
Molecular Diagnosis of COVID-19 Sudden and Unexplained Deaths: The Insidious Face of the Pandemic

 ,
,
Abstract
:1. Introduction
2. Material and Methods
3. Results
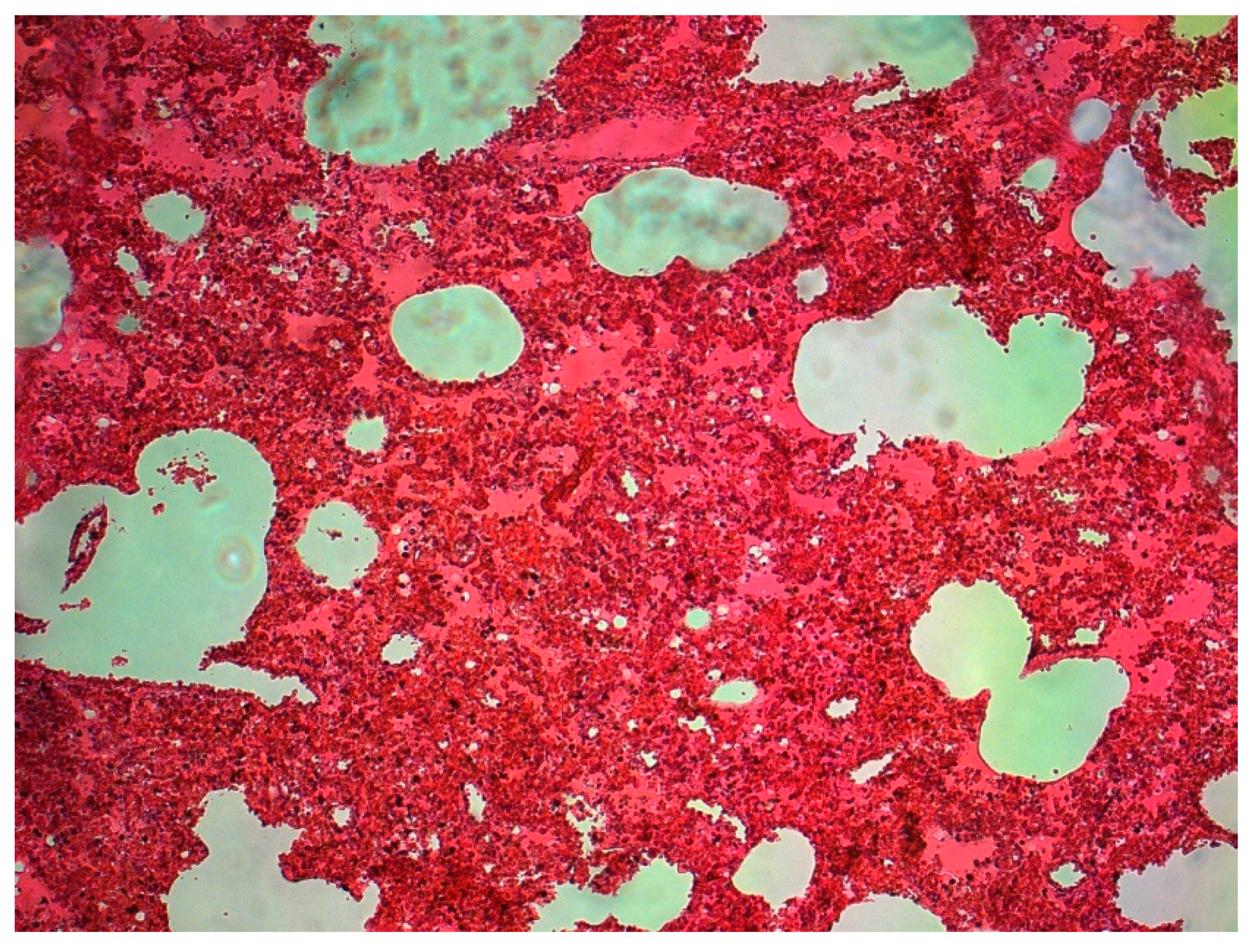
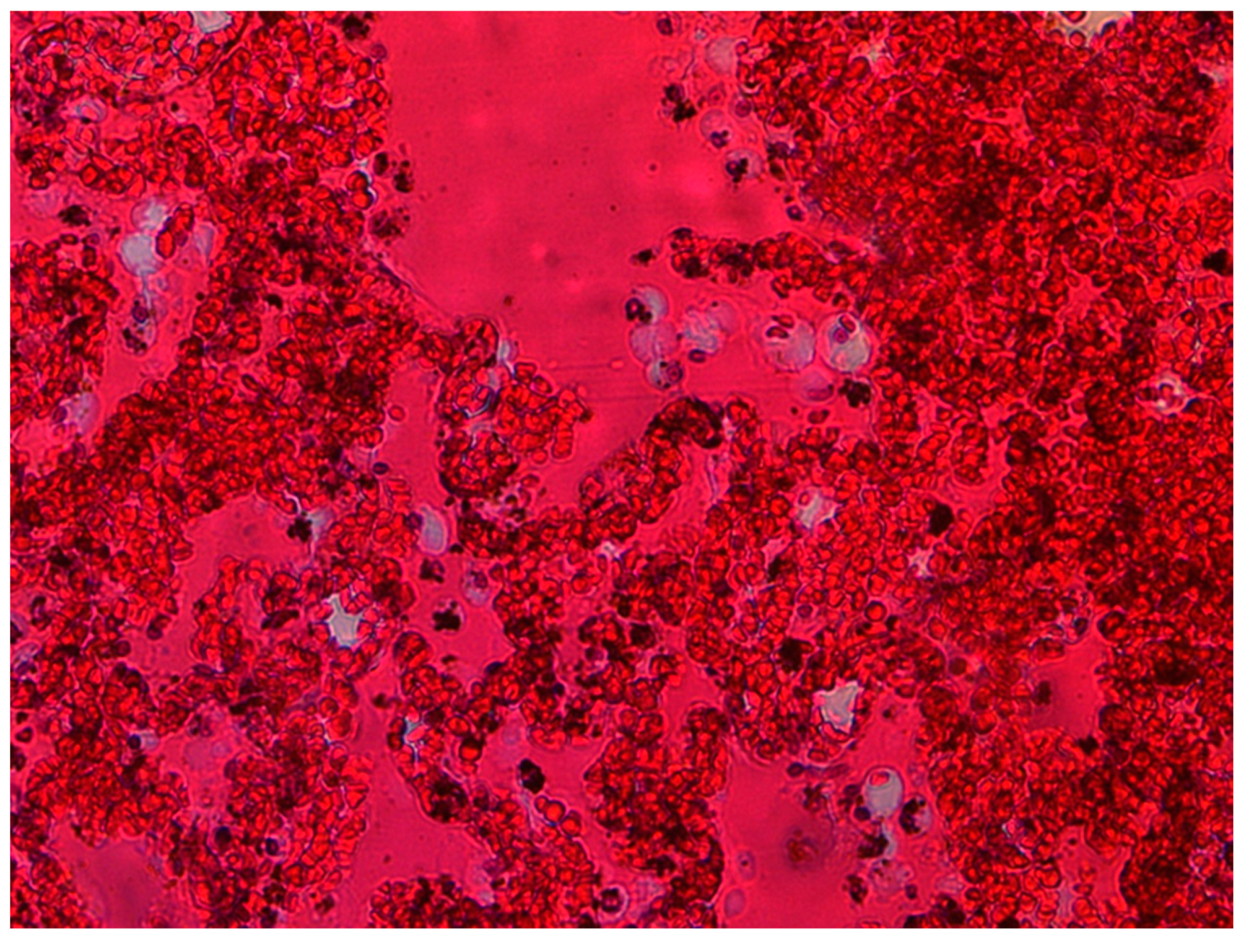
3.1. Pathology Findings
3.2. Genetic Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Timeline: WHO’s COVID-19 Response. p. Accessed May 2022. 2021. Available online: https://www.europarl.europa.eu/news/pl/headlines/society/20220120STO21427/covid-19-os-czasu-dzialan-ue-w-2022-r (accessed on 1 July 2023).
- Banner, J.; Basso, C.; Tolkien, Z.; Kholova, I.; Michaud, K.; Gallagher, P.J. Autopsy examination in sudden cardiac death: A current perspective on behalf of the Association for European Cardiovascular Pathology. Virchows Arch. 2021, 478, 687–693. [Google Scholar] [CrossRef]
- Barton, L.M.; Duval, E.J.; Stroberg, E.; Ghosh, S.; Mukhopadhyay, S. COVID-19 Autopsies, Oklahoma, USA. Am. J. Clin. Pathol. 2020, 153, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Basso, C.; Calabrese, F.; Sbaraglia, M.; Del Vecchio, C.; Carretta, G.; Saieva, A.; Donato, D.; Flor, L.; Crisanti, A.; Tos, A.P.D. Feasibility of postmortem examination in the era of COVID-19 pandemic: The experience of a Northeast Italy University Hospital. Virchows Arch. 2020, 477, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Borczuk, A.C.; Salvatore, S.P.; Seshan, S.V.; Patel, S.S.; Bussel, J.B.; Mostyka, M.; Elsoukkary, S.; He, B.; Del Vecchio, C.; Fortarezza, F.; et al. COVID-19 pulmonary pathology: A multi-institutional autopsy cohort from Italy and New York City. Mod. Pathol. 2020, 33, 2156–2168. [Google Scholar] [CrossRef] [PubMed]
- Bradley, B.T.; Maioli, H.; Johnston, R.; Chaudhry, I.; Fink, S.L.; Xu, H.; Najafian, B.; Deutsch, G.; Lacy, J.M.; Williams, T.; et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington State: A case series. Lancet 2020, 396, 320–332. [Google Scholar] [CrossRef]
- Bryce, C.; Grimes, Z.; Pujadas, E.; Ahuja, S.; Beasley, M.B.; Albrecht, R.; Hernandez, T.; Stock, A.; Zhao, Z.; AlRasheed, M.R.; et al. Pathophysiology of SARS-CoV-2: The Mount Sinai COVID-19 autopsy experience. Mod. Pathol. 2021, 34, 1456–1467. [Google Scholar] [CrossRef]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Dorward, D.A.; Russell, C.D.; Um, I.H.; Elshani, M.; Armstrong, S.D.; Penrice-Randal, R.; Millar, T.; Lerpiniere, C.E.B.; Tagliavini, G.; Hartley, C.S.; et al. Tissue-Specific Immunopathology in Fatal COVID-19. Am. J. Respir. Crit. Care Med. 2021, 203, 192–201. [Google Scholar] [CrossRef]
- Edler, C.; Schröder, A.S.; Aepfelbacher, M.; Fitzek, A.; Heinemann, A.; Heinrich, F.; Klein, A.; Langenwalder, F.; Lütgehetmann, M.; Meißner, K.; et al. Dying with SARS-CoV-2 infection—An autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int. J. Legal. Med. 2020, 134, 1275–1284. [Google Scholar] [CrossRef]
- Fassan, M.; Mescoli, C.; Sbaraglia, M.; Guzzardo, V.; Russo, F.P.; Fabris, R.; Trevenzoli, M.; Pelizzaro, F.; Cattelan, A.M.; Basso, C.; et al. Liver histopathology in COVID-19 patients: A mono-Institutional series of liver biopsies and autopsy specimens. Pathol. Res. Pract. 2021, 221, 153451. [Google Scholar] [CrossRef] [PubMed]
- Hooper, J.E.; Padera, R.F.; Dolhnikoff, M.; da Silva, L.F.F.; Duarte-Neto, A.N.; Kapp, M.E.; Lacy, J.M.; Mauad, T.; Saldiva, P.H.N.; Rapkiewicz, A.V.; et al. A Postmortem Portrait of the Coronavirus Disease 2019 (COVID-19) Pandemic: A Large Multi-institutional Autopsy Survey Study. Arch. Pathol. Lab. Med. 2021, 145, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Lv, B.; Liu, H.; He, S.; Zhang, G.; Li, C.; Li, W.; Li, W.; He, Y.; Zhang, T.; et al. Autopsy and statistical evidence of disturbed hemostasis progress in COVID-19: Medical records from 407 patients. Thromb. J. 2021, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Pacheco, M.; Silva, P.L.; Cruz, F.F.; Battaglini, D.; Robba, C.; Pelosi, P.; Morales, M.M.; Neves, C.C.; Rocco, P.R.M. Pathogenesis of Multiple Organ Injury in COVID-19 and Potential Therapeutic Strategies. Front. Physiol. 2021, 12, 593223. [Google Scholar] [CrossRef] [PubMed]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef]
- Nie, X.; Qian, L.; Sun, R.; Huang, B.; Dong, X.; Xiao, Q.; Zhang, Q.; Lu, T.; Yue, L.; Chen, S.; et al. Multi-organ proteomic landscape of COVID-19 autopsies. Cell 2021, 184, 775–791.e14. [Google Scholar] [CrossRef]
- Schaller, T.; Hirschbühl, K.; Burkhardt, K.; Braun, G.; Trepel, M.; Märkl, B.; Claus, R. Postmortem Examination of Patients With COVID-19. JAMA 2020, 323, 2518. [Google Scholar] [CrossRef]
- Sessa, F.; Bertozzi, G.; Cipolloni, L.; Baldari, B.; Cantatore, S.; D’Errico, S.; Di Mizio, G.; Asmundo, A.; Castorina, S.; Salerno, M.; et al. Clinical-Forensic Autopsy Findings to Defeat COVID-19 Disease: A Literature Review. J. Clin. Med. 2020, 9, 2026. [Google Scholar] [CrossRef]
- Szekely, L.; Bozoky, B.; Bendek, M.; Ostad, M.; Lavignasse, P.; Haag, L.; Wu, J.; Jing, X.; Gupta, S.; Saccon, E.; et al. Pulmonary stromal expansion and intra-alveolar coagulation are primary causes of COVID-19 death. Heliyon 2021, 7, e07134. [Google Scholar] [CrossRef]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.-Y. Pathological study of the 2019 novel coronavirus disease (COVID-19) through postmortem core biopsies. Mod. Pathol. 2020, 33, 1007–1014. [Google Scholar] [CrossRef]
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019–COVID-19. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Asselah, T.; Durantel, D.; Pasmant, E.; Lau, G.; Schinazi, R.F. COVID-19: Discovery, diagnostics and drug development. J. Hepatol. 2021, 74, 168–184. [Google Scholar] [CrossRef] [PubMed]
- Douceron, H.; Deforges, L.; Gherardi, R.; Sobel, A.; Chariot, P. Long-lasting postmortem viability of human immunodeficiency virus: A potential risk in forensic medicine practice. Forensic. Sci. Int. 1993, 60, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Prescott, J.; Bushmaker, T.; Fischer, R.; Miazgowicz, K.; Judson, S.; Munster, V.J. Postmortem Stability of Ebola Virus. Emerg. Infect. Dis. 2015, 21, 856–859. [Google Scholar] [CrossRef] [PubMed]
- De Cock, K.M.; Zielinski-Gutiérrez, E.; Lucas, S.B. Learning from the Dead. N. Engl. J. Med. 2019, 381, 1889–1891. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, P.N. International Society for Infectious Diseases United States. The Infection Hazards of Human Cadavers. Guide to Infection Control in the Healthcare Setting. 2021. Available online: https://isid.org/guide/infectionprevention/humancadavers/ (accessed on 30 June 2023).
- Applied BiosystemsTM, MagMAX Viral/Pathogen II Nucleic Acid Isolation Kit (CE-IVD): Instructions for Use. Pub. No. MAN0019746. USA, 2021. Available online: https://www.thermofisher.com/document-connect/document-connect.html?url=https://assets.thermofisher.com/TFS-Assets%2FBID%2FApplication-Notes%2Fmagmax-viral-pathogen-nucleic-acid-isolation-kit-kingfisher-flex-purification-system-app-note.pdf (accessed on 1 July 2023).
- Langeland, N.; Cox, R.J. Are low SARS-CoV-2 viral loads in infected children missed by RT-PCR testing? Lancet Reg. Health-Eur. 2021, 5, 100138. [Google Scholar] [CrossRef]
- Little, B.P. False-Negative Nasopharyngeal Swabs and Positive Bronchoalveolar Lavage: Implications for Chest CT in Diagnosis of COVID-19 Pneumonia. Radiology 2021, 298, E160–E161. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.R.; Sundararaju, S.; Manickam, C.; Mirza, F.; Al-Hail, H.; Lorenz, S.; Tang, P. A Novel Point Mutation in the N Gene of SARS-CoV-2 May Affect the Detection of the Virus by Reverse Transcription-Quantitative PCR. J. Clin. Microbiol. 2021, 59. [Google Scholar] [CrossRef]
- Heald-Sargent, T.; Muller, W.J.; Zheng, X.; Rippe, J.; Patel, A.B.; Kociolek, L.K. Age-Related Differences in Nasopharyngeal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Levels in Patients with Mild to Moderate Coronavirus Disease 2019 (COVID-19). JAMA Pediatr. 2020, 174, 902. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Servadei, F.; Mauriello, S.; Scimeca, M.; Caggiano, B.; Ciotti, M.; Anemona, L.; Montanaro, M.; Giacobbi, E.; Treglia, M.; Bernardini, S.; et al. Persistence of SARS-CoV-2 Viral RNA in Nasopharyngeal Swabs after Death: An Observational Study. Microorganisms 2021, 9, 800. [Google Scholar] [CrossRef] [PubMed]
- Aiello, F.; Ciotti, M.; Afflitto, G.G.; Rapanotti, M.C.; Caggiano, B.; Treglia, M.; Grelli, S.; Bernardini, S.; Mauriello, S.; Nucci, C.; et al. Post-Mortem RT-PCR Assay for SARS-CoV-2 RNA in COVID-19 Patients’ Corneal Epithelium, Conjunctival and Nasopharyngeal Swabs. J. Clin. Med. 2021, 10, 4256. [Google Scholar] [CrossRef] [PubMed]
- Maiese, A.; Frati, P.; Del Duca, F.; Santoro, P.; Manetti, A.C.; La Russa, R.; Di Paolo, M.; Turillazzi, E.; Fineschi, V. Myocardial Pathology in COVID-19-Associated Cardiac Injury: A Systematic Review. Diagnostics 2021, 11, 1647. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef]
- Patrucco, F.; Carriero, A.; Falaschi, Z.; Paschè, A.; Gavelli, F.; Airoldi, C.; Bellan, M.; Sainaghi, P.P.; Solidoro, P.; Balbo, P.E. COVID-19 Diagnosis in Case of Two Negative Nasopharyngeal Swabs: Association between Chest CT and Bronchoalveolar Lavage Results. Radiology 2021, 298, E152–E155. [Google Scholar] [CrossRef]
- Fineschi, V.; Aprile, A.; Aquila, I.; Arcangeli, M.; Asmundo, A.; Bacci, M.; Cingolani, M.; Cipolloni, L.; D’Errico, S.; De Casamassimi, I.; et al. Management of the corpse with suspect, probable or confirmed COVID-19 respiratory infection-Italian interim recommendations for personnel potentially exposed to material from corpses, including body fluids, in morgue structures and during autopsy practi. Pathologica 2020, 112, 64–77. [Google Scholar] [CrossRef]
- Italian Ministry of Health. Emergency Indications Related to the COVID-19 Epidemic Concerning the Funeral, Cemetery and Cremation Sector; Italian Ministry of Health: Rome, Italy, 2020.
- Maiese, A.; Manetti, A.C.; La Russa, R.; Di Paolo, M.; Turillazzi, E.; Frati, P.; Fineschi, V. Autopsy findings in COVID-19-related deaths: A literature review. Forensic. Sci. Med. Pathol. 2021, 17, 279–296. [Google Scholar] [CrossRef]
- Zanza, C.; Racca, F.; Longhitano, Y.; Piccioni, A.; Franceschi, F.; Artico, M.; Abenavoli, L.; Maiese, A.; Passaro, G.; Volonnino, G.; et al. Risk Management and Treatment of Coagulation Disorders Related to COVID-19 Infection. Int. J. Environ. Res. Public Health 2021, 18, 1268. [Google Scholar] [CrossRef] [PubMed]
- WHO. Infection Prevention and Control for the Safe Management of a Dead Body in the Context of COVID-19; Interim Guidance; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Polese-Bonatto, M.; Sartor, I.T.S.; Varela, F.H.; Giannini, G.L.T.; Azevedo, T.R.; Kern, L.B.; Fernandes, I.R.; Zavaglia, G.O.; de David, C.N.; Santos, A.P.; et al. Children Have Similar Reverse Transcription Polymerase Chain Reaction Cycle Threshold for Severe Acute Respiratory Syndrome Coronavirus 2 in Comparison with Adults. Pediatr. Infect. Dis. J. 2021, 40, e413–e417. [Google Scholar] [CrossRef]
- ICMR/GOVNEWS Indian Council of Medical Research; Ansari Nagar: New Delhi, India, 2022; Available online: https://main.icmr.nic.in/ (accessed on 1 July 2023).
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef]
- Pagano, A.M.; Maiese, A.; Izzo, C.; Maiese, A.; Ametrano, M.; De Matteis, A.; Attianese, M.R.; Busaato, G.; Caruso, R.; Cestari, M.; et al. COVID-19 Risk Management and Screening in the Penitentiary Facilities of the Salerno Province in Southern Italy. Int. J. Environ. Res. Public Health 2020, 17, 8033. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Sample | Sex | Age | Method | Lung | Nasopharynx | ||||
|---|---|---|---|---|---|---|---|---|---|
| Gene ORF | Gene N | Gene S | Gene ORF | Gene N | Gene S | ||||
| 1 | F | 2 month | (-) | (-) | (-) | 30 | 30 | 30 | |
| 2 | F | 3 month | RT-PCR | 31 | 31 | (-) | 28 | 30 | (-) |
| 3 | F | 14 month | (-) | (-) | (-) | 9 | 9 | 9 | |
| 4 | F | 7 | 14 | 14 | 12 | 20 | 18 | (-) | |
| 5 | M | 26 | 9 | 9 | 9 | (-) | (-) | (-) | |
| 6 | M | 39 | 37 | 37 | 37 | (-) | (-) | (-) | |
| 7 | M | 43 | 25 | 25 | 25 | (-) | (-) | (-) | |
| 8 | F | 44 | 20 | 20 | 20 | (-) | (-) | (-) | |
| 9 | M | 47 | 34 | 34 | (-) | (-) | (-) | (-) | |
| 10 | F | 51 | 36 | 36 | (-) | (-) | (-) | (-) | |
| 11 | M | 59 | 16 | 16 | 17 | 16 | 17 | 16 | |
| 12 | M | 64 | (-) | (-) | (-) | 23 | 22 | (-) | |
| 13 | M | 65 | 26 | 27 | (-) | 13 | 13 | (-) | |
| 14 | M | 66 | 24 | 24 | (-) | 24 | 21 | (-) | |
| 15 | M | 67 | 31 | 31 | 33 | 37 | 37 | 37 | |
| 16 | M | 70 | 20 | 21 | 27 | (-) | (-) | (-) | |
| 17 | M | 70 | 37 | 37 | (-) | (-) | (-) | (-) | |
| 18 | M | 70 | 25 | 25 | 25 | 15 | 15 | 15 | |
| 19 | M | 71 | 26 | 26 | 26 | (-) | (-) | (-) | |
| 20 | F | 77 | 37 | 37 | 37 | (-) | (-) | (-) | |
| 21 | F | 80 | 26 | 26 | (-) | (-) | (-) | (-) | |
| 22 | F | 84 | 15 | 16 | 15 | 15 | 16 | 15 | |
| 23 | M | 84 | 28 | 26 | 30 | (-) | (-) | (-) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lisman, D.; Zielińska, G.; Drath, J.; Łaszczewska, A.; Savochka, I.; Parafiniuk, M.; Ossowski, A. Molecular Diagnosis of COVID-19 Sudden and Unexplained Deaths: The Insidious Face of the Pandemic. Diagnostics 2023, 13, 2980. https://doi.org/10.3390/diagnostics13182980
Lisman D, Zielińska G, Drath J, Łaszczewska A, Savochka I, Parafiniuk M, Ossowski A. Molecular Diagnosis of COVID-19 Sudden and Unexplained Deaths: The Insidious Face of the Pandemic. Diagnostics. 2023; 13(18):2980. https://doi.org/10.3390/diagnostics13182980
Chicago/Turabian StyleLisman, Dagmara, Grażyna Zielińska, Joanna Drath, Aleksandra Łaszczewska, Ilona Savochka, Mirosław Parafiniuk, and Andrzej Ossowski. 2023. "Molecular Diagnosis of COVID-19 Sudden and Unexplained Deaths: The Insidious Face of the Pandemic" Diagnostics 13, no. 18: 2980. https://doi.org/10.3390/diagnostics13182980
APA StyleLisman, D., Zielińska, G., Drath, J., Łaszczewska, A., Savochka, I., Parafiniuk, M., & Ossowski, A. (2023). Molecular Diagnosis of COVID-19 Sudden and Unexplained Deaths: The Insidious Face of the Pandemic. Diagnostics, 13(18), 2980. https://doi.org/10.3390/diagnostics13182980