
- Liao, Q.; Zhang, Q.; Feng, X.; Huang, H.; Xu, H.; Tian, B.; Liu, J.; Yu, Q.; Guo, N.; Liu, Q.; et al. Development of deep learning algorithms for predicting blastocyst formation and quality by time-lapse monitoring. Commun. Biol. 2021, 4, 415. [Google Scholar] [CrossRef] [PubMed]
- Hung Vuong Hospital, Ho Chi Minh City. Embryo Quality Classification Dataset. Available online: https://www.kaggle.com/competitions/world-championship-2023-embryo-classification/data (accessed on 21 April 2024).
- Wu, C.; Fu, L.; Tian, Z.; Liu, J.; Song, J.; Guo, W.; Zhao, Y.; Zheng, D.; Jin, Y.; Yi, D.; et al. LWMA-Net: Light-weighted morphology attention learning for human embryo grading. Comput. Biol. Med. 2022, 151, 106242. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Brumar, C.; Maeder-York, P.; Barash, O.; Malmsten, J.; Zaninovic, N.; Sakkas, D.; Miller, K.; Levy, M.; VerMilyea, M.; et al. P-171 Sensitivity analysis of an embryo grading artificial intelligence model to different focal planes. Hum. Reprod. 2022, 37, deac107–deac166. [Google Scholar] [CrossRef]
- Kragh, M.F.; Rimestad, J.; Berntsen, J.; Karstoft, H. Automatic grading of human blastocysts from time-lapse imaging. Comput. Biol. Med. 2019, 115, 103494. [Google Scholar] [CrossRef]
- Chen, T.J.; Zheng, W.L.; Liu, C.H.; Huang, I.; Lai, H.H.; Liu, M. Using deep learning with large dataset of microscope images to develop an automated embryo grading system. Fertil. Reprod. 2019, 1, 51–56. [Google Scholar] [CrossRef]
- SFC. Stork Fertility Center. Available online: https://e-stork.com.tw/ (accessed on 31 January 2024).
- Vaidya, G.; Chandrasekhar, S.; Gajjar, R.; Gajjar, N.; Patel, D.; Banker, M. Time series prediction of viable embryo and automatic grading in IVF using deep learning. Open Biomed. Eng. J. 2021, 15, 190–203. [Google Scholar] [CrossRef]
- Nova IVF Fertility. Available online: www.novaivffertility.com/ivf-centre/ahmedabad/fertility-clinic-ahmedabad (accessed on 1 February 2024).
- Wang, S.; Zhou, C.; Zhang, D.; Chen, L.; Sun, H. A deep learning framework design for automatic blastocyst evaluation with multifocal images. IEEE Access 2021, 9, 18927–18934. [Google Scholar] [CrossRef]
- Buiu, C.; Dănăilă, V.R.; Răduţă, C.N. MobileNetV2 ensemble for cervical precancerous lesions classification. Processes 2020, 8, 595. [Google Scholar] [CrossRef]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Bormann, C.L.; Thirumalaraju, P.; Kanakasabapathy, M.K.; Kandula, H.; Souter, I.; Dimitriadis, I.; Gupta, R.; Pooniwala, R.; Shafiee, H. Consistency and objectivity of automated embryo assessments using deep neural networks. Fertil. Steril. 2020, 113, 781–787. [Google Scholar] [CrossRef]
- Zeman, A.; Maerten, A.S.; Mengels, A.; Sharon, L.F.; Spiessens, C.; de Beeck, H.O. Deep learning for human embryo classification at the cleavage stage (Day 3). In Proceedings of the Pattern Recognition. ICPR International Workshops and Challenges, Virtual, 10–15 January 2021; Proceedings, Part I. Springer: Berlin/Heidelberg, Germany, 2021; pp. 278–292. [Google Scholar]
- Zoph, B.; Vasudevan, V.; Shlens, J.; Le, Q.V. Learning transferable architectures for scalable image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 8697–8710. [Google Scholar]
- Xie, S.; Girshick, R.; Dollár, P.; Tu, Z.; He, K. Aggregated residual transformations for deep neural networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1492–1500. [Google Scholar]
- Bormann, C.L.; Kanakasabapathy, M.K.; Thirumalaraju, P.; Gupta, R.; Pooniwala, R.; Kandula, H.; Hariton, E.; Souter, I.; Dimitriadis, I.; Ramirez, L.B.; et al. Performance of a deep learning based neural network in the selection of human blastocysts for implantation. Elife 2020, 9, e55301. [Google Scholar] [CrossRef]
- Fitz, V.; Kanakasabapathy, M.; Thirumalaraju, P.; Kandula, H.; Ramirez, L.; Boehnlein, L.; Swain, J.; Curchoe, C.; James, K.; Dimitriadis, I.; et al. Should there be an “AI” in TEAM? Embryologists selection of high implantation potential embryos improves with the aid of an artificial intelligence algorithm. J. Assist. Reprod. Genet. 2021, 38, 2663–2670. [Google Scholar] [CrossRef] [PubMed]
- Loewke, K.E.; Cho, J.H.; Maeder-York, P.; Barash, O.O.; Meseguer, M.; Zaninovic, N.; Miller, K.A.; Sakkas, D.; Levy, M.; VerMilyea, M.D. A Generalizable Model for Ranking Blastocyst Stage Embryos Using Deep Learning. Fertil. Steril. 2021, 116, e152. [Google Scholar] [CrossRef]
- Pamungkasari, P.D.; Uchida, K.; Saito, S.; Juwono, F.H.; Hanoum, I.F.; Shirakawa, S. Embryo Grade Prediction for In-Vitro Fertilization. In Deep Learning for Biomedical Applications; CRC Press: Boca Raton, FL, USA, 2021; pp. 21–40. [Google Scholar]
- Huang, G.; Liu, Z.; Pleiss, G.; Van Der Maaten, L.; Weinberger, K.Q. Convolutional networks with dense connectivity. IEEE Trans. Pattern Anal. Mach. Intell. 2019, 44, 8704–8716. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Li, D.; Dai, C.; Shan, G.; Zhang, Z.; Zhuang, S.; Lee, C.W.; Wong, A.; Yue, C.; Huang, Z.; et al. Automated Morphological Grading of Human Blastocysts From Multi-Focus Images. IEEE Trans. Autom. Sci. Eng. 2023, 21, 2584–2592. [Google Scholar] [CrossRef]
- Huang, B.; Tan, W.; Li, Z.; Jin, L. An artificial intelligence model (euploid prediction algorithm) can predict embryo ploidy status based on time-lapse data. Reprod. Biol. Endocrinol. 2021, 19, 1–10. [Google Scholar] [CrossRef]
- Hara, K.; Kataoka, H.; Satoh, Y. Can spatiotemporal 3D CNNs retrace the history of 2D CNNs and ImageNet? In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 6546–6555. [Google Scholar]
- Khosravi, P.; Kazemi, E.; Zhan, Q.; Malmsten, J.E.; Toschi, M.; Zisimopoulos, P.; Sigaras, A.; Lavery, S.; Cooper, L.A.; Hickman, C.; et al. Deep learning enables robust assessment and selection of human blastocysts after in vitro fertilization. npj Digit. Med. 2019, 2, 21. [Google Scholar] [CrossRef]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- Barnes, J.; Brendel, M.; Gao, V.R.; Rajendran, S.; Kim, J.; Li, Q.; Malmsten, J.E.; Sierra, J.T.; Zisimopoulos, P.; Sigaras, A.; et al. A non-invasive artificial intelligence approach for the prediction of human blastocyst ploidy: A retrospective model development and validation study. Lancet Digit. Health 2023, 5, e28–e40. [Google Scholar] [CrossRef]
- Diakiw, S.; Hall, J.; VerMilyea, M.; Amin, J.; Aizpurua, J.; Giardini, L.; Briones, Y.; Lim, A.; Dakka, M.; Nguyen, T.; et al. Development of an artificial intelligence model for predicting the likelihood of human embryo euploidy based on blastocyst images from multiple imaging systems during IVF. Hum. Reprod. 2022, 37, 1746–1759. [Google Scholar] [CrossRef]
- VerMilyea, M.; Hall, J.; Diakiw, S.; Johnston, A.; Nguyen, T.; Perugini, D.; Miller, A.; Picou, A.; Murphy, A.; Perugini, M. Development of an artificial intelligence-based assessment model for prediction of embryo viability using static images captured by optical light microscopy during IVF. Hum. Reprod. 2020, 35, 770–784. [Google Scholar] [CrossRef]
- Dakka, M.; Nguyen, T.; Hall, J.; Diakiw, S.; VerMilyea, M.; Linke, R.; Perugini, M.; Perugini, D. Automated detection of poor-quality data: Case studies in healthcare. Sci. Rep. 2021, 11, 18005. [Google Scholar] [CrossRef]
- Hinton, G.; Vinyals, O.; Dean, J. Distilling the knowledge in a neural network. arXiv 2015, arXiv:1503.02531. [Google Scholar]
- Ortiz, J.A.; Morales, R.; Lledo, B.; Vicente, J.A.; Gonzalez, J.; García-Hernandez, E.M.; Cascales, A.; Ten, J.; Bernabeu, A.; Bernabeu, R. Application of machine learning to predict aneuploidy and mosaicism in embryos from in vitro fertilization cycles. AJOG Glob. Rep. 2022, 2, 100103. [Google Scholar] [CrossRef] [PubMed]
- Ou, Z.; Zhang, Q.; Li, Y.; Meng, X.; Wang, Y.; Ouyang, Y.; Li, Z.; Zeng, K. Classification of human embryos by using deep learning. In Proceedings of the International Conference on Cloud Computing, Performance Computing, and Deep Learning (CCPCDL 2023), Huzhou, China, 17–19 February 2023; SPIE: Bellingham, DC, USA, 2023; Volume 12712, pp. 342–347. [Google Scholar]
- Xie, Q.; Luong, M.T.; Hovy, E.; Le, Q.V. Self-training with noisy student improves imagenet classification. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 13–19 June 2020; pp. 10687–10698. [Google Scholar]
- Liu, Z.; Lin, Y.; Cao, Y.; Hu, H.; Wei, Y.; Zhang, Z.; Lin, S.; Guo, B. Swin transformer: Hierarchical vision transformer using shifted windows. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Montreal, QC, Canada, 10–17 October 2021; pp. 10012–10022. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 25, 84–90. [Google Scholar] [CrossRef]
- Marsh, P.; Radif, D.; Rajpurkar, P.; Wang, Z.; Hariton, E.; Ribeiro, S.; Simbulan, R.; Kaing, A.; Lin, W.; Rajah, A.; et al. A proof of concept for a deep learning system that can aid embryologists in predicting blastocyst survival after thaw. Sci. Rep. 2022, 12, 21119. [Google Scholar] [CrossRef]
- Chavez-Badiola, A.; Flores-Saiffe-Farías, A.; Mendizabal-Ruiz, G.; Drakeley, A.J.; Cohen, J. Embryo Ranking Intelligent Classification Algorithm (ERICA): Artificial intelligence clinical assistant predicting embryo ploidy and implantation. Reprod. BioMed. Online 2020, 41, 585–593. [Google Scholar] [CrossRef]
- Darus, R.; Yusuf, U.K.; Yu, S.J.; Isa, I.S.; Zain, M.M.; Fauzi, N.A. EmbryoSys: An Intelligence-Web-based In Vitro Fertilization (IVF) Embryo Tracking & Grading System. In Proceedings of the 2023 IEEE Industrial Electronics and Applications Conference (IEACon), Penang, Malaysia, 6–7 November 2023; IEEE: New York, NY, USA, 2023; pp. 243–248. [Google Scholar]
- Lockhart, L.; Saeedi, P.; Au, J.; Havelock, J. Multi-Label Classification for Automatic Human Blastocyst Grading with Severely Imbalanced Data. In Proceedings of the 2019 IEEE 21st International Workshop on Multimedia Signal Processing (MMSP), Kuala Lumpur, Malaysia, 27–29 September 2019; IEEE: New York, NY, USA, 2019; pp. 1–6. [Google Scholar]
- Cimadomo, D.; Chiappetta, V.; Innocenti, F.; Saturno, G.; Taggi, M.; Marconetto, A.; Casciani, V.; Albricci, L.; Maggiulli, R.; Coticchio, G.; et al. Towards Automation in IVF: Pre-Clinical Validation of a Deep Learning-Based Embryo Grading System during PGT-A Cycles. J. Clin. Med. 2023, 12, 1806. [Google Scholar] [CrossRef]
- Wu, C.; Yan, W.; Li, H.; Li, J.; Wang, H.; Chang, S.; Yu, T.; Jin, Y.; Ma, C.; Luo, Y.; et al. A classification system of day 3 human embryos using deep learning. Biomed. Signal Process. Control 2021, 70, 102943. [Google Scholar] [CrossRef]
- Liang, S.; Zhang, R.; Liang, D.; Song, T.; Ai, T.; Xia, C.; Xia, L.; Wang, Y. Multimodal 3D DenseNet for IDH genotype prediction in gliomas. Genes 2018, 9, 382. [Google Scholar] [CrossRef]
- Mednikov, Y.; Nehemia, S.; Zheng, B.; Benzaquen, O.; Lederman, D. Transfer representation learning using Inception-V3 for the detection of masses in mammography. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; IEEE: New York, NY, USA, 2018; pp. 2587–2590. [Google Scholar]
- Brito, C.; Machado, A.; Sousa, A.L. Electrocardiogram Beat-Classification Based on a ResNet Network. In Proceedings of the MedInfo, Lyon, France, 25–30 August 2019; pp. 55–59. [Google Scholar]
- Cheng, P.M.; Malhi, H.S. Transfer learning with convolutional neural networks for classification of abdominal ultrasound images. J. Digit. Imaging 2017, 30, 234–243. [Google Scholar] [CrossRef]
- Veeck, L.L. An Atlas of Human Gametes and Conceptuses: An Illustrated Reference for Assisted Reproductive Technology; CRC Press: Boca Raton, FL, USA, 1999. [Google Scholar]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.C. Mobilenetv2: Inverted residuals and linear bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar]
- Howard, J.; Gugger, S. Fastai: A layered API for deep learning. Information 2020, 11, 108. [Google Scholar] [CrossRef]
- Kanakasabapathy, M.K.; Thirumalaraju, P.; Bormann, C.L.; Kandula, H.; Dimitriadis, I.; Souter, I.; Yogesh, V.; Pavan, S.K.S.; Yarravarapu, D.; Gupta, R.; et al. Development and evaluation of inexpensive automated deep learning-based imaging systems for embryology. Lab A Chip 2019, 19, 4139–4145. [Google Scholar] [CrossRef] [PubMed]
- Bormann, C.L.; Curchoe, C.L.; Thirumalaraju, P.; Kanakasabapathy, M.K.; Gupta, R.; Pooniwala, R.; Kandula, H.; Souter, I.; Dimitriadis, I.; Shafiee, H. Deep learning early warning system for embryo culture conditions and embryologist performance in the ART laboratory. J. Assist. Reprod. Genet. 2021, 38, 1641–1646. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Z.; Yuan, M.; Song, X.; Huang, X.; Yan, W. Development of an artificial intelligence based model for predicting the euploidy of blastocysts in PGT-A treatments. Sci. Rep. 2023, 13, 2322. [Google Scholar] [CrossRef] [PubMed]
- Bamford, T.; Easter, C.; Montgomery, S.; Smith, R.; Dhillon-Smith, R.K.; Barrie, A.; Campbell, A.; Coomarasamy, A. A comparison of 12 machine learning models developed to predict ploidy, using a morphokinetic meta-dataset of 8147 embryos. Hum. Reprod. 2023, 38, 569–581. [Google Scholar] [CrossRef]
- Danardono, G.B.; Handayani, N.; Louis, C.M.; Polim, A.A.; Sirait, B.; Periastiningrum, G.; Afadlal, S.; Boediono, A.; Sini, I. Embryo ploidy status classification through computer-assisted morphology assessment. AJOG Glob. Rep. 2023, 3, 100209. [Google Scholar] [CrossRef]
- Houri, O.; Gil, Y.; Danieli-Gruber, S.; Shufaro, Y.; Sapir, O.; Hochberg, A.; Ben-Haroush, A.; Wertheimer, A. Prediction of oocyte maturation rate in the GnRH antagonist flexible IVF protocol using a novel machine learning algorithm–A retrospective study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2023, 284, 100–104. [Google Scholar] [CrossRef]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd ACM Sigkdd International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Vergos, G.; Iliadis, L.A.; Kritopoulou, P.; Papatheodorou, A.; Boursianis, A.D.; Kokkinidis, K.I.D.; Papadopoulou, M.S.; Goudos, S.K. Ensemble Learning Technique for Artificial Intelligence Assisted IVF Applications. In Proceedings of the 2023 12th International Conference on Modern Circuits and Systems Technologies (MOCAST), Athens, Greece, 28–30 June 2023; IEEE: New York, NY, USA, 2023; pp. 1–4. [Google Scholar]
- Toporcerová, S.; Špaková, I.; Šoltys, K.; Klepcová, Z.; Kl’oc, M.; Bohošová, J.; Trachtová, K.; Peterová, L.; Mičková, H.; Urdzík, P.; et al. Small Non-Coding RNAs as New Biomarkers to Evaluate the Quality of the Embryo in the IVF Process. Biomolecules 2022, 12, 1687. [Google Scholar] [CrossRef]
- Hammer, K.C.; Jiang, V.S.; Kanakasabapathy, M.K.; Thirumalaraju, P.; Kandula, H.; Dimitriadis, I.; Souter, I.; Bormann, C.L.; Shafiee, H. Using artificial intelligence to avoid human error in identifying embryos: A retrospective cohort study. J. Assist. Reprod. Genet. 2022, 39, 2343–2348. [Google Scholar] [CrossRef]
- Kanakasabapathy, M.K.; Thirumalaraju, P.; Bormann, C.L.; Gupta, R.; Pooniwala, R.; Kandula, H.; Souter, I.; Dimitriadis, I.; Shafiee, H. Deep learning mediated single time-point image-based prediction of embryo developmental outcome at the cleavage stage. arXiv 2020, arXiv:2006.08346. [Google Scholar]
- Chen, L.; Li, W.; Liu, Y.; Peng, Z.; Cai, L.; Zhang, N.; Xu, J.; Wang, L.; Teng, X.; Yao, Y.; et al. Non-invasive embryo selection strategy for clinical IVF to avoid wastage of potentially competent embryos. Reprod. BioMed. Online 2022, 45, 26–34. [Google Scholar] [CrossRef]
- Ibrahim, H.A.; Thamilvanan, M.N.; Zaian, A.; Supriyanto, E. Fertility Assessment Model For Embryo Grading Using Convolutional Neural Network (CNN). In Proceedings of the 2022 International Conference on Healthcare Engineering (ICHE), Johor, Malaysia, 23–25 September 2022; IEEE: New York, NY, USA, 2022; pp. 1–4. [Google Scholar]
- Yang, H.Y.; Leahy, B.D.; Jang, W.D.; Wei, D.; Kalma, Y.; Rahav, R.; Carmon, A.; Kopel, R.; Azem, F.; Venturas, M.; et al. BlastAssist: A deep learning pipeline to measure interpretable features of human embryos. Hum. Reprod. 2024, 39, 698–708. [Google Scholar] [CrossRef] [PubMed]
- Jang, W.D.; Wei, D.; Zhang, X.; Leahy, B.; Yang, H.; Tompkin, J.; Ben-Yosef, D.; Needleman, D.; Pfister, H. Learning vector quantized shape code for amodal blastomere instance segmentation. In Proceedings of the 2023 IEEE 20th International Symposium on Biomedical Imaging (ISBI), Cartagena, Colombia, 18–21 April 2023; IEEE: New York, NY, USA, 2023; pp. 1–5. [Google Scholar]
- Leahy, B.D.; Jang, W.D.; Yang, H.Y.; Struyven, R.; Wei, D.; Sun, Z.; Lee, K.R.; Royston, C.; Cam, L.; Kalma, Y.; et al. Automated measurements of key morphological features of human embryos for IVF. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2020: 23rd International Conference, Lima, Peru, 4–8 October 2020; Proceedings, Part V 23. Springer: Berlin/Heidelberg, Germany, 2020; pp. 25–35. [Google Scholar]
- Lukyanenko, S.; Jang, W.D.; Wei, D.; Struyven, R.; Kim, Y.; Leahy, B.; Yang, H.; Rush, A.; Ben-Yosef, D.; Needleman, D.; et al. Developmental stage classification of embryos using two-stream neural network with linear-chain conditional random field. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2021: 24th International Conference, Strasbourg, France, 27 September–1 October 2021; Proceedings, Part VIII 24. Springer: Berlin/Heidelberg, Germany, 2021; pp. 363–372. [Google Scholar]
- Celard, P.; Seara Vieira, A.; Sorribes-Fdez, J.M.; Iglesias, E.L.; Borrajo, L. Improving Generation and Evaluation of Long Image Sequences for Embryo Development Prediction. Electronics 2024, 13, 476. [Google Scholar] [CrossRef]
- Gomez, T.; Feyeux, M.; Boulant, J.; Normand, N.; David, L.; Paul-Gilloteaux, P.; Fréour, T.; Mouchère, H. A time-lapse embryo dataset for morphokinetic parameter prediction. Data Brief 2022, 42, 108258. [Google Scholar] [CrossRef] [PubMed]
- Letterie, G.; Mac Donald, A. Artificial intelligence in in vitro fertilization: A computer decision support system for day-to-day management of ovarian stimulation during in vitro fertilization. Fertil. Steril. 2020, 114, 1026–1031. [Google Scholar] [CrossRef]
- Fanton, M.; Nutting, V.; Rothman, A.; Maeder-York, P.; Hariton, E.; Barash, O.; Weckstein, L.; Sakkas, D.; Copperman, A.B.; Loewke, K. An interpretable machine learning model for individualized gonadotrophin starting dose selection during ovarian stimulation. Reprod. BioMed. Online 2022, 45, 1152–1159. [Google Scholar] [CrossRef]
- Hariton, E.; Chi, E.A.; Chi, G.; Morris, J.R.; Braatz, J.; Rajpurkar, P.; Rosen, M. A machine learning algorithm can optimize the day of trigger to improve in vitro fertilization outcomes. Fertil. Steril. 2021, 116, 1227–1235. [Google Scholar] [CrossRef]
- Fanton, M.; Nutting, V.; Solano, F.; Maeder-York, P.; Hariton, E.; Barash, O.; Weckstein, L.; Sakkas, D.; Copperman, A.B.; Loewke, K. An interpretable machine learning model for predicting the optimal day of trigger during ovarian stimulation. Fertil. Steril. 2022, 118, 101–108. [Google Scholar] [CrossRef]
- Reuvenny, S.; Youngster, M.; Luz, A.; Hourvitz, R.; Maman, E.; Baum, M.; Hourvitz, A. An artificial intelligence-based approach for selecting the optimal day for triggering in antagonist protocol cycles. Reprod. BioMed. Online 2024, 48, 103423. [Google Scholar] [CrossRef]
- Correa, N.; Cerquides, J.; Arcos, J.L.; Vassena, R. Supporting first FSH dosage for ovarian stimulation with machine learning. Reprod. BioMed. Online 2022, 45, 1039–1045. [Google Scholar] [CrossRef]
- Ferrand, T.; Boulant, J.; He, C.; Chambost, J.; Jacques, C.; Pena, C.A.; Hickman, C.; Reignier, A.; Fréour, T. Predicting the number of oocytes retrieved from controlled ovarian hyperstimulation with machine learning. Hum. Reprod. 2023, 38, 1918–1926. [Google Scholar] [CrossRef]
- Galtier, M.N.; Marini, C. Substra: A framework for privacy-preserving, traceable and collaborative machine learning. arXiv 2019, arXiv:1910.11567. [Google Scholar]
- Liang, X.; Liang, J.; Zeng, F.; Lin, Y.; Li, Y.; Cai, K.; Ni, D.; Chen, Z. Evaluation of oocyte maturity using artificial intelligence quantification of follicle volume biomarker by three-dimensional ultrasound. Reprod. BioMed. Online 2022, 45, 1197–1206. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, H.; Wang, Y.; Liang, X.; Chen, C.; Zhou, X.; Zeng, F.; Fang, J.; Frangi, A.; Chen, Z.; et al. Contrastive rendering with semi-supervised learning for ovary and follicle segmentation from 3D ultrasound. Med. Image Anal. 2021, 73, 102134. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Shen, F.; Liang, H.; Yang, Z.; Yang, J.; Chen, J. Machine learning-based modeling of ovarian response and the quantitative evaluation of comprehensive impact features. Diagnostics 2022, 12, 492. [Google Scholar] [CrossRef]
- Fordham, D.E.; Rosentraub, D.; Polsky, A.L.; Aviram, T.; Wolf, Y.; Perl, O.; Devir, A.; Rosentraub, S.; Silver, D.H.; Gold Zamir, Y.; et al. Embryologist agreement when assessing blastocyst implantation probability: Is data-driven prediction the solution to embryo assessment subjectivity? Hum. Reprod. 2022, 37, 2275–2290. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q. Efficientnetv2: Smaller models and faster training. In Proceedings of the International Conference on Machine Learning, PMLR, Online, 18–24 July 2021; pp. 10096–10106. [Google Scholar]
- Alpha Scientists in Reproductive Medicine; ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting. Hum. Reprod. 2011, 26, 1270–1283. [Google Scholar] [CrossRef]
- Dai, Z.; Liu, H.; Le, Q.V.; Tan, M. Coatnet: Marrying convolution and attention for all data sizes. Adv. Neural Inf. Process. Syst. 2021, 34, 3965–3977. [Google Scholar]
- Diakiw, S.M.; Hall, J.M.; VerMilyea, M.; Lim, A.Y.; Quangkananurug, W.; Chanchamroen, S.; Bankowski, B.; Stones, R.; Storr, A.; Miller, A.; et al. An artificial intelligence model correlated with morphological and genetic features of blastocyst quality improves ranking of viable embryos. Reprod. BioMed. Online 2022, 45, 1105–1117. [Google Scholar] [CrossRef]
- Berntsen, J.; Rimestad, J.; Lassen, J.T.; Tran, D.; Kragh, M.F. Robust and generalizable embryo selection based on artificial intelligence and time-lapse image sequences. PLoS ONE 2022, 17, e0262661. [Google Scholar] [CrossRef]
- Vitrolife. KIDScore D5 Decision Support Tool. 2019. Available online: https://www.vitrolife.com/support/support-material/ (accessed on 31 January 2024).
- Ezoe, K.; Shimazaki, K.; Miki, T.; Takahashi, T.; Tanimura, Y.; Amagai, A.; Sawado, A.; Akaike, H.; Mogi, M.; Kaneko, S.; et al. Association between a deep learning-based scoring system with morphokinetics and morphological alterations in human embryos. Reprod. BioMed. Online 2022, 45, 1124–1132. [Google Scholar] [CrossRef]
- Johansen, M.N.; Parner, E.T.; Kragh, M.F.; Kato, K.; Ueno, S.; Palm, S.; Kernbach, M.; Balaban, B.; Keleş, İ.; Gabrielsen, A.V.; et al. Comparing performance between clinics of an embryo evaluation algorithm based on time-lapse images and machine learning. J. Assist. Reprod. Genet. 2023, 40, 2129–2137. [Google Scholar] [CrossRef] [PubMed]
- Ueno, S.; Berntsen, J.; Ito, M.; Okimura, T.; Kato, K. Correlation between an annotation-free embryo scoring system based on deep learning and live birth/neonatal outcomes after single vitrified-warmed blastocyst transfer: A single-centre, large-cohort retrospective study. J. Assist. Reprod. Genet. 2022, 39, 2089–2099. [Google Scholar] [CrossRef] [PubMed]
- Theilgaard Lassen, J.; Fly Kragh, M.; Rimestad, J.; Nygård Johansen, M.; Berntsen, J. Development and validation of deep learning based embryo selection across multiple days of transfer. Sci. Rep. 2023, 13, 4235. [Google Scholar] [CrossRef] [PubMed]
- Petersen, B.M.; Boel, M.; Montag, M.; Gardner, D.K. Development of a generally applicable morphokinetic algorithm capable of predicting the implantation potential of embryos transferred on Day 3. Hum. Reprod. 2016, 31, 2231–2244. [Google Scholar] [CrossRef]
- Li, T.; Liao, R.; Chan, C.; Greenblatt, E.M. Deep learning analysis of endometrial histology as a promising tool to predict the chance of pregnancy after frozen embryo transfers. J. Assist. Reprod. Genet. 2023, 40, 1–10. [Google Scholar] [CrossRef]
- Fu, K.; Li, Y.; Lv, H.; Wu, W.; Song, J.; Xu, J. Development of a Model Predicting the Outcome of In Vitro Fertilization Cycles by a Robust Decision Tree Method. Front. Endocrinol. 2022, 13, 877518. [Google Scholar] [CrossRef]
- Wen, J.Y.; Liu, C.F.; Chung, M.T.; Tsai, Y.C. Artificial intelligence model to predict pregnancy and multiple pregnancy risk following in vitro fertilization-embryo transfer (IVF-ET). Taiwan J. Obstet. Gynecol. 2022, 61, 837–846. [Google Scholar] [CrossRef]
- Goyal, A.; Kuchana, M.; Ayyagari, K.P.R. Machine learning predicts live-birth occurrence before in-vitro fertilization treatment. Sci. Rep. 2020, 10, 20925. [Google Scholar] [CrossRef]
- HFEA. Human Fertilisation & Embryology Authority Dataset. Available online: https://www.hfea.gov.uk/media/2667/ar-2015-2016-xlsb.xlsb (accessed on 31 January 2024).
- Huang, B.; Zheng, S.; Ma, B.; Yang, Y.; Zhang, S.; Jin, L. Using deep learning to predict the outcome of live birth from more than 10,000 embryo data. BMC Pregnancy Childbirth 2022, 22, 36. [Google Scholar] [CrossRef]
- Liu, L.; Jiao, Y.; Li, X.; Ouyang, Y.; Shi, D. Machine learning algorithms to predict early pregnancy loss after in vitro fertilization-embryo transfer with fetal heart rate as a strong predictor. Comput. Methods Programs Biomed. 2020, 196, 105624. [Google Scholar] [CrossRef]
- Loewke, K.; Cho, J.H.; Brumar, C.D.; Maeder-York, P.; Barash, O.; Malmsten, J.E.; Zaninovic, N.; Sakkas, D.; Miller, K.A.; Levy, M.; et al. Characterization of an artificial intelligence model for ranking static images of blastocyst stage embryos. Fertil. Steril. 2022, 117, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Loewke, K.E.; Cho, J.H.; Maeder-York, P.; Barash, O.O.; Meseguer, M.; Malmsten, J.; Miller, K.A.; Sakkas, D.; Levy, M.; VerMilyea, M.D. Identifying Potential Sources of Bias in Deep Learning Models for Embryo Assessment. Fertil. Steril. 2021, 116, e158–e159. [Google Scholar] [CrossRef]
- Abbasi, M.; Saeedi, P.; Au, J.; Havelock, J. A deep learning approach for prediction of IVF implantation outcome from day 3 and day 5 time-lapse human embryo image sequences. In Proceedings of the 2021 IEEE International Conference on Image Processing (ICIP), Anchorage, AL, USA, 19–22 September 2021; IEEE: New York, NY, USA, 2021; pp. 289–293. [Google Scholar]
- Chavez-Badiola, A.; Flores-Saiffe Farias, A.; Mendizabal-Ruiz, G.; Garcia-Sanchez, R.; Drakeley, A.J.; Garcia-Sandoval, J.P. Predicting pregnancy test results after embryo transfer by image feature extraction and analysis using machine learning. Sci. Rep. 2020, 10, 4394. [Google Scholar] [CrossRef] [PubMed]
- Serdarogullari, M.; Raad, G.; Yarkiner, Z.; Bazzi, M.; Mourad, Y.; Alpturk, S.; Fakih, F.; Fakih, C.; Liperis, G. Identifying predictors of Day 5 blastocyst utilization rate using an artificial neural network. Reprod. BioMed. Online 2023, 47, 103399. [Google Scholar] [CrossRef]
- Bamford, T.; Smith, R.; Easter, C.; Dhillon-Smith, R.; Barrie, A.; Montgomery, S.; Campbell, A.; Coomarasamy, A. Association between a morphokinetic ploidy prediction model risk score and miscarriage and live birth: A multicentre cohort study. Fertil. Steril. 2023, 120, 834–843. [Google Scholar] [CrossRef]
- Duval, A.; Nogueira, D.; Dissler, N.; Maskani Filali, M.; Delestro Matos, F.; Chansel-Debordeaux, L.; Ferrer-Buitrago, M.; Ferrer, E.; Antequera, V.; Ruiz-Jorro, M.; et al. A hybrid artificial intelligence model leverages multi-centric clinical data to improve fetal heart rate pregnancy prediction across time-lapse systems. Hum. Reprod. 2023, 38, 596–608. [Google Scholar] [CrossRef]
- Enatsu, N.; Miyatsuka, I.; An, L.M.; Inubushi, M.; Enatsu, K.; Otsuki, J.; Iwasaki, T.; Kokeguchi, S.; Shiotani, M. A novel system based on artificial intelligence for predicting blastocyst viability and visualizing the explanation. Reprod. Med. Biol. 2022, 21, e12443. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, Z.; Gu, Y.; Dai, C.; Shan, G.; Song, H.; Li, D.; Chen, W.; Lin, G.; Sun, Y. Development and evaluation of a live birth prediction model for evaluating human blastocysts from a retrospective study. eLife 2023, 12, e83662. [Google Scholar] [CrossRef]
- Fu, R.; Hu, Q.; Dong, X.; Guo, Y.; Gao, Y.; Li, B. Axiom-based grad-cam: Towards accurate visualization and explanation of cnns. arXiv 2020, arXiv:2008.02312. [Google Scholar]
- Buldo-Licciardi, J.; Large, M.J.; McCulloh, D.H.; McCaffrey, C.; Grifo, J.A. Utilization of standardized preimplantation genetic testing for aneuploidy (PGT-A) via artificial intelligence (AI) technology is correlated with improved pregnancy outcomes in single thawed euploid embryo transfer (STEET) cycles. J. Assist. Reprod. Genet. 2023, 40, 289–299. [Google Scholar] [CrossRef]
- Shen, L.; Zhang, Y.; Chen, W.; Yin, X. The application of artificial intelligence in predicting embryo transfer outcome of recurrent implantation failure. Front. Physiol. 2022, 13, 885661. [Google Scholar] [CrossRef] [PubMed]
- Xi, Q.; Yang, Q.; Wang, M.; Huang, B.; Zhang, B.; Li, Z.; Liu, S.; Yang, L.; Zhu, L.; Jin, L. Individualized embryo selection strategy developed by stacking machine learning model for better in vitro fertilization outcomes: An application study. Reprod. Biol. Endocrinol. 2021, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Peavey, M.; Kaskar, K.; Chappell, N.; Zhu, L.; Devlin, D.; Valdes, C.; Schutt, A.; Woodard, T.; Zarutskie, P.; et al. Development of a dynamic machine learning algorithm to predict clinical pregnancy and live birth rate with embryo morphokinetics. F&S Rep. 2022, 3, 116–123. [Google Scholar]
- Sawada, Y.; Sato, T.; Nagaya, M.; Saito, C.; Yoshihara, H.; Banno, C.; Matsumoto, Y.; Matsuda, Y.; Yoshikai, K.; Sawada, T.; et al. Evaluation of artificial intelligence using time-lapse images of IVF embryos to predict live birth. Reprod. BioMed. Online 2021, 43, 843–852. [Google Scholar] [CrossRef]
- Fukui, H.; Hirakawa, T.; Yamashita, T.; Fujiyoshi, H. Attention branch network: Learning of attention mechanism for visual explanation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 15–20 June 2019; pp. 10705–10714. [Google Scholar]
- Ueno, S.; Berntsen, J.; Ito, M.; Uchiyama, K.; Okimura, T.; Yabuuchi, A.; Kato, K. Pregnancy prediction performance of an annotation-free embryo scoring system on the basis of deep learning after single vitrified-warmed blastocyst transfer: A single-center large cohort retrospective study. Fertil. Steril. 2021, 116, 1172–1180. [Google Scholar] [CrossRef]
- Mehrjerd, A.; Rezaei, H.; Eslami, S.; Ghaebi, N.K. Determination of Cut Off for Endometrial Thickness in Couples with Unexplained Infertility: Trustable AI. In Proceedings of the MIE, Nice, France, 27–30 May 2022; pp. 264–268. [Google Scholar]
- Youngster, M.; Luz, A.; Baum, M.; Hourvitz, R.; Reuvenny, S.; Maman, E.; Hourvitz, A. Artificial intelligence in the service of intrauterine insemination and timed intercourse in spontaneous cycles. Fertil. Steril. 2023, 120, 1004–1012. [Google Scholar] [CrossRef]
- Hariton, E.; Andrusier, M.A.; Khorshid, A. Timing intrauterine inseminations: Do we need an ultrasound, or can artificial intelligence do the trick? Fertil. Steril. 2023, 120, 985–986. [Google Scholar] [CrossRef]
- Kumar, R.S.; Sharma, S.; Halder, A.; Gupta, V. Deep learning-based robust automated system for predicting human sperm DNA fragmentation index. J. Hum. Reprod. Sci. 2023, 16, 16–21. [Google Scholar] [CrossRef]
- Salvaris, M.; Dean, D.; Tok, W.H.; Salvaris, M.; Dean, D.; Tok, W.H. Cognitive services and custom vision. In Deep Learning with Azure: Building and Deploying Artificial Intelligence Solutions on the Microsoft AI Platform; Apress: New York, NY, USA, 2018; pp. 99–128. [Google Scholar]
- Ory, J.; Tradewell, M.B.; Blankstein, U.; Lima, T.F.; Nackeeran, S.; Gonzalez, D.C.; Nwefo, E.; Moryousef, J.; Madhusoodanan, V.; Lau, S.; et al. Artificial intelligence based machine learning models predict sperm parameter upgrading after varicocele repair: A multi-institutional analysis. World J. Men’s Health 2022, 40, 618. [Google Scholar] [CrossRef]
- Naseem, S.; Mahmood, T.; Saba, T.; Alamri, F.S.; Bahaj, S.A.; Ateeq, H.; Farooq, U. DeepFert: An Intelligent Fertility Rate Prediction Approach for Men Based on Deep Learning Neural Networks. IEEE Access 2023, 11, 75006–75022. [Google Scholar] [CrossRef]
- Abou Ghayda, R.; Cannarella, R.; Calogero, A.E.; Shah, R.; Rambhatla, A.; Zohdy, W.; Kavoussi, P.; Avidor-Reiss, T.; Boitrelle, F.; Mostafa, T.; et al. Artificial intelligence in andrology: From semen analysis to image diagnostics. World J. Men’s Health 2024, 42, 39. [Google Scholar] [CrossRef] [PubMed]
- Curchoe, C.L.; Bormann, C.; Hammond, E.; Salter, S.; Timlin, C.; Williams, L.B.; Gilboa, D.; Seidman, D.; Campbell, A.; Morbeck, D. Assuring quality in assisted reproduction laboratories: Assessing the performance of ART Compass—A digital art staff management platform. J. Assist. Reprod. Genet. 2023, 40, 265–278. [Google Scholar] [CrossRef] [PubMed]
- Cherouveim, P.; Jiang, V.S.; Kanakasabapathy, M.K.; Thirumalaraju, P.; Souter, I.; Dimitriadis, I.; Bormann, C.L.; Shafiee, H. Quality assurance (QA) for monitoring the performance of assisted reproductive technology (ART) staff using artificial intelligence (AI). J. Assist. Reprod. Genet. 2023, 40, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Letterie, G.; MacDonald, A.; Shi, Z. An artificial intelligence platform to optimize workflow during ovarian stimulation and IVF: Process improvement and outcome-based predictions. Reprod. BioMed. Online 2022, 44, 254–260. [Google Scholar] [CrossRef]
- Curchoe, C.L.; Tarafdar, O.; Aquilina, M.C.; Seifer, D.B. SART CORS IVF registry: Looking to the past to shape future perspectives. J. Assist. Reprod. Genet. 2022, 39, 2607–2616. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, Y.; Martin, C.; Ma, X.; Shen, B. Translational bioinformatics for human reproductive biology research: Examples, opportunities and challenges for a future reproductive medicine. Int. J. Mol. Sci. 2022, 24, 4. [Google Scholar] [CrossRef]
- Kohli, M.D.; Summers, R.M.; Geis, J.R. Medical Image Data and Datasets in the Era of Machine Learning—Whitepaper from the 2016 C-MIMI Meeting Dataset Session. J. Digit. Imaging 2017, 30, 392–399. [Google Scholar] [CrossRef]
- Muthu, S.; Nabi, F.; Nabi, J. AIM in Obstetrics and Gynecology. In Artificial Intelligence in Medicine; Springer: Berlin/Heidelberg, Germany, 2021; pp. 1–4. [Google Scholar]
- Shafiee, H.; Kanakasabapathy, M.K.; Bormann, C.L.; Topol, E.J. Digitising the human embryo. Lancet 2022, 400, 1577. [Google Scholar] [CrossRef]
- Bhaskar, D.; Chang, T.A.; Wang, S. Current trends in artificial intelligence in reproductive endocrinology. Curr. Opin. Obstet. Gynecol. 2022, 34, 159–163. [Google Scholar] [CrossRef]
- Sadeghi, M.R. Will Artificial Intelligence Change the Future of IVF? J. Reprod. Infertil. 2022, 23, 139. [Google Scholar] [CrossRef]
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, I.J.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.W.; da Silva Santos, L.B.; Bourne, P.E.; et al. The FAIR Guiding Principles for scientific data management and stewardship. Sci. Data 2016, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kromp, F.; Wagner, R.; Balaban, B.; Cottin, V.; Cuevas-Saiz, I.; Schachner, C.; Fancsovits, P.; Fawzy, M.; Fischer, L.; Findikli, N.; et al. An annotated human blastocyst dataset to benchmark deep learning architectures for in vitro fertilization. Sci. Data 2023, 10, 271. [Google Scholar] [CrossRef] [PubMed]
- Touvron, H.; Cord, M.; Douze, M.; Massa, F.; Sablayrolles, A.; Jégou, H. Training data-efficient image transformers & distillation through attention. In Proceedings of the International Conference on Machine Learning, PMLR, Online, 18–24 July 2021; pp. 10347–10357. [Google Scholar]
- Varoquaux, G.; Cheplygina, V. Machine learning for medical imaging: Methodological failures and recommendations for the future. Npj Digit. Med. 2022, 5, 48. [Google Scholar] [CrossRef] [PubMed]
- Price, W.N.; Cohen, I.G. Privacy in the age of medical big data. Nat. Med. 2019, 25, 37–43. [Google Scholar] [CrossRef]
- Gerke, S.; Minssen, T.; Cohen, G. Ethical and legal challenges of artificial intelligence-driven healthcare. In Artificial Intelligence in Healthcare; Elsevier: Amsterdam, The Netherlands, 2020; pp. 295–336. [Google Scholar]
- Mostert, M.; Bredenoord, A.L.; Biesaart, M.C.; Van Delden, J.J. Big Data in medical research and EU data protection law: Challenges to the consent or anonymise approach. Eur. J. Hum. Genet. 2016, 24, 956–960. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef]
- Li, X.; Xiong, H.; Li, X.; Wu, X.; Zhang, X.; Liu, J.; Bian, J.; Dou, D. Interpretable deep learning: Interpretation, interpretability, trustworthiness, and beyond. Knowl. Inf. Syst. 2022, 64, 3197–3234. [Google Scholar] [CrossRef]
- Smith, H.; Fotheringham, K. Artificial intelligence in clinical decision-making: Rethinking liability. Med. Law Int. 2020, 20, 131–154. [Google Scholar] [CrossRef]
- Maliha, G.; Gerke, S.; Cohen, I.G.; Parikh, R.B. Artificial Intelligence and Liability in Medicine. Milbank Q. 2021, 99, 629–647. [Google Scholar] [CrossRef]
- Price, W.N.; Gerke, S.; Cohen, I.G. Potential liability for physicians using artificial intelligence. JAMA 2019, 322, 1765–1766. [Google Scholar] [CrossRef]
- Cestonaro, C.; Delicati, A.; Marcante, B.; Caenazzo, L.; Tozzo, P. Defining medical liability when artificial intelligence is applied on diagnostic algorithms: A systematic review. Front. Med. 2023, 10, 1305756. [Google Scholar] [CrossRef] [PubMed]
- Serdarogullari, M.; Ammar, O.F.; Sharma, K.; Kohlhepp, F.; Montjean, D.; Meseguer, M.; Fraire-Zamora, J.J. #ESHREjc report: Seeing is believing! How time lapse imaging can improve IVF practice and take it to the future clinic. Hum. Reprod. 2022, 37, 1370–1372. [Google Scholar] [PubMed]
- Bori, L.; Meseguer, M. Will the introduction of automated ART laboratory systems render the majority of embryologists redundant? Reprod. BioMedicine Online 2021, 43, 979–981. [Google Scholar] [CrossRef] [PubMed]
- Allahbadia, G.N.; Allahbadia, S.G.; Gupta, A. In Contemporary Reproductive Medicine Human Beings are Not Yet Dispensable. J. Obstet. Gynecol. India 2023, 73, 295–300. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moysis, L.; Iliadis, L.A.; Vergos, G.; Sotiroudis, S.P.; Boursianis, A.D.; Papatheodorou, A.; Kokkinidis, K.-I.D.; Abdul Matin, M.; Sarigiannidis, P.; Siniosoglou, I.; et al. Artificial Intelligence-Empowered Embryo Selection for IVF Applications: A Methodological Review. Mach. Learn. Knowl. Extr. 2025, 7, 56. https://doi.org/10.3390/make7020056
Moysis L, Iliadis LA, Vergos G, Sotiroudis SP, Boursianis AD, Papatheodorou A, Kokkinidis K-ID, Abdul Matin M, Sarigiannidis P, Siniosoglou I, et al. Artificial Intelligence-Empowered Embryo Selection for IVF Applications: A Methodological Review. Machine Learning and Knowledge Extraction. 2025; 7(2):56. https://doi.org/10.3390/make7020056
Chicago/Turabian StyleMoysis, Lazaros, Lazaros Alexios Iliadis, George Vergos, Sotirios P. Sotiroudis, Achilles D. Boursianis, Achilleas Papatheodorou, Konstantinos-Iraklis D. Kokkinidis, Mohammad Abdul Matin, Panagiotis Sarigiannidis, Ilias Siniosoglou, and et al. 2025. "Artificial Intelligence-Empowered Embryo Selection for IVF Applications: A Methodological Review" Machine Learning and Knowledge Extraction 7, no. 2: 56. https://doi.org/10.3390/make7020056
APA StyleMoysis, L., Iliadis, L. A., Vergos, G., Sotiroudis, S. P., Boursianis, A. D., Papatheodorou, A., Kokkinidis, K.-I. D., Abdul Matin, M., Sarigiannidis, P., Siniosoglou, I., Argyriou, V., & Goudos, S. K. (2025). Artificial Intelligence-Empowered Embryo Selection for IVF Applications: A Methodological Review. Machine Learning and Knowledge Extraction, 7(2), 56. https://doi.org/10.3390/make7020056