
A Review of Rickettsial Diseases Other Than Scrub Typhus in India

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
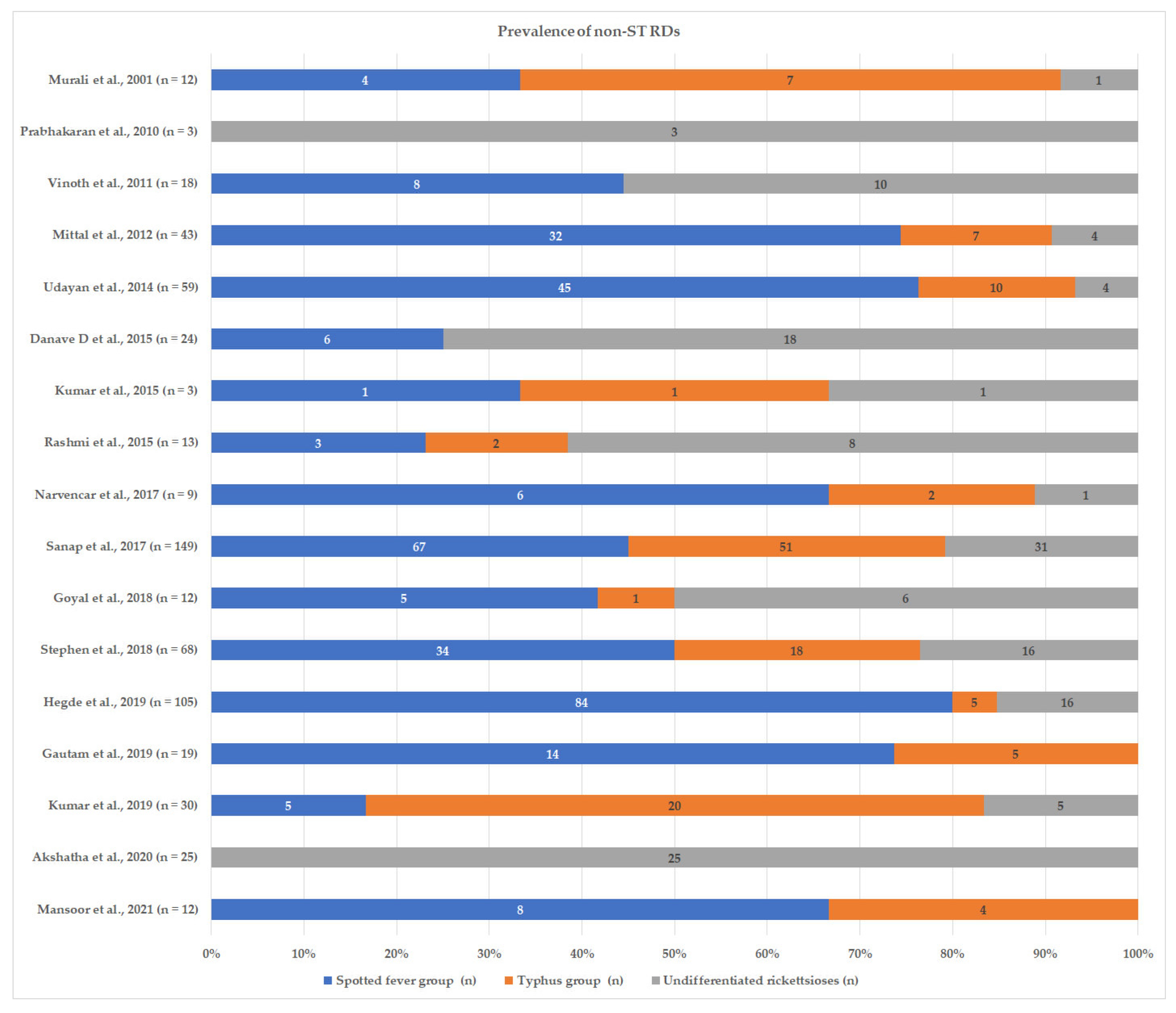
3.1. Burden of Non-ST RDs in India
3.1.1. Serological Studies
3.1.2. Molecular Studies
3.1.3. Co-Infections
3.1.4. Pregnancy
3.1.5. Travel-Related Non-ST RDs
3.1.6. Role of Climate and Ecology
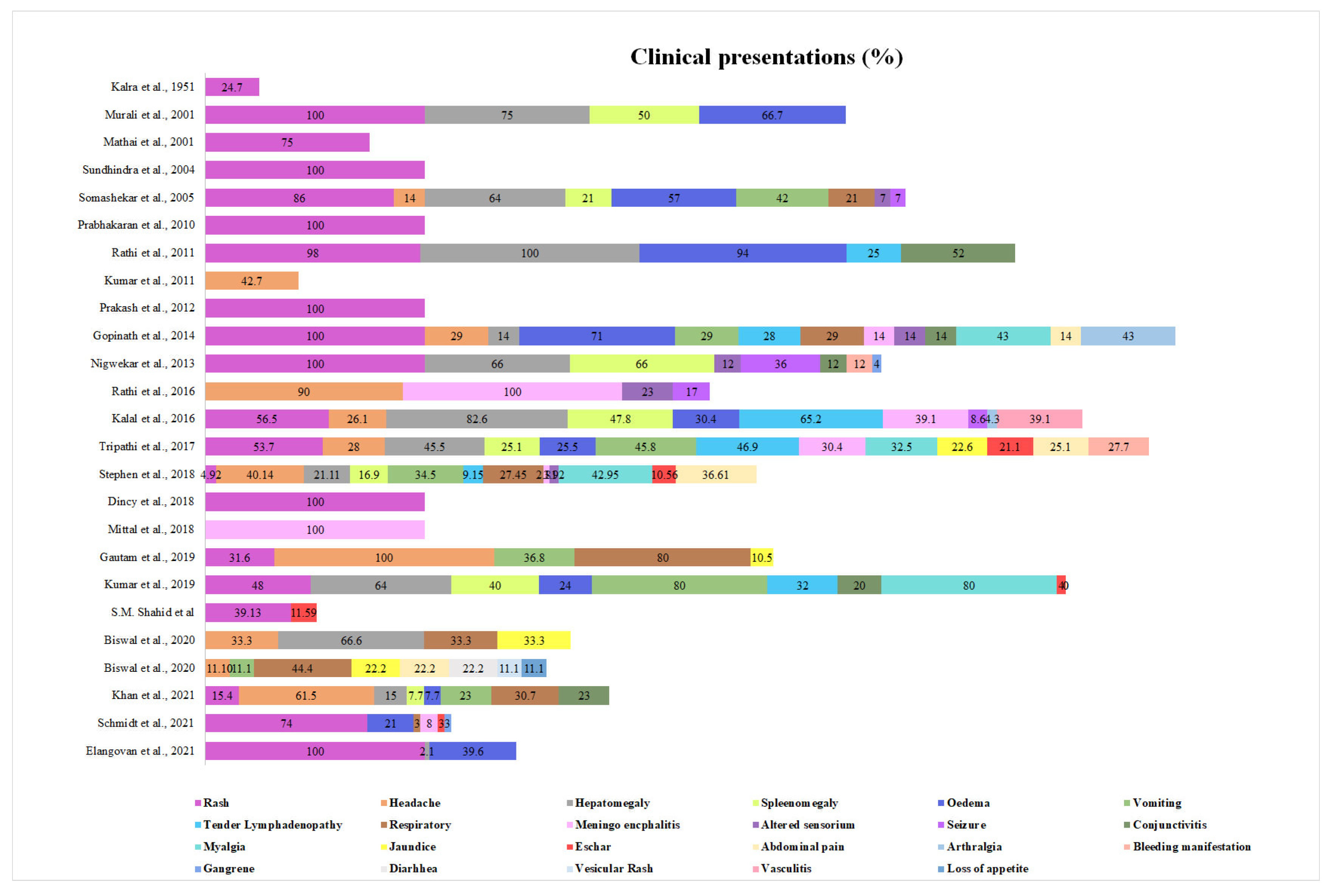
3.2. Clinical Presentations
3.2.1. Common Presentation
3.2.2. Other Presentations
Ocular Manifestations
Neurological Manifestations
Other Less Common/Atypical Presentations
3.2.3. Laboratory Findings
3.2.4. Treatment and Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Megaw, J.W.D. A Case of Fever Resembling Brill’s Disease. Indian Med. Gaz. 1917, 52, 15–18. [Google Scholar]
- Phipson, E.S. Observations on an Outbreak of Typhus in Simla with Special Reference to the Weil-Felix Reaction. Indian J. Med. Res. 1923, XI, 305–318. [Google Scholar]
- Kalra, S.L.; Rao, K.N.A. Typhus Fevers in Kashmir State. Part II. Murine Typhus. Indian J. Med. Res. 1951, 39, 297–302. [Google Scholar] [PubMed]
- Tilak, R.; Kunte, R. Scrub Typhus Strikes Back: Are We Ready? Armed Forces Med. J. India 2019, 75, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.K. Scrub Typhus. J. Assoc. Physicians India 2005, 53, 954–958. [Google Scholar]
- Khan, S.A.; Murhekar, M.V.; Bora, T.; Kumar, S.; Saikia, J.; Kamaraj, P.; Sabarinanthan, R. Seroprevalence of Rickettsial Infections in Northeast India: A Population-Based Cross-Sectional Survey. Asia Pac. J. Public Health 2021, 33, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Kamarasu, K.; Malathi, M.; Rajagopal, V.; Subramani, K.; Jagadeeshramasamy, D.; Mathai, E. Serological Evidence for Wide Distribution of Spotted Fevers & Typhus Fever in Tamil Nadu. Indian J. Med. Res. 2007, 126, 128–130. [Google Scholar] [PubMed]
- Kavirayani, V.; Madiyal, M.; Aroor, S.; Chhabra, S. Clinical Profile and Role of Serology in Pediatric Acute Febrile Illness: Experience from a Tertiary Care Hospital in South India. Clin. Epidemiol. Glob. Health 2021, 12, 100898. [Google Scholar] [CrossRef]
- Stephen, S.; Ambroise, S.; Gunasekaran, D.; Hanifah, M.; Sangeetha, B.; Pradeep, J.; Sarangapani, K. Serological Evidence of Spotted Fever Group Rickettsiosis in and around Puducherry, South India-A Three Years Study. J. Vector Borne Dis. 2018, 55, 144–150. [Google Scholar] [CrossRef]
- Kulkarni, A.; Vaidya, S.; Kulkarni, P.; Bidri, L.H.; Padwal, S. Rickettsial Disease—An Experience. Pediatr. Infect. Dis. 2009, 1, 118–126. [Google Scholar]
- Murali, N.; Pillai, S.; Cherian, T.; Raghupathy, P.; Padmini, V.; Mathai, E. Rickettsial Infections in South India—How to Spot the Spotted Fever. Indian Pediatr. 2001, 38, 1393–1396. [Google Scholar] [PubMed]
- Prakash, J.A.J.; Sohan Lal, T.; Rosemol, V.; Verghese, V.P.; Pulimood, S.A.; Reller, M.; Dumler, J.S. Molecular Detection and Analysis of Spotted Fever Group Rickettsia in Patients with Fever and Rash at a Tertiary Care Centre in Tamil Nadu, India. Pathog. Glob. Health 2012, 106, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Biswal, M.; Krishnamoorthi, S.; Bisht, K.; Sehgal, A.; Kaur, J.; Sharma, N.; Suri, V.; Sethi, S. Rickettsial Diseases: Not Uncommon Causes of Acute Febrile Illness in India. Trop. Med. Infect. Dis. 2020, 5, 59. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Prakash, S.; Khan, D.N.; Garg, R.K.; Kumar, R.; Bhagat, A.; Ramakrishna, V.; Jain, A. Aetiology of Acute Encephalitis Syndrome in Uttar Pradesh, India from 2014 to 2016. J. Vector Borne Dis. 2017, 54, 311–316. [Google Scholar] [CrossRef]
- Prabhakaran, A.; Lal, S.; Biswas, S.; Vinoth, S.; Asraf, A.S.; Mittal, V. Serological Study of Rickettsial Diseases in Human and Rodent Population in Chittoor Dist. (A.P.). J. Commun. Dis. 2010, 42, 209–213. [Google Scholar]
- Vinoth, S.; Prabhakaran, A.; Lal, S.; Murali, V.; Jayabalan, N. Outbreak of Scrub Typhus and Spotted Fever Group in Human and Rodent Populations in Kolar, South India. Arch. Clin. Microbiol. 2011, 2. [Google Scholar]
- Mittal, V.; Gupta, N.; Bhattacharya, D.; Kumar, K.; Ichhpujani, R.L.; Singh, S.; Chhabra, M.; Rana, U.V.S. Serological Evidence of Rickettsial Infections in Delhi. Indian J. Med. Res. 2012, 135, 538–541. [Google Scholar]
- Udayan, U.; Dias, M.; Machado, S. A Hospital Based Study of Rickettsial Diseases Evidenced by Weil Felix Test in a Tertiary Care Hospital. CHRISMED J. Health Res. 2014, 1, 150. [Google Scholar]
- Danave, D.; Kothadia, S.N. Role of Weil Felix Test for Rickettsial Infections. IOSR J. Dent. Med. Sci. 2015, 14, 52–54. [Google Scholar]
- Kg, R.K.; Tejashree, P.; Basavarajappa, K.G. Serological Evidence of Rickettsial Infections in and around Davangere. Int. J. Med. Sci. Public Health 2015, 4, 1731–1734. [Google Scholar] [CrossRef]
- Rashmi, K.S.; Murthy, N.S.; Ravikumar, K.L. Rickettsial Diseases: A Study Evidenced by Weil-Felix Test in a Tertiary Care Hospital. Int. J. Sci. Study 2015, 3, 128–131. [Google Scholar]
- Thomas, R.; Puranik, P.; Kalal, B.; Britto, C.; Kamalesh, S.; Rego, S.; Shet, A. Five-Year Analysis of Rickettsial Fevers in Children in South India: Clinical Manifestations and Complications. J. Infect. Dev. Ctries. 2016, 10, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Narvencar, K.; Kaur, G.; Rodrigues, S. Rickettsial Infections in Goa-Not Just Scrub Typhus! J. Assoc. Physicians India 2017, 65, 24–27. [Google Scholar] [PubMed]
- Sanap, S.S.; Thakur, V.A.; Maniar, J.M.; Vasave, S.V.; Vaidya, S.P. Weil-Felix Test—A Diagnostic Tool for Rickettsial Diseases. Austin J. Clin. Pathol. 2017, 4, 1046. Available online: https://austinpublishinggroup.com/clinical-pathology/fulltext/ajcp-v4-id1046.php (accessed on 10 August 2022).
- Goyal, P.K.; Babu, R.; Agarwal, S.; Behal, K.A.; Behal, K. Increasing Incidence of Rickettsial Infection in Patients of Pyrexia of Unknown Origin. J. Assoc. Physicians India 2018, 66, 46–48. [Google Scholar]
- Gautam, G.; Jais, M.; Prakash, A.; Pemde, H.K. Emerging Rickettsial Diseases: An Analysis of Undifferentiated Acute Febrile Illness Cases from a Tertiary Care Hospital in New Delhi. Int. J. Curr. Microbiol. Appl. Sci. 2019, 8, 463–471. [Google Scholar] [CrossRef]
- Kumar, S.; Aroor, S.; Kini, P.G.; Mundkur, S.; Gadiparthi, M. Clinical and Laboratory Features of Rickettsial Diseases in Children in South India. Pediatr. Oncall J. 2019, 16, 9–16. [Google Scholar] [CrossRef]
- Vijayalakshmi, J. Akshatha Prevalence of Rickettsial Infections in a Tertiary Care Centre. Ind. J. Microbiol. Res. 2020, 7, 6–9. [Google Scholar] [CrossRef]
- Mane, A.; Kamble, S.; Singh, M.K.; Ratnaparakhi, M.; Nirmalkar, A.; Gangakhedkar, R. Seroprevalence of Spotted Fever Group and Typhus Group Rickettsiae in Individuals with Acute Febrile Illness from Gorakhpur, India. Int. J. Infect. Dis. 2019, 79, 195–198. [Google Scholar] [CrossRef]
- Devamani, C.S.; Schmidt, W.-P.; Ariyoshi, K.; Anitha, A.; Kalaimani, S.; Prakash, J.A.J. Risk Factors for Scrub Typhus, Murine Typhus, and Spotted Fever Seropositivity in Urban Areas, Rural Plains, and Peri-Forest Hill Villages in South India: A Cross-Sectional Study. Am. J. Trop. Med. Hyg. 2020, 103, 238–248. [Google Scholar] [CrossRef]
- Mathai, E.; Lloyd, G.; Cherian, T.; Abraham, O.C.; Cherian, A.M. Serological Evidence for the Continued Presence of Human Rickettsioses in Southern India. Ann. Trop. Med. Parasitol. 2001, 95, 395–398. [Google Scholar] [CrossRef] [PubMed]
- Somashekar, H.R.; Moses, P.D.; Pavithran, S.; Mathew, L.G.; Agarwal, I.; Rolain, J.M.; Raoult, D.; Varghese, G.M.; Mathai, E. Magnitude and Features of Scrub Typhus and Spotted Fever in Children in India. J. Trop. Pediatr. 2006, 52, 228–229. [Google Scholar] [CrossRef] [PubMed]
- Chrispal, A.; Boorugu, H.; Gopinath, K.G.; Chandy, S.; Prakash, J.A.J.; Thomas, E.M.; Abraham, A.M.; Abraham, O.C.; Thomas, K. Acute Undifferentiated Febrile Illness in Adult Hospitalized Patients: The Disease Spectrum and Diagnostic Predictors—An Experience from a Tertiary Care Hospital in South India. Trop. Dr. 2010, 40, 230–234. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, K.G.; Chrispal, A.; Boorugu, H.; Chandy, S.; Prakash, J.J.; Abraham, A.M.; Abraham, O.C.; Thomas, K. Clinico-Epidemiological Profile of Seven Adults with Spotted Fever from a Tertiary Care Hospital in South India. Trop. Dr. 2014, 44, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Kalal, B.S.; Puranik, P.; Nagaraj, S.; Rego, S.; Shet, A. Scrub Typhus and Spotted Fever among Hospitalised Children in South India: Clinical Profile and Serological Epidemiology. Indian J. Med. Microbiol. 2016, 34, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Koralur, M.; Bairy, I.; Varma, M.; Athan, E.; Stenos, J. Spotted Fever Group and Typhus Fever Group Rickettsiosis in South Western India. Int. J. Infect. Dis. 2016, 45, 180–181. [Google Scholar] [CrossRef]
- Tripathi, C.D.P.; Singh, M.; Agarwal, J.; Kanta, C.; Atam, V. Seroepidemiology of Spotted Fever Rickettsiosis in Uttar Pradesh: A Prospective Study. J. Clin. Diagn. Res. 2017, 11, DC04–DC09. [Google Scholar] [CrossRef]
- Hegde, M.L.; Peerapur, B.V.; Shahapur, P.R. Serological Evidence of Spotted Fever Group Rickettsial Infection in North Karnataka Region. J. Adv. Pharm. Technol. Res. 2019, 12, 6024–6026. [Google Scholar] [CrossRef]
- Khan, S.A.; Bora, T.; Thangaraj, J.W.V.; Murhekar, M.V. Spotted Fever Group Rickettsiae among Children with Acute Febrile Illness, in Gorakhpur, India. J. Trop. Pediatr. 2021, 67, fmaa031. [Google Scholar] [CrossRef]
- Mansoor, T.; Fomda, B.A.; Koul, A.N.; Bhat, M.A.; Abdullah, N.; Bhattacharya, S.; Saleem, S.M. Rickettsial Infections among the Undifferentiated Febrile Patients Attending a Tertiary Care Teaching Hospital of Northern India: A Longitudinal Study. Infect. Chemother. 2021, 53, 96–106. [Google Scholar] [CrossRef]
- Schmidt, W.-P.; Devamani, C.S.; Elangovan, D.; Alexander, N.; Rose, W.; Prakash, J.A.J. Clinical Characteristics of and Antibody Response to Spotted Fever Group Rickettsial Infections in South India: Case Series and Serological Cohort Study. Trop. Med. Int. Health 2021, 26, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Rathi, N.B.; Rathi, A.N.; Goodman, M.H.; Aghai, Z.H. Rickettsial Diseases in Central India: Proposed Clinical Scoring System for Early Detection of Spotted Fever. Indian Pediatr. 2011, 48, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Chahota, R.; Thakur, S.D.; Sharma, M.; Mittra, S. Detection of Flea-Borne Rickettsia Species in the Western Himalayan Region of India. Indian J. Med. Microbiol. 2015, 33, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Bora, T.; Chattopadhyay, S.; Jiang, J.; Richards, A.L.; Dutta, P. Seroepidemiology of Rickettsial Infections in Northeast India. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 487–494. [Google Scholar] [CrossRef]
- Dincy, P.C.; Susanne, P.A.; Leni, G.; Sohanlal, S.; Meera, T.; Aj, P.J. Clinicopathological Study on Rickettsial Spotted Fever from South India. Trop. Dr. 2018, 48, 325–329. [Google Scholar] [CrossRef]
- Mittal, M.; Bondre, V.; Murhekar, M.; Deval, H.; Rose, W.; Verghese, V.P.; Mittal, M.; Patil, G.; Sabarinathan, R.; Vivian Thangaraj, J.W.; et al. Acute Encephalitis Syndrome in Gorakhpur, Uttar Pradesh, 2016: Clinical and Laboratory Findings. Pediatr. Infect. Dis. J. 2018, 37, 1101. [Google Scholar] [CrossRef]
- Mohammed Shahid, S.; Sirwar, S.B.; Vijayaraghavan, R. A Study on Rickettsial Infections and Its Isolation by Serological and Molecular Methods. Res. J. Pharm. Technol. 2019, 12, 3687–3689. [Google Scholar] [CrossRef]
- Khan, S.A.; Bora, T.; Saikia, J.; Shah, A.; Richards, A.L.; Chattopadhyay, S.; Kakati, S.; Rahi, M.; Kaur, H. Seroprevalence of Typhus Group Rickettsial Infections in the North-East Region of India. Indian J. Med. Res. 2019, 150, 203–205. [Google Scholar] [CrossRef]
- Biswal, M.; Zaman, K.; Suri, V.; Gopi, S.; Kumar, A.; Gopi, T.; Vig, S.; Sharma, N.; Bhalla, A. Molecular Confirmation & Characterization of Rickettsia Conorii in North India: A Report of Three Cases. Indian J. Med. Res. 2020, 151, 59–64. [Google Scholar]
- Elangovan, D.; Perumalla, S.; Gunasekaran, K.; Rose, W.; Verghese, V.P.; Abhilash, K.P.; Jaj, P.; Dumler, J.S. Spotted Fever Diagnosis: Experience from a South Indian Center. Pathog. Glob. Health 2021, 115, 300–306. [Google Scholar]
- Kumar, K.; Jain, S.K.; Kumar, A. Outbreak Indian Tick Typhus amongst Residents of Deol Village, District, Kangra, Himachal Pradesh (INDIA). Int. J. Med. Public Health 2011, 1, 67–71. [Google Scholar] [CrossRef]
- Hii, S.-F.; Lawrence, A.L.; Cuttell, L.; Tynas, R.; Abd Rani, P.A.M.; Šlapeta, J.; Traub, R.J. Evidence for a Specific Host-Endosymbiont Relationship between “Rickettsia Sp. Genotype RF2125” and Ctenocephalides Felis Orientis Infesting Dogs in India. Parasit. Vectors 2015, 8, 169. [Google Scholar] [CrossRef] [PubMed]
- Bhuyan, P.J.; Nath, A.J. Record of Tropical Rat Mite, Ornithonyssus Bacoti (Acari: Mesostigmata: Macronyssidae) from Domestic and Peridomestic Rodents (Rattus Rattus) in Nilgiris, Tamil Nadu, India. J. Arthropod Borne Dis. 2016, 10, 98–101. [Google Scholar] [PubMed]
- Nimisha, M.; Devassy, J.K.; Pradeep, R.K.; Pakideery, V.; Sruthi, M.K.; Pious, A.; Kurbet, P.S.; Amrutha, B.M.; Chandrasekhar, L.; Deepa, C.K.; et al. Ticks and Accompanying Pathogens of Domestic and Wild Animals of Kerala, South India. Exp. Appl. Acarol. 2019, 79, 137–155. [Google Scholar] [CrossRef]
- Nataraj, N.; Muthuraman, K.; Sundaram, D.; Ayyanar, E.; Ashokkumar, M.; Kasinathan, G.; Devaraju, P. Molecular Detection of Candidatus Rickettsia Asembonensis in Fleas Collected from Pets and Domestic Animals in Puducherry, India. Med. Vet. Entomol. 2020, 34, 498–502. [Google Scholar] [CrossRef]
- Stewart, A.G.; Stewart, A.G.A. An Update on the Laboratory Diagnosis of Rickettsia Spp. Infection. Pathogens 2021, 10, 1319. [Google Scholar] [CrossRef]
- Fournier, P.-E.; Dumler, J.S.; Greub, G.; Zhang, J.; Wu, Y.; Raoult, D. Gene Sequence-Based Criteria for Identification of New Rickettsia Isolates and Description of Rickettsia Heilongjiangensis sp. Nov. J. Clin. Microbiol. 2003, 41, 5456–5465. [Google Scholar] [CrossRef]
- Weinberger, M.; Keysary, A.; Sandbank, J.; Zaidenstein, R.; Itzhaki, A.; Strenger, C.; Leitner, M.; Paddock, C.D.; Eremeeva, M.E. Fatal Rickettsia Conorii Subsp. Israelensis Infection, Israel. Emerg. Infect. Dis. 2008, 14, 821–824. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Babushkin, F.; Shapiro, M.; Uda, M.; Atiya-Nasagi, Y.; Finn, T. Case Report: Typhoid Fever and Spotted Fever Group Rickettsiosis Presenting Concomitantly in an Indian Immigrant. Am. J. Trop. Med. Hyg. 2018, 99, 864–866. [Google Scholar] [CrossRef]
- Takajo, I.; Sekizuka, T.; Fujita, H.; Kawano, A.; Kawaguchi, T.; Matsuda, M.; Kubo, K.; Miyauchi, S.; Umekita, K.; Nagatomo, Y.; et al. Possible Case of Novel Spotted Fever Group Rickettsiosis in Traveler Returning to Japan from India. Emerg. Infect. Dis. 2016, 22, 1079–1082. [Google Scholar] [CrossRef]
- Binder, W.D.; Gupta, R. African Tick-Bite Fever in a Returning Traveler. J. Emerg. Med. 2015, 48, 562–565. [Google Scholar] [CrossRef] [PubMed]
- Hecht, A.; Seilmaier, M.; Guggemos, W.; Löscher, T. Gastroenteritis with fever, headache and rash after travelling in India. Internist 2011, 52, 590–594. [Google Scholar] [CrossRef]
- Hassan, I.S.; Ong, E.L. Fever in the Returned Traveller. Remember Murine Typhus! J. Infect. 1995, 31, 173–174. [Google Scholar] [CrossRef]
- Wilson, M.E.; Brush, A.D.; Meany, M.C. Murine Typhus Acquired during Short-Term Urban Travel. Am. J. Med. 1989, 87, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Nagar, G. Problem of Ticks and Tick-Borne Diseases in India with Special Emphasis on Progress in Tick Control Research: A Review. J. Vector Borne Dis. 2014, 51, 259–270. [Google Scholar]
- Nigwekar, P.; Kavar, Y.; Shrikhande, D.; Kumar, C. Clinico-Pathological Profile of Rickettsial Fever in a Rural Area of Western Maharashtra, India. Pravara Med. Rev. 2014, 5, 5–9. [Google Scholar]
- Sundhindra, B.K.; Vijayakumar, S.; Kutty, K.A.; Tholpadi, S.R.; Rajan, R.S.; Mathai, E.; Raoult, D.M.; John, T.J. Rickettsial Spotted Fever in Kerala. Natl. Med. J. India 2004, 17, 51–52. [Google Scholar] [PubMed]
- Rathi, N.; Maheshwari, M.; Khandelwal, R. Neurological Manifestations of Rickettsial Infections in Children. Pediatr. Infect. Dis. 2015, 7, 64–66. [Google Scholar] [CrossRef]
- Chugh, S.; Kumari, P.; Goel, S.; Biswal, M.; Sehgal, I.S.; Sekar, A. Rickettsia Conorii Infection with Fatal Complication. Autops. Case Rep. 2022, 12, e2021392. [Google Scholar] [CrossRef] [PubMed]
- Balasundaram, M.B.; Manjunath, M.; Baliga, G.; Kapadi, F. Ocular Manifestations of Rickettsia Conorii in South India. Indian J. Ophthalmol. 2018, 66, 1840–1844. [Google Scholar] [CrossRef]
- Kawali, A.; Mahendradas, P.; Mohan, A.; Mallavarapu, M.; Shetty, B. Epidemic Retinitis. Ocul. Immunol. Inflamm. 2019, 27, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Chawla, R.; Pundlik, G.A.; Chaudhry, R.; Thakur, C. Rickettsial Retinitis: Direct Bacterial Infection or an Immune-Mediated Response? Indian J. Ophthalmol. 2017, 65, 1038–1041. [Google Scholar] [PubMed]
- Shanmugam, M.; Konana, V.K.; Ramanjulu, R.; Divyansh Mishra, K.C.; Sagar, P.; Kumar, D. Optical Coherence Tomography Angiography Features of Retinitis Post-Rickettsial Fever. Indian J. Ophthalmol. 2019, 67, 297–300. [Google Scholar] [CrossRef]
- Babu, K.; Sudheer, B.; Murthy, K.R. Bilateral Arterial Occlusions Masking Retinitis in a HIV-Positive Male. Indian J. Ophthalmol. 2018, 66, 332–334. [Google Scholar] [CrossRef]
- Das, S.; Ninan, G.A.; Jasper, S.; George, M.; Iyadurai, R. Spotted Fever Rickettsiosis Presenting with Bilateral Anterior Uveitis and Retinitis: A Case Report. J. Fam. Med. Prim. Care 2020, 9, 1236–1239. [Google Scholar] [CrossRef]
- Rajadhyaksha, A.; Phatak, S.; Nolkha, N.; Pathan, Y.; Sonawale, A. Rickettsial Fever Presenting with Isolated Third Nerve Palsy. J. Assoc. Physicians India 2013, 61, 144–145. [Google Scholar] [PubMed]
- Chikkanna, S.; Ramabhatta, S.; Kumar, M.; Dhatri, K. Fundus Examination: A Key to Spot the Spotted Fever! Indian J. Pediatr. 2016, 83, 1020–1021. [Google Scholar] [CrossRef] [PubMed]
- Rama Prasad, G.S.; Mekala, S.; Gadagani, N. A Rare Case of Rickettsial Infection Presented as Febrile Delirium in a 4 Years Old Child from a Government Hospital, Andhra Pradesh, India. J. Dr. NTR Univ. Health Sci. 2019, 8, 272. [Google Scholar]
- Jayaseelan, E.; Rajendran, S.C.; Shariff, S.; Fishbein, D.; Keystone, J.S. Cutaneous Eruptions in Indian Tick Typhus. Int. J. Dermatol. 1991, 30, 790–794. [Google Scholar] [CrossRef]
- Katoch, S.; Kallappa, R.; Shamanur, M.B.; Gandhi, S. Purpura Fulminans Secondary to Rickettsial Infections: A Case Series. Indian Dermatol. Online J. 2016, 7, 24–28. [Google Scholar]
- Prabhakar, U.; Singh, A. Atypical Presentation of Rickettsial Spotted Fever. J. Ayub Med. Coll. Abbottabad 2017, 29, 692–693. [Google Scholar] [PubMed]
- Hulmani, M.; Alekya, P.; Kumar, V.J. Indian Tick Typhus Presenting as Purpura Fulminans with Review on Rickettsial Infections. Indian J. Dermatol. 2017, 62, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tirumala, S.; Behera, B.; Jawalkar, S.; Mishra, P.K.; Patalay, P.V.; Ayyagari, S.; Nimmala, P. Scrub Typhus Presenting as Purpura Fulminans. Indian J. Crit. Care Med. 2014, 18, 476–478. [Google Scholar] [PubMed]
- Kundavaram, A.; Francis, N.R.; Jude, A.P.J.; Varghese, G.N. Acute Infectious Purpura Fulminans due to Probable Spotted Fever. J. Postgrad. Med. 2014, 60, 198–199. [Google Scholar] [CrossRef]
- Joshi, H.S.; Thomas, M.; Warrier, A.; Kumar, S. Gangrene in Cases of Spotted Fever: A Report of Three Cases. BMJ Case Rep. BMJ Case Rep. 2012, 2012, bcr2012007295. [Google Scholar] [CrossRef]
- Kumar, M.; Singh, R.; Yadav, M. Indian Tick Typhus Presenting with Gangrene: A Case Report from an Urban Slum of Delhi. Indian J. Pediatr. 2014, 81, 95–97. [Google Scholar] [CrossRef]
- Lunge, S.B.; Patil, V.; Ambar, S.; Naik, V. Malignant Mediterranean Spotted Fever. Indian Dermatol. Online J. 2015, 6, S1–S4. [Google Scholar]
- Goyal, T.; Varshney, A.; Bakshi, S.K.; Mittal, V. Malignant Mediterranean Spotted Fever in the Setting of Diabetes Mellitus: An Uncommon Cutaneous Entity. Community Acquir. Infect. 2014, 1, 29. [Google Scholar] [CrossRef]
- Gupta, R.; Singh, V. Indian Tick Typhus—An Uncommon Cause of Hepatitis: A Case Report. J. Clin. Diagn. Res. 2014, 8, MD01–MD02. [Google Scholar] [CrossRef]
- Patil, H.B.; Shahapur, P.; Bidari, L.H. Myocarditis and Rickettsia Conorii Infection. Pediatr. Oncall 2010, 7, 108–109. [Google Scholar]
- Salje, J.; Weitzel, T.; Newton, P.N.; Varghese, G.M.; Day, N. Rickettsial Infections: A Blind Spot in Our View of Neglected Tropical Diseases. PLoS Negl. Trop. Dis. 2021, 15, e0009353. [Google Scholar] [CrossRef] [PubMed]
- Fournier, P.-E.; Zhu, Y.; Ogata, H.; Raoult, D. Use of Highly Variable Intergenic Spacer Sequences for Multispacer Typing of Rickettsia Conorii Strains. J. Clin. Microbiol. 2004, 42, 5757–5766. [Google Scholar] [CrossRef] [PubMed]
- Dzelalija, B.; Punda-Polic, V.; Medic, A.; Dobec, M. Rickettsiae and Rickettsial Diseases in Croatia: Implications for Travel Medicine. Travel Med. Infect. Dis. 2016, 14, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Minahan, N.T.; Chao, C.-C.; Tsai, K.-H. The Re-Emergence and Emergence of Vector-Borne Rickettsioses in Taiwan. Trop. Med. Infect. Dis. 2018, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Trung, N.V.; Hoi, L.T.; Hoa, T.M.; Huong, D.T.; Huyen, M.T.; Tien, V.Q.; Mai, D.T.T.; Ha, N.T.T.; Kinh, N.V.; Farris, C.M.; et al. Systematic Surveillance of Rickettsial Diseases in 27 Hospitals from 26 Provinces throughout Vietnam. Trop. Med. Infect. Dis. 2022, 7, 88. [Google Scholar] [CrossRef]
- Tshokey, T.; Stenos, J.; Durrheim, D.N.; Eastwood, K.; Nguyen, C.; Vincent, G.; Graves, S.R. Rickettsial Infections and Q Fever Amongst Febrile Patients in Bhutan. Trop. Med. Infect. Dis. 2018, 3, 12. [Google Scholar] [CrossRef]
- Yuhana, M.Y.; Hanboonkunupakarn, B.; Tanganuchitcharnchai, A.; Sujariyakul, P.; Sonthayanon, P.; Chotivanich, K.; Pukrittayakamee, S.; Blacksell, S.D.; Paris, D.H. Rickettsial Infections Are Neglected Causes of Acute Febrile Illness in Teluk Intan, Peninsular Malaysia. Trop. Med. Infect. Dis. 2022, 7, 77. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Region | Study Details | RD (%) | SFGR (%) | TGR (%) | Undifferentiated Rickettsioses (%) |
|---|---|---|---|---|---|---|
| Kamarasu et al., 2007 [7] | South India (Tamil Nadu) | 964 prospective samples over 2 years in various PHCs | 4.6 | ND | ND | ND |
| Prabhakaran et al., 2010 [15] | South India (Andhra Pradesh) | 39 prospective patients of fever with rash | 7.7 | 0 | 0 | 7.7 |
| Vinoth et al., 2011 [16] | South India (Karnataka) | 200 suspected outbreak patients | 9 | 4 | 0 | 5 |
| Mittal et al., 2012 [17] | North India (New Delhi) | 824 prospective samples [737 (initial 5 years) and 87 in subsequent 5 years] | 5.2 | 3.9 | 0.8 | 0.5 |
| Udayan et al., 2014 [18] | South India (Karnataka) | 100 prospective febrile patients | 55 | 45 | 10 | 4 |
| Danave et al., 2015 [19] | West India (Maharashtra) | 156 prospective febrile patients | 15 | 3.8 | 0 | 11.5 |
| Kumar et al., 2015 [20] | South India (Karnataka) | 60 prospective PUO patients | 5 | 1.7 | 1.7 | 1.7 |
| Rashmi et al., 2015 [21] | South India (Karnataka) | 133 prospective AUFI patients | 44.8 | 10.3 | 6.8 | 27.6 |
| Thomas et al., 2016 [22] | South India (Karnataka, Andhra Pradesh and Tamil Nadu) | 262 children of suspected rickettsial infection (Retrospective) | 20 | ND | ND | ND |
| Narvencar et al., 2017 [23] | West India (Goa) | 55 prospective AUFI patients | 20 | 16.4 | 3.6 | 1.8 |
| Sanap et al., 2017 [24] | West India (Maharashtra) | 1464 prospective PUO patients | 10.1 | 4.6 | 3.5 | 2.1 |
| Goyal et al., 2018 [25] | North India (New Delhi) | 22 prospective PUO patients | 41 | 27.3 | 13.6 | 13.6 |
| Gautam et al., 2019 [26] | North India (New Delhi) | 370 prospective AUFI patients | 5.1 | 3.8 | 1.4 | ND |
| Kumar et al., 2019 [27] | South India (Karnataka) | 324 prospective samples from children with fever | 9.2 | 1.5 | 7.7 | 1.5 |
| Akshatha et al., 2020 [28] | South India (Andhra Pradesh) | 120 prospective samples from febrile patients | 21 | ND | ND | 20.8 |
| Kavirayani et al., 2021 [8] | South India (Karnataka) | 214 AFI patients | 7.1 | ND | ND | ND |
| Author | Region | Study Details | Diagnostic Methods Used | Results |
|---|---|---|---|---|
| Cross-sectional studies | ||||
| Kalra et al., 1951 [3] | North India (Kashmir) | 178 endemic patients | 53 patients tested for WFT and CFT | WFT = TGR—90.6% (47); SFGR—1.9% (1) CFT = Murine typhus—70% (37); 11—Epidemic typhus—20.8% (11); 5—non reactive |
| Mane et al., 2019 [29] | Central India (Gorakhpur, Uttar Pradesh) | 329 AFI patients (294 samples) | R. conorii IgG/IgM ELISA kit R. typhi IgG/IgM ELISA | SFGR = IgM—13.6% (40)/IgG—36.7% (108); TGR = IgM—7.1% (21), IgG—15.3% (45); undifferentiated rickettsioses = 1.4% (4) (total 218 case) |
| Devamani et al., 2020 [30] | South India (Tamil Nadu) | 1353 samples | IgG ELISA for SFG/TG | IgG ELISA—15.8% (10.4% SFGR and 5.4% TGR rickettsioses) |
| Khan et al., 2021 [6] | Northeast India (Assam, Meghalaya, Tripura) | 2360 samples; (772—Assam 768—Meghalaya 820—Tripura) | IgG ELISA for SFG/TG | Overall—1.8% (1.4% SFGR and 0.3% TGR) Assam—1.4% (1.2% SFGR and 0.2% TGR) Meghalaya—0.5% (0.3% SFGR and 0.2% TGR) Tripura—2.9% (2.4% SFGR and 0.5% TGR) |
| Prospective studies (In defined population) | ||||
| Murali et al., 2001 [11] | South India (Tamil Nadu) | 57 children of fever with rash | WFT, immuno haemagglutination (IHA; in 4 patients) | WFT = 21% (12); SFGR—7% (4), TGR—10.5% (6), undifferentiated rickettsioses—3.5% (2); IHA = SFGR—3/4, TGR—1/4) |
| Mathai et al., 2001 [31] | South India (Tamil Nadu) | 475 PUO patients | WFT, indirect haemagglutination assay (RBC sensitised with R. typhi, R. rickettsii antigens) | SFGR—1.3% (6), TGR—1.3% (6); (Total—2.6%) |
| Somashekar et al., 2005 [32] | South India (Tamil Nadu) | 180 children with PUO | WFT, ELISA or microIFA | 43 patients of RDs; 15 non scrub typhus patients; TGR—1.1% (2), SFGR—7.8% (14) |
| Kulkarni et al., 2009 [10] | West India (Maharashtra) | 156 PICU patients suspected with RDs | WFT, SFGR ELISA in 26 patients, IFA in CDC for 2 patients | WFT positive in 73 patients and SFGR was predominant; ELISA = SFGR—13.5% (80.8%; 21/26); IFA = 2 patients R. conorii |
| Chrispal et al., 2010 [33] | South India (Tamil Nadu) | 398 AFI in patients | SF IgM ELISA | ELISA = SFGR—1.8% (7) |
| Gopinath et al., 2014 [34] | South India (Vellore, Tamil Nadu) | 398 AUFI in adult with SFGR defined patients | SF IgM ELISA | ELISA = SFGR—1.76% (7) |
| Kalal et al., 2016 [35] | South India (Karnataka, Andhra Pradesh and Tamil Nadu) | 103 children with suspected Rickettsial disease | ELISA (R. conorii IgM/IgG kit), WFT | ELISA = SFGR—37.1% (23); WFT = 44.4% (4) of ELISA positive patients |
| Koralur et al., 2016 [36] | South India (Karnataka) | 1036 patients with suspected RDs | WFT, IFA | IFA= SFGR—2.1% (22); TGR—1.8% (19) (Cross reactions; 18 patients were positive for Rickettsia australis, 16 for Rickettsia honei, 15 for R. conorii, 16 for Rickettsia africae, 15 for Rickettsia rickettsii, 11 for Rickettsia felis, 4 for Rickettsia prowazekii and 6 patients for R. typhi) |
| Tripathi et al., 2017 [37] | Central India (Uttar Pradesh) | 432 PUO patients | WFT, ELISA for specific IgM antibody against R. conorii and IFA for IgM antibody against R. conorii/R. typhi | WFT = 46.3% (200); ELISA and IFA = 26.6% (115) |
| Stephen et al., 2018 [9] | South India (Puducherry) | 320 clinically defined patients for RDs | WFT, SFG specific R. conorii IgM/IgG ELISA | 21.3% (68 patients) by WFT; 11.6% (37) by ELISA; 142 SFGR by all test (44.4%); |
| Shriharsha et al., 2019 [38] | South India (Karnataka) | 231 AFI patients | WFT, R. conorii IgG/IgM ELISA | WFT = 36.3% SFGR; 2.1% TGR; 6.9% undifferentiated rickettsioses IgG ELISA—11.7% SFGR |
| Khan et al., 2021 [39] | Central India (Gorakhpur, Uttar Pradesh) | 217 children with AFI | IgG ELISA for SFGR/TGR | IgG ELISA—6% SFGR (13 children) and 0% TGR |
| Mansoor et al., 2021 [40] | North India (Srinagar) | 344 AUFI patients | WFT, ELISA, IFA | WFT = 3.5% (12) non-scrub typhus RDs patients (2.3% SFGR; 1.2% TGR); IgM/IgG TGR ELISA—8.1% (28/344); IgM/IgG SFGR ELISA—10.5% (36/344); IFA—8.2% (4.7% SFGR and 3.5% TGR) |
| Schmidt et al., 2021 [41] | South India (Vellore, Tamil Nadu) | 77 AUFI patients | IgM/IgG ELISA for SFGR | All 77 IgG/IgM SFGR positive cases enrolled- IgM/IgG response over time |
| Retrospective studies (In defined population) | ||||
| Rathi et al., 2011 [42] | West India (Maharashtra) | 161 children with RD defined patients | SFGR IgM ELISA, WFT, IFA IgM for SFGR | 52 patients SFGR (70%) among 75 RDs ELISA = SFGR—32.3% (47) (10 of ELISA positive were tested for IFA—all positive) |
| Author | Region | Total Study Population | Diagnostic Methods Used | Results | Most Closely Related Pathogens based on Submitted Sequence in NCBI GenBank. |
|---|---|---|---|---|---|
| Prakash et al., 2012 [12] | South India (Vellore, Tamil Nadu) | 58 patients of suspected SFGR fever with rash sample | IgM ELISA in serum, nPCR (targeted gltA, ompA, ompB, 17kDa genes) in skin biopsy | 34 cases PCR confirmed (58.6%), 27/34—ELISA positive | Rickettsia parkeri, Rickettsia africae, Rickettsia sibirica, Rickettsia mongolotimonae, Rickettsia japonica, Rickettsia honei, Rickettsia rickettsii, R. conorii, Rickettsia spp. IG-1, Candidatus Rickettsia kellyi, Rickettsia slovaca |
| Chahota et al., 2015 [43] | North India (Himachal Pradesh) | Clusters of 300 fever patients from 3 villages | WFT, PCR (targeted gltA and ompB gene) in blood | 7 WFT positive cases tested (2.3) with PCR which were negative | No PCR positive |
| Khan et al., 2016 [44] | Northeast India (Assam, Arunachal Pradesh and Nagaland) | 1265 random samples of residents of scrub typhus endemic region. | indirect ELISA, PCR (targeted gltA and ompB gene) in seropositive serum samples | SFGR—175 (13.8%) TGR—53 (4.2%) PCR—nil | No PCR positive |
| Dincy et al., 2018 [45] | South India (Vellore, Tamil Nadu) | 30 of 35 clinically defined patients | PCR (targeted gltA, ompA, ompB, 17kDa genes) in biopsy from rash and ELISA in serum, HPE of skin biopsy of rashes | 30 cases PCR and /or ELISA | No sequence data available |
| Mittal et al., 2018 [46] | Central India (Gorakhpur, Uttar Pradesh) | 389 AES patients | PCR for SFGR in CSF and/or Serum sample (targeted IGS 23S-5S region), in brain biopsy sample (targeting ompA) | 4 (1%) from CSF or Serum, 1 positive from brain biopsy | No sequence data available |
| Shahid et al., 2019 [47] | South India (Karnataka) | 262 AFI blood samples | WFT, PCR (targeted gltA gene) in whole blood | WFT—116 (44.3%), gltA PCR—69/116 cases (59.5%) | No sequence data available |
| Khan et al., 2019 [48] | Northeast India (Assam, Arunachal Pradesh, Nagaland, Manipur, Mizoram, Meghalaya and Tripura) | 2199 (762 AES patients; 1437 PUO patients) | ELISA (Antibody against TGR), snPCR (targeted 17kDa gene) in serum samples | ELISA for TGR: 30/762; 3.9% among AES, 39/1437; 2.7% among PUO (Assam—0, Arunachal Pradesh—0, Nagaland—2.2%, Manipur—3.8%, Mizoram—2%, Meghalaya—0 and Tripura—6.3%) PCR—No positive among 15 ELISA positive sample | No PCR positive |
| Biswal et al., 2020 [49] | North India (Chandigarh) | 51 patients of PUO | nPCR (targeted ompA gene) in clot sample | 3 cases of R. conorii (5.8%) | R. conorii clone 09 (KR401144) and R. conorii subsp. conorii clone 45 (JN182802) |
| Biswal et al., 2020 [13] | North India (Chandigarh) | 200 patients of AUFI | nPCR (targeted gltA gene) in clot sample | 7% (14 cases), SFGR -4%, TGR-3% | Rickettsia conorii and Rickettsia typhi |
| Elangovan et al., 2021 [50] | South India (Vellore, Tamil Nadu) | 175 patients of suspected SFGR with fever and rash | IgM ELISA in serum, nPCR (targeted gltA, ompA genes) in buffy coat | 50% (48 SFGR cases; 48/96 by either by PCR or ELISA; 22%—21/96 by PCR; 28%—27/96 by ELISA) | Uncultured Rickettsia sp. Clone cmc 08 (GQ260637), Rickettsia sp. Tenjiku01 (LC089864), Rickettsia raoulti (KR131756) and Rickettsia parkeri (CP040325) |
| Author | Region | Host | Vector | Rickettsiae |
|---|---|---|---|---|
| Kumar et al., 2011 [51] | North India (Kangra) | Domestic ruminants, Rodents | Ticks (Ixodes ricinus, Rhipicephalus sanguenieussanguineus) | ND |
| Vinoth et al., 2011 [16] | South India (Kolar) | Rodents | ND | 1 Proteus OX-2 positive |
| Chahota et al., 2015 [43] | North India (Himalayan Region) | Rodents | Rat flea (Ceratophyllus fasciatus) | Rickettsia sp. R14 |
| Hii et al., 2015 [52] | West India (Mumbai), North India (Delhi & Rajasthan) | Stray dogs | Cat flea (Ctenocephalides felis Orientis—89.6%, Ctenocephalides felis felis—10.4%) | Rickettsia sp. genotype RF2125 |
| Khan et al., 2016 [44] | Northeast India (Assam) | Dog, cattle, cats | Cat fleas (Ctenocephalides felis) | Candidatus Rickettsia senegalensis |
| Bhuyan et al., 2016 [53] | South India (Nilgiris, Tamil Nadu) | Domestic and peri-domestic rats | Ornithonyssus bacoti | ND |
| Nimisha et al., 2019 [54] | South India (Kerala) | Domestic ruminants (cattle and goats) and wild animals (sambar deer and elephant calf) | Rhipicephalus haemaphysaloides, Haemaphysalis bispinosa, Amblyomma sp. | Rickettsia massiliae, Rickettsia slovaca, Rickettsia raoultii, Rickettsia africae |
| Nataraj et al., 2020 [55] | South India (Puducherry) | Pets (dogs) and domestic ruminants (buffaloes, cattle, and goats) | Cat fleas (Ctenocephalides felis felis) | Rickettsia asembonensis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krishnamoorthi, S.; Goel, S.; Kaur, J.; Bisht, K.; Biswal, M. A Review of Rickettsial Diseases Other Than Scrub Typhus in India. Trop. Med. Infect. Dis. 2023, 8, 280. https://doi.org/10.3390/tropicalmed8050280
Krishnamoorthi S, Goel S, Kaur J, Bisht K, Biswal M. A Review of Rickettsial Diseases Other Than Scrub Typhus in India. Tropical Medicine and Infectious Disease. 2023; 8(5):280. https://doi.org/10.3390/tropicalmed8050280
Chicago/Turabian StyleKrishnamoorthi, Sivanantham, Shriya Goel, Jasleen Kaur, Kamlesh Bisht, and Manisha Biswal. 2023. "A Review of Rickettsial Diseases Other Than Scrub Typhus in India" Tropical Medicine and Infectious Disease 8, no. 5: 280. https://doi.org/10.3390/tropicalmed8050280
APA StyleKrishnamoorthi, S., Goel, S., Kaur, J., Bisht, K., & Biswal, M. (2023). A Review of Rickettsial Diseases Other Than Scrub Typhus in India. Tropical Medicine and Infectious Disease, 8(5), 280. https://doi.org/10.3390/tropicalmed8050280