
A Survey of Deep Learning for Alzheimer’s Disease




Abstract
1. Introduction
1.1. Alzheimer’s Disease and Mild Cognitive Impairment
1.2. Diagnostic Methods and Criteria
1.3. The Deep Learning Approach
1.4. Areas of Interest
- Classification of various stages of AD. This area targets diagnosis or efficient progression monitoring. Current studies mostly focus on AD, MCI subtypes, and normal cognitive controls (NC). A few studies contain the subjective cognitive decline (SCD) stage before MCI.
- Predicting MCI conversion. This area is mainly approached by formulating prediction as a classification problem, which usually involves defining MCI converters and non-converters based on a time threshold from the initial diagnosis. Some studies also aim at the prediction of time-to-conversion for MCI to AD.
- Prediction of clinical measures. This area aims at producing surrogate biomarkers to reduce cost or invasivity, e.g., neuroimaging to replace lumbar puncture. Prediction of clinical measures, e.g., ADAS-Cog13 [75] and ventricular volume [76], is also used for longitudinal studies and attempts to achieve a more comprehensive evaluation of disease progression and model performance benchmarking.
1.5. Challenges in Research
- Numerical representation of the differences between AD stages. Monfared et al. [81] calculated the range of Alzheimer’s disease composite scores to assess the severity of the cognitive decline in patients. Sheng et al. [82] made multiple classifications and concluded that the gap between late mild cognitive impairment and early mild cognitive impairment was small, whereas a greater difference exists between early and late MCI patients. Studies comparing clinical and post-mortem diagnoses have shown 10–20% false cases [83]. In addition, autopsy studies in individuals who were cognitively normal for their age found that ~30% had Alzheimer’s-related brain changes in the form of plaque and tangles [84,85]. Sometimes the signs that distinguish AD, for example, brain shrinkage [86], can be found in a normal healthy brain of older people.
- Difficulty in preprocessing. Preprocessing medical data, especially neuroimaging data, often requires complex pipelines. There is no set standard for preprocessing, while a broad range of processing options and relevant parameters exist. Preprocessing quality is also vastly based on the subjective judgment of clinicians.
- Unavailability of a comprehensive dataset. Though the amount and variety of data available for AD and related diseases are abundant compared with many other conditions, the number of subjects is only moderate compared with large datasets such as Image-Net and is below the optimal requirements for generalization.
- Lack of reproducibility. Most frameworks and models are not publicly available. Without open-source code, implementation details such as specific data cohort selection, preprocessing procedures and parameters, evaluation procedures, and metrics are usually lacking. These are all factors that can significantly impact results. Additionally, few comprehensive frameworks are designed for benchmarking different models based on the same preprocessing/processing and testing standards [89,90].
- Lack of expert knowledge. Researchers adept at using DL often have no medical background, while medical data are significantly more complicated than natural images or language data. Therefore, these researchers lack expert knowledge, especially in preprocessing and identifying brain regions of interest (ROIs).
- Generalizability and interpretability. Current DL models are plagued by information leakage and only provide limited measures of generalizability, the model’s performance in real-world populations. The inherent ‘black box’ nature of neural networks impedes the interpretation of model functions and the subsequent feedback of knowledge for clinicians [91].
- Other practical challenges include the subjectivity of cognitive assessments, the invasiveness of diagnostic techniques such as a lumbar puncture to measure CSF biomarkers and the high cost of neuroimaging such as MRI.
1.6. Survey Protocol
- Recognized journals, including Brain, Neuroimage, Medical Image Analysis, Alzheimer’s and Dementia, Nature Communications, and Radiology.
- Conferences in computer vision and deep learning, including ACM, NeurIPS, CVPR, MICCAI, and ICCV.
- Related to Alzheimer’s disease, MCI, or other related diseases.
- Related to deep learning, with the use of neural networks.
- Contains valid classification/prediction metrics.
- Utilizes a reasonable form of validation.
- Written in English or contains a valid translation.
- Contains a minimum of 180 individual subjects.
2. Data Types and Sources
2.1. Types of Data
2.2. Sources of Data
3. Data Preprocessing
3.1. Structural MRI Data
3.2. PET Data
3.3. Functional MRI Data
4. Data Processing
4.1. Feature-Based
4.2. Slice-Based
4.3. Patch-Based
4.4. ROI-Based
4.5. Voxel-Based
5. Introduction to Deep Learning
6. Unsupervised Learning
6.1. Autoencoder (AE)
6.2. Generative Models
6.3. Restricted Boltzmann Machine (RBM) and Other Unsupervised Methods
7. Supervised and Semi-Supervised Learning
7.1. Convolutional Neural Networks (CNN)
7.1.1. 2D-CNN
7.1.2. 3D-CNN
7.2. Recurrent Neural Networks (RNN)
7.3. Graph and Geometric Neural Networks (GNNs)
7.4. Other Methods
8. Deep Learning Techniques
8.1. Transfer Learning
8.2. Ensemble Learning
8.3. Multi-Modal Fusion
9. Training and Evaluation
9.1. Evaluation Methods
9.1.1. Hold-Out and Cross-Validation
9.1.2. Metrics for Classification
9.1.3. Metrics for Prediction
9.1.4. Other Metrics
9.1.5. Level of Evaluation
9.1.6. Combination of Evaluation Methods
9.1.7. Comparison and Ablation
9.2. Training Protocols
9.2.1. Training and Evaluation Protocols
9.2.2. Information Leakage
9.2.3. Optimization Protocols
9.3. Development Platforms
10. Path to Interpretation of Deep Learning Models
11. Path to Generalization in the Real World
12. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Cortes-Briones, J.A.; Tapia-Rivas, N.I.; D’Souza, D.C.; Estevez, P.A. Going deep into schizophrenia with artificial intelligence. Schizophr. Res. 2022, 245, 122–140. [Google Scholar] [CrossRef]
- Choo, H.; Yoo, S.Y.; Moon, S.; Park, M.; Lee, J.; Sung, K.W.; Cha, W.C.; Shin, S.-Y.; Son, M.H. Deep-learning-based personalized prediction of absolute neutrophil count recovery and comparison with clinicians for validation. J. Biomed. Inform. 2023, 137, 104268. [Google Scholar] [CrossRef] [PubMed]
- Nam, D.; Chapiro, J.; Paradis, V.; Seraphin, T.P.; Kather, J.N. Artificial intelligence in liver diseases: Improving diagnostics, prognostics and response prediction. JHEP Rep. 2022, 4, 100443. [Google Scholar] [CrossRef] [PubMed]
- Tatulian, S.A. Challenges and hopes for Alzheimer’s disease. Drug Discov. Today 2022, 27, 1027–1043. [Google Scholar] [CrossRef] [PubMed]
- Brookmeyer, R.; Johnson, E.; Ziegler-Graham, K.; Arrighi, H.M. Forecasting the global burden of Alzheimer’s disease. Alzheimer’s Dement. 2007, 3, 186–191. [Google Scholar] [CrossRef]
- Loi, S.M.; Pijnenberg, Y.; Velakoulis, D. Recent research advances in young-onset dementia. Curr. Opin. Psychiatry 2023, 36, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Xu, C.; Sun, J.; Shen, H.-M.; Wang, J.; Yang, C. Impairment of the autophagy–lysosomal pathway in Alzheimer’s diseases: Pathogenic mechanisms and therapeutic potential. Acta Pharm. Sin. B 2022, 12, 1019–1040. [Google Scholar] [CrossRef] [PubMed]
- Boeve, B.F.; Boxer, A.L.; Kumfor, F.; Pijnenburg, Y.; Rohrer, J.D. Advances and controversies in frontotemporal dementia: Diagnosis, biomarkers, and therapeutic considerations. Lancet Neurol. 2022, 21, 258–272. [Google Scholar] [CrossRef]
- Sügis, E.; Dauvillier, J.; Leontjeva, A.; Adler, P.; Hindie, V.; Moncion, T.; Collura, V.; Daudin, R.; Loe-Mie, Y.; Herault, Y.; et al. HENA, heterogeneous network-based data set for Alzheimer’s disease. Sci. Data 2019, 6, 151. [Google Scholar] [CrossRef]
- Wimo, A.; Jönsson, L.; Bond, J.; Prince, M.; Winblad, B.; Alzheimer Disease International. The worldwide economic impact of dementia 2010. Alzheimer’s Dement. 2013, 9, 1–11.e3. [Google Scholar] [CrossRef] [PubMed]
- López-Cuenca, I.; Nebreda, A.; García-Colomo, A.; Salobrar-García, E.; de Frutos-Lucas, J.; Bruña, R.; Ramírez, A.I.; Ramirez-Toraño, F.; Salazar, J.J.; Barabash, A.; et al. Early visual alterations in individuals at-risk of Alzheimer’s disease: A multidisciplinary approach. Alzheimer’s Res. Ther. 2023, 15, 19. [Google Scholar] [CrossRef] [PubMed]
- Toschi, N.; Baldacci, F.; Zetterberg, H.; Blennow, K.; Kilimann, I.; Teipel, S.J.; Cavedo, E.; dos Santos, A.M.; Epelbaum, S.; Lamari, F. Alzheimer’s disease biomarker-guided diagnostic workflow using the added value of six combined cerebrospinal fluid candidates: Ab1–42, total-tau, phosphorylated-tau, NFL, neurogranin, and YKL-40. Alzheimer’s Dement. 2017, 1, 10. [Google Scholar]
- Scheltens, P.; Blennow, K.; Breteler, M.M.B.; de Strooper, B.; Frisoni, G.B.; Salloway, S.; Van der Flier, W.M. Alzheimer’s disease. Lancet 2016, 388, 505–517. [Google Scholar] [CrossRef]
- Vogt, A.-C.S.; Jennings, G.T.; Mohsen, M.O.; Vogel, M.; Bachmann, M.F. Alzheimer’s Disease: A Brief History of Immunotherapies Targeting Amyloid β. Int. J. Mol. Sci. 2023, 24, 3895. [Google Scholar] [CrossRef] [PubMed]
- Van der Lee, S.J.; Wolters, F.J.; Ikram, M.K.; Hofman, A.; Ikram, M.A.; Amin, N.; van Duijn, C.M. The effect of APOE and other common genetic variants on the onset of Alzheimer’s disease and dementia: A community-based cohort study. Lancet Neurol. 2018, 17, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Fortea, J.; Vilaplana, E.; Carmona-Iragui, M.; Benejam, B.; Videla, L.; Barroeta, I.; Fernández, S.; Altuna, M.; Pegueroles, J.; Montal, V. Clinical and biomarker changes of Alzheimer’s disease in adults with Down syndrome: A cross-sectional study. Lancet 2020, 395, 1988–1997. [Google Scholar] [CrossRef]
- Brett, B.L.; Gardner, R.C.; Godbout, J.; Dams-O’connor, K.; Keene, C.D. Traumatic Brain Injury and Risk of Neurodegenerative Disorder. Biol. Psychiatry 2021, 91, 498–507. [Google Scholar] [CrossRef]
- Letnes, J.M.; Nes, B.M.; Wisløff, U. Age-related decline in peak oxygen uptake: Cross-sectional vs. longitudinal findings. A review. Int. J. Cardiol. Cardiovasc. Risk Prev. 2023, 16, 200171. [Google Scholar] [CrossRef]
- Tari, A.R.; Nauman, J.; Zisko, N.; Skjellegrind, H.K.; Bosnes, I.; Bergh, S.; Stensvold, D.; Selbæk, G.; Wisløff, U. Temporal changes in cardiorespiratory fitness and risk of dementia incidence and mortality: A population-based prospective cohort study. Lancet Public Health 2019, 4, e565–e574. [Google Scholar] [CrossRef] [PubMed]
- Birkenhäger, W.H.; Forette, F.; Seux, M.-L.; Wang, J.-G.; Staessen, J.A. Blood Pressure, Cognitive Functions, and Prevention of Dementias in Older Patients with Hypertension. Arch. Intern. Med. 2001, 161, 152–156. [Google Scholar] [CrossRef]
- Donaghy, P.C.; Ciafone, J.; Durcan, R.; Hamilton, C.A.; Barker, S.; Lloyd, J.; Firbank, M.; Allan, L.M.; O’Brien, J.T.; Taylor, J.-P.; et al. Mild cognitive impairment with Lewy bodies: Neuropsychiatric supportive symptoms and cognitive profile. Psychol. Med. 2020, 52, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Burns, A.; Iliffe, S. Alzheimer’s disease. BMJ Br. Med. J. (Int. Ed.) 2009, 338, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.; Knopman, D.S. Classification and Epidemiology of MCI. Clin. Geriatr. Med. 2013, 29, 753–772. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S.; et al. Author response: Practice guideline update summary: Mild cognitive impairment: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 2018, 91, 373–374. [Google Scholar] [CrossRef]
- Ward, A.; Tardiff, S.; Dye, C.; Arrighi, H.M. Rate of Conversion from Prodromal Alzheimer’s Disease to Alzheimer’s Dementia: A Systematic Review of the Literature. Dement. Geriatr. Cogn. Disord. Extra 2013, 3, 320–332. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Shiri-Feshki, M. Rate of progression of mild cognitive impairment to dementia—Meta-analysis of 41 robust inception cohort studies. Acta Psychiatr. Scand. 2009, 119, 252–265. [Google Scholar] [CrossRef]
- Sherman, D.S.; Mauser, J.; Nuno, M.; Sherzai, D. The Efficacy of Cognitive Intervention in Mild Cognitive Impairment (MCI): A Meta-Analysis of Outcomes on Neuropsychological Measures. Neuropsychol. Rev. 2017, 27, 440–484. [Google Scholar] [CrossRef] [PubMed]
- Ala, T.; Bakir, D.; Goel, S.; Feller, N.; Botchway, A.; Womack, C. A Mini-Mental State Examination Formula May Help to Distinguish Alzheimer’s Disease from Dementia with Lewy Bodies. J. Alzheimer’s Dis. 2022, 89, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- McGurn, M.; Dworkin, J.D.; Chapman, S.; Huey, E.D.; Cosentino, S.; Louis, E.D. Can the Montreal Cognitive Assessment and Mini-Mental State Examination detect cognitive decline in elderly patients with essential tremor? Clin. Neuropsychol. 2022, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, R.-C.; Yang, Y.-W.; Hsu, K.-C.; Chang, H.-T.; Chiu, P.-Y. Sum of boxes of the clinical dementia rating scale highly predicts conversion or reversion in predementia stages. Front. Aging Neurosci. 2022, 14, 1021792. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.P.; Berg, L.; Danziger, W.L.; Coben, L.A.; Martin, R.L. A New Clinical Scale for the Staging of Dementia. Br. J. Psychiatry 1982, 140, 566–572. [Google Scholar] [CrossRef]
- Titheradge, D.; Isaac, M.; Bremner, S.; Tabet, N. Cambridge Cognitive Examination and Hachinski Ischemic Score as predictors of MRI confirmed pathology in dementia: A cross-sectional study. Int. J. Clin. Pract. 2019, 74, e13446. [Google Scholar] [CrossRef] [PubMed]
- Schmand, B.; Walstra, G.; Lindeboom, J.; Teunisse, S.; Jonker, C. Early detection of Alzheimer’s disease using the Cambridge Cognitive Examination (CAMCOG). Psychol. Med. 2000, 30, 619–627. [Google Scholar] [CrossRef] [PubMed]
- López-Cuenca, I.; Marcos-Dolado, A.; Yus-Fuertes, M.; Salobrar-García, E.; Elvira-Hurtado, L.; Fernández-Albarral, J.A.; Salazar, J.J.; Ramírez, A.I.; Sánchez-Puebla, L.; Fuentes-Ferrer, M.E.; et al. The relationship between retinal layers and brain areas in asymptomatic first-degree relatives of sporadic forms of Alzheimer’s disease: An exploratory analysis. Alzheimer’s Res. Ther. 2022, 14, 79. [Google Scholar] [CrossRef] [PubMed]
- Rocha, A.; Bellaver, B.; Souza, D.G.; Schu, G.; Fontana, I.C.; Venturin, G.T.; Greggio, S.; Fontella, F.U.; Schiavenin, M.L.; Machado, L.S.; et al. Clozapine induces astrocyte-dependent FDG-PET hypometabolism. Eur. J. Nucl. Med. 2022, 49, 2251–2264. [Google Scholar] [CrossRef]
- Oe, K.; Zeng, F.; Niikura, T.; Fukui, T.; Sawauchi, K.; Matsumoto, T.; Nogami, M.; Murakami, T.; Kuroda, R. Influence of Metal Implants on Quantitative Evaluation of Bone Single-Photon Emission Computed Tomography/Computed Tomography. J. Clin. Med. 2022, 11, 6732. [Google Scholar] [CrossRef]
- Madetko-Alster, N.; Alster, P.; Migda, B.; Nieciecki, M.; Koziorowski, D.; Królicki, L. The Use of Cerebellar Hypoperfusion Assessment in the Differential Diagnosis of Multiple System Atrophy with Parkinsonism and Progressive Supranuclear Palsy-Parkinsonism Predominant. Diagnostics 2022, 12, 3022. [Google Scholar] [CrossRef]
- Charpentier, P.; Lavenu, I.; Defebvre, L.; Duhamel, A.; Lecouffe, P.; Pasquier, F.; Steinling, M. Alzheimer’s disease and frontotemporal dementia are differentiated by discriminant analysis applied to 99mTc HmPAO SPECT data. J. Neurol. Neurosurg. Psychiatry 2000, 69, 661–663. [Google Scholar] [CrossRef][Green Version]
- Garriga, M.; Emila, M.; Mir, M.; Eal-Baradie, R.; Ehuertas, S.; Ecastejon, C.; Ecasas, L.; Badenes, D.; Gimenez, N.; Font, M.A.; et al. 123I-FP-CIT SPECT imaging in early diagnosis of dementia in patients with and without a vascular component. Front. Syst. Neurosci. 2015, 9, 99. [Google Scholar] [CrossRef]
- Fortea, J.; Carmona-Iragui, M.; Benejam, B.; Fernández, S.; Videla, L.; Barroeta, I.; Alcolea, D.; Pegueroles, J.; Muñoz, L.; Belbin, O.; et al. Plasma and CSF biomarkers for the diagnosis of Alzheimer’s disease in adults with Down syndrome: A cross-sectional study. Lancet Neurol. 2018, 17, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Olsson, B.; Lautner, R.; Andreasson, U.; Öhrfelt, A.; Portelius, E.; Bjerke, M.; Hölttä, M.; Rosén, C.; Olsson, C.; Strobel, G.; et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: A systematic review and meta-analysis. Lancet Neurol. 2016, 15, 673–684. [Google Scholar] [CrossRef]
- Chen, C.L.; Lu, Q.; Moorakonda, R.B.; Kandiah, N.; Tan, B.Y.; Villaraza, S.G.; Cano, J.; Venketasubramanian, N. Alzheimer’s Disease THErapy with NEuroaid (ATHENE): A Randomized Double-Blind Delayed-Start Trial. J. Am. Med. Dir. Assoc. 2021, 23, 379–386.e3. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Feldman, H.H.; Jacova, C.; DeKosky, S.T.; Barberger-Gateau, P.; Cummings, J.L.; Delacourte, A.; Galasko, D.; Gauthier, S.; Jicha, G.A.; et al. Research Criteria for the Diagnosis of Alzheimer’s Disease: Revising the NINCDS–ADRDA Criteria. Lancet Neurol. 2007, 6, 734–746. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Cummings, J.L.; DeKosky, S.T.; Barberger-Gateau, P.; Delacourte, A.; Frisoni, G.; Fox, N.C.; Galasko, D.; et al. Revising the definition of Alzheimer’s disease: A new lexicon. Lancet Neurol. 2010, 9, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Hampel, H.; Molinuevo, J.L.; Blennow, K.; DeKosky, S.T.; Gauthier, S.; Selkoe, D.; Bateman, R.; et al. Advancing research diagnostic criteria for Alzheimer’s disease: The IWG-2 criteria. Lancet Neurol. 2014, 13, 614–629. [Google Scholar] [CrossRef] [PubMed]
- Jack, C.R., Jr.; Albert, M.; Knopman, D.S.; McKhann, G.M.; Sperling, R.A.; Carillo, M.; Thies, W.; Phelps, C.H. Introduction to revised criteria for the diagnosis of Alzheimer’s disease: National Institute on Aging and the Alzheimer Association Workgroups. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2011, 7, 257. [Google Scholar] [CrossRef]
- Zhou, J.; Benoit, M.; Sharoar, G. Recent advances in pre-clinical diagnosis of Alzheimer’s disease. Metab. Brain Dis. 2021, 37, 1703–1725. [Google Scholar] [CrossRef]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R., Jr.; Kaye, J.; Montine, T.J.; et al. Toward Defining the Preclinical Stages of Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimer’s Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef]
- Chao, L.; Mueller, S.; Buckley, S.; Peek, K.; Raptentsetseng, S.; Elman, J.; Yaffe, K.; Miller, B.; Kramer, J.; Madison, C.; et al. Evidence of neurodegeneration in brains of older adults who do not yet fulfill MCI criteria. Neurobiol. Aging 2010, 31, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.S.; DeKosky, S.T.; Dickson, D.; Dubois, B.; Feldman, H.H.; Fox, N.C.; Gamst, A.; Holtzman, D.M.; Jagust, W.J.; Petersen, R.C.; et al. The Diagnosis of Mild Cognitive Impairment due to Alzheimer’s Disease: Recommendations from the National Institute on Aging-Alzheimer’s Association Workgroups on Diagnostic Guidelines for Alzheimer’s Disease. Alzheimer’s Dement. 2011, 7, 270–279. [Google Scholar] [CrossRef] [PubMed]
- McGrattan, A.M.; Pakpahan, E.; Siervo, M.; Mohan, D.; Reidpath, D.D.; Prina, M.; Allotey, P.; Zhu, Y.; Shulin, C.; Yates, J. Risk of conversion from mild cognitive impairment to dementia in low-and middle-income countries: A systematic review and meta-analysis. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2022, 8, e12267. [Google Scholar] [CrossRef] [PubMed]
- McKhann, G.M.; Knopman, D.S.; Chertkow, H.; Hyman, B.T.; Jack, C.R., Jr.; Kawas, C.H.; Klunk, W.E.; Koroshetz, W.J.; Manly, J.J.; Mayeux, R. The diagnosis of dementia due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s Dement. 2011, 7, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Hyman, B.T.; Phelps, C.H.; Beach, T.G.; Bigio, E.H.; Cairns, N.J.; Carrillo, M.C.; Dickson, D.W.; Duyckaerts, C.; Frosch, M.P.; Masliah, E. National Institute on Aging–Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease. Alzheimer’s Dement. 2012, 8, 1–13. [Google Scholar] [CrossRef]
- Risacher, S.; Saykin, A.; Wes, J.; Shen, L.; Firpi, H.; McDonald, B. Baseline MRI Predictors of Conversion from MCI to Probable AD in the ADNI Cohort. Curr. Alzheimer Res. 2009, 6, 347–361. [Google Scholar] [CrossRef]
- Qiu, A.; Fennema-Notestine, C.; Dale, A.M.; Miller, M.I. Regional shape abnormalities in mild cognitive impairment and Alzheimer’s disease. Neuroimage 2009, 45, 656–661. [Google Scholar] [CrossRef]
- Guévremont, D.; Tsui, H.; Knight, R.; Fowler, C.J.; Masters, C.L.; Martins, R.N.; Abraham, W.C.; Tate, W.P.; Cutfield, N.; Williams, J.M. Plasma microRNA vary in association with the progression of Alzheimer’s disease. Alzheimer’s Dement. 2022, 14, e12251. [Google Scholar] [CrossRef]
- Mesa-Herrera, F.; Marin, R.; Torrealba, E.; Santos, G.; Diaz, M. Neuronal ER-Signalosome Proteins as Early Biomarkers in Prodromal Alzheimer’s Disease Independent of Amyloid-beta Production and Tau Phosphorylation. Front. Mol. Neurosci. 2022, 15, 1–20. [Google Scholar] [CrossRef]
- Shahid, S.S.; Wen, Q.; Risacher, S.L.; Farlow, M.R.; Unverzagt, F.W.; Apostolova, L.G.; Foroud, T.M.; Zetterberg, H.; Blennow, K.; Saykina, A.J.; et al. Hippocampal-subfield microstructures and their relation to plasma biomarkers in Alzheimer’s disease. Brain 2022, 145, 2149–2160. [Google Scholar] [CrossRef]
- Vaghari, D.; Kabir, E.; Henson, R.N. Late combination shows that MEG adds to MRI in classifying MCI versus controls. Neuroimage 2022, 252, 119054. [Google Scholar] [CrossRef] [PubMed]
- Klöppel, S.; Stonnington, C.M.; Chu, C.; Draganski, B.; Scahill, R.I.; Rohrer, J.D.; Fox, N.C.; Jack, C.R., Jr.; Ashburner, J.; Frackowiak, R.S. Automatic classification of MR scans in Alzheimer’s disease. Brain 2008, 131, 681–689. [Google Scholar] [CrossRef]
- Janousova, E.; Vounou, M.; Wolz, R.; Gray, K.R.; Rueckert, D.; Montana, G. Biomarker discovery for sparse classification of brain images in Alzheimer’s disease. Ann. BMVA 2012, 2, 1–11. [Google Scholar]
- Zhang, D.; Wang, Y.; Zhou, L.; Yuan, H.; Shen, D. Multimodal classification of Alzheimer’s disease and mild cognitive impairment. Neuroimage 2011, 55, 856–867. [Google Scholar] [CrossRef]
- Liu, S.; Song, Y.; Cai, W.; Pujol, S.; Kikinis, R.; Wang, X.; Feng, D. Multifold Bayesian kernelization in Alzheimer’s diagnosis. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Nagoya, Japan, 22–26 September 2013; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Zhang, Y.; Dong, Z.; Phillips, P.; Wang, S.; Ji, G.; Yang, J.; Yuan, T.-F. Detection of subjects and brain regions related to Alzheimer’s disease using 3D MRI scans based on eigenbrain and machine learning. Front. Comput. Neurosci. 2015, 9, 66. [Google Scholar] [CrossRef]
- Hong, S.; Coelho, C.A.; Park, J. An Exact and Near-Exact Distribution Approach to the Behrens–Fisher Problem. Mathematics 2022, 10, 2953. [Google Scholar] [CrossRef]
- Esteki, S.; Naghsh-Nilchi, A.R. Frequency component Kernel for SVM. Neural Comput. Appl. 2022, 34, 22449–22464. [Google Scholar] [CrossRef]
- Nayak, J.; Swapnarekha, H.; Naik, B.; Dhiman, G.; Vimal, S. 25 Years of Particle Swarm Optimization: Flourishing Voyage of Two Decades. Arch. Comput. Methods Eng. 2022, 30, 1663–1725. [Google Scholar] [CrossRef]
- Sonoda, S.; Murata, N. Neural network with unbounded activation functions is universal approximator. Appl. Comput. Harmon. Anal. 2017, 43, 233–268. [Google Scholar] [CrossRef]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A.; et al. International evaluation of an AI system for breast cancer screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef]
- Zaidi, S.M.A.; Habib, S.S.; Van Ginneken, B.; Ferrand, R.A.; Creswell, J.; Khowaja, S.; Khan, A. Evaluation of the diagnostic accuracy of Computer-Aided Detection of tuberculosis on Chest radiography among private sector patients in Pakistan. Sci. Rep. 2018, 8, 12339. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Park, J.E.; Kim, Y.-H.; Kim, J.H.; Oh, J.Y.; Kim, J.; Kim, Y.; Kim, S.T.; Kim, H.S. Diffusion radiomics as a diagnostic model for atypical manifestation of primary central nervous system lymphoma: Development and multicenter external validation. Neuro-Oncology 2018, 20, 1251–1261. [Google Scholar] [CrossRef]
- Feng, X.; Provenzano, F.A.; Small, S.A.; Initiative, F.T.A.D.N. A deep learning MRI approach outperforms other biomarkers of prodromal Alzheimer’s disease. Alzheimer’s Res. Ther. 2022, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Zhang, Y.Y.; Li, H.L.; Tong, X.R.; Ouyang, M.H. How segmentation methods affect hippocampal radiomic feature accuracy in Alzheimer’s disease analysis? Eur. Radiol. 2022, 32, 6965–6976. [Google Scholar] [CrossRef]
- Aly, M.F.A.; Kleijn, S.A.; van Lenthe, J.H.; Menken-Negroiu, R.F.; Robbers, L.F.; Beek, A.M.; Kamp, O. Prediction of prognosis in patientswith left ventricular dysfunction using three-dimensional strain echocardiography and cardiac magnetic resonance imaging. Neth. Heart J. 2022, 30, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Khojaste-Sarakhsi, M.; Haghighi, S.S.; Ghomi, S.; Marchiori, E. Deep learning for Alzheimer’s disease diagnosis: A survey. Artif. Intell. Med. 2022, 130, 102332. [Google Scholar] [CrossRef]
- Reith, F.H.; Mormino, E.C.; Zaharchuk, G. Predicting future amyloid biomarkers in dementia patients with machine learning to improve clinical trial patient selection. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2021, 7, e12212. [Google Scholar] [CrossRef]
- Kim, Y.; Jiang, X.; Giancardo, L.; Pena, D.; Bukhbinder, A.S.; Amran, A.Y.; Schulz, P.E.; Initiative, A.D.N. Multimodal Phenotyping of Alzheimer’s Disease with Longitudinal Magnetic Resonance Imaging and Cognitive Function Data. Sci. Rep. 2020, 10, 5527. [Google Scholar] [CrossRef]
- Chen, K.T.; Gong, E.; Macruz, F.B.D.C.; Xu, J.; Boumis, A.; Khalighi, M.; Poston, K.L.; Sha, S.J.; Greicius, M.D.; Mormino, E.; et al. Ultra–Low-Dose18F-Florbetaben Amyloid PET Imaging Using Deep Learning with Multi-Contrast MRI Inputs. Radiology 2019, 290, 649–656. [Google Scholar] [CrossRef]
- Monfared, A.A.T.; Houghton, K.; Zhang, Q.; Mauskopf, J.; Initiative, F.T.A.D.N. Staging Disease Severity Using the Alzheimer’s Disease Composite Score (ADCOMS): A Retrospective Data Analysis. Neurol. Ther. 2022, 11, 413–434. [Google Scholar] [CrossRef] [PubMed]
- Sheng, J.H.; Wang, B.C.; Zhang, Q.; Zhou, R.G.; Wang, L.Y.; Xin, Y. Identifying and characterizing different stages toward Alzheimer’s disease using ordered core features and machine learning. Heliyon 2021, 7, e07287. [Google Scholar] [CrossRef]
- Kazee, A.; Eskin, T.; Lapham, L.; Gabriel, K.; McDaniel, K.; Hamill, R. Clinicopathologic correlates in Alzheimer disease: Assessment of clinical and pathologic diagnostic criteria. Alzheimer Dis. Assoc. Disord. 1993, 7, 152–164. [Google Scholar] [CrossRef] [PubMed]
- Price, J.L.; Davis, P.; Morris, J.; White, D. The distribution of tangles, plaques and related immunohistochemical markers in healthy aging and Alzheimer’s disease. Neurobiol. Aging 1991, 12, 295–312. [Google Scholar] [CrossRef]
- Bennett, D.A.; Schneider, J.A.; Arvanitakis, Z.; Kelly, J.F.; Aggarwal, N.T.; Shah, R.; Wilson, R.S. Neuropathology of older persons without cognitive impairment from two community-based studies. Neurology 2006, 66, 1837–1844. [Google Scholar] [CrossRef] [PubMed]
- Gopinadhan, A.; Prasanna, G.; Anbarasu, S. AD-EHS: Alzheimer’s disease severity detection using efficient hybrid image segmentation. Adv. Eng. Softw. 2022, 173, 103234. [Google Scholar] [CrossRef]
- Krell-Roesch, J.; Rakusa, M.; Syrjanen, J.A.; van Harten, A.C.; Lowe, V.J.; Jack, C.R.; Kremers, W.K.; Knopman, D.S.; Stokin, G.B.; Petersen, R.C.; et al. Association between CSF biomarkers of Alzheimer’s disease and neuropsychiatric symptoms: Mayo Clinic Study of Aging. Alzheimer’s Dement. 2022, 1–9. [Google Scholar] [CrossRef]
- Mol, M.O.; van der Lee, S.J.; Hulsman, M.; Pijnenburg, Y.A.L.; Scheltens, P.; Seelaar, H.; van Swieten, J.C.; Kaat, L.D.; Holstege, H.; van Rooij, J.G.J.; et al. Mapping the genetic landscape of early-onset Alzheimer’s disease in a cohort of 36 families. Alzheimer’s Res. Ther. 2022, 14, 1–14. [Google Scholar] [CrossRef]
- Wen, J.; Thibeau-Sutre, E.; Diaz-Melo, M.; Samper-González, J.; Routier, A.; Bottani, S.; Dormont, D.; Durrleman, S.; Burgos, N.; Colliot, O. Convolutional Neural Networks for Classification of Alzheimer’s Disease: Overview and Reproducible Evaluation. Med. Image Anal. 2020, 63, 101694. [Google Scholar] [CrossRef]
- Samper-Gonzalez, J.; Burgos, N.; Bottani, S.; Fontanella, S.; Lu, P.; Marcoux, A.; Routier, A.; Guillon, J.; Bacci, M.; Wen, J. Reproducible evaluation of classification methods in Alzheimer’s disease: Framework and application to MRI and PET data. NeuroImage 2018, 183, 504–521. [Google Scholar] [CrossRef]
- Fraternali, P.; Milani, F.; Torres, R.N.; Zangrando, N. Black-box error diagnosis in Deep Neural Networks for computer vision: A survey of tools. Neural Comput. Appl. 2022, 35, 3041–3062. [Google Scholar] [CrossRef]
- Garnier, R.; Langhendries, R. Concentration inequalities for non-causal random fields. Electron. J. Stat. 2022, 16, 1681–1725. [Google Scholar] [CrossRef]
- Adali, T.; Calhoun, V.D. Reproducibility and replicability in neuroimaging data analysis. Curr. Opin. Neurol. 2022, 35, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, G.C.; Twose, C.; Weller, A.; Dougherty, J.W.; Goes, F.S.; Sair, H.I.; Smith, G.S.; Roy, D. Neuroimaging Correlates of Depression after Traumatic Brain Injury: A Systematic Review. J. Neurotrauma 2022, 39, 755–772. [Google Scholar] [CrossRef] [PubMed]
- Rathore, S.; Habes, M.; Iftikhar, M.A.; Shacklett, A.; Davatzikos, C. A review on neuroimaging-based classification studies and associated feature extraction methods for Alzheimer’s disease and its prodromal stages. NeuroImage 2017, 155, 530–548. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimighahnavieh, M.A.; Luo, S.; Chiong, R. Deep learning to detect Alzheimer’s disease from neuroimaging: A systematic literature review. Comput. Methods Programs Biomed. 2020, 187, 105242. [Google Scholar] [CrossRef]
- Fernando, K.R.M.; Tsokos, C.P. Deep and statistical learning in biomedical imaging: State of the art in 3D MRI brain tumor segmentation. Inf. Fusion 2023, 92, 450–465. [Google Scholar] [CrossRef]
- Du, B.; Cheng, X.; Duan, Y.; Ning, H. fMRI Brain Decoding and Its Applications in Brain–Computer Interface: A Survey. Brain Sci. 2022, 12, 228. [Google Scholar] [CrossRef]
- Patel, B.; Irwin, D.J.; Kaufer, D.; Boeve, B.F.; Taylor, A.; Armstrong, M.J. Outcome Measures for Dementia with Lewy Body Clinical Trials A Review. Alzheimer Dis. Assoc. Disord. 2022, 36, 64–72. [Google Scholar] [CrossRef]
- Zhang, T.J.; Sui, Y.X.; Lu, Q.; Xu, X.J.; Zhu, Y.; Dai, W.J.; Shen, Y.; Wang, T. Effects of rTMS treatment on global cognitive function in Alzheimer’s disease: A systematic review and meta-analysis. Front. Aging Neurosci. 2022, 14, 984708. [Google Scholar] [CrossRef]
- Skinner, J.; Initiative, F.T.A.D.N.; Carvalho, J.O.; Potter, G.G.; Thames, A.D.; Zelinski, E.M.; Crane, P.; Gibbons, L.E. The Alzheimer’s Disease Assessment Scale-Cognitive-Plus (ADAS-Cog-Plus): An expansion of the ADAS-Cog to improve responsiveness in MCI. Brain Imaging Behav. 2012, 6, 489–501. [Google Scholar] [CrossRef]
- Vyhnalek, M.; Jester, D.J.; Andel, R.; Horakova, H.; Nikolai, T.; Laczó, J.; Matuskova, V.; Cechova, K.; Sheardova, K.; Hort, J. Contribution of Memory Tests to Early Identification of Conversion from Amnestic Mild Cognitive Impairment to Dementia. J. Alzheimer’s Dis. 2022, 88, 1397–1409. [Google Scholar] [CrossRef] [PubMed]
- Abikoff, H.; Alvir, J.; Hong, G.; Sukoff, R.; Orazio, J.; Solomon, S.; Saravay, S. Logical memory subtest of the wechsler memory scale: Age and education norms and alternate-form reliability of two scoring systems. J. Clin. Exp. Neuropsychol. 1987, 9, 435–448. [Google Scholar] [CrossRef]
- Mills, S.J.; Mackintosh, S.; McDonnell, M.N.; Thewlis, D. Improvement in postural alignment is associated with recovery of mobility after complex acquired brain injury: An observational study. Physiother. Theory Pract. 2022, 39, 1274–1286. [Google Scholar] [CrossRef]
- Costa, L.; Gago, M.F.; Yelshyna, D.; Ferreira, J.; Silva, H.D.; Rocha, L.; Sousa, N.; Bicho, E. Application of Machine Learning in Postural Control Kinematics for the Diagnosis of Alzheimer’s Disease. Comput. Intell. Neurosci. 2016, 2016, 1–15. [Google Scholar] [CrossRef]
- Gannouni, S.; Aledaily, A.; Belwafi, K.; Aboalsamh, H. Electroencephalography based emotion detection using ensemble classification and asymmetric brain activity. J. Affect. Disord. 2022, 319, 416–427. [Google Scholar] [CrossRef]
- Morabito, F.C.; Campolo, M.; Ieracitano, C.; Ebadi, J.M.; Bonanno, L.; Bramanti, A.; Desalvo, S.; Mammone, N.; Bramanti, P. Deep convolutional neural networks for classification of mild cognitive impaired and Alzheimer’s disease patients from scalp EEG recordings. In Proceedings of the 2016 IEEE 2nd International Forum on Research and Technologies for Society and Industry Leveraging a Better Tomorrow (RTSI), Bologna, Italy, 7–9 September 2016. [Google Scholar]
- Anyaiwe, D.E.; Wilson, G.D.; Geddes, T.J.; Singh, G.B. Harnessing mass spectra data using KNN principle: Diagnosing Alzheimer’s disease. ACM SIGBioinformatics Rec. 2018, 7, 1–7. [Google Scholar] [CrossRef]
- Wisely, C.E.; Wang, D.; Henao, R.; Grewal, D.S.; Yoon, S.P.; Polascik, B.; Thompson, A.C.; Burke, J.R.; Carin, L.; Fekrat, S. Deep learning algorithm for diagnosis of Alzheimer’s disease using multimodal retinal imaging. Investig. Ophthalmol. Vis. Sci. 2019, 60, 1461. [Google Scholar]
- Landi, I.; Glicksberg, B.S.; Lee, H.-C.; Cherng, S.; Landi, G.; Danieletto, M.; Dudley, J.T.; Furlanello, C.; Miotto, R. Deep representation learning of electronic health records to unlock patient stratification at scale. NPJ Digit. Med. 2020, 3, 96. [Google Scholar] [CrossRef]
- Park, J.H.; Cho, H.E.; Kim, J.H.; Wall, M.M.; Stern, Y.; Lim, H.; Yoo, S.; Kim, H.S.; Cha, J. Machine learning prediction of incidence of Alzheimer’s disease using large-scale administrative health data. NPJ Digit. Med. 2020, 3, 46. [Google Scholar] [CrossRef]
- Tang, F.; Uchendu, I.; Wang, F.; Dodge, H.H.; Zhou, J. Scalable diagnostic screening of mild cognitive impairment using AI dialogue agent. Sci. Rep. 2020, 10, 5732. [Google Scholar] [CrossRef]
- Chien, Y.-W.; Hong, S.-Y.; Cheah, W.-T.; Yao, L.-H.; Chang, Y.-L.; Fu, L.-C. An Automatic Assessment System for Alzheimer’s Disease Based on Speech Using Feature Sequence Generator and Recurrent Neural Network. Sci. Rep. 2019, 9, 19597. [Google Scholar] [CrossRef]
- Lam, K.-Y.; Tsang, N.W.-H.; Han, S.; Zhang, W.; Ng, J.K.-Y.; Nath, A. Activity tracking and monitoring of patients with Alzheimer’s disease. Multimed. Tools Appl. 2015, 76, 489–521. [Google Scholar] [CrossRef]
- Toosizadeh, N.; Ehsani, H.; Wendel, C.; Zamrini, E.; Connor, K.O.; Mohler, J. Screening older adults for amnestic mild cognitive impairment and early-stage Alzheimer’s disease using upper-extremity dual-tasking. Sci. Rep. 2019, 9, 10911. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.U.; Pongos, A.L.; Manzanares, C.M.; Lah, J.J.; Levey, A.I.; Clifford, G.D. Deep Convolutional Neural Networks and Transfer Learning for Measuring Cognitive Impairment Using Eye-Tracking in a Distributed Tablet-Based Environment. IEEE Trans. Biomed. Eng. 2020, 68, 11–18. [Google Scholar] [CrossRef]
- Farina, F.; Emek-Savaş, D.; Rueda-Delgado, L.; Boyle, R.; Kiiski, H.; Yener, G.; Whelan, R. A comparison of resting state EEG and structural MRI for classifying Alzheimer’s disease and mild cognitive impairment. Neuroimage 2020, 215, 116795. [Google Scholar] [CrossRef] [PubMed]
- Ashford, M.T.; Raman, R.; Miller, G.; Donohue, M.C.; Okonkwo, O.C.; Mindt, M.R.; Nosheny, R.L.; Coker, G.A.; Petersen, R.C.; Aisen, P.S.; et al. Screening and enrollment of underrepresented ethnocultural and educational populations in the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Alzheimer’s Dement. 2022, 18, 2603–2613. [Google Scholar] [CrossRef]
- Nanayakkara, N.D.; Arnott, S.R.; Scott, C.J.; Solovey, I.; Liang, S.; Fonov, V.S.; Gee, T.; Broberg, D.N.; Haddad, S.M.; Ramirez, J.; et al. Increased brain volumetric measurement precision from multi-site 3D T1-weighted 3 T magnetic resonance imaging by correcting geometric distortions. Magn. Reson. Imaging 2022, 92, 150–160. [Google Scholar] [CrossRef]
- Weiner, M.W.; Aisen, P.S.; Jack, C.R., Jr.; Jagust, W.J.; Trojanowski, J.Q.; Shaw, L.; Saykin, A.J.; Morris, J.C.; Cairns, N.; Beckett, L.A. The Alzheimer’s disease neuroimaging initiative: Progress report and future plans. Alzheimer’s Dement. 2010, 6, 202–211.e7. [Google Scholar] [CrossRef] [PubMed]
- Weiner, M.W.; Veitch, D.P.; Aisen, P.S.; Beckett, L.A.; Cairns, N.J.; Cedarbaum, J.; Donohue, M.C.; Green, R.C.; Harvey, D.; Jack, C.R., Jr. Impact of the Alzheimer’s disease neuroimaging initiative, 2004 to 2014. Alzheimer’s Dement. 2015, 11, 865–884. [Google Scholar] [CrossRef]
- Weiner, M.W.; Veitch, D.P.; Aisen, P.S.; Beckett, L.A.; Cairns, N.J.; Green, R.C.; Harvey, D.; Jack, C.R., Jr.; Jagust, W.; Morris, J.C. The Alzheimer’s Disease Neuroimaging Initiative 3: Continued innovation for clinical trial improvement. Alzheimer’s Dement. 2017, 13, 561–571. [Google Scholar] [CrossRef]
- LaMontagne, P.J.; Benzinger, T.L.; Morris, J.C.; Keefe, S.; Hornbeck, R.; Xiong, C.; Grant, E.; Hassenstab, J.; Moulder, K.; Vlassenko, A.G.; et al. OASIS-3: Longitudinal neuroimaging, clinical, and cognitive dataset for normal aging and Alzheimer disease. medRxiv 2019, 12, 19014902. [Google Scholar]
- Dagley, A.; LaPoint, M.; Huijbers, W.; Hedden, T.; McLaren, D.G.; Chatwal, J.P.; Papp, K.V.; Amariglio, R.E.; Blacker, D.; Rentz, D.M.; et al. Harvard Aging Brain Study: Dataset and accessibility. Neuroimage 2017, 144, 255–258. [Google Scholar] [CrossRef]
- Malone, I.; Cash, D.; Ridgway, G.; MacManus, D.; Ourselin, S.; Fox, N.; Schott, J. MIRIAD (Minimal Interval Resonance Imaging in Alzheimer’s Disease). NeuroImage 2013, 70, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Iwatsubo, T. Japanese Alzheimer’s Disease Neuroimaging Initiative: Present status and future. Alzheimer’s Dement. 2010, 6, 297–299. [Google Scholar] [CrossRef]
- Sun, W.; Wu, Q.; Chen, H.; Yu, L.; Yin, J.; Liu, F.; Tian, R.; Song, B.; Qu, B.; Xing, M.; et al. A Validation Study of the Hong Kong Brief Cognitive Test for Screening Patients with Mild Cognitive Impairment and Alzheimer’s Disease. J. Alzheimer’s Dis. 2022, 88, 1523–1532. [Google Scholar] [CrossRef]
- Ellis, K.A.; Bush, A.I.; Darby, D.; De Fazio, D.; Foster, J.; Hudson, P.; Lautenschlager, N.T.; Lenzo, N.; Martins, R.N.; Maruff, P. The Australian Imaging, Biomarkers and Lifestyle (AIBL) study of aging: Methodology and baseline characteristics of 1112 individuals recruited for a longitudinal study of Alzheimer’s disease. Int. Psychogeriatr. 2009, 21, 672–687. [Google Scholar] [CrossRef] [PubMed]
- Nigri, A.; Ferraro, S.; Wheeler-Kingshott, C.A.M.G.; Tosetti, M.; Redolfi, A.; Forloni, G.; D’Angelo, E.; Aquino, D.; Biagi, L.; Bosco, P.; et al. Quantitative MRI Harmonization to Maximize Clinical Impact: The RIN–Neuroimaging Network. Front. Neurol. 2022, 13, 855125. [Google Scholar] [CrossRef]
- Redolfi, A.; McClatchey, R.; Anjum, A.; Zijdenbos, A.; Manset, D.; Barkhof, F.; Spenger, C.; Legré, Y.; Wahlund, L.-O.; Pietro, C.B.d.S.; et al. Grid infrastructures for computational neuroscience: The neuGRID example. Futur. Neurol. 2009, 4, 703–722. [Google Scholar] [CrossRef]
- Toga, A.W.; Neu, S.C.; Bhatt, P.; Crawford, K.L.; Ashish, N. The global Alzheimer’s association interactive network. Alzheimer’s Dement. 2016, 12, 49–54. [Google Scholar] [CrossRef]
- Bron, E.E.; Smits, M.; van der Flier, W.M.; Vrenken, H.; Barkhof, F.; Scheltens, P.; Papma, J.M.; Steketee, R.M.; Orellana, C.M.; Meijboom, R.; et al. Standardized evaluation of algorithms for computer-aided diagnosis of dementia based on structural MRI: The CADDementia challenge. Neuroimage 2015, 111, 562–579. [Google Scholar] [CrossRef]
- Hernandez, M.; Ramon-Julvez, U.; Ferraz, F. With the ADNI Consortium Explainable AI toward understanding the performance of the top three TADPOLE Challenge methods in the forecast of Alzheimer’s disease diagnosis. PLoS ONE 2022, 17, e0264695. [Google Scholar] [CrossRef]
- Marinescu, R.V.; Oxtoby, N.P.; Young, A.L.; Bron, E.E.; Toga, A.W.; Weiner, M.W.; Barkhof, F.; Fox, N.C.; Klein, S.; Alexander, D.C. Tadpole challenge: Prediction of longitudinal evolution in Alzheimer’s disease. arXiv 2018, arXiv:1805.03909. [Google Scholar]
- Allen, G.I.; Amoroso, N.; Anghel, C.; Balagurusamy, V.; Bare, C.J.; Beaton, D.; Bellotti, R.; Bennett, D.A.; Boehme, K.L.; Boutros, P.C. Crowdsourced estimation of cognitive decline and resilience in Alzheimer’s disease. Alzheimer’s Dement. 2016, 12, 645–653. [Google Scholar] [CrossRef]
- El-Gazzar, A.; Thomas, R.M.; van Wingen, G. Dynamic Adaptive Spatio-Temporal Graph Convolution for fMRI Modelling. In Machine Learning in Clinical Neuroimaging. Proceedings of the 4th International Workshop, MLCN 2021, Held in Conjunction with MICCAI 2021, Strasbourg, France, 27 September 2021; Proceedings 4; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 125–134. [Google Scholar] [CrossRef]
- Varzandian, A.; Razo, M.A.S.; Sanders, M.R.; Atmakuru, A.; Di Fatta, G. Classification-Biased Apparent Brain Age for the Prediction of Alzheimer’s Disease. Front. Neurosci. 2021, 15, 673120. [Google Scholar] [CrossRef]
- Fu, Y.; Huang, Y.; Wang, Y.; Dong, S.; Xue, L.; Yin, X.; Yang, Q.; Shi, Y.; Zhuo, C. OTFPF: Optimal Transport-Based Feature Pyramid Fusion Network for Brain Age Estimation with 3D Overlapped ConvNeXt. arXiv 2022, arXiv:2205.04684. [Google Scholar]
- Bycroft, C.; Freeman, C.; Petkova, D.; Band, G.; Elliott, L.T.; Sharp, K.; Motyer, A.; Vukcevic, D.; Delaneau, O.; O’connell, J.; et al. The UK Biobank resource with deep phenotyping and genomic data. Nature 2018, 562, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.-l.; Marcora, E.; Pimenova, A.A.; Di Narzo, A.F.; Kapoor, M.; Jin, S.C.; Harari, O.; Bertelsen, S.; Fairfax, B.P.; Czajkowski, J. A common haplotype lowers PU. 1 expression in myeloid cells and delays onset of Alzheimer’s disease. Nat. Neurosci. 2017, 20, 1052–1061. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Luchetti, M.; Aschwanden, D.; Sesker, A.A.; Stephan, Y.; Sutin, A.R.; Terracciano, A. Satisfaction With Life and Risk of Dementia: Findings From the Korean Longitudinal Study of Aging. J. Gerontol. Ser. B 2022, 77, 1831–1840. [Google Scholar] [CrossRef]
- Suh, S.; Han, J.; Oh, S.; Kim, K. Impact of sleep on future cognition in non-demented elderly: Results from the korean longitudinal study on cognitive aging and dementia (kloscad). J. Neurol. Sci. 2017, 381, 182. [Google Scholar] [CrossRef]
- Sakr, F.A.; Grothe, M.J.; Cavedo, E.; Jelistratova, I.; Habert, M.-O.; Dyrba, M.; Gonzalez-Escamilla, G.; Bertin, H.; Locatelli, M.; Lehericy, S.; et al. Applicability of in vivo staging of regional amyloid burden in a cognitively normal cohort with subjective memory complaints: The INSIGHT-preAD study. Alzheimer’s Res. Ther. 2019, 11, 15. [Google Scholar] [CrossRef]
- Dubois, B.; Epelbaum, S.; Nyasse, F.; Bakardjian, H.; Gagliardi, G.; Uspenskaya, O.; Houot, M.; Lista, S.; Cacciamani, F.; Potier, M.-C. Cognitive and neuroimaging features and brain β-amyloidosis in individuals at risk of Alzheimer’s disease (INSIGHT-preAD): A longitudinal observational study. Lancet Neurol. 2018, 17, 335–346. [Google Scholar] [CrossRef]
- Wilkins, C.H.; Windon, C.C.; Dilworth-Anderson, P.; Romanoff, J.; Gatsonis, C.; Hanna, L.; Apgar, C.; Gareen, I.F.; Hill, C.V.; Hillner, B.E. Racial and Ethnic Differences in Amyloid PET Positivity in Individuals with Mild Cognitive Impairment or Dementia: A Secondary Analysis of the Imaging Dementia–Evidence for Amyloid Scanning (IDEAS) Cohort Study. JAMA Neurol. 2022, 79, 1139–1147. [Google Scholar] [CrossRef]
- Silva, T.C.; Zhang, W.; Young, J.I.; Gomez, L.; Schmidt, M.A.; Varma, A.; Chen, X.S.; Martin, E.R.; Wang, L. Distinct sex-specific DNA methylation differences in Alzheimer’s disease. Alzheimer’s Res. Ther. 2022, 14, 1–21. [Google Scholar] [CrossRef]
- Lovestone, S.; Francis, P.; Kloszewska, I.; Mecocci, P.; Simmons, A.; Soininen, H.; Spenger, C.; Tsolaki, M.; Vellas, B.; Wahlund, L.O.; et al. AddNeuroMed—The European collaboration for the discovery of novel biomarkers for Alzheimer’s disease. Ann. N. Y. Acad. Sci. 2009, 1180, 36–46. [Google Scholar] [CrossRef]
- Chen, S.; Stromer, D.; Alabdalrahim, H.A.; Schwab, S.; Weih, M.; Maier, A. Automatic dementia screening and scoring by applying deep learning on clock-drawing tests. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Gorgolewski, K.J.; Auer, T.; Calhoun, V.D.; Craddock, R.C.; Das, S.; Duff, E.P.; Flandin, G.; Ghosh, S.S.; Glatard, T.; Halchenko, Y.O.; et al. The brain imaging data structure, a format for organizing and describing outputs of neuroimaging experiments. Sci. Data 2016, 3, 1–9. [Google Scholar] [CrossRef]
- Hu, Z.; Wang, Z.; Jin, Y.; Hou, W. VGG-TSwinformer: Transformer-based deep learning model for early Alzheimer’s disease prediction. Comput. Methods Programs Biomed. 2023, 229, 107291. [Google Scholar] [CrossRef]
- Houria, L.; Belkhamsa, N.; Cherfa, A.; Cherfa, Y. Multi-modality MRI for Alzheimer’s disease detection using deep learning. Phys. Eng. Sci. Med. 2022, 45, 1043–1053. [Google Scholar] [CrossRef]
- Pan, D.; Zeng, A.; Yang, B.Y.; Lai, G.Y.; Hu, B.; Song, X.W.; Jiang, T.Z. Deep Learning for Brain MRI Confirms Patterned Pathological Progression in Alzheimer’s Disease. Adv. Sci. 2022, 10, 2204717. [Google Scholar] [CrossRef]
- Jindal, S.K.; Banerjee, S.; Patra, R.; Paul, A. Deep learning-based brain malignant neoplasm classification using MRI image segmentation assisted by bias field correction and histogram equalization. In Brain Tumor MRI Image Segmentation Using Deep Learning Techniques; Elsevier: Amsterdam, The Netherlands, 2022; pp. 135–161. [Google Scholar]
- Gispert, J.D.; Reig, S.; Pascau, J.; Vaquero, J.J.; García-Barreno, P.; Desco, M. Method for bias field correction of brain T1-weighted magnetic resonance images minimizing segmentation error. Hum. Brain Mapp. 2004, 22, 133–144. [Google Scholar] [CrossRef]
- Wu, L.; He, T.; Yu, J.; Liu, H.; Zhang, S.; Zhang, T. Volume and surface coil simultaneous reception (VSSR) method for intensity inhomogeneity correction in MRI. Technol. Health Care 2022, 30, 827–838. [Google Scholar] [CrossRef]
- Sled, J.G.; Zijdenbos, A.P.; Evans, A.C. A nonparametric method for automatic correction of intensity nonuniformity in MRI data. IEEE Trans. Med. Imaging 1998, 17, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.; Liu, Z.; Yan, W.Q.; Klette, R. Early diagnosis of Alzheimer’s disease using deep learning. In Proceedings of the 2nd International Conference on Control and Computer Vision, Jeju, Republic of Korea, 15–18 June 2019. [Google Scholar]
- Bhattacharjee, R.; Heitz, F.; Noblet, V.; Sharma, S.; Sharma, N. Evaluation of a Learning-based Deformable Registration Method on Abdominal CT Images. IRBM 2020, 42, 94–105. [Google Scholar] [CrossRef]
- Andersson, J.L.; Jenkinson, M.; Smith, S. Non-Linear Registration Aka Spatial Normalisation FMRIB Technial Report TR07JA2; FMRIB Analysis Group of the University of Oxford: Oxford, UK, 2007; pp. 1–22. [Google Scholar]
- Jenkinson, M.; Smith, S. A global optimisation method for robust affine registration of brain images. Med. Image Anal. 2001, 5, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Mazziotta, J.; Toga, A.; Evans, A.; Fox, P.; Lancaster, J.; Zilles, K.; Woods, R.; Paus, T.; Simpson, G.; Pike, B. A four-dimensional probabilistic atlas of the human brain. J. Am. Med. Inform. Assoc. 2001, 8, 401–430. [Google Scholar] [CrossRef]
- Ramon-Julvez, U.; Hernandez, M.; Mayordomo, E. Adni Analysis of the Influence of Diffeomorphic Normalization in the Prediction of Stable VS Progressive MCI Conversion with Convolutional Neural Networks. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020. [Google Scholar] [CrossRef]
- Chen, C.-L.; Hsu, Y.-C.; Yang, L.-Y.; Tung, Y.-H.; Luo, W.-B.; Liu, C.-M.; Hwang, T.-J.; Hwu, H.-G.; Tseng, W.-Y.I. Generalization of diffusion magnetic resonance imaging–based brain age prediction model through transfer learning. Neuroimage 2020, 217, 116831. [Google Scholar] [CrossRef]
- Ahmed, S.; Choi, K.Y.; Lee, J.J.; Kim, B.C.; Kwon, G.-R.; Lee, K.H.; Jung, H.Y. Ensembles of Patch-Based Classifiers for Diagnosis of Alzheimer Diseases. IEEE Access 2019, 7, 73373–73383. [Google Scholar] [CrossRef]
- Patenaude, B.; Smith, S.M.; Kennedy, D.N.; Jenkinson, M. A Bayesian model of shape and appearance for subcortical brain segmentation. NeuroImage 2011, 56, 907–922. [Google Scholar] [CrossRef]
- Suk, H.-I.; Lee, S.-W.; Shen, D. Hierarchical feature representation and multimodal fusion with deep learning for AD/MCI diagnosis. Neuroimage 2014, 101, 569–582. [Google Scholar] [CrossRef]
- Lin, W.; Tong, T.; Gao, Q.; Guo, D.; Du, X.; Yang, Y.; Guo, G.; Xiao, M.; Du, M.; Qu, X.; et al. Convolutional Neural Networks-Based MRI Image Analysis for the Alzheimer’s Disease Prediction from Mild Cognitive Impairment. Front. Neurosci. 2018, 12, 777. [Google Scholar] [CrossRef]
- Basher, A.; Choi, K.Y.; Lee, J.J.; Lee, B.; Kim, B.C.; Lee, K.H.; Jung, H.Y. Hippocampus Localization Using a Two-Stage Ensemble Hough Convolutional Neural Network. IEEE Access 2019, 7, 73436–73447. [Google Scholar] [CrossRef]
- Liu, M.; Li, F.; Yan, H.; Wang, K.; Ma, Y.; Shen, L.; Xu, M. A multi-model deep convolutional neural network for automatic hippocampus segmentation and classification in Alzheimer’s disease. Neuroimage 2020, 208, 116459. [Google Scholar] [CrossRef]
- Liu, M.; Initiative, T.A.D.N.; Cheng, D.; Wang, K.; Wang, Y. Multi-Modality Cascaded Convolutional Neural Networks for Alzheimer’s Disease Diagnosis. Neuroinformatics 2018, 16, 295–308. [Google Scholar] [CrossRef]
- Prem Kumar, A.; Singh, N.; Nair, D.; Justin, A. Neuronal PET tracers for Alzheimer’s disease. Biochem. Biophys. Res. Commun. 2022, 587, 58–62. [Google Scholar] [CrossRef]
- Zhou, D.A.; Xu, K.; Zhao, X.B.; Chen, Q.; Sang, F.; Fan, D.; Su, L.; Zhang, Z.J.; Ai, L.; Chen, Y.J. Spatial Distribution and Hierarchical Clustering of beta-Amyloid and Glucose Metabolism in Alzheimer’s Disease. Front. Aging Neurosci. 2022, 14, 788567. [Google Scholar] [CrossRef]
- Tanner, J.A.; Iaccarino, L.; Edwards, L.; Asken, B.M.; Gorno-Tempini, M.L.; Kramer, J.H.; Pham, J.; Perry, D.C.; Possin, K.; Malpetti, M.; et al. Amyloid, tau and metabolic PET correlates of cognition in early and late-onset Alzheimer’s disease. Brain 2022, 145, 4489–4505. [Google Scholar] [CrossRef]
- Lagarde, J.; Olivieri, P.; Tonietto, M.; Tissot, C.; Rivals, I.; Gervais, P.; Caillé, F.; Moussion, M.; Bottlaender, M.; Sarazin, M. Tau-PET imaging predicts cognitive decline and brain atrophy progression in early Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 2022, 93, 459–467. [Google Scholar] [CrossRef]
- Ding, Y.; Sohn, J.H.; Kawczynski, M.G.; Trivedi, H.; Harnish, R.; Jenkins, N.W.; Lituiev, D.; Copeland, T.P.; Aboian, M.S.; Aparici, C.M.; et al. A Deep Learning Model to Predict a Diagnosis of Alzheimer Disease by Using 18F-FDG PET of the Brain. Radiology 2019, 290, 456–464. [Google Scholar] [CrossRef]
- Hwang, S.J.; Tao, Z.; Singh, V.; Kim, W.H. Onditional recurrent flow: Conditional generation of longitudinal samples with applications to neuroimaging. In Proceedings of the IEEE International Conference on Computer Vision, Seoul, Republic of Korea, 27–28 October 2019. [Google Scholar] [CrossRef]
- Son, H.J.; Oh, J.S.; Oh, M.; Kim, S.J.; Lee, J.-H.; Roh, J.H.; Kim, J.S. The clinical feasibility of deep learning-based classification of amyloid PET images in visually equivocal cases. Eur. J. Nucl. Med. 2019, 47, 332–341. [Google Scholar] [CrossRef]
- Palmer, W.C.; Park, S.M.; Levendovszky, S.R. Brain state transition analysis using ultra-fast fMRI differentiates MCI from cognitively normal controls. Front. Neurosci. 2022, 16, 1531. [Google Scholar] [CrossRef]
- Tondelli, M.; Benuzzi, F.; Ballotta, D.; Molinari, M.A.; Chiari, A.; Zamboni, G. Eliciting Implicit Awareness in Alzheimer’s Disease and Mild Cognitive Impairment: A Task-Based Functional MRI Study. Front. Aging Neurosci. 2022, 14, 816648. [Google Scholar] [CrossRef] [PubMed]
- Han, X.-M.; Gu, X.-Q.; Liu, Y.; Gu, J.-B.; Li, L.-F.; Fu, L.-L. Correlations between hippocampal functional connectivity, structural changes, and clinical data in patients with relapsing-remitting multiple sclerosis: A case-control study using multimodal magnetic resonance imaging. Neural Regen. Res. 2022, 17, 1115. [Google Scholar] [CrossRef] [PubMed]
- Miao, D.W.; Zhou, X.G.; Wu, X.Y.; Chen, C.D.; Tian, L. Distinct profiles of functional connectivity density aberrance in Alzheimer’s disease and mild cognitive impairment. Front. Psychiatry 2022, 13, 1079149. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Agboola, F.; Grant, E.; Morris, J.C.; Masters, C.L.; Albert, M.S.; Johnson, S.C.; McDade, E.M.; Fagan, A.M.; Benzinger, T.L.S.; et al. Accelerated longitudinal changes and ordering of Alzheimer disease biomarkers across the adult lifespan. Brain 2022, 145, 4459–4473. [Google Scholar] [CrossRef] [PubMed]
- Sarraf, S.; Desouza, D.D.; Anderson, J.A.E.; Saverino, C. MCADNNet: Recognizing Stages of Cognitive Impairment Through Efficient Convolutional fMRI and MRI Neural Network Topology Models. IEEE Access 2019, 7, 155584–155600. [Google Scholar] [CrossRef]
- Wang, Z.; Xin, J.; Wang, Z.; Gu, H.; Zhao, Y.; Qian, W. Computer-Aided Dementia Diagnosis Based on Hierarchical Extreme Learning Machine. Cogn. Comput. 2020, 13, 34–48. [Google Scholar] [CrossRef]
- Bi, X.; Zhao, X.; Huang, H.; Chen, D.; Ma, Y. Functional Brain Network Classification for Alzheimer’s Disease Detection with Deep Features and Extreme Learning Machine. Cogn. Comput. 2019, 12, 513–527. [Google Scholar] [CrossRef]
- Jie, B.; Liu, M.; Lian, C.; Shi, F.; Shen, D. Designing weighted correlation kernels in convolutional neural networks for functional connectivity based brain disease diagnosis. Med. Image Anal. 2020, 63, 101709. [Google Scholar] [CrossRef]
- Cui, R.; Liu, M. Hippocampus Analysis by Combination of 3-D DenseNet and Shapes for Alzheimer’s Disease Diagnosis. IEEE J. Biomed. Health Inform. 2018, 23, 2099–2107. [Google Scholar] [CrossRef]
- Jung, W.; Mulyadi, A.; Suk, H.-I. Unified modeling of imputation, forecasting, and prediction for ad progression. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Aderghal, K.; Benois-Pineau, J.; Afdel, K. Classification of sMRI for Alzheimer’s disease Diagnosis with CNN: Single Siamese Networks with 2D+? Approach and Fusion on ADNI. In Proceedings of the 2017 ACM on International Conference on Multimedia Retrieval, Bucharest, Romania, 6–9 June 2017. [Google Scholar]
- Huang, H.; Zheng, S.; Yang, Z.; Wu, Y.; Li, Y.; Qiu, J.; Cheng, Y.; Lin, P.; Guan, J.; Mikulis, D.J.; et al. Voxel-based morphometry and a deep learning model for the diagnosis of early Alzheimer’s disease based on cerebral gray matter changes. Cereb. Cortex 2022, 33, 754–763. [Google Scholar] [CrossRef]
- Liu, M.; Zhang, J.; Adeli, E.; Shen, D. Joint classification and regression via deep multi-task multi-channel learning for Alzheimer’s disease diagnosis. IEEE Trans. Biomed. Eng. 2018, 66, 1195–1206. [Google Scholar] [CrossRef]
- Lian, C.; Liu, M.; Zhang, J.; Shen, D. Hierarchical fully convolutional network for joint atrophy localization and Alzheimer’s Disease diagnosis using structural MRI. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 42, 880–893. [Google Scholar] [CrossRef]
- Kabani, N.J.; MacDonald, D.J.; Holmes, C.J.; Evans, A.C. 3D Anatomical Atlas of the Human Brain. Neuroimage 1998, 7, S717. [Google Scholar] [CrossRef]
- Sydnor, V.J.; Cieslak, M.; Duprat, R.; Deluisi, J.; Flounders, M.W.; Long, H.; Scully, M.; Balderston, N.L.; Sheline, Y.I.; Bassett, D.S.; et al. Cortical-subcortical structural connections support transcranial magnetic stimulation engagement of the amygdala. Sci. Adv. 2022, 8, eabn5803. [Google Scholar] [CrossRef]
- Du, Y.; Yang, W.; Zhang, J.; Liu, J. Changes in ALFF and ReHo values in methamphetamine abstinent individuals based on the Harvard-Oxford atlas: A longitudinal resting-state fMRI study. Addict. Biol. 2021, 27, e13080. [Google Scholar] [CrossRef]
- Sengupta, D.; Gupta, P.; Biswas, A. A survey on mutual information based medical image registration algorithms. Neurocomputing 2021, 486, 174–188. [Google Scholar] [CrossRef]
- Shen, D.; Davatzikos, C. HAMMER: Hierarchical attribute matching mechanism for elastic registration. IEEE Trans. Med. Imaging 2002, 21, 1421–1439. [Google Scholar] [CrossRef]
- Liu, S.; Liu, S.; Cai, W.; Pujol, S.; Kikinis, R.; Feng, D. Early diagnosis of Alzheimer’s disease with deep learning. In Proceedings of the 2014 IEEE 11th International Symposium on Biomedical Imaging (ISBI), Beijing, China, 29 April–2 May 2014. [Google Scholar]
- Li, T.; Hoogman, M.; Mota, N.R.; Buitelaar, J.K.; Vasquez, A.A.; Franke, B.; Rooij, D.; The ENIGMA-ASD Working Group. Dissecting the heterogeneous subcortical brain volume of autism spectrum disorder using community detection. Autism Res. 2021, 15, 42–55. [Google Scholar] [CrossRef]
- Song, H.; Bharadwaj, P.K.; Raichlen, D.A.; Habeck, C.G.; Huentelman, M.J.; Hishaw, G.A.; Trouard, T.P.; Alexander, G.E. Association of homocysteine-related subcortical brain atrophy with white matter lesion volume and cognition in healthy aging. Neurobiol. Aging 2023, 121, 129–138. [Google Scholar] [CrossRef]
- Chen, W.; Li, H.; Hou, X.; Jia, X. Gray matter alteration in medication overuse headache: A coordinates-based activation likelihood estimation meta-analysis. Brain Imaging Behav. 2022, 16, 2307–2319. [Google Scholar] [CrossRef]
- Vercellino, M.; Marasciulo, S.; Grifoni, S.; Vallino-Costassa, E.; Bosa, C.; Pasanisi, M.B.; Crociara, P.; Casalone, C.; Chio, A.; Giordana, M.T.; et al. Acute and chronic synaptic pathology in multiple sclerosis gray matter. Mult. Scler. J. 2022, 28, 369–382. [Google Scholar] [CrossRef] [PubMed]
- White, M.F.; Tanabe, S.; Casey, C.; Parker, M.; Bo, A.; Kunkel, D.; Nair, V.; Pearce, R.A.; Lennertz, R.; Prabhakaran, V.; et al. Relationships between preoperative cortical thickness, postoperative electroencephalogram slowing, and postoperative delirium. Br. J. Anaesth. 2021, 127, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Demirci, N.; Holland, M.A. Cortical thickness systematically varies with curvature and depth in healthy human brains. Hum. Brain Mapp. 2022, 43, 2064–2084. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Sheng, C.; Chen, G.; Liu, C.; Jin, S.; Li, L.; Jiang, X.; Han, Y.; Weiner, M.W.; Aisen, P.; et al. Glucose metabolism patterns: A potential index to characterize brain ageing and predict high conversion risk into cognitive impairment. Geroscience 2022, 44, 2319–2336. [Google Scholar] [CrossRef]
- Choi, J.H.; Kim, M.-S. Homeostatic Regulation of Glucose Metabolism by the Central Nervous System. Endocrinol. Metab. 2022, 37, 9–25. [Google Scholar] [CrossRef]
- Rabin, J.S.; Nichols, E.; La Joie, R.; Casaletto, K.B.; Palta, P.; Dams-O’connor, K.; Kumar, R.G.; George, K.M.; Satizabal, C.L.; Schneider, J.A.; et al. Cerebral amyloid angiopathy interacts with neuritic amyloid plaques to promote tau and cognitive decline. Brain 2022, 145, 2823–2833. [Google Scholar] [CrossRef]
- Saito, S.; Yamashiro, T.; Yamauchi, M.; Yamamoto, Y.; Noguchi, M.; Tomita, T.; Kawakami, D.; Shikata, M.; Tanaka, T.; Ihara, M. Complement 3 Is a Potential Biomarker for Cerebral Amyloid Angiopathy. J. Alzheimer’s Dis. 2022, 89, 381–387. [Google Scholar] [CrossRef]
- Wang, M.; Cui, B.; Shan, Y.; Yang, H.; Yan, Z.; Sundar, L.K.S.; Alberts, I.; Rominger, A.; Wendler, T.; Shi, K.; et al. Non-Invasive Glucose Metabolism Quantification Method Based on Unilateral ICA Image Derived Input Function by Hybrid PET/MR in Ischemic Cerebrovascular Disease. IEEE J. Biomed. Health Inform. 2022, 26, 5122–5129. [Google Scholar] [CrossRef]
- Liu, J.; Wang, J.; Tang, Z.; Hu, B.; Wu, F.-X.; Pan, Y. Improving Alzheimer’s disease classification by combining multiple measures. IEEE/ACM Trans. Comput. Biol. Bioinform. 2017, 15, 1649–1659. [Google Scholar] [CrossRef]
- Messina, D.; Borrelli, P.; Russo, P.; Salvatore, M.; Aiello, M. Voxel-Wise Feature Selection Method for CNN Binary Classification of Neuroimaging Data. Front. Neurosci. 2021, 15, 630747. [Google Scholar] [CrossRef]
- Gerber, S.; Niethammer, M.; Ebrahim, E.; Piven, J.; Dager, S.R.; Styner, M.; Aylward, S.; Enquobahrie, A. Optimal transport features for morphometric population analysis. Med. Image Anal. 2023, 84, 102696. [Google Scholar] [CrossRef]
- Wu, S.; Zhao, W.; Ji, S. Real-time dynamic simulation for highly accurate spatiotemporal brain deformation from impact. Comput. Methods Appl. Mech. Eng. 2022, 394, 114913. [Google Scholar] [CrossRef]
- Bao, Z.; Zhang, T.; Pan, T.; Zhang, W.; Zhao, S.; Liu, H.; Nie, B. Automatic method for individual parcellation of manganese-enhanced magnetic resonance imaging of rat brain. Front. Neurosci. 2022, 16, 954237. [Google Scholar] [CrossRef]
- Zhang, X.; Feng, Y.; Chen, W.; Li, X.; Faria, A.V.; Feng, Q.; Mori, S. Linear Registration of Brain MRI Using Knowledge-Based Multiple Intermediator Libraries. Front. Neurosci. 2019, 13, 909. [Google Scholar] [CrossRef]
- Dadar, M.; Manera, A.L.; Fonov, V.S.; Ducharme, S.; Collins, D.L. MNI-FTD templates, unbiased average templates of frontotemporal dementia variants. Sci. Data 2021, 8, 222. [Google Scholar] [CrossRef]
- Giraldo, D.L.; Smith, R.E.; Struyfs, H.; Niemantsverdriet, E.; De Roeck, E.; Bjerke, M.; Engelborghs, S.; Romero, E.; Sijbers, J.; Jeurissen, B. Investigating Tissue-Specific Abnormalities in Alzheimer’s Disease with Multi-Shell Diffusion MRI. J. Alzheimer’s Dis. 2022, 90, 1771–1791. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, Y.; Zhang, Q.; Yuan, F. Multi-Modality Reconstruction Attention and Difference Enhancement Network for Brain MRI Image Segmentation. IEEE Access 2022, 10, 31058–31069. [Google Scholar] [CrossRef]
- Jones, D.; Lowe, V.; Graff-Radford, J.; Botha, H.; Barnard, L.; Wiepert, D.; Murphy, M.C.; Murray, M.; Senjem, M.; Gunter, J.; et al. A computational model of neurodegeneration in Alzheimer’s disease. Nat. Commun. 2022, 13, 1643. [Google Scholar] [CrossRef]
- Wang, Z.; Albarghouthi, A.; Prakriya, G.; Jha, S. Interval universal approximation for neural networks. Proc. ACM Program. Lang. 2022, 6, 1–29. [Google Scholar] [CrossRef]
- Pham, V.T.; Jang, Y.; Park, J.W.; Kim, D.J.; Kim, S.E. Cable damage identification of cable-stayed bridge using multi-layer perceptron and graph neural network. Steel Compos. Struct. 2022, 44, 227–240. [Google Scholar]
- Rosenblatt, F. The perceptron: A probabilistic model for information storage and organization in the brain. Psychol. Rev. 1958, 65, 386–408. [Google Scholar] [CrossRef] [PubMed]
- Sabharwal, T.; Gupta, R. Deep facial recognition after medical alterations. Multimed. Tools Appl. 2022, 81, 25675–25706. [Google Scholar] [CrossRef]
- Fattah, E.A.; Van Niekerk, J.; Rue, H. Smart Gradient—An adaptive technique for improving gradient estimation. Found. Data Sci. 2022, 4, 123. [Google Scholar] [CrossRef]
- Ojha, V.; Nicosia, G. Backpropagation Neural Tree. Neural Netw. 2022, 149, 66–83. [Google Scholar] [CrossRef] [PubMed]
- Rumelhart, D.E.; Hinton, G.E.; Williams, R.J. Learning representations by back-propagating errors. Nature 1986, 323, 533–536. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A.; Bengio, Y. Deep Learning; MIT Press Cambridge: Cambridge, MA, USA, 2016; Volume 1. [Google Scholar]
- Liu, X.; Faes, L.; Kale, A.U.; Wagner, S.K.; Fu, D.J.; Bruynseels, A.; Mahendiran, T.; Moraes, G.; Shamdas, M.; Kern, C.; et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: A systematic review and meta-analysis. Lancet Digit. Health 2019, 1, e271–e297. [Google Scholar] [CrossRef]
- Dolph, C.V.; Alam, M.; Shboul, Z.; Samad, M.D.; Iftekharuddin, K.M. Deep learning of texture and structural features for multiclass Alzheimer’s disease classification. In Proceedings of the 2017 International Joint Conference on Neural Networks (IJCNN), Anchorage, AK, USA, 14–19 May 2017. [Google Scholar]
- Liu, S.; Liu, S.; Cai, W.; Che, H.; Pujol, S.; Kikinis, R.; Feng, D.; Fulham, M.J. Multimodal neuroimaging feature learning for multiclass diagnosis of Alzheimer’s disease. IEEE Trans. Biomed. Eng. 2014, 62, 1132–1140. [Google Scholar] [CrossRef]
- Kobayashi, T. Optimistic reinforcement learning by forward Kullback–Leibler divergence optimization. Neural Netw. 2022, 152, 169–180. [Google Scholar] [CrossRef]
- Ji, S.; Zhang, Z.; Ying, S.; Wang, L.; Zhao, X.; Gao, Y. Kullback–Leibler Divergence Metric Learning. IEEE Trans. Cybern. 2020, 52, 2047–2058. [Google Scholar] [CrossRef]
- Nair, V.; Hinton, G. 3D object recognition with deep belief nets. In Proceedings of the Advances in Neural Information Processing Systems, NIPS 2009, Vancouver, BC, Canada, 7–10 December 2009. [Google Scholar]
- Ju, R.; Hu, C.; Li, Q. Early diagnosis of Alzheimer’s disease based on resting-state brain networks and deep learning. IEEE/ACM Trans. Comput. Biol. Bioinform. 2017, 16, 244–257. [Google Scholar] [CrossRef]
- Ithapu, V.K.; Singh, V.; Okonkwo, O.C.; Chappell, R.J.; Dowling, N.M.; Johnson, S.C.; Initiative, A.D.N. Imaging-based enrichment criteria using deep learning algorithms for efficient clinical trials in mild cognitive impairment. Alzheimer’s Dement. 2015, 11, 1489–1499. [Google Scholar] [CrossRef]
- Bhatkoti, P.; Paul, M. Early diagnosis of Alzheimer’s disease: A multi-class deep learning framework with modified k-sparse autoencoder classification. In Proceedings of the 2016 International Conference on Image and Vision Computing New Zealand (IVCNZ), Palmerston North, New Zealand, 21–22 November 2016. [Google Scholar]
- Oh, K.; Chung, Y.-C.; Kim, K.W.; Kim, W.-S.; Oh, I.-S. Classification and Visualization of Alzheimer’s Disease using Volumetric Convolutional Neural Network and Transfer Learning. Sci. Rep. 2019, 9, 1–16. [Google Scholar] [CrossRef]
- Hosseini-Asl, E.; Keynton, R.; El-Baz, A. Alzheimer’s disease diagnostics by adaptation of 3D convolutional network. In Proceedings of the 2016 IEEE International Conference on Image Processing (ICIP), Phoenix, AZ, USA, 25–28 September 2016. [Google Scholar]
- Er, F.; Goularas, D. Predicting the Prognosis of MCI Patients Using Longitudinal MRI Data. IEEE/ACM Trans. Comput. Biol. Bioinform. 2020, 18, 1164–1173. [Google Scholar] [CrossRef]
- Suk, H.-I.; Initiative, T.A.D.N.; Lee, S.-W.; Shen, D. Latent feature representation with stacked auto-encoder for AD/MCI diagnosis. Anat. Embryol. 2013, 220, 841–859. [Google Scholar] [CrossRef]
- Shakeri, M.; Lombaert, H.; Tripathi, S.; Kadoury, S. Deep spectral-based shape features for Alzheimer’s disease classification. In Proceedings of the International Workshop on Spectral and Shape Analysis in Medical Imaging, Athens, Greece, 21 October 2016; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Jiao, Z.; Ji, Y.; Gao, P.; Wang, S.-H. Extraction and analysis of brain functional statuses for early mild cognitive impairment using variational auto-encoder. J. Ambient Intell. Humaniz. Comput. 2020, 14, 5439–5450. [Google Scholar] [CrossRef]
- Basu, S. Early prediction of alzheimer’s disease progression using variational autoencoders. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Biffi, C.; Cerrolaza, J.J.; Tarroni, G.; Bai, W.; de Marvao, A.; Oktay, O.; Ledig, C.; Le Folgoc, L.; Kamnitsas, K.; Doumou, G.; et al. Explainable Anatomical Shape Analysis Through Deep Hierarchical Generative Models. IEEE Trans. Med. Imaging 2020, 39, 2088–2099. [Google Scholar] [CrossRef]
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. Adv. Neural Inf. Process. Syst. 2014, 27, 2672–2680. [Google Scholar]
- Yi, X.; Walia, E.; Babyn, P. Generative adversarial network in medical imaging: A review. Med. Image Anal. 2019, 58, 101552. [Google Scholar] [CrossRef]
- Islam, J.; Zhang, Y. GAN-based synthetic brain PET image generation. Brain Inform. 2020, 7, 1–12. [Google Scholar] [CrossRef]
- Liu, Y.; Pan, Y.; Yang, W.; Ning, Z.; Yue, L.; Liu, M.; Shen, D. Joint Neuroimage Synthesis and Representation Learning for Conversion Prediction of Subjective Cognitive Decline. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Virtual, 4–6 October 2020; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Roychowdhury, S.; Roychowdhury, S. A Modular Framework to Predict Alzheimer’s Disease Progression Using Conditional Generative Adversarial Networks. In Proceedings of the 2020 International Joint Conference on Neural Networks (IJCNN), Glasgow, UK, 19–24 July 2020. [Google Scholar]
- Baumgartner, C.F.; Koch, L.M.; Tezcan, K.C.; Ang, J.X.; Konukoglu, E. Visual feature attribution using wasserstein gans. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018. [Google Scholar]
- Kim, H.W.; Lee, H.E.; Lee, S.; Oh, K.T.; Yun, M.; Yoo, S.K. Slice-selective learning for Alzheimer’s disease classification using a generative adversarial network: A feasibility study of external validation. Eur. J. Nucl. Med. 2020, 47, 2197–2206. [Google Scholar] [CrossRef]
- Rachmadi, M.F.; Valdés-Hernández, M.d.C.; Makin, S.; Wardlaw, J.; Komura, T. Automatic spatial estimation of white matter hyperintensities evolution in brain MRI using disease evolution predictor deep neural networks. Med. Image Anal. 2020, 63, 101712. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Mehta, R.; Zhou, H.; Huang, Z.; Johnson, S.; Prabhakaran, V.; Singh, V. Dual-glow: Conditional flow-based generative model for modality transfer. In Proceedings of the IEEE International Conference on Computer Vision, Seoul, Republic of Korea, 27 October–2 November 2019. [Google Scholar] [CrossRef]
- Li, F.; Tran, L.; Thung, K.-H.; Ji, S.; Shen, D.; Li, J. A Robust Deep Model for Improved Classification of AD/MCI Patients. IEEE J. Biomed. Health Inform. 2015, 19, 1610–1616. [Google Scholar] [CrossRef] [PubMed]
- Suk, H.-I.; Wee, C.-Y.; Lee, S.-W.; Shen, D. State-space model with deep learning for functional dynamics estimation in resting-state fMRI. Neuroimage 2016, 129, 292–307. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.K.; Smith, A.M.; Walsh, J.R. Machine learning for comprehensive forecasting of Alzheimer’s Disease progression. Sci. Rep. 2019, 9, 13622. [Google Scholar] [CrossRef] [PubMed]
- Razavi, F.; Tarokh, M.J.; Alborzi, M. An intelligent Alzheimer’s disease diagnosis method using unsupervised feature learning. J. Big Data 2019, 6, 32. [Google Scholar] [CrossRef]
- Baumgartner, C.F.; Koch, L.M.; Can Tezcan, K.; Xi Ang, J.; Konukoglu, E. Computer aided Alzheimer’s disease diagnosis by an unsupervised deep learning technology. Neurocomputing 2020, 392, 296–304. [Google Scholar]
- Majumdar, A.; Singhal, V. Noisy deep dictionary learning: Application to Alzheimer’s Disease classification. In Proceedings of the 2017 International Joint Conference on Neural Networks (IJCNN), Anchorage, AK, USA, 14–19 May 2017. [Google Scholar]
- Cheng, J.; Dalca, A.V.; Fischl, B.; Zöllei, L. Cortical surface registration using unsupervised learning. arXiv 2020, arXiv:2004.04617. [Google Scholar] [CrossRef]
- Imen, W.; Amna, M.; Fatma, B.; Ezahra, S.F.; Masmoudi, N. Fast HEVC intra-CU decision partition algorithm with modified LeNet-5 and AlexNet. Signal Image Video Process. 2022, 16, 1811–1819. [Google Scholar] [CrossRef]
- Lu, S.; Wang, S.-H.; Zhang, Y.-D. Detection of abnormal brain in MRI via improved AlexNet and ELM optimized by chaotic bat algorithm. Neural Comput. Appl. 2021, 33, 10799–10811. [Google Scholar] [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Soffer, S.; Ben-Cohen, A.; Shimon, O.; Amitai, M.M.; Greenspan, H.; Klang, E. Convolutional Neural Networks for Radiologic Images: A Radiologist’s Guide. Radiology 2019, 290, 590–606. [Google Scholar] [CrossRef]
- Wang, S.-H.; Phillips, P.; Sui, Y.; Liu, B.; Yang, M.; Cheng, H. Classification of Alzheimer’s Disease Based on Eight-Layer Convolutional Neural Network with Leaky Rectified Linear Unit and Max Pooling. J. Med. Syst. 2018, 42, 85. [Google Scholar] [CrossRef]
- Oseledets, I.V. Tensor-train decomposition. SIAM J. Sci. Comput. 2011, 33, 2295–2317. [Google Scholar] [CrossRef]
- Tang, Z.; Chuang, K.V.; DeCarli, C.; Jin, L.-W.; Beckett, L.; Keiser, M.J.; Dugger, B.N. Interpretable classification of Alzheimer’s disease pathologies with a convolutional neural network pipeline. Nat. Commun. 2019, 10, 2173. [Google Scholar] [CrossRef]
- Choi, H.-S.; Choe, J.Y.; Kim, H.; Han, J.W.; Chi, Y.K.; Kim, K.; Hong, J.; Kim, T.; Kim, T.H.; Yoon, S.; et al. Deep learning based low-cost high-accuracy diagnostic framework for dementia using comprehensive neuropsychological assessment profiles. BMC Geriatr. 2018, 18, 234. [Google Scholar] [CrossRef]
- Ieracitano, C.; Mammone, N.; Hussain, A.; Morabito, F.C. A Convolutional Neural Network based self-learning approach for classifying neurodegenerative states from EEG signals in dementia. In Proceedings of the 2020 International Joint Conference on Neural Networks (IJCNN), Glasgow, UK, 19–24 July 2020. [Google Scholar]
- Pan, X.; Phan, T.-L.; Adel, M.; Fossati, C.; Gaidon, T.; Wojak, J.; Guedj, E. Multi-View Separable Pyramid Network for AD Prediction at MCI Stage by 18F-FDG Brain PET Imaging. IEEE Trans. Med. Imaging 2020, 40, 81–92. [Google Scholar] [CrossRef]
- Alavi, A.; Ruffalo, M.; Parvangada, A.; Huang, Z.; Bar-Joseph, Z. A web server for comparative analysis of single-cell RNA-seq data. Nat. Commun. 2018, 9, 4768. [Google Scholar] [CrossRef]
- Islam, J.; Zhang, Y. Understanding 3D CNN Behavior for Alzheimer’s Disease Diagnosis from Brain PET Scan. arXiv 2019, arXiv:1912.04563. [Google Scholar]
- Duc, N.T.; Ryu, S.; Qureshi, M.N.I.; Choi, M.; Lee, K.H.; Lee, B. 3D-Deep Learning Based Automatic Diagnosis of Alzheimer’s Disease with Joint MMSE Prediction Using Resting-State fMRI. Neuroinformatics 2019, 18, 71–86. [Google Scholar] [CrossRef]
- Basaia, S.; Agosta, F.; Wagner, L.; Canu, E.; Magnani, G.; Santangelo, R.; Filippi, M. Automated classification of Alzheimer’s disease and mild cognitive impairment using a single MRI and deep neural networks. NeuroImage Clin. 2019, 21, 101645. [Google Scholar] [CrossRef]
- Qiu, S.; Joshi, P.S.; Miller, M.I.; Xue, C.; Zhou, X.; Karjadi, C.; Chang, G.H.; Joshi, A.S.; Dwyer, B.; Zhu, S.; et al. Development and validation of an interpretable deep learning framework for Alzheimer’s disease classification. Brain 2020, 143, 1920–1933. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Initiative, F.T.A.D.N.; Kim, Y.K.; Yoon, E.J.; Lee, J.-Y.; Lee, D.S. Cognitive signature of brain FDG PET based on deep learning: Domain transfer from Alzheimer’s disease to Parkinson’s disease. Eur. J. Nucl. Med. 2019, 47, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Basaia, S.; Agosta, F.; Wagner, L.; Canu, E.; Magnani, G.; Santangelo, R.; Filippi, M. Studying the manifold structure of Alzheimer’s Disease: A deep learning approach using convolutional autoencoders. IEEE J. Biomed. Health Inform. 2019, 24, 17–26. [Google Scholar]
- Payan, A.; Montana, G. Predicting Alzheimer’s disease: A neuroimaging study with 3D convolutional neural networks. arXiv 2015, arXiv:1502.02506. [Google Scholar]
- Ge, C.; Qu, Q.; Gu, I.Y.-H.; Jakola, A.S. Multiscale Deep Convolutional Networks for Characterization and Detection of Alzheimer’s Disease Using MR images. In Proceedings of the 2019 IEEE International Conference on Image Processing (ICIP), Taipei, Taiwan, 22–25 September 2019. [Google Scholar]
- Islam, J.; Zhang, Y. Early Diagnosis of Alzheimer’s Disease: A Neuroimaging Study with Deep Learning Architectures. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops, Salt Lake City, UT, USA, 18–22 June 2018. [Google Scholar]
- Liu, S.; Yadav, C.; Fernandez-Granda, C.; Razavian, N. On the design of convolutional neural networks for automatic detection of Alzheimer’s disease. In Proceedings of the Machine Learning for Health Workshop, Vancouver, BC, Canada, 8–14 December 2020. [Google Scholar]
- Wang, H.; Shen, Y.; Wang, S.; Xiao, T.; Deng, L.; Wang, X.; Zhao, X. Ensemble of 3D densely connected convolutional network for diagnosis of mild cognitive impairment and Alzheimer’s disease. Neurocomputing 2018, 333, 145–156. [Google Scholar] [CrossRef]
- Spasov, S.; Passamonti, L.; Duggento, A.; Liò, P.; Toschi, N. A parameter-efficient deep learning approach to predict conversion from mild cognitive impairment to Alzheimer’s disease. Neuroimage 2019, 189, 276–287. [Google Scholar] [CrossRef]
- Yang, Z.; Zhuang, X.; Mishra, V.; Sreenivasan, K.; Cordes, D. CAST: A multi-scale convolutional neural network based automated hippocampal subfield segmentation toolbox. Neuroimage 2020, 218, 116947. [Google Scholar] [CrossRef]
- Pang, S.; Feng, Q.; Lu, Z.; Jiang, J.; Zhao, L.; Lin, L.; Li, X.; Lian, T.; Huang, M.; Yang, W. Hippocampus Segmentation Based on Iterative Local Linear Mapping with Representative and Local Structure-Preserved Feature Embedding. IEEE Trans. Med. Imaging 2019, 38, 2271–2280. [Google Scholar] [CrossRef]
- Li, J.; Rong, Y.; Meng, H.; Lu, Z.; Kwok, T.; Cheng, H. Tatc: Predicting Alzheimer’s disease with actigraphy data. In Proceedings of the 24th ACM SIGKDD International Conference on Knowledge Discovery & Data Mining, London, UK, 19–23 August 2018. [Google Scholar]
- Cui, R.; Liu, M.; Li, G. Longitudinal analysis for Alzheimer’s disease diagnosis using RNN. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018. [Google Scholar]
- Feng, C.; Elazab, A.; Yang, P.; Wang, T.; Lei, B.; Xiao, X. 3D convolutional neural network and stacked bidirectional recurrent neural network for Alzheimer’s disease diagnosis. In Proceedings of the International Workshop on PRedictive Intelligence in MEdicine, Granada, Spain, 16 September 2018; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Cheng, D.; Liu, M. Combining convolutional and recurrent neural networks for Alzheimer’s disease diagnosis using PET images. In Proceedings of the 2017 IEEE International Conference on Imaging Systems and Techniques (IST), Beijing, China, 18–20 October 2017. [Google Scholar]
- Xia, Z.; Yue, G.; Xu, Y.; Feng, C.; Yang, M.; Wang, T.; Lei, B. A Novel End-to-End Hybrid Network for Alzheimer’s Disease Detection Using 3D CNN and 3D CLSTM. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020. [Google Scholar]
- Wang, M.; Lian, C.; Yao, D.; Zhang, D.; Liu, M.; Shen, D. Spatial-Temporal Dependency Modeling and Network Hub Detection for Functional MRI Analysis via Convolutional-Recurrent Network. IEEE Trans. Biomed. Eng. 2019, 67, 2241–2252. [Google Scholar] [CrossRef]
- Lee, G.; Nho, K.; Kang, B.; Sohn, K.-A.; Kim, D.; Weiner, M.W.; Aisen, P.; Petersen, R.; Jack, C.R.; Jagust, W.; et al. Predicting Alzheimer’s disease progression using multi-modal deep learning approach. Sci. Rep. 2019, 9, 1952. [Google Scholar] [CrossRef]
- Li, H.; Fan, Y. Early prediction of Alzheimer’s disease dementia based on baseline hippocampal MRI and 1-year follow-up cognitive measures using deep recurrent neural networks. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019. [Google Scholar]
- Nguyen, M.; He, T.; An, L.; Alexander, D.C.; Feng, J.; Yeo, B.T. Predicting Alzheimer’s disease progression using deep recurrent neural networks. NeuroImage 2020, 222, 117203. [Google Scholar] [CrossRef]
- Bronstein, M.M.; Bruna, J.; LeCun, Y.; Szlam, A.; Vandergheynst, P. Geometric Deep Learning: Going beyond Euclidean data. IEEE Signal Process. Mag. 2017, 34, 18–42. [Google Scholar] [CrossRef]
- Ma, X.; Wu, G.; Kim, W.H. Enriching Statistical Inferences on Brain Connectivity for Alzheimer’s Disease Analysis via Latent Space Graph Embedding. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020. [Google Scholar]
- Wu, Z.; Pan, S.; Chen, F.; Long, G.; Zhang, C.; Philip, S.Y. A comprehensive survey on graph neural networks. IEEE Trans. Neural Netw. Learn. Syst. 2020, 32, 4–24. [Google Scholar] [CrossRef]
- Song, T.-A.; Chowdhury, S.R.; Yang, F.; Jacobs, H.; El Fakhri, G.; Li, Q.; Johnson, K.; Dutta, J. Graph Convolutional Neural Networks for Alzheimer’s Disease Classification. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019. [Google Scholar]
- Song, T.-A.; Chowdhury, S.R.; Yang, F.; Jacobs, H.I.L.; Sepulcre, J.; Wedeen, V.J.; Johnson, K.A.; Dutta, J. A Physics-Informed Geometric Learning Model for Pathological Tau Spread in Alzheimer’s Disease. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Song, X.; Frangi, A.; Xiao, X.; Cao, J.; Wang, T.; Lei, B. Integrating similarity awareness and adaptive calibration in graph convolution network to predict disease. In Medical Image Computing and Computer Assisted Intervention–MICCAI 2020: Proceedings of the 23rd International Conference, Lima, Peru, 4–8 October 2020; Proceedings, Part VII 23; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Yang, J.; Zheng, W.-S.; Yang, Q.; Chen, Y.-C.; Tian, Q. Spatial-Temporal Graph Convolutional Network for Video-Based Person Re-Identification. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 13–19 June 2020. [Google Scholar]
- Mirakhorli, J.; Mirakhorli, M. Graph-Based Method for Anomaly Detection in Functional Brain Network using Variational Autoencoder. bioRxiv 2019, 616367. [Google Scholar] [CrossRef]
- Zhu, W.; Razavian, N. Graph Neural Network on Electronic Health Records for Predicting Alzheimer’s Disease. arXiv 2019, arXiv:1912.03761. [Google Scholar]
- Ma, J.; Zhu, X.; Yang, D.; Chen, J.; Wu, G. Attention-Guided Deep Graph Neural Network for Longitudinal Alzheimer’s Disease Analysis. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Bruna, J.; Zaremba, W.; Szlam, A.; LeCun, Y. Spectral networks and locally connected networks on graphs. arXiv 2013, arXiv:1312.6203. [Google Scholar]
- Wee, C.-Y.; Liu, C.; Lee, A.; Poh, J.S.; Ji, H.; Qiu, A. Cortical graph neural network for AD and MCI diagnosis and transfer learning across populations. NeuroImage Clin. 2019, 23, 101929. [Google Scholar] [CrossRef]
- Zhao, X.; Zhou, F.; Ou-Yang, L.; Wang, T.; Lei, B. Graph Convolutional Network Analysis for Mild Cognitive Impairment Prediction. In Proceedings of the 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI 2019), Venice, Italy, 8–11 April 2019. [Google Scholar]
- Kazi, A.; Shekarforoush, S.; Krishna, S.A.; Burwinkel, H.; Vivar, G.; Wiestler, B.; Kortüm, K.; Ahmadi, S.-A.; Albarqouni, S.; Navab, N. Graph convolution based attention model for personalized disease prediction. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention; Shenzhen, China, 13–17 October 2019, Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Huang, Y.; Chung, A.C. Edge-Variational Graph Convolutional Networks for Uncertainty-Aware Disease Prediction. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Yu, S.; Wang, S.; Xiao, X.; Cao, J.; Yue, G.; Liu, D.; Wang, T.; Xu, Y.; Lei, B. Multi-scale Enhanced Graph Convolutional Network for Early Mild Cognitive Impairment Detection. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Chakraborty, R.; Zhen, X.; Vogt, N.; Bendlin, B.; Singh, V. Dilated convolutional neural networks for sequential manifold-valued data. In Proceedings of the IEEE International Conference on Computer Vision, Seoul, Republic of Korea, 27–28 October 2019. [Google Scholar]
- You, Z.; Zeng, R.; Lan, X.; Ren, H.; You, Z.; Shi, X.; Zhao, S.; Guo, Y.; Jiang, X.; Hu, X. Alzheimer’s Disease Classification with a Cascade Neural Network. Front. Public Health 2020, 8, 584387. [Google Scholar] [CrossRef]
- Gadgil, S.; Zhao, Q.; Pfefferbaum, A.; Sullivan, E.V.; Adeli, E.; Pohl, K.M. Spatio-Temporal Graph Convolution for Resting-State fMRI Analysis. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Pfau, D.; Vinyals, O. Connecting generative adversarial networks and actor-critic methods. arXiv 2016, arXiv:1610.01945. [Google Scholar]
- Capecci, E.; Doborjeh, Z.G.; Mammone, N.; La Foresta, F.; Morabito, F.C.; Kasabov, N. Longitudinal study of alzheimer’s disease degeneration through EEG data analysis with a NeuCube spiking neural network model. In Proceedings of the 2016 International Joint Conference on Neural Networks (IJCNN), Vancouver, BC, Canada, 24–29 July 2016. [Google Scholar]
- Suk, H.-I.; Shen, D. Deep learning-based feature representation for AD/MCI classification. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Nagoya, Japan, 22–26 October 2016; Springer: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Suk, H.-I.; Lee, S.-W.; Shen, D. Deep ensemble learning of sparse regression models for brain disease diagnosis. Med. Image Anal. 2017, 37, 101–113. [Google Scholar] [CrossRef]
- Shi, J.; Zheng, X.; Li, Y.; Zhang, Q.; Ying, S. Multimodal neuroimaging feature learning with multimodal stacked deep polynomial networks for diagnosis of Alzheimer’s disease. IEEE J. Biomed. Health Inform. 2017, 22, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.; Popuri, K.; Ding, G.W.; Balachandar, R.; Beg, M.F. Multiscale deep neural network based analysis of FDG-PET images for the early diagnosis of Alzheimer’s disease. Med. Image Anal. 2018, 46, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Ning, K.; Chen, B.; Sun, F.; Hobel, Z.; Zhao, L.; Matloff, W.; Toga, A.W. Classifying Alzheimer’s disease with brain imaging and genetic data using a neural network framework. Neurobiol. Aging 2018, 68, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Choi, J.-S.; Kim, M.; Suk, H.-I. Toward an interpretable Alzheimer’s disease diagnostic model with regional abnormality representation via deep learning. Neuroimage 2019, 202, 116113. [Google Scholar] [CrossRef] [PubMed]
- Bashyam, V.M.; Erus, G.; Doshi, J.; Habes, M.; Nasrallah, I.M.; Truelove-Hill, M.; Srinivasan, D.; Mamourian, L.; Pomponio, R.; Fan, Y.; et al. MRI signatures of brain age and disease over the lifespan based on a deep brain network and 14,468 individuals worldwide. Brain 2020, 143, 2312–2324. [Google Scholar] [CrossRef]
- Lundervold, A.S.; Lundervold, A. An overview of deep learning in medical imaging focusing on MRI. Z. Med. Phys. 2019, 29, 102–127. [Google Scholar] [CrossRef]
- Morid, M.A.; Borjali, A.; Del Fiol, G. A scoping review of transfer learning research on medical image analysis using ImageNet. Comput. Biol. Med. 2020, 128, 104115. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.-J.; Li, K.; Fei-Fei, L. Imagenet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009. [Google Scholar]
- Kam, H.J.; Kim, H.Y. Learning representations for the early detection of sepsis with deep neural networks. Comput. Biol. Med. 2017, 89, 248–255. [Google Scholar] [CrossRef]
- Wang, S.-H.; Zhan, T.-M.; Chen, Y.; Zhang, Y.; Yang, M.; Lu, H.-M.; Wang, H.-N.; Liu, B.; Phillips, P. Multiple Sclerosis Detection Based on Biorthogonal Wavelet Transform, RBF Kernel Principal Component Analysis, and Logistic Regression. IEEE Access 2016, 4, 7567–7576. [Google Scholar] [CrossRef]
- Zhang, X.; Yan, L.-F.; Hu, Y.-C.; Li, G.; Yang, Y.; Han, Y.; Sun, Y.-Z.; Liu, Z.-C.; Tian, Q.; Han, Z.-Y.; et al. Optimizing a machine learning based glioma grading system using multi-parametric MRI histogram and texture features. Oncotarget 2017, 8, 47816–47830. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, S.; Sui, Y.; Yang, M.; Liu, B.; Cheng, H.; Sun, J.; Jia, W.; Phillips, P.; Gorriz, J.M. Multivariate Approach for Alzheimer’s Disease Detection Using Stationary Wavelet Entropy and Predator-Prey Particle Swarm Optimization. J. Alzheimer’s Dis. 2018, 65, 855–869. [Google Scholar] [CrossRef]
- Zhuang, F.; Qi, Z.; Duan, K.; Xi, D.; Zhu, Y.; Zhu, H.; Xiong, H.; He, Q. A Comprehensive Survey on Transfer Learning. Proc. IEEE 2021, 109, 43–76. [Google Scholar] [CrossRef]
- Yosinski, J.; Clune, J.; Bengio, Y.; Lipson, H. How transferable are features in deep neural networks? In Proceedings of the Advances in Neural Information Processing Systems, NIPS 2014, Montréal, QC, Canada, 8–13 December 2014. [Google Scholar]
- Bae, J.B.; Lee, S.; Jung, W.; Park, S.; Kim, W.; Oh, H.; Han, J.W.; Kim, G.E.; Kim, J.S.; Kim, J.H. Identification of Alzheimer’s disease using a convolutional neural network model based on T1-weighted magnetic resonance imaging. Sci. Rep. 2020, 10, 22252. [Google Scholar] [CrossRef]
- Lin, L.; Wu, Y.; Wu, X.; Wu, S. APOE-ε4 allele load modifies the brain aging process in cognitively normal late middle aged and older adults. In Proceedings of the International Conference on Artificial Intelligence, Information Processing and Cloud Computing, Sanya, China, 21–22 June 2019. [Google Scholar]
- Cheng, B.; Initiative, T.A.D.N.; Liu, M.; Shen, D.; Li, Z.; Zhang, D. Multi-Domain Transfer Learning for Early Diagnosis of Alzheimer’s Disease. Neuroinformatics 2016, 15, 115–132. [Google Scholar] [CrossRef]
- Sagi, O.; Rokach, L. Ensemble learning: A survey. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2018, 8, e1249. [Google Scholar] [CrossRef]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Geras, K.J.; Wolfson, S.; Shen, Y.; Wu, N.; Kim, S.; Kim, E.; Heacock, L.; Parikh, U.; Moy, L.; Cho, K. High-resolution breast cancer screening with multi-view deep convolutional neural networks. arXiv 2017, arXiv:1703.07047. [Google Scholar]
- Seeley, M.; Clement, M.; Giraud-Carrier, C.; Snell, Q.; Bodily, P.; Fujimoto, S. A structured approach to ensemble learning for Alzheimer’s disease prediction. In Proceedings of the 5th ACM Conference on Bioinformatics, Computational Biology, and Health Informatics, Newport Beach, CA, USA, 20–23 September 2014. [Google Scholar]
- Zhou, T.; Thung, K.-H.; Liu, M.; Shi, F.; Zhang, C.; Shen, D. Multi-modal latent space inducing ensemble SVM classifier for early dementia diagnosis with neuroimaging data. Med. Image Anal. 2020, 60, 101630. [Google Scholar] [CrossRef]
- Liu, S.; Cai, W.; Liu, S.; Zhang, F.; Fulham, M.; Feng, D.; Pujol, S.; Kikinis, R. Multimodal neuroimaging computing: A review of the applications in neuropsychiatric disorders. Brain Inform. 2015, 2, 167. [Google Scholar] [CrossRef]
- Qiu, S.; Chang, G.H.; Panagia, M.; Gopal, D.M.; Au, R.; Kolachalama, V.B. Fusion of deep learning models of MRI scans, Mini–Mental State Examination, and logical memory test enhances diagnosis of mild cognitive impairment. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2018, 10, 737–749. [Google Scholar] [CrossRef]
- Zheng, X.; Shi, J.; Li, Y.; Liu, X.; Zhang, Q. Multi-modality stacked deep polynomial network based feature learning for Alzheimer’s disease diagnosis. In Proceedings of the 2016 IEEE 13th International Symposium on Biomedical Imaging (ISBI), Prague, Czech Republic, 13–16 April 2016. [Google Scholar]
- Zhou, T.; Thung, K.-H.; Zhu, X.; Shen, D. Effective feature learning and fusion of multimodality data using stage-wise deep neural network for dementia diagnosis. Hum. Brain Mapp. 2018, 40, 1001–1016. [Google Scholar] [CrossRef] [PubMed]
- Saribudak, A.; Subick, A.A.; Kim, N.H.; Rutta, J.A.; Uyar, M.Ü. Gene Expressions, Hippocampal Volume Loss and MMSE Scores in Computation of Progression and Pharmacologic Therapy Effects for Alzheimer’s Disease. IEEE/ACM Trans. Comput. Biol. Bioinform. 2018, 17, 608–622. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Shang, S.; Zheng, K.; Wen, J.-R. Multi-view ensemble learning for dementia diagnosis from neuroimaging: An artificial neural network approach. Neurocomputing 2016, 195, 112–116. [Google Scholar] [CrossRef]
- Lu, D.; Popuri, K.; Ding, G.W.; Balachandar, R.; Beg, M.F.; Weiner, M.; Aisen, P.; Petersen, R.; Jack, C.; Jagust, W.; et al. Multimodal and Multiscale Deep Neural Networks for the Early Diagnosis of Alzheimer’s Disease using structural MR and FDG-PET images. Sci. Rep. 2018, 8, 5697. [Google Scholar] [CrossRef]
- Senanayake, U.; Sowmya, A.; Dawes, L. Deep fusion pipeline for mild cognitive impairment diagnosis. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018. [Google Scholar]
- Moscovich, A.; Rosset, S. On the cross-validation bias due to unsupervised preprocessing. J. R. Stat. Soc. Ser. B Stat. Methodol. 2022, 84, 1474–1502. [Google Scholar] [CrossRef]
- Kenett, R.S.; Gotwalt, C.; Freeman, L.; Deng, X. Self -supervised cross validation using data generation structure. Appl. Stoch. Model. Bus. Ind. 2022, 38, 750–765. [Google Scholar] [CrossRef]
- Nayak, G.; Padhy, N.; Mishra, T.K. 2D-DOST for seizure identification from brain MRI during pregnancy using KRVFL. Health Technol. 2022, 12, 757–764. [Google Scholar] [CrossRef]
- Mila, C.; Mateu, J.; Pebesma, E.; Meyer, H. Nearest neighbour distance matching Leave-One-Out Cross-Validation for map validation. Methods Ecol. Evol. 2022, 13, 1304–1316. [Google Scholar] [CrossRef]
- Wang, B.; Zou, H. Fast and exact leave-one-out analysis of large-margin classifiers. Technometrics 2022, 64, 291–298. [Google Scholar] [CrossRef]
- Kim, J.; Basak, J.M.; Holtzman, D.M. The role of apolipoprotein E in Alzheimer’s disease. Neuron 2009, 63, 287–303. [Google Scholar] [CrossRef]
- Mårtensson, G.; Ferreira, D.; Granberg, T.; Cavallin, L.; Oppedal, K.; Padovani, A.; Rektorova, I.; Bonanni, L.; Pardini, M.; Kramberger, M.G.; et al. The reliability of a deep learning model in clinical out-of-distribution MRI data: A multicohort study. Med. Image Anal. 2020, 66, 101714. [Google Scholar] [CrossRef]
- Li, H.; Habes, M.; Wolk, D.A.; Fan, Y. A deep learning model for early prediction of Alzheimer’s disease dementia based on hippocampal magnetic resonance imaging data. Alzheimer’s Dement. 2019, 15, 1059–1070. [Google Scholar] [CrossRef]
- Delong, E.R.; Delong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Bäckström, K.; Nazari, M.; Gu, I.Y.-H.; Jakola, A.S. An efficient 3D deep convolutional network for Alzheimer’s disease diagnosis using MR images. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018. [Google Scholar]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M. Tensorflow: A system for large-scale machine learning. In Proceedings of the 12th {USENIX} Symposium on Operating Systems Design and Implementation ({OSDI} 16), Savannah, GA, USA, 2–4 November 2016. [Google Scholar]
- Jia, Y.; Shelhamer, E.; Donahue, J.; Karayev, S.; Long, J.; Girshick, R.; Guadarrama, S.; Darrell, T. Caffe: Convolutional architecture for fast feature embedding. In Proceedings of the 22nd ACM International Conference on Multimedia, Orlando, FL, USA, 3–7 November 2014. [Google Scholar]
- Team, T.T.D.; Al-Rfou, R.; Alain, G.; Almahairi, A.; Angermueller, C.; Bahdanau, D.; Ballas, N.; Bastien, F.; Bayer, J.; Belikov, A. Theano: A Python framework for fast computation of mathematical expressions. arXiv 2016, arXiv:1605.02688. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.; Gimelshein, N.; Antiga, L. Pytorch: An imperative style, high-performance deep learning library. In Proceedings of the Advances in Neural Information Processing Systems, NIPS 2019, Vancouver, BC, Canada, 8–14 December 2019. [Google Scholar]
- Nigri, E.; Ziviani, N.; Cappabianco, F.; Antunes, A.; Veloso, A. Explainable Deep CNNs for MRI-Based Diagnosis of Alzheimer’s Disease. arXiv 2020, arXiv:2004.12204. [Google Scholar]
- Lian, C.; Liu, M.; Wang, L.; Shen, D. End-to-end dementia status prediction from brain mri using multi-task weakly-supervised attention network. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Li, Q.; Xing, X.; Sun, Y.; Xiao, B.; Wei, H.; Huo, Q.; Zhang, M.; Zhou, X.S.; Zhan, Y.; Xue, Z.; et al. Novel iterative attention focusing strategy for joint pathology localization and prediction of MCI progression. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Shenzhen, China, 13–17 October 2019; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Hoeffding, W. Probability inequalities for sums of bounded random variables. In The Collected Works of Wassily Hoeffding; Springer: Berlin/Heidelberg, Germany, 1994; pp. 409–426. [Google Scholar]
- Kawaguchi, K.; Kaelbling, L.; Bengio, Y. Generalization in deep learning. arXiv 2017, arXiv:1710.05468. [Google Scholar]
- Jin, P.; Lu, L.; Tang, Y.; Karniadakis, G.E. Quantifying the generalization error in deep learning in terms of data distribution and neural network smoothness. Neural Netw. 2020, 130, 85–99. [Google Scholar] [CrossRef]
- Geirhos, R.; Temme, C.R.; Rauber, J.; Schütt, H.H.; Bethge, M.; Wichmann, F.A. Generalisation in humans and deep neural networks. In Proceedings of the Advances in Neural Information Processing Systems, NIPS 2018, Montréal, QC, Canada, 2–8 December 2018. [Google Scholar]
- Wu, B.; Sun, X.; Hu, L.; Wang, Y. Learning with unsure data for medical image diagnosis. In Proceedings of the IEEE International Conference on Computer Vision, Seoul, Republic of Korea, 27 October–2 November 2019. [Google Scholar]
- Isaacs, J.D.; Boenink, M. Biomarkers for dementia: Too soon for routine clinical use. Lancet Neurol. 2020, 19, 884–885. [Google Scholar] [CrossRef]
- Jack, C.R., Jr.; Wiste, H.J.; Weigand, S.D.; Rocca, W.A.; Knopman, D.S.; Mielke, M.M.; Lowe, V.J.; Senjem, M.L.; Gunter, J.L.; Preboske, G.M. Age-specific population frequencies of cerebral β-amyloidosis and neurodegeneration among people with normal cognitive function aged 50–89 years: A cross-sectional study. Lancet Neurol. 2014, 13, 997–1005. [Google Scholar] [CrossRef]












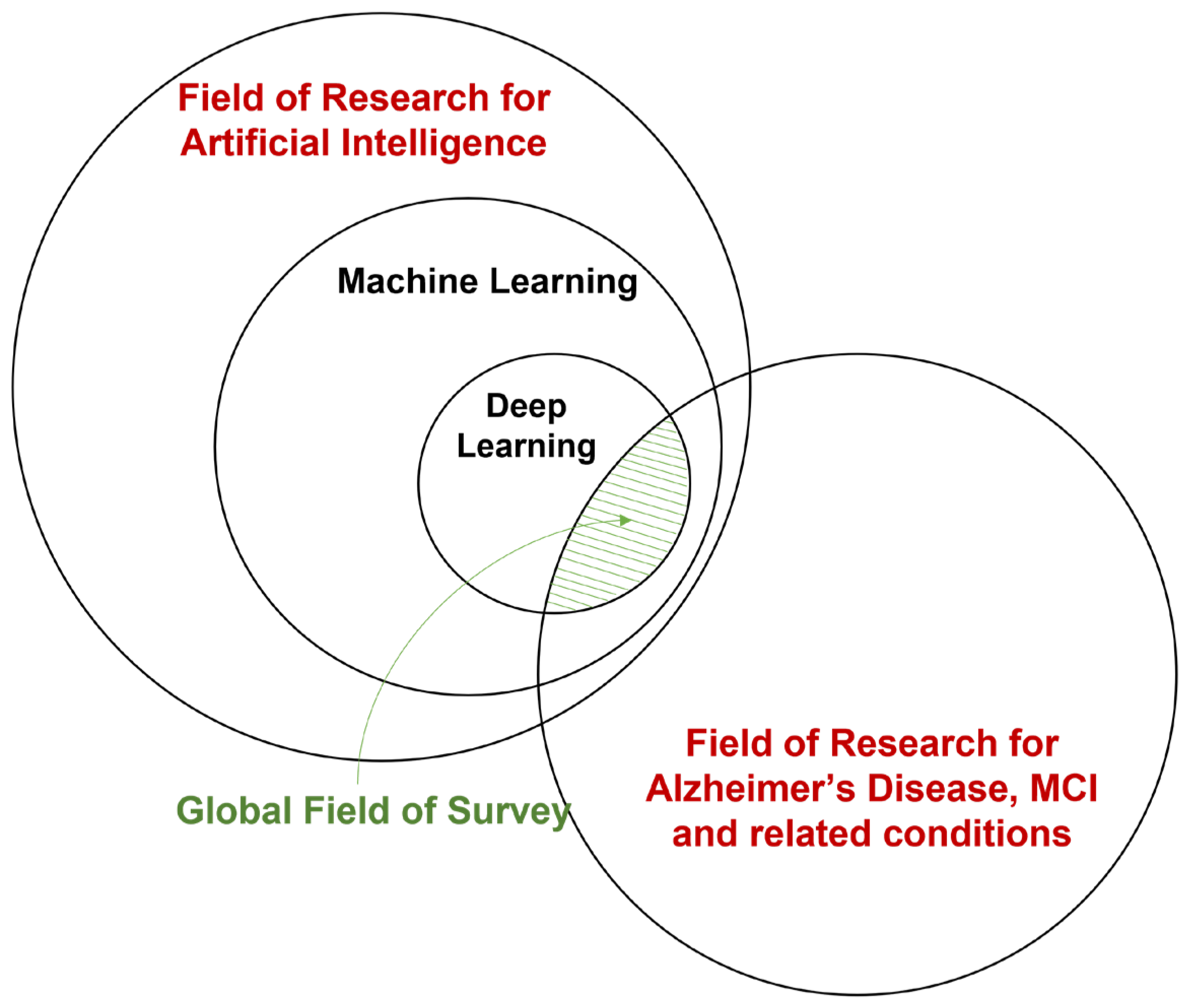{kind=link}
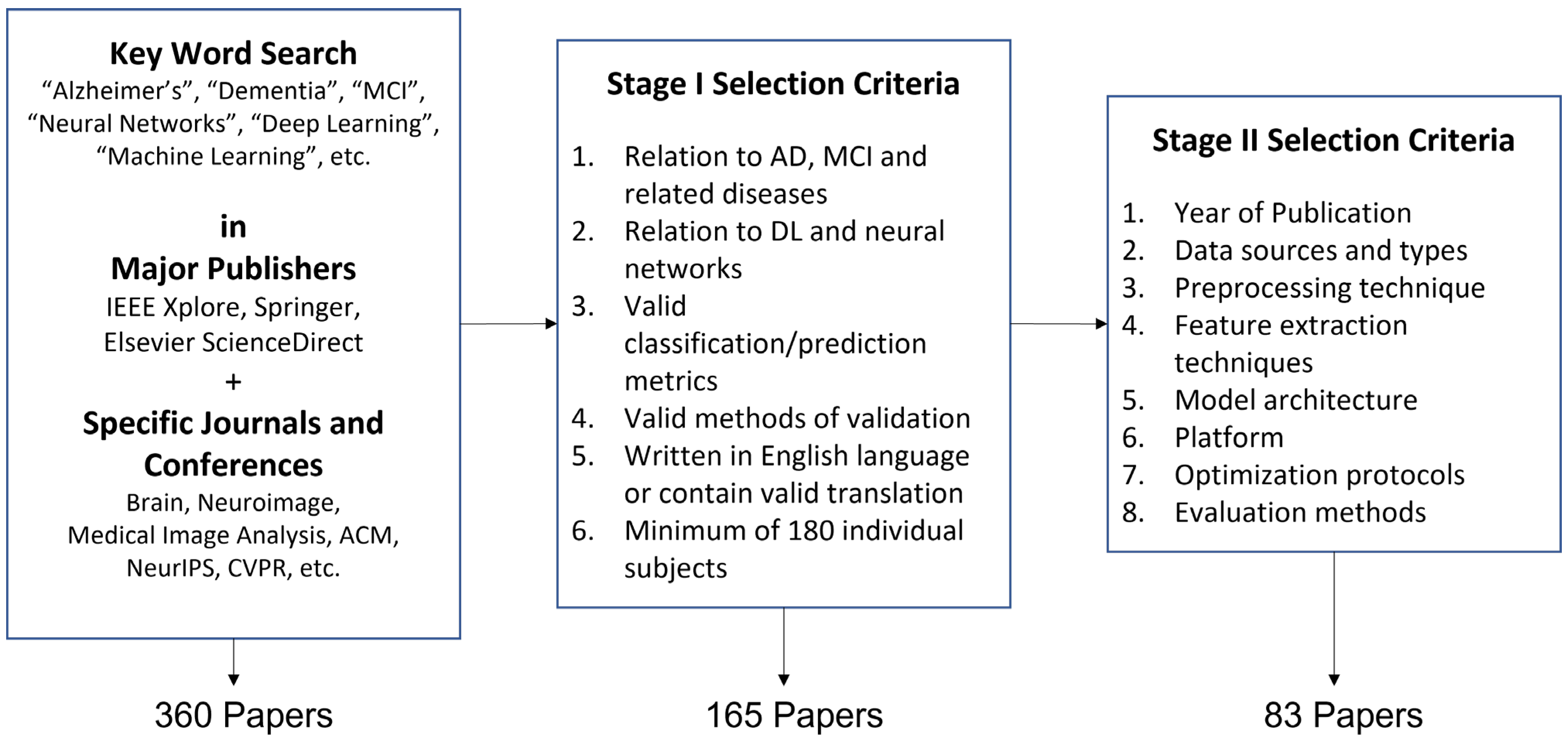{kind=link}
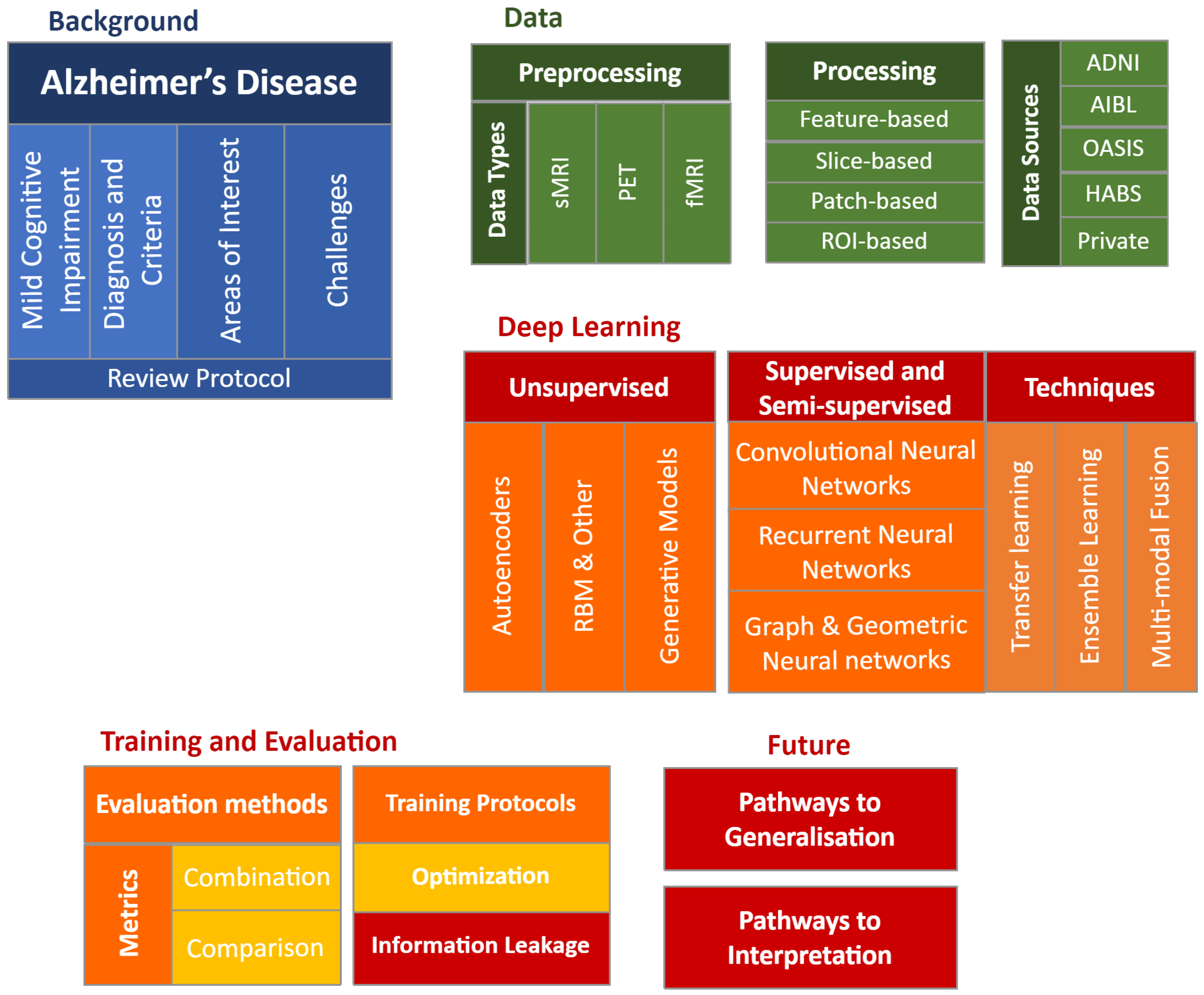{kind=link}
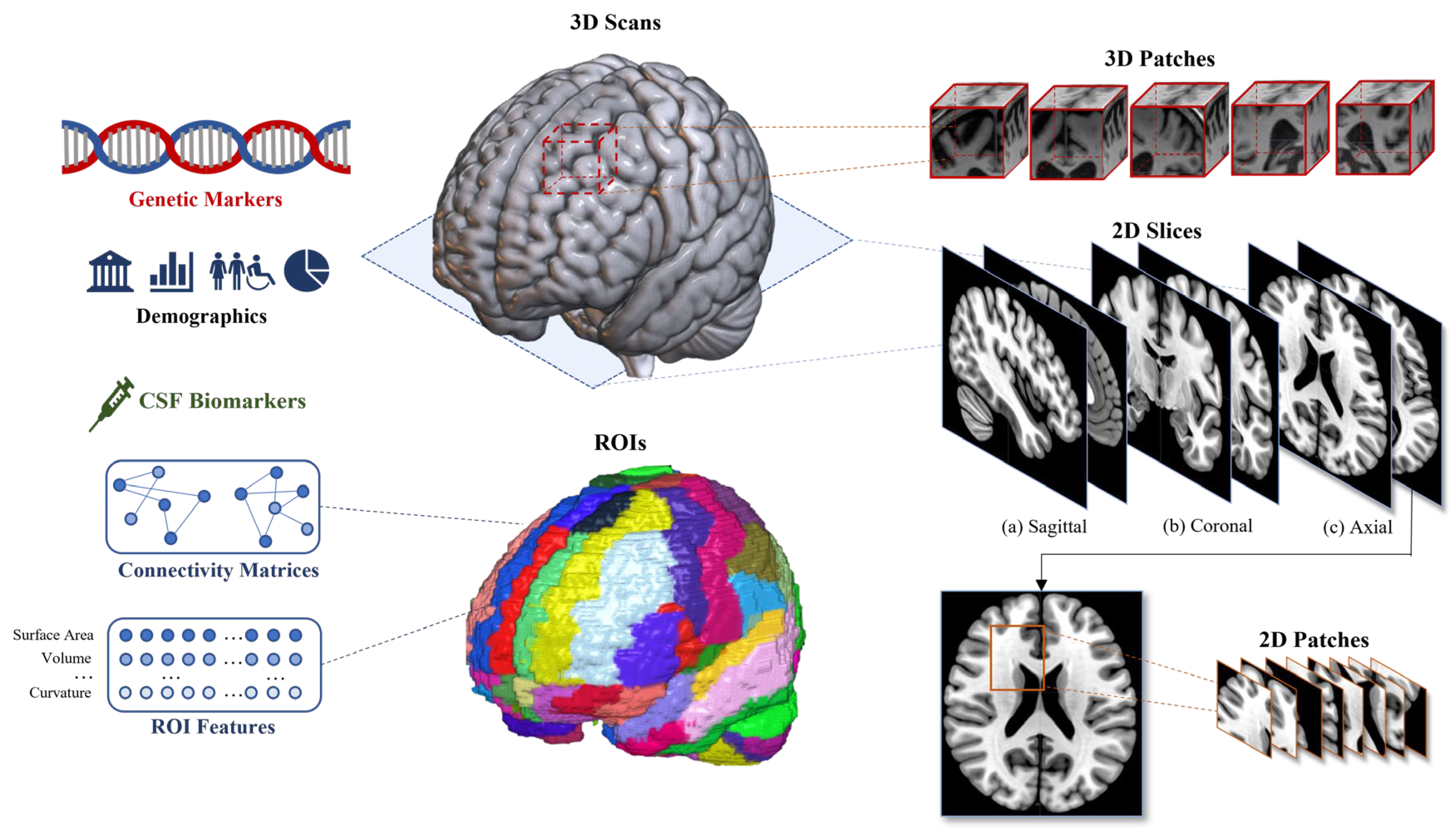{kind=link}
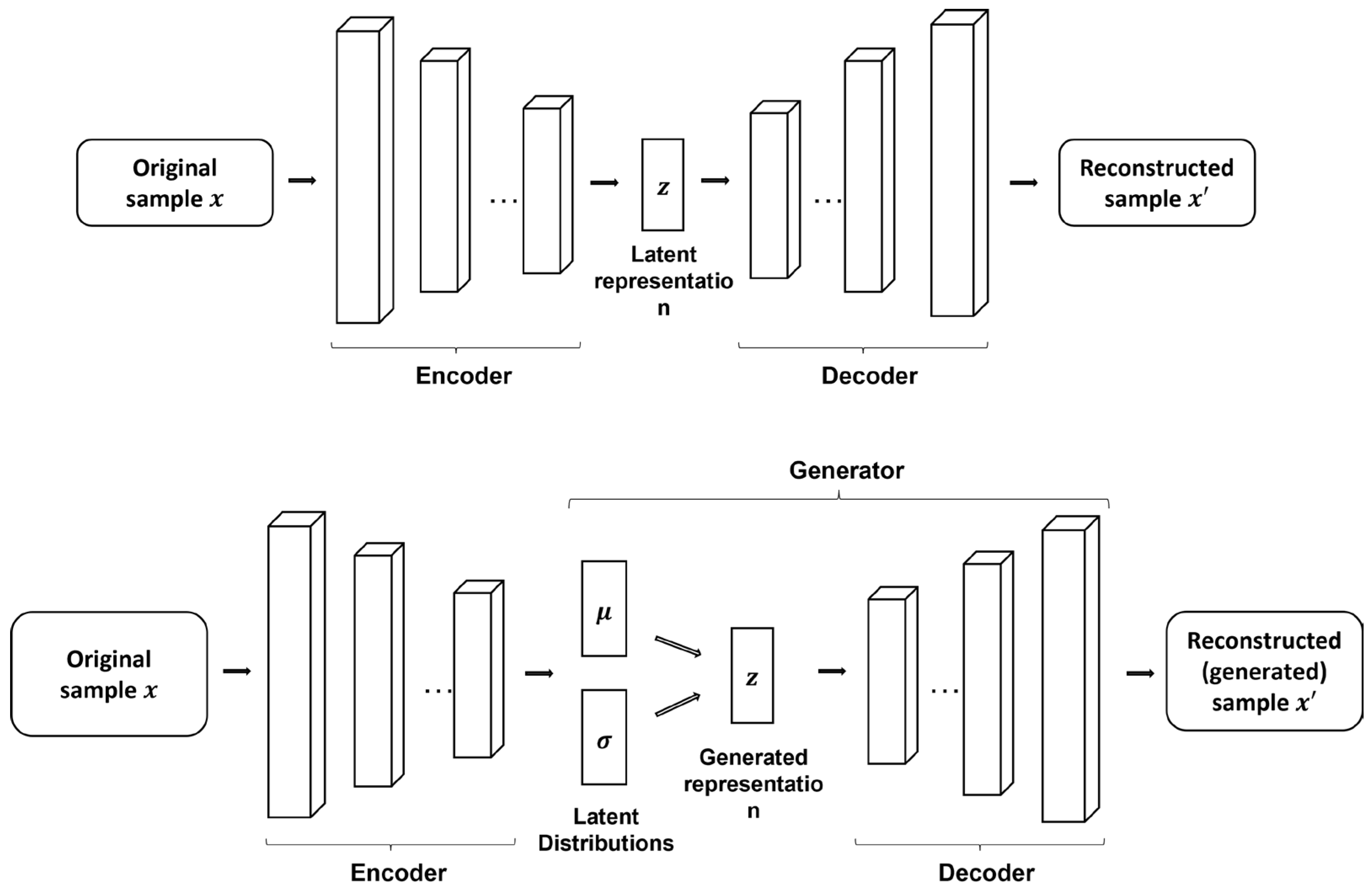{kind=link}
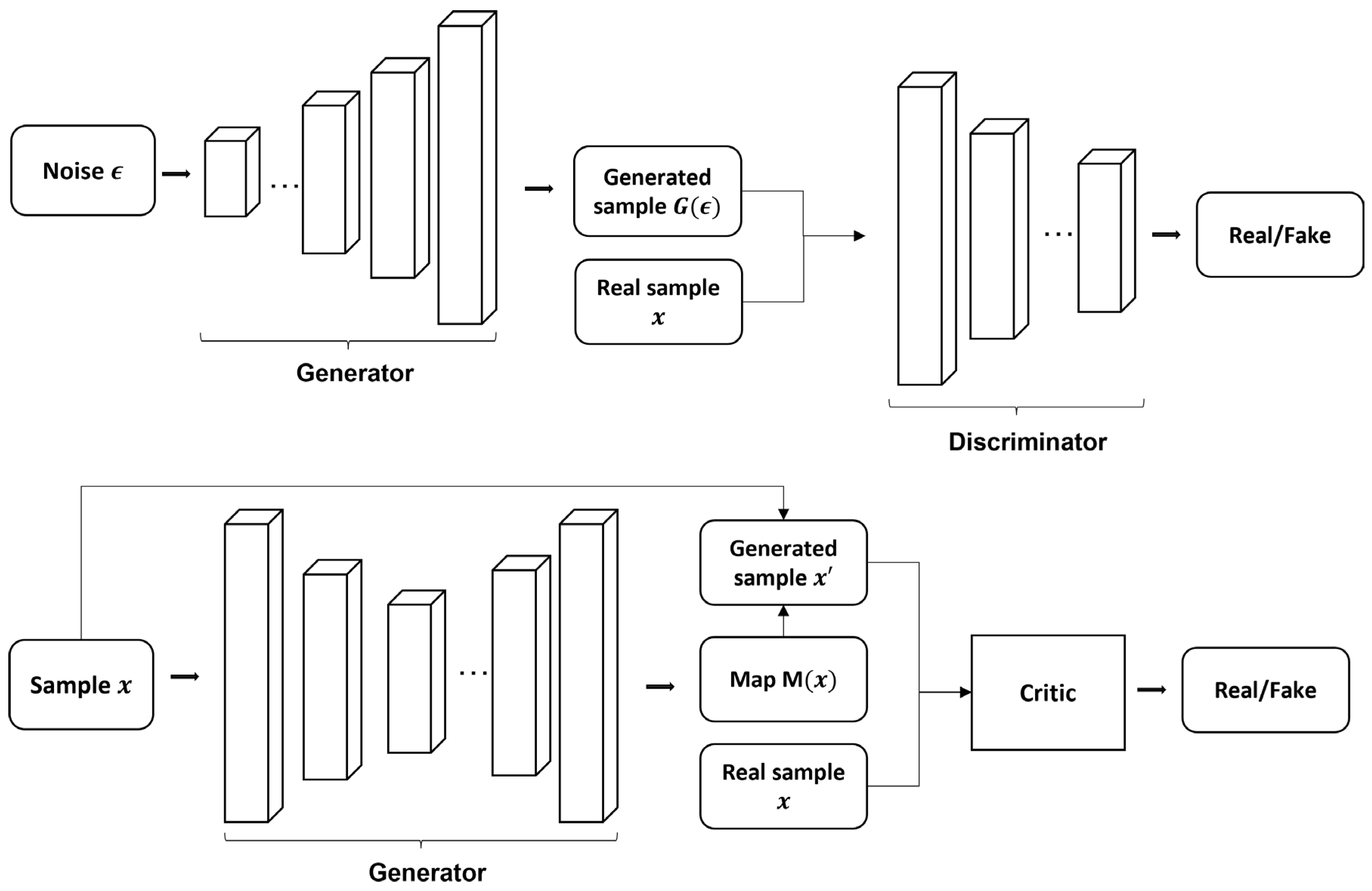{kind=link}
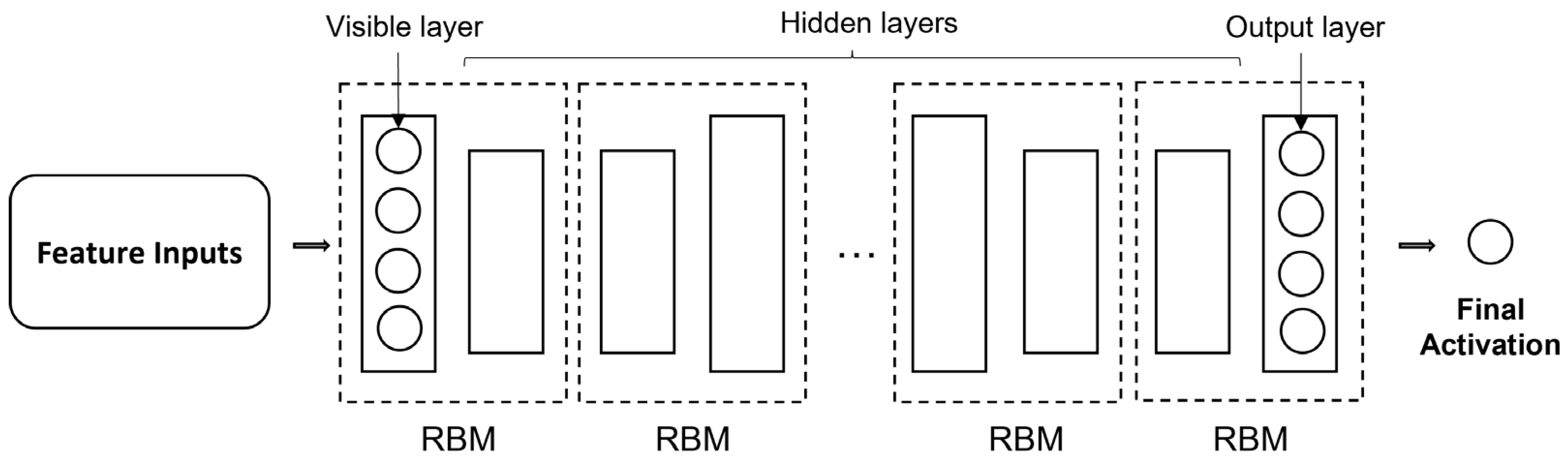{kind=link}
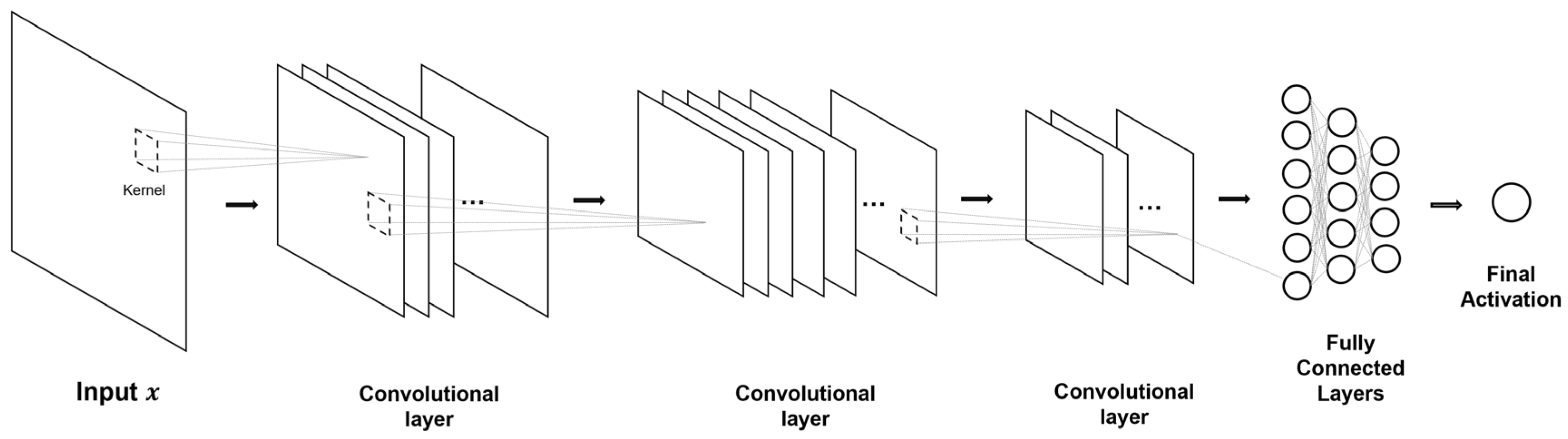{kind=link}
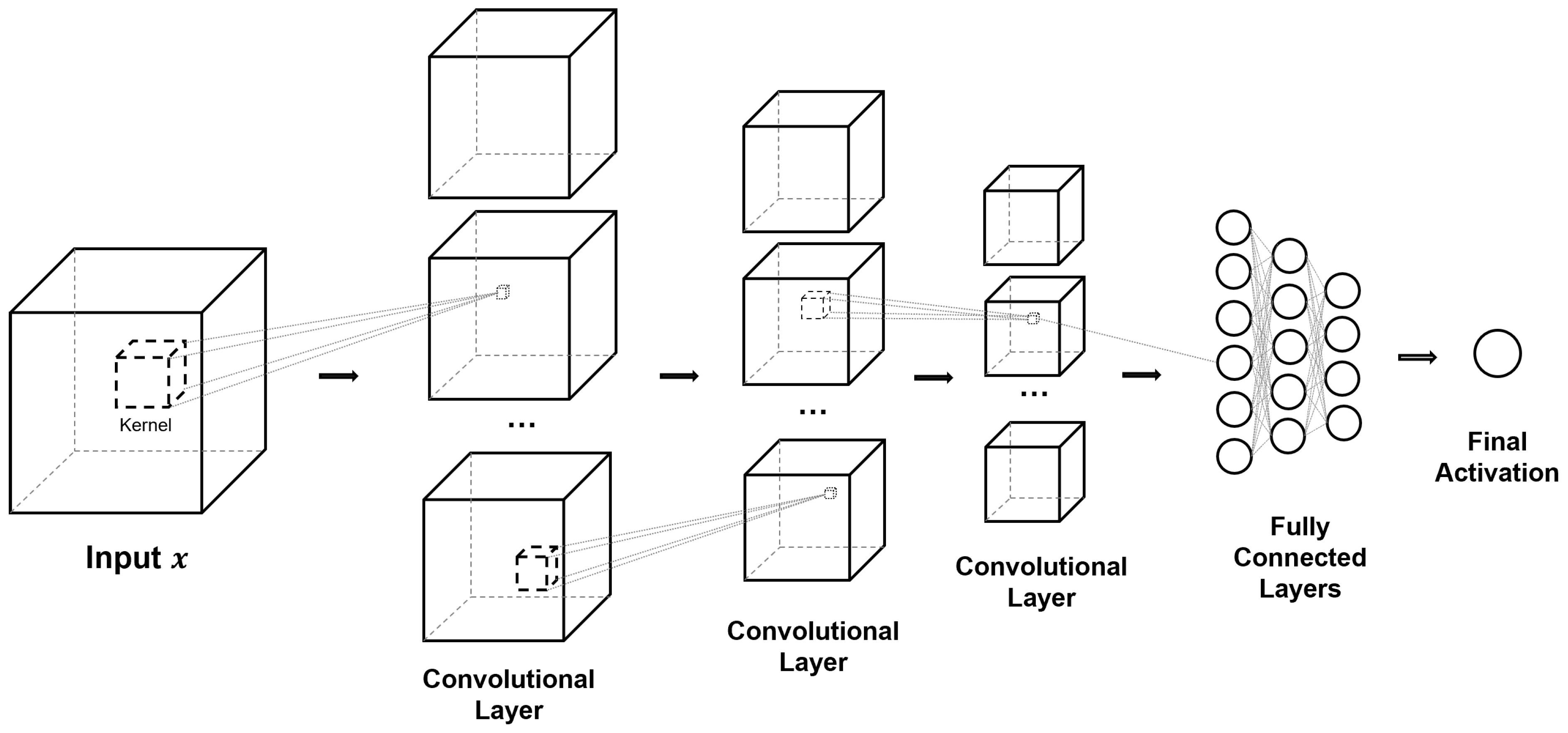{kind=link}
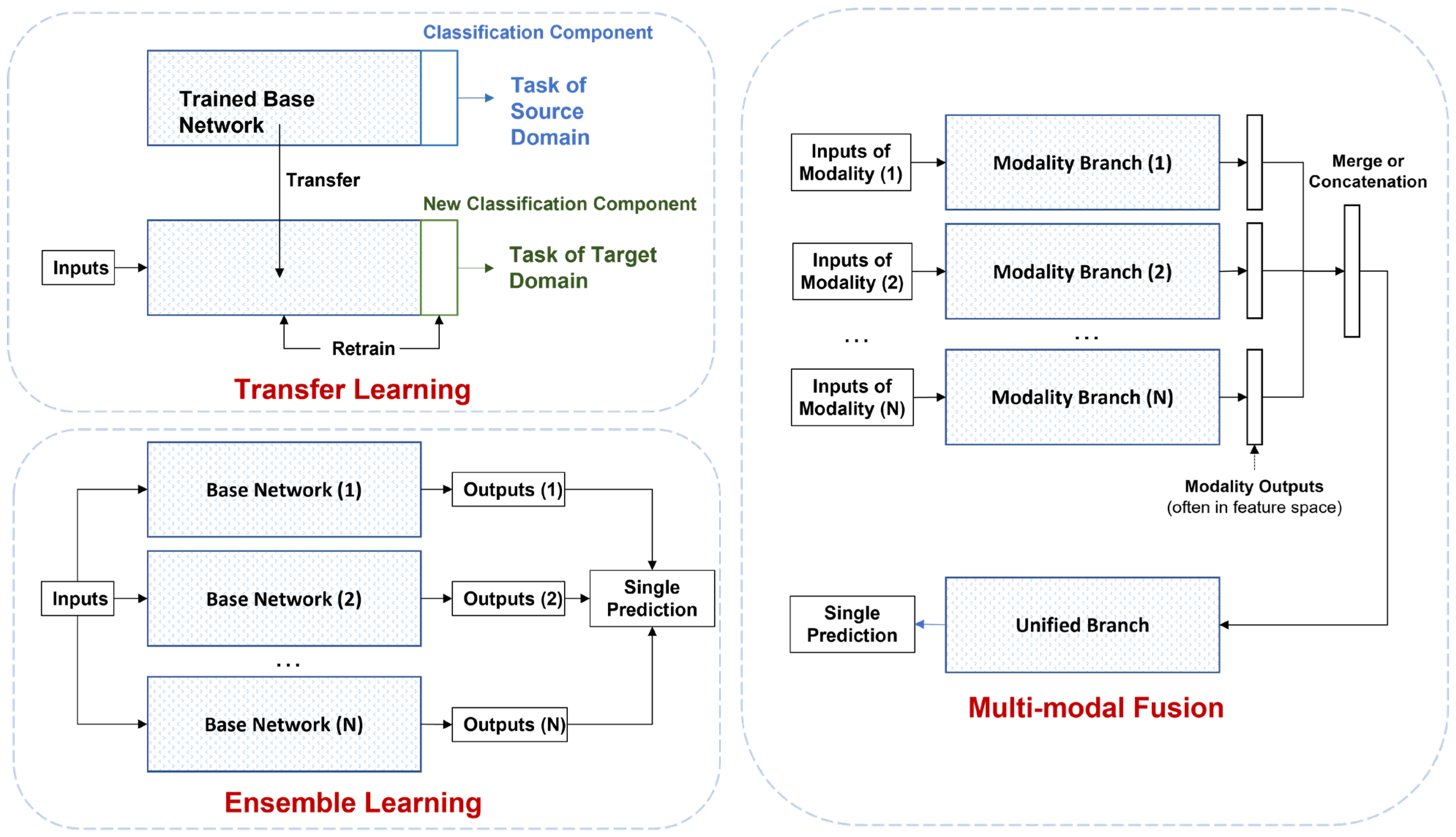{kind=link}
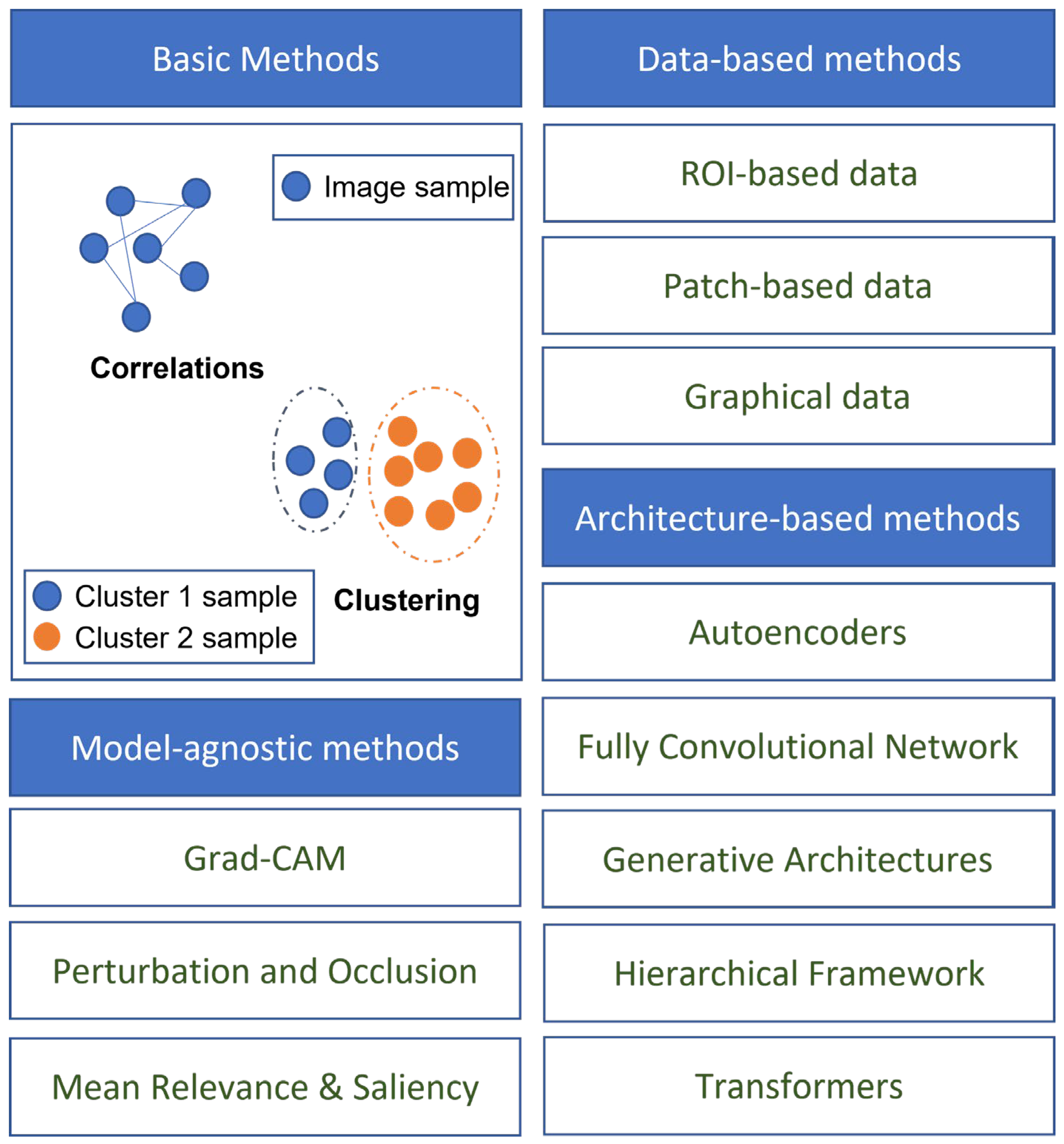{kind=link}
| Challenge | Description | Weight (1–5) |
|---|---|---|
| Numerical representation of AD stages | Variability in Alzheimer’s disease composite scores and difficulty distinguishing between stages of cognitive impairment. | 3 |
| Difficulty in preprocessing | Complex pipelines for preprocessing medical data, lack of standardization, subjective judgment of clinicians. | 3 |
| Unavailability of a comprehensive dataset | Abundance of data for AD but moderate number of subjects, below optimal requirements for generalization. | 2 |
| Difference in diagnostic criteria | Variations in diagnostic criteria and ground truth labels between studies, impacting comparability of results. | 3 |
| Lack of reproducibility | Lack of publicly available frameworks, implementation details, and comprehensive benchmarking standards. | 4 |
| Lack of expert knowledge | Researchers with DL expertise may lack medical background, particularly in preprocessing and identifying brain regions. | 2 |
| Generalizability and interpretability | Limited measures of generalizability, ‘black box’ nature of neural networks, hindering model interpretation and feedback. | 5 |
| Practical challenges | Subjectivity of cognitive assessments, invasiveness and cost of diagnostic techniques such as lumbar puncture and MRI. | 3 |
| Library | Number of Subjects | Modalities | Link |
|---|---|---|---|
| ADNI | 2750 | MRI, PET, CSF, Genetic | http://adni.loni.usc.edu/ (accessed on 17 April 2023) |
| OASIS | 1300+ | MRI, PET | https://oasis-brains.org/ (accessed on 17 April 2023) |
| AIBL | 1100+ | MRI, PET, CSF, Genetic | https://aibl.csiro.au/ (accessed on 17 April 2023) |
| NACC | 47,000+ | Neuropathology, Genetic | https://www.alz.washington.edu/ (accessed on 17 April 2023) |
| EDSD | 471 | MRI, DTI, Genetic | https://www.neugrid2.eu/ (accessed on 17 April 2023) |
| ARWIBO | 2700+ | MRI, PET, Genetic | http://www.arwibo.it/ (accessed on 17 April 2023) |
| HABS | 290 | MRI, PET, Genetic | https://habs.mgh.harvard.edu/ (accessed on 17 April 2023) |
| KLOSCAD | 6818 | MRI, QOL, Behavioral | http://kloscad.com/ (accessed on 17 April 2023) |
| VITA | 606 | MRT, Genetic | https://www.neugrid2.eu/ (accessed on 17 April 2023) |
| Study | Data Modalities | Number of Subjects | Classification ACC (%) | Classification AUC | ||||
|---|---|---|---|---|---|---|---|---|
| AD | NC | MCI | AD vs. NC | MCI vs. NC | AD vs. NC | MCI vs. NC | ||
| Suk and Shen [316] | MRI, PET | 51 | 52 | 99 | 95.9 | 85 | - | - |
| Suk, Lee, Shen and Initiative [166] | MRI, PET | 93 | 101 | 204 | 95.35 | 85.67 | - | - |
| Liu, Liu, Cai, Che, Pujol, Kikinis, Feng and Fulham [230] | MRI, PET | 85 | 109 | 77 | 82.59 | 82.10 | - | - |
| Li, Tran, Thung, Ji, Shen and Li [254] | MRI, PET, CSF | 51 | 99 | 52 | 91.4 | 77.4 | - | - |
| Aderghal, Benois-Pineau and Afdel [189] | MRI | 188 | 228 | 399 | 69.53 | 91.41 | - | - |
| Suk et al. [317] | MRI | 186 | 393 | 226 | 91.02 | - | 0.927 | - |
| Majumdar and Singhal [259] | MRI, PET, CSF | 51 | 99 | 52 | 95.4 | 85.7 | - | - |
| Cui, Liu and Li [287] | MRI | 198 | 229 | - | 89.69 | - | 0.9214 | - |
| Shi et al. [318] | MRI, PET | 51 | 52 | 99 | 97.13 | 87.24 | 0.972 | 0.901 |
| Liu, Wang, Tang, Hu, Wu and Pan [210] | MRI | - | 303 | 83 | - | 90.9 | - | - |
| Lu et al. [319] | PET | 226 | 304 | 521 | 93.58 | - | - | - |
| Ning et al. [320] | MRI, Genetic | 138 | 225 | 358 | - | - | 0.992 | - |
| Liu, Cheng, Wang, Wang and Initiative [170] | MRI, PET | 93 | 100 | 204 | 93.26 | 74.34 | 0.957 | 0.802 |
| Ge, Qu, Gu and Jakola [279] | MRI | 193 | 139 | - | 93.53 | - | - | - |
| Ju, Hu and Li [234] | fMRI | - | 79 | 91 | - | 86.47 | - | 0.916 |
| Liu, Zhang, Adeli and Shen [191] | MRI | 227 | 249 | 390 | 93.7 | - | - | - |
| Islam and Zhang [272] | PET | 169 | 400 | 661 | 88.76 | - | - | - |
| Wen, Thibeau-Sutre, Diaz-Melo, Samper-González, Routier, Bottani, Dormont, Durrleman, Burgos and Colliot [89] | MRI | 336 | 330 | 787 | 87 b | - | - | - |
| Liu, Li, Yan, Wang, Ma, Shen, Xu and Initiative [169] | MRI | 97 | 119 | 233 | 88.9 | 76.2 | 0.925 | 0.775 |
| Lee et al. [321] | MRI | 198 | 229 | 374 | 92.75 | 89.22 | 0.980 | 0.957 |
| Lian, Liu, Zhang and Shen [192] | MRI | 358 | 205 | 2964 | 89.5 | - | 0.959 | - |
| Cui and Liu [187] | MRI | 192 | 223 | 396 | 92.29 | 74.64 | 0.75 | 0.797 |
| Martinez-Murcia, Ortiz, Gorriz, Ramirez and Castillo-Barnes [277] | MRI | 99 | 168 | 212 | 84.9 | - | - | - |
| Duc, Ryu, Qureshi, Choi, Lee and Lee [273] | fMRI | 133 | 198 | - | 85.3 b | - | - | - |
| Kim, Lee, Lee, Oh, Yun and Yoo [251] | PET | 212 | 415 | - | 94.82 | - | 0.98 | - |
| Choi, Kim, Yoon, Lee, Lee and Initiative [276] | PET | 243 | 393 | 666 | 0.94 | - | ||
| Xia, Yue, Xu, Feng, Yang, Wang and Lei [290] | MRI | 198 | 299 | 408 | 94.19 | 79.01 | 0.96 | 0.88 |
| Ieracitano, Mammone, Hussain and Morabito [269] | EEG | 63 | 63 | 63 | 85.78 | 85.34 | - | - |
| Islam and Zhang [247] | PET | 98 | 105 | 208 | 71.45 | - | - | - |
| Qiu, Joshi, Miller, Xue, Zhou, Karjadi, Chang, Joshi, Dwyer and Zhu [275] | MRI, Demo, CA | 488 | 978 | - | 96.8 | - | 0.996 | - |
| Bashyam et al. [322] | MRI | 353 | 833 | 513 | 86 | 70.2 | 0.91 | 0.743 |
| Pan, Phan, Adel, Fossati, Gaidon, Wojak and Guedj [270] | PET | 237 | 242 | 526 | 93.13 | - | 0.9747 | - |
| Study | Data Modalities | Time to Conversion | Number of Subjects | ACC (%) | AUC | |
|---|---|---|---|---|---|---|
| cMCI | ncMCI | |||||
| Suk, Lee, Shen and Initiative [166] | MRI, PET | 78 | 128 | 75.92 | ||
| Suk, Lee, Shen and Initiative [317] | MRI | 18 M | 167 | 226 | 74.82 | 0.754 |
| Ning, Chen, Sun, Hobel, Zhao, Matloff, Toga and Initiative [320] | MRI, Genetic | 24 M | 166 | 192 | 0.835 | |
| Lu, Popuri, Ding, Balachandar, Beg and Initiative [319] | PET | 36 M | 112 | 409 | 82.51 | |
| Cui and Liu [187] | MRI | 165 | 231 | 74.64 | 0.777 | |
| Spasov, Passamonti, Duggento, Liò, Toschi and Initiative [283] | MRI, Demo, CA, Genetic | 36 M | 181 | 228 | 86 | 0.925 |
| Lee, Choi, Kim, Suk and Initiative [321] | MRI | 18 M | 160 | 214 | 88.52 | |
| Choi, Kim, Yoon, Lee, Lee and Initiative [276] | PET | 36 M | 167 | 274 | 0.82 | |
| Lian, Liu, Zhang and Shen [192] | MRI | 36 M | 205 | 465 | 80.9 | 0.781 |
| Wen, Thibeau-Sutre, Diaz-Melo, Samper-González, Routier, Bottani, Dormont, Durrleman, Burgos and Colliot [89] | MRI | 36 M | 295 | 298 | 76 | |
| Er and Goularas [239] | MRI | 125 | 169 | 87.2 | ||
| Pan, Phan, Adel, Fossati, Gaidon, Wojak and Guedj [270] | PET | 36 M | 166 | 360 | 83.05 | 0.868 |
| Study | Data Modalities | Classes | Accuracy |
|---|---|---|---|
| Liu, Liu, Cai, Che, Pujol, Kikinis, Feng and Fulham [230] | MRI, PET | AD, cMCI, ncMCI, NC | 64.07 |
| Dolph, Alam, Shboul, Samad and Iftekharuddin [229] | MRI | AD, MCI, NC | 58 |
| Shi, Zheng, Li, Zhang and Ying [318] | MRI, PET | AD, cMCI, ncMCI, NC | 57.00 |
| Liu, Zhang, Adeli and Shen [191] | MRI | AD, pMCI, sMCI, NC | 51.8 |
| Lee, Choi, Kim, Suk and Initiative [321] | MRI | AD, MCI, NC | 71.17 |
| Liu, Yadav, Fernandez-Granda and Razavian [281] | MRI | AD, MCI, NC | 70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Q.; Wang, J.; Yu, X.; Wang, S.; Zhang, Y. A Survey of Deep Learning for Alzheimer’s Disease. Mach. Learn. Knowl. Extr. 2023, 5, 611-668. https://doi.org/10.3390/make5020035
Zhou Q, Wang J, Yu X, Wang S, Zhang Y. A Survey of Deep Learning for Alzheimer’s Disease. Machine Learning and Knowledge Extraction. 2023; 5(2):611-668. https://doi.org/10.3390/make5020035
Chicago/Turabian StyleZhou, Qinghua, Jiaji Wang, Xiang Yu, Shuihua Wang, and Yudong Zhang. 2023. "A Survey of Deep Learning for Alzheimer’s Disease" Machine Learning and Knowledge Extraction 5, no. 2: 611-668. https://doi.org/10.3390/make5020035
APA StyleZhou, Q., Wang, J., Yu, X., Wang, S., & Zhang, Y. (2023). A Survey of Deep Learning for Alzheimer’s Disease. Machine Learning and Knowledge Extraction, 5(2), 611-668. https://doi.org/10.3390/make5020035