Abstract
North-west Syria (NWS) is a conflict-affected and unstable area. Due to its limited health infrastructure, accessing advanced COVID-19 testing services is challenging. COVID-19 antigen rapid diagnostic tests (Ag-RDTs) have the potential to overcome this barrier. A pilot project was implemented to introduce Ag-RDTs in NWS, aiming to determine the feasibility, uptake, and results of Ag-RDTs and identify facilitators and barriers to testing with Ag-RDTs. A cross-sectional study design involving secondary analysis of data collected during the project was employed. A local non-governmental organization implemented 25,000 Ag-RDTs that were conducted cross-border by trained community health workers. In total, 27,888 eligible individuals were enrolled, 24,956 (89.5%) consented to test, and 121 (0.5%) were COVID-19-positive. The highest positivity was observed among those with severe COVID-19 symptoms (12.7%), with respiratory illnesses (2.5%), enrolled at hospitals in Afrin (2.5%), and healthcare workers (1.9%). A non-random sample of 236 individuals underwent confirmatory RT-PCR testing. Observed sensitivity, specificity, and positive and negative predictive values were 80.0%, 96.1%, 91.4%, and 90.3%, respectively. Challenges included obtaining informed consent and conducting confirmatory testing. Ag-RDTs represent a feasible screening/diagnostic tool for COVID-19 infections in NWS, with nearly 90% uptake. Embedding Ag-RDTs into COVID-19 testing and screening strategies would be highly beneficial.
1. Introduction
The Middle East and North Africa (MENA) countries experienced high morbidity and mortality during the COVID-19 pandemic, with more than 18 million individuals infected and over 750,000 deaths [1]. The pandemic led to a considerable burden on the health systems of MENA countries that cater to refugees and migrants, leading to inadequate diagnostic testing. This has resulted in refugees and migrants experiencing disproportionately limited access to COVID-19 testing [2,3]. Therefore, it is likely that the number of people infected and deaths due to COVID-19 were higher than reported [4].
North-west Syria (NWS), with a population of 4.6 million, is one of the world’s most politically unstable geographical areas. Nearly 2.9 million people in this area comprise internally displaced populations (IDPs) due to war. This population has faced several challenges in accessing COVID-19 testing services due to deficiencies in the health infrastructure [5,6]. However, there is minimal scientific evidence about the barriers to COVID-19 testing in this setting [5]. Studies from neighboring countries have highlighted that displaced populations face financial burdens and fear of stigma, discrimination, and isolation while undergoing COVID-19 tests [6]. In addition, these studies indicate that the pandemic was mainly viewed by refugees as “overestimated”, and many hold conspiracy theory beliefs that have affected the uptake of COVID-19 testing in these populations [6,7].
Antigen rapid diagnostic tests (Ag-RDTs) are easy to perform, require minimal resources and infrastructure, can yield results in just 15 to 20 min, and are cheaper than molecular reverse transcription polymerase chain reaction (RT-PCR)-based tests [8]. Although they are more accurate than Ag-RDTs, RT-PCR tests require advanced resources and infrastructure [9]. Nevertheless, Ag-RDTs can have high diagnostic utility in tackling the spread of COVID-19, especially during the first seven days of symptom onset [10]. Thus, they can be effective in settings with limited access to RT-PCR testing.
In this context, the International Organization for Migration (IOM), in collaboration with the Foundation for Innovative New Diagnostics (FIND [11], implemented a pilot project for assessing the feasibility of using Ag-RDTs in NWS. This pilot project aimed to facilitate easy access to COVID-19 testing and to understand the barriers to and best practices for diagnostic testing in this displaced population setting. The pilot project was implemented in NWS in partnership with a local non-governmental organization—Hand in Hand for Aid and Development (HiHFAD)—and involved the distribution and use of 25,000 Ag-RDTs at health facilities, refugee camps, informal tented settlements, and in outreach settings.
As part of this pilot project, operational research was undertaken to document the experience of implementing Ag-RDTs in NWS. The main objectives were to (a) determine the feasibility of conducting Ag-RDTs within camps and health facilities; (b) determine the willingness of eligible participants to accept Ag-RDTs; (c) describe the results of the Ag-RDTs; (d) identify the enablers and barriers to the use of Ag-RDTs in these settings from the perspective of the healthcare workers who were involved in conducting these tests within NWS.
2. Materials and Methods
2.1. Study Design
This cross-sectional study involved secondary analysis of data collected as part of the pilot project’s recording, reporting, and monitoring processes.
2.2. Study Population Settings
As of 2023, the population of NWS is estimated to be around 4.6 million people [12]. The number of individuals needing humanitarian assistance in NWS increased from 3.4 to 4.1 million between 2021 and 2022. Women and children make up 80% of NWS’s population [13]. About 2.9 million people in NWS are IDPs, and the majority are food insecure, with more than 3 million of these individuals unable to meet their basic needs [12,13]. In addition, as of December 2022, the latest health updates in NWS suggest there are continuing large increases in daily COVID-19 cases, with a limited humanitarian response [14,15].
2.3. Ag-RDT Project Settings
The Ag-RDT project was implemented between September and November 2022 in various camps, mobile clinics, and health facilities in three districts within NWS: Afrin, Idleb, and Jarablus/Albab. The Ag-RDT used was the World Health Organization (WHO)-prequalified Sure Status COVID-19 Antigen Card Test® (professional version), manufactured by Premier Medical Corporation (PMC) India, which has a ‘manufacturer reported’ sensitivity of 94.16% and specificity of 100%. An implementing partner organization, HiHFAD, was involved in distributing the Ag-RDTs within the study districts. HiHFAD deployed 48 community health workers (CHWs), comprising 50% males and 50% females, in 24 teams, with an additional 4 team leaders to oversee the implementation of 25,000 Ag-RDTs. All CHWs and team leaders underwent a two-day training program about how to perform the Ag-RDTs. A context-specific algorithm (shown in Figure 1), consistent with WHO recommendations for low-prevalence settings, was used to interpret the Ag-RDT results.
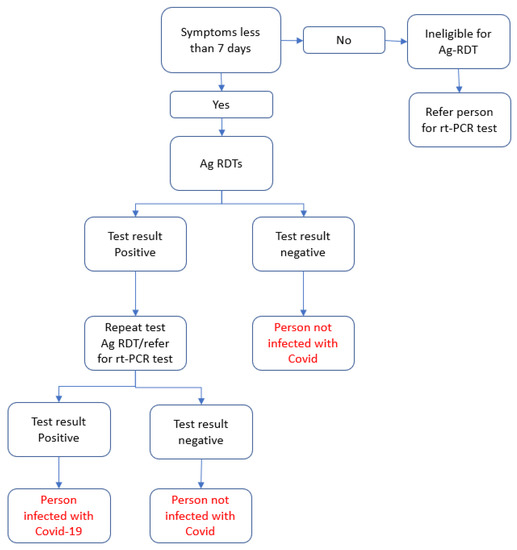
Figure 1.
Algorithm used to interpret antigen rapid diagnostic test (Ag-RDT) results in a pilot project conducted in north-west Syria (NWS).
2.4. Eligibility Criteria
Individuals from the target communities who met the following criteria were offered an Ag-RDT: (a) patients presenting with COVID-19 symptoms to health facilities (primary healthcare centers (PHCs), hospitals, and tuberculosis (TB) centers) within seven days of onset of symptoms; (b) symptomatic or asymptomatic individuals who were contacts of a COVID-19-infected individual; (c) refugees and migrants in densely populated areas where the risk of COVID-19 transmission was greater; (d) healthcare workers; (e) any other individuals who voluntarily sought a COVID-19 test. All individuals who met the eligibility criteria were enrolled for Ag-RDT testing; tests were only conducted once a participant had provided written informed consent.
2.5. Data Recording and Reporting
A data recording and reporting system was designed to capture the demographic and clinical characteristics of participants undergoing testing. The data were initially recorded as hard copies (in logbooks). They were later entered into an online digital platform created using the KOBO Toolbox® (Harvard Humanitarian Initiative, Cambridge, MA, USA) to enable real-time monitoring of the project’s implementation.
2.6. Project Supervision
To supervise and monitor the project’s implementation activities, supervisory visits were made by the four project leaders, during which they interacted with CHWs and participants involved in performing or undergoing the Ag-RDTs. In addition, a supervisory visit by the project coordinator was made to the head offices of IOM and HiHFAD in Turkey, which included interviews with team leaders and CHWs to discuss the progress made and challenges faced. Detailed reports of field visits were prepared and used as the basis for determining whether any corrective actions were necessary. In addition, the project coordinators reviewed the data entered by the CHWs into the Kobo application on a weekly basis to assess any gaps in the implementation or the data entered and provide feedback to address any deficiencies.
2.7. Study Sample
All individuals in the study areas who were eligible for an Ag-RDT, regardless of their age, were included in the pilot project, which was implemented between September and November 2022. The pilot project enrolled 27,888 individuals who were eligible to be offered an Ag-RDT.
2.8. Data Variables
For the first three objectives of the study, the variables included the name of the health facility and participants’ date of enrollment, age, gender, presence or absence of symptoms, reason for testing, vaccination status, response to being asked to provide consent, Ag-RDT results, date of the test, presence or absence of risk factors, and confirmatory RT-PCR test result (if conducted) and its date. For the fourth objective, data gathered during the supervisory visits by the project coordinators were used to obtain information about the facilitators and barriers to the implementation and uptake of Ag-RDTs in the field.
2.9. Data Analysis and Interpretation
To describe the feasibility, uptake, results of Ag-RDTs, and demographic and clinical data of participants, these variables were summarized as frequencies and percentages using R and RStudio statistical software. Associations between demographic and clinical characteristics (age, gender, reason for testing, and district) and the uptake of tests were assessed using bivariable and multivariable logistic regression models. The model fit was assessed using the Hosmer–Lemeshow goodness of fit test. Inferences around feasibility were based on the ease with which the CHWs could conduct the tests correctly, as per the designed algorithm, in different health facilities and geographical areas. These assumptions were based on discussions with CHWs and were documented in the supervisory visits. Furthermore, inferences around the uptake of Ag-RDTs were assessed based on the number and proportion of eligible individuals who gave consent to undergo the tests. Finally, to identify the facilitators and barriers to testing with Ag-RDTs, we produced a narrative table of the lessons learned and challenges encountered by CHWs when implementing the project, as determined by the project coordinators.
2.10. Ethical Issues
This project was implemented after obtaining administrative approval from the Turkish directorates (Hatay and Gaziantep) responsible for implementing all health activities within NWS. Ethics approval was obtained from the Institutional Review Board committee of Rayak Hospital, Lebanon, with the reference code ECO-R-35. Confidentiality of all data obtained from the pilot project’s recording system has been maintained. Consent was obtained from all individuals prior to them taking a test and to use their data for operational research. No names or identifying information of any person have been used in the analysis. Only aggregate data were used to disseminate the results of the study to all stakeholders.
3. Results
Between September and November 2022, 27,888 individuals in the study sites were eligible to enroll in the project and were offered an Ag-RDT. The demographic and clinical characteristics of all enrolled participants and the COVID-19 positivity rates were analyzed by gender, age group (Table 1), reason for testing, vaccination status, duration, severity of symptoms (Table 2), and testing facility (Table 3).

Table 1.
Demographic and clinical characteristics of enrolled individuals and their COVID-19 positivity rates, by gender and age group.
Table 2.
Demographic and clinical characteristics of enrolled individuals and their COVID-19 positivity rates by reason for testing, vaccination status, and duration and severity of symptoms.
Table 3.
Demographic and clinical characteristics of enrolled individuals and their COVID-19 positivity rates, by testing facility.
Overall, 24,956 (89.5%) of the 27,888 individuals enrolled consented to undergo an Ag-RDT, with 121 (0.5%) testing positive for COVID-19 by Ag-RDT. The study population comprised more females (57.1%) than males (42.9%), and approximately 74% of participants were between the ages of 18 and 49 years. Consent to take a test was lower among males (86.7%) than females (90.3%).
The main reasons for testing at the enrollment stage were being a refugee living within a densely populated and crowded area (44.5%), followed by having COVID-19 symptoms (43.1%). The highest proportions of positive cases in individuals who consented to test were observed among those with severe COVID-19 symptoms (12.7%), those with respiratory illnesses (2.5%), and healthcare workers (1.9%).
Overall, 12,026 (43.1%) individuals reporting having COVID-19 symptoms, of whom 11,777 (97.9%) reported mild symptoms, while 98.9% of participants reported the onset of symptoms within the previous seven days or less. Testing the 136 (1.1%) participants who had experienced symptoms for more than 7 days was performed because of challenges in convincing them they were excluded from the study simply because of their long duration of symptoms. There were 17,166 (61.6%) participants who had not received a single dose of any COVID-19 vaccine.
The majority (86.0%) of enrollments occurred at health facilities. The positivity rate among those who consented to testing was highest among participants from hospitals in Afrin (2.5%).
The demographic and clinical characteristics associated with the uptake of Ag-RDTs are shown in Table 4. Our bivariate analysis demonstrated that males were less likely than females to consent to an Ag-RDT. Participants aged 5 to 17 years were 1.35 times more likely to consent to having an Ag-RDT than those aged 18 to 34 years. Most participants who had a reason for testing, such as COVID-19-like symptoms, contact with a confirmed case of COVID-19, or recent travel, were more likely to agree to have an Ag-RDT than those without a reason for testing. However, participants’ willingness to have an Ag-RDT was considerably lower for IDPs than non-IDPs in NWS. Participants with severe COVID-19-like symptoms were 1.6 times more likely to agree to have an Ag-RDT than those with mild symptoms. Consent rates were highest at facilities in Jarablus, with participants at health facilities and PHCs in Afrin and Idlib being less likely to consent to having an Ag-RDT.
Table 4.
Demographic characteristics associated with uptake of Ag-RDTs in NWS.
In the multivariable analysis, gender remained a significant predictor of consenting to having an Ag-RDT, after considering potential confounders (odds ratio (OR) = 0.69, 95% confidence interval (CI) (0.645, 0.753)). After controlling for confounders, we observed that being younger (less than 18 years old) was significantly associated with being more likely to consent to having an Ag-RDT when compared with individuals aged 18 to 34 years. Health workers, refugees, and symptomatic individuals were more likely to agree to having an Ag-RDT than other groups. A significant predictor of uptake was the severity of symptoms, as individuals with severe symptoms were 2.3 times more likely to consent to having an Ag-RDT than people with mild symptoms.
Of those who underwent an Ag-RDT, a non-random sample of 239 individuals also had a confirmatory RT-PCR test (Table 5). This sample was selected based on the availability and accessibility of RT-PCR testing services for participants during the implementation period. This included 72/121 (59.5%) individuals who received a positive Ag-RDT result and 166/24,811 (6.7%) individuals who received a negative Ag-RDT result.
Table 5.
Comparison of Ag-RDT and RT-PCR results in individuals who had both tests.
Of the participants who underwent a confirmatory RT-PCR test (N = 239), the project team could not collect/receive information about the RT-PCR test results for three individuals. Therefore, after excluding these individuals, 236 individuals had results for both Ag-RDT and RT-PCR tests (Table 5). Based on this dataset, the ‘observed’ sensitivity of Ag-RDTs was 80.0% (95% CI: 71.2–88.7%) (64/80); specificity was 96.1% (95% CI 93–99%) (149/155); the positive predictive value was 91.4% (95% CI 84.8–97.9%) (64/70); and the negative predictive value was 90.3% (95%CI 85.7–94.8%) (149/165). The overall flow of participants under the project is given in Figure 2.
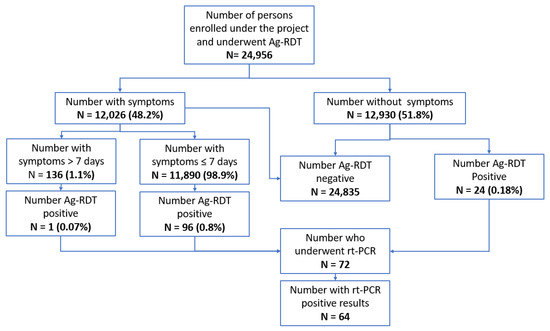
Figure 2.
Antigen rapid diagnostic test (Ag-RDT) results in a pilot project conducted in north-west Syria (NWS).
The reported barriers and facilitators encountered during the implementation of the project are shown in Table 6 and Table 7. The key challenges were obtaining informed consent, referral for confirmatory RT-PCR testing, and recording and reporting the data for the project.
Table 6.
Challenges encountered during the Ag-RDT pilot project in NWS.
Table 7.
Facilitators that contributed to the good feasibility and uptake of Ag-RDTs.
4. Discussion
This is one of the first studies from NWS describing the use of COVID-19 Ag-RDTs in a pilot project. Individuals who were eligible for testing were contacted, and the project’s target quota of participants was achieved within a very short, 2-month implementation period. The wide variations seen in the numbers enrolled at the nine study sites are due to the differences in the population distribution in these geographical areas. Enrollment at PHCs and hospitals was higher than at camps/mobile clinics, as all of the health facilities and hospitals in NWS are distributed inside the camps. As reported by the implementing partner, only a few camps lack these facilities. All nine facilities selected successfully deployed all their Ag-RDTs, indicating good feasibility of using these tests at all sites within NWS, distributed through CHWs. Furthermore, the interviews with CHWs during the supervisory visits did not reveal any major challenges in deploying or performing these tests, adding to the global body of evidence for the feasibility of rapid deployment of Ag-RDTs to inform essential infection control and prevention measures in all settings [16,17].
Almost 90% of participants were willing to take an Ag-RDT. This was mainly due to the positive communication from the CHWs about the advantages of Ag-RDTs and the need to ensure there was no break in COVID-19 surveillance. This communication helped to engender positive perceptions about the Ag-RDTs and facilitated their uptake. The uptake of Ag-RDTs was higher among individuals with COVID-19 symptoms, healthcare workers, refugees, individuals who had received two or more doses of vaccine, and individuals identified at TB clinics than it was among other groups. Previous studies have shown good overall uptake of Ag-RDTs among different populations, especially among symptomatic individuals [18,19]. The reasons for the lower uptake of Ag-RDTs among those aged less than 18 years and among individuals in Afrin and Idleb districts could not be determined from the interviews with CHWs. This is an area that will therefore need further investigation through the use of qualitative research methods.
The overall positivity rate within our sample was very low (just 0.5%), indicating low levels of COVID-19 prevalence at the community level. The highest positivity was observed among individuals with severe COVID-19 symptoms (12.7%), followed by individuals with respiratory illnesses (2.5%), participants enrolled at hospitals in Afrin (2.5%), and healthcare workers (1.9%). On one hand, these findings indicate the high-risk groups who should be targeted for COVID-19 testing in these low-prevalence/-transmission settings. On the other hand, these findings also suggest that some geographical regions or pockets of persisting COVID-19 infection could lead to a flare-up of COVID-19 transmission if there were to be a new variant of the virus. Therefore, continuous surveillance is needed. Data about positivity rates and the association with participants’ various characteristics can play an essential role in surveillance activities, especially for the screening and diagnosis of COVID-19 infection in these high-risk groups.
Unfortunately, a formal assessment of the sensitivity and specificity of the selected Ag-RDTs when deployed in the field could not be carried out due to challenges in identifying an academic partner in this setting. Nevertheless, the observed sensitivity and specificity of the Ag-RDTs in relation to the RT-PCR appears to be in line with those reported for other studies involving the same Ag-RDTs as used in our pilot project [20,21]. It should be noted, however, that the performance of Ag-RDTs varies among brands [22]. Therefore, policymakers should pay careful attention when selecting suitable Ag-RDTs for testing programs. The sensitivity and negative predictive values observed in this pilot project, which were lower than the manufacturer-reported values, could be due to the quality of the nasopharyngeal samples collected, and the difficulties processing the collected samples and the reagents in the test kits [23,24,25,26,27].
Such deficiencies must be identified and rectified through training and supportive supervision in any future projects. However, considering the high specificity (96.1%) and good negative predictive value (90.3%), screening for COVID-19 using Ag-RDTs results would be a reasonable approach in this setting, whether or not a confirmatory PCR test is used.
It was only possible to perform confirmatory RT-PCR tests (as per the algorithm) in 60% of individuals who had a positive Ag-RDT result. This indicates operational challenges in following the complete algorithm needed for the optimal deployment of Ag-RDTs. Similar observations were made in other studies that evaluated the implementation of Ag-RDTs [28,29]. Therefore, there is a need to enhance both the capacity and accessibility of RT-PCR testing within the health system catering to these populations. If this is not completed, clinical and public health decisions in relation to COVID-19 infection/transmission will have to be based on Ag-RDTs alone.
Finally, 61.6% of our sample reported they had not received a single dose of COVID-19 vaccine. WHO reported that the proportion of people in NWS who had not received a single dose of COVID-19 vaccine during our implementation period was 86.4% [30], showing that there are considerable global inequities in vaccination coverage in these populations.
Strengths and Limitations
The major strength of this study is that it was based on data from a pilot project implemented under routine programmatic conditions and using the existing health service delivery mechanisms. Therefore, the study’s findings in relation to feasibility, uptake, Ag-RDT performance, and positivity rates likely reflect ground-level realities. The study’s major limitations are as follows: First, the project was conducted in a low-prevalence/-transmission setting. Therefore, the results may not be replicable if there is a surge in COVID-19 prevalence. Second, the implementation challenges were identified, and facilitators’ data were collected during routine supervision visits. As a result, the information provided by CHWs may have been biased if they felt they had failed in any way or were uncomfortable reporting any critical issues to their supervisors. Third, due to challenges/restrictions in meeting the members of the community, their perspectives about the feasibility and acceptability of Ag-RDTs could not be fully captured. This is an area for future research.
5. Conclusions
This pilot project conducted in NWS demonstrated that using Ag-RDTs and delivering them through CHWs as a screening/diagnostic tool for COVID-19 infections is feasible. The data for uptake and positivity rates indicate that Ag-RDTs can be targeted to health facilities; individuals with respiratory, febrile, or COVID-19 symptoms; contacts of COVID-19 cases; and health workers. The project also highlighted the need for a comprehensive strategy to independently use Ag-RDT results to screen for COVID-19 infections among refugees and in IDP settings. Finally, the study confirms the need for continuous surveillance and enhancement of COVID-19 vaccination coverage.
Author Contributions
Conceptualization, N.W., S.S. (Sanjay Sarin) and K.K.; Methodology, N.W., S.S. (Srinath Satyanarayana), L.T., H.G., H.A. and S.H.; Data Curation, H.G. and M.N.A.; Writing—Original Draft Preparation, H.G., M.N.A. and S.S. (Srinath Satyanarayana); Writing—Review and Editing, H.G., S.S. (Srinath Satyanarayana), M.N.A., L.T., H.A., S.H., S.S. (Sanjay Sarin), K.K. and N.W.; Supervision, N.W., H.G., S.S. (Srinath Satyanarayana), H.A. and S.H.; Funding Acquisition, S.S. (Sanjay Sarin) and K.K. All authors have read and agreed to the published version of the manuscript.
Funding
This project is funded through a catalytic grant from the Foundation for Innovative New Diagnostics.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Rayak Hospital—Institutional Review Board in Lebanon (Ref.: ECO-R-35), on 13 March 2023.
Informed Consent Statement
All participants gave their written informed consent for inclusion in the Ag-RDT project.
Data Availability Statement
The clean set of raw data presented in this study are available from the corresponding author in MS Excel format upon reasonable request. The data are not publicly available due to data protection and privacy policies following the UN Migration Agency (IOM) standards.
Acknowledgments
Grace Javier and Noor Abzadough, project administration; Christopher Togara, procurement, and supply management; Nick Banks, information technology, FIND;HiHFAD, and all of the CHWs who participated in this work.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Bank. MENA-Crisis-Tracker-2-7-2022. Office of the Chief Economist. 2022. Available online: https://thedocs.worldbank.org/en/doc/a32a611d09ad47947f154d81c635b658-0280032022/original/MENA-Crisis-Tracker-2-7-2022.pdf (accessed on 2 February 2023).
- Karamouzian, M.; Madani, N. COVID-19 response in the Middle East and north Africa: Challenges and paths forward. Lancet Glob. Health 2020, 8, e886–e887. [Google Scholar] [CrossRef] [PubMed]
- Flores, G.; Abbasi, A.; Korachais, C.; Lavado, R. Unaffordability of COVID-19 tests: Assessing age-related inequalities in 83 countries. Int. J. Equity Health 2022, 21, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Esposito, A.; Palmisano, A.; Scotti, G.M.; Morelli, M.J.; Vignale, D.; De Cobelli, F.; Tonon, G.; Tacchetti, C. Why is chest CT important for early diagnosis of COVID-19? Prevalence matters. medRxiv 2020. [Google Scholar] [CrossRef]
- Ly, T.D.A.; Nguyen, N.N.; Hoang, V.T.; Goumballa, N.; Louni, M.; Canard, N.; Dao, T.L.; Medkour, H.; Borg, A.; Bardy, K.; et al. Screening of SARS-CoV-2 among homeless people, asylum-seekers and other people living in precarious conditions in Marseille, France, March-April 2020. Int. J. Infect. Dis. 2021, 105, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kheirallah, K.A.; Ababneh, B.F.; Bendak, H.; Alsuwaidi, A.R.; Elbarazi, I. Exploring the Mental, Social, and Lifestyle Effects of a Positive COVID-19 Infection on Syrian Refugees in Jordan: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 12588. [Google Scholar] [CrossRef]
- Marc Lynch. (PDF) COVID-19: Lebanon’s Experience and Response. In: POMEPS Studies [Internet]. 2020. Available online: https://www.researchgate.net/publication/340819777_COVID-19_Lebanon’s_Experience_and_Response (accessed on 7 January 2023).
- Peeling, R.W.; Heymann, D.L. Innovations in COVID-19 testing: The road from pandemic response to control. Lancet Infect. Dis. 2021, 21, 1334–1335. [Google Scholar] [CrossRef]
- Peeling, R.W.; Heymann, D.L.; Teo, Y.Y.; Garcia, P.J. Diagnostics for COVID-19: Moving from pandemic response to control. Lancet 2022, 399, 757–768. [Google Scholar] [CrossRef]
- Brümmer, L.E.; Katzenschlager, S.; Gaeddert, M.; Erdmann, C.; Schmitz, S.; Bota, M.; Grilli, M.; Larmann, J.; Weigand, M.A.; Pollock, N.R.; et al. Accuracy of novel antigen rapid diagnostics for SARS-CoV-2: A living systematic review and meta-analysis. PLoS Med. 2021, 18, e1003735. [Google Scholar] [CrossRef]
- Foundation of Innovative New Diagnostics. FIND | Diagnosis for All. 2023. Available online: https://www.finddx.org/ (accessed on 23 January 2023).
- UNOCHA. North-West Syria|Situation Reports. 2023. Available online: https://reports.unocha.org/en/country/syria/ (accessed on 23 January 2023).
- ARCS. Statement on the Continuation of UN-Led Cross-Border Humanitarian Assistance in Northwest Syria|American Relief Coalition for Syria. 2023. Available online: https://arcsyria.org/article/statement-continuation-un-led-cross-border-humanitarian-assistance-northwest-syria (accessed on 23 January 2023).
- Alanba, A.-K. ارتفاع يومي بإصابات الكوليرا وكورونا شمال (Daily increase in Cholera and COVID-19 infections in North-West Syria). 23 December 2022. Available online: https://www.alanba.com.kw/1160966 (accessed on 7 January 2023).
- OCHA. COVID-19 Monthly Update Northwest Syria (As of 31 December 2022)-Syrian Arab Republic|ReliefWeb. 2022. Available online: https://reliefweb.int/report/syrian-arab-republic/covid-19-monthly-update-northwest-syria-31-december-2022 (accessed on 13 April 2023).
- Lindner, A.K.; Nikolai, O.; Rohardt, C.; Kausch, F.; Wintel, M.; Gertler, M.; Burock, S.; Hörig, M.; Bernhard, J.; Tobian, F.; et al. Diagnostic accuracy and feasibility of patient self-testing with a SARS-CoV-2 antigen-detecting rapid test. J. Clin. Virol. 2021, 141, 104874. [Google Scholar] [CrossRef]
- WHO. Use of SARS-CoV-2 Antigen-Detection Rapid Diagnostic Tests for COVID-19 Self-Testing; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- Vink, M.; Iglói, Z.; Fanoy, E.B.; van Beek, J.; Boelsums, T.; de Graaf, M.; Voeten, H.A.; Molenkamp, R.; Koopmans, M.P.; Mevissen, F.E. Community-based SARS-CoV-2 testing in low-income neighbourhoods in Rotterdam: Results from a pilot study. J. Glob. Health 2022, 12, 05042. [Google Scholar] [CrossRef]
- Finch, L.S.; Harris, A.; Lester, C.; Veal, D.; Jones, K.; Fulton, J.; Jones, L.; Lee, M.; Walker, T.; Rossiter, M.; et al. Implementation study of SARS-CoV-2 antigen lateral flow tests in men’s professional (Premiership) rugby union sports squads in England during the COVID-19 pandemic. J. Infect. 2022, 84, e3–e5. [Google Scholar] [CrossRef]
- Krüger, L.J.; Lindner, A.K.; Gaeddert, M.; Tobian, F.; Klein, J.; Steinke, S.; Lainati, F.; Schnitzler, P.; Nikolai, O.; Mockenhaupt, F.P.; et al. A Multicenter Clinical Diagnostic Accuracy Study of SureStatus, an Affordable, WHO Emergency Use-Listed, Rapid, Point-Of-Care Antigen-Detecting Diagnostic Test for SARS-CoV-2. Microbiol. Spectr. 2022, 10, e0122922. [Google Scholar] [CrossRef]
- Byrne, R.L.; Aljayyoussi, G.; Kontogianni, K.; Clerkin, K.; McIntyre, M.; Wardale, J.; Williams, C.T.; CONDOR Steering Group; Body, R.; Adams, E.R.; et al. Head-to head comparison of anterior nares and nasopharyngeal swabs for SARS-CoV-2 1 antigen detection in a community drive-through test centre in the UK Running title: Anterior nares or NP swabs for SARS-CoV-2 RDTs. medRxiv 2022. [Google Scholar] [CrossRef]
- Keskin, A.U.; Ciragil, P.; Topkaya, A.E. Clinical Accuracy of Instrument-Read SARS-CoV-2 Antigen Rapid Diagnostic Tests (Ag-IRRDTs). Int. J. Microbiol. 2022, 2022, 9489067. [Google Scholar] [CrossRef]
- Baro, B.; Rodo, P.; Ouchi, D.; Bordoy, A.E.; Amaro, E.N.S.; Salsench, S.V.; Molinos, S.; Alemany, A.; Ubals, M.; Corbacho-Monné, M.; et al. Performance characteristics of five antigen-detecting rapid diagnostic test (Ag-RDT) for SARS-CoV-2 asymptomatic infection: A head-to-head benchmark comparison. J. Infect. 2021, 82, 269–275. [Google Scholar] [CrossRef]
- La Scola, B.; Le Bideau, M.; Andreani, J.; Hoang, V.T.; Grimaldier, C.; Colson, P.; Gautret, P.; Raoult, D. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1059–1061. [Google Scholar] [CrossRef]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; et al. Virological assessment of hospitalized patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef]
- Quicke, K.; Gallichote, E.; Sexton, N.; Young, M.; Janich, A.; Gahm, G.; Carlton, E.J.; Ehrhart, N.; Ebel, G.D. Longitudinal Surveillance for SARS-CoV-2 RNA Among Asymptomatic Staff in Five Colorado Skilled Nursing Facilities: Epidemiologic, Virologic and Sequence Analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Mina, M.J.; Parker, R.; Larremore, D.B. Rethinking COVID-19 Test Sensitivity—A Strategy for Containment. N. Engl. J. Med. 2020, 383, e120. [Google Scholar] [CrossRef]
- Wachinger, J.; Olaru, I.D.; Horner, S.; Schnitzler, P.; Heeg, K.; Denkinger, C.M. The potential of SARS-CoV-2 antigen-detection tests in the screening of asymptomatic persons. Clin. Microbiol. Infect. 2021, 27, e1–e1700. [Google Scholar] [CrossRef]
- Sagna, A.S.; Seydi, A.G.; Gueye, M.M.; Fall, M.T.A.; Mansuy, J.M. Contribution of COVID Antigenic RDT to the Management Strategy of COVID-19 Pandemic in a Senegalese Company. J. Occup. Environ. Med. 2022, 64, e257. [Google Scholar] [CrossRef] [PubMed]
- WHO. Monthly COVID-19 Bulletin October 2022. 2022. Available online: https://www.emro.who.int/images/stories/Monthly_COVID-19_Bulletin_October_2022.pdf?ua=1 (accessed on 20 March 2023).


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).