



Dengue as a Disease Threatening Global Health: A Narrative Review Focusing on Latin America and Brazil

 ,
,
Abstract
1. Introduction
2. Disease Overview
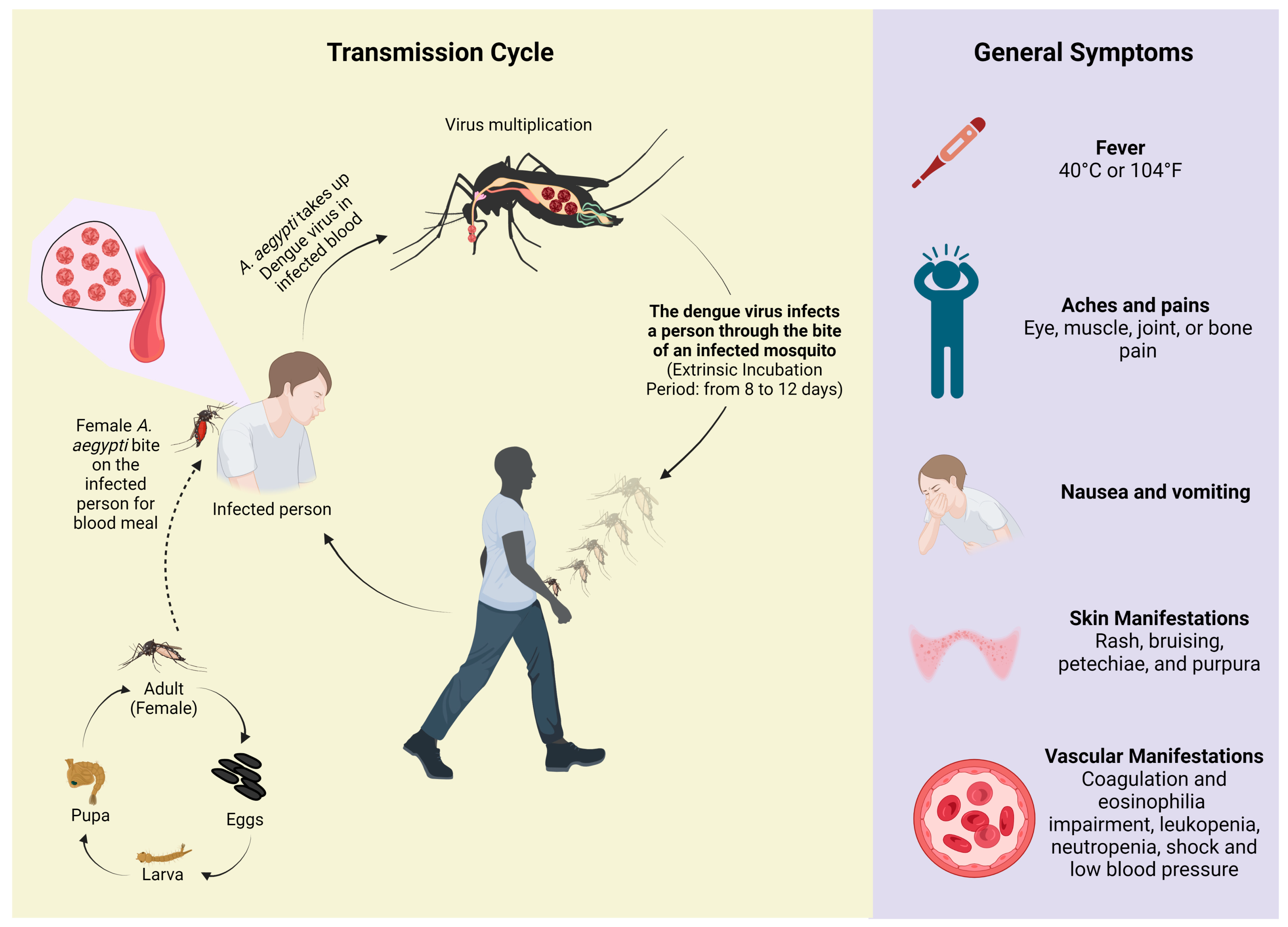
2.1. Transmission Mode and Clinical Manifestations
2.2. Management Aspects
2.3. Disease Control
3. Dengue in the World
3.1. Epidemiologic Overview
3.2. Economic Burden
4. Dengue in the Americas
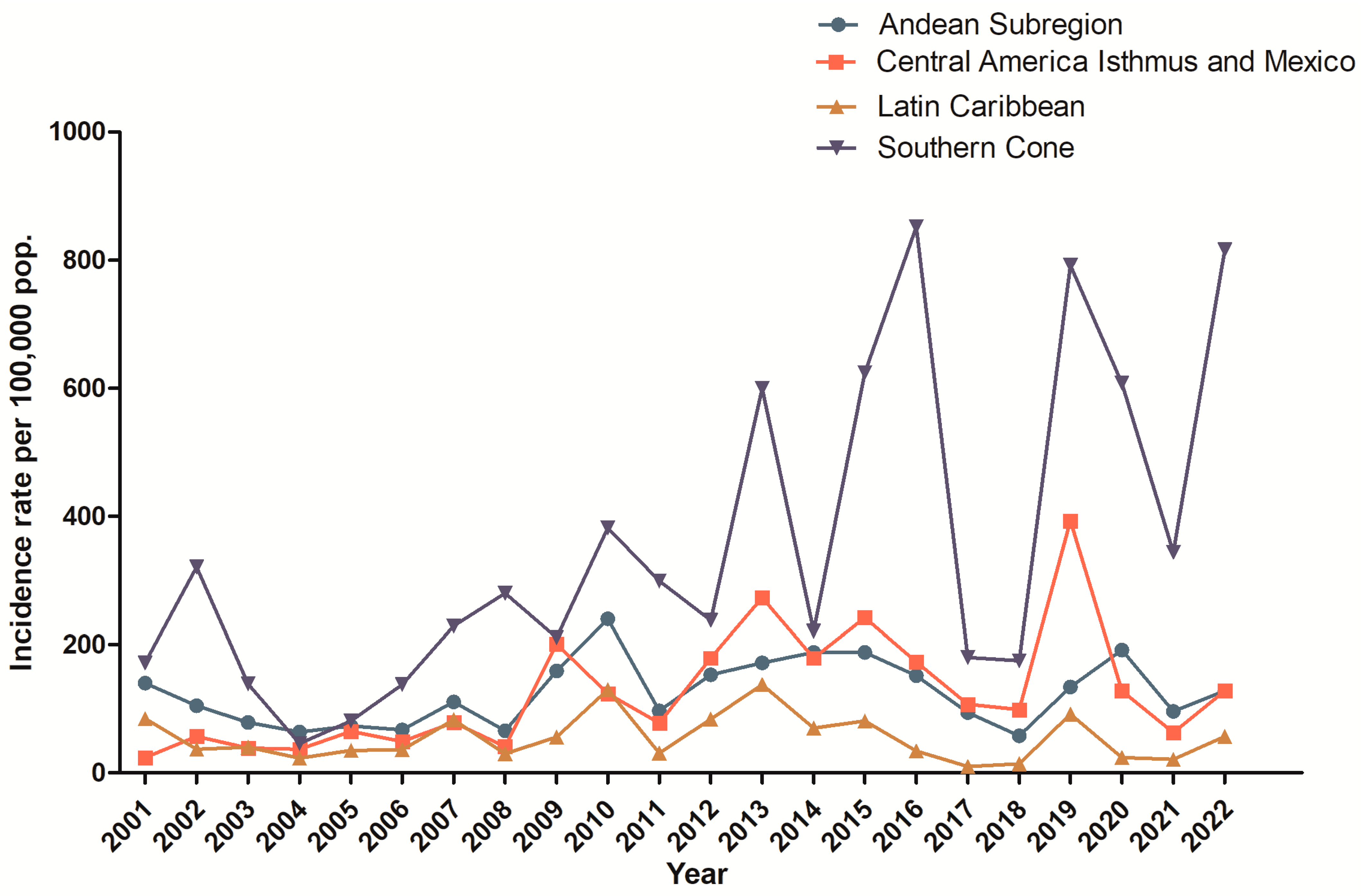
4.1. Epidemiologic Issues of Dengue in Latin America
4.2. Economic Aspects of Dengue in Latin America
5. Dengue in Brazil
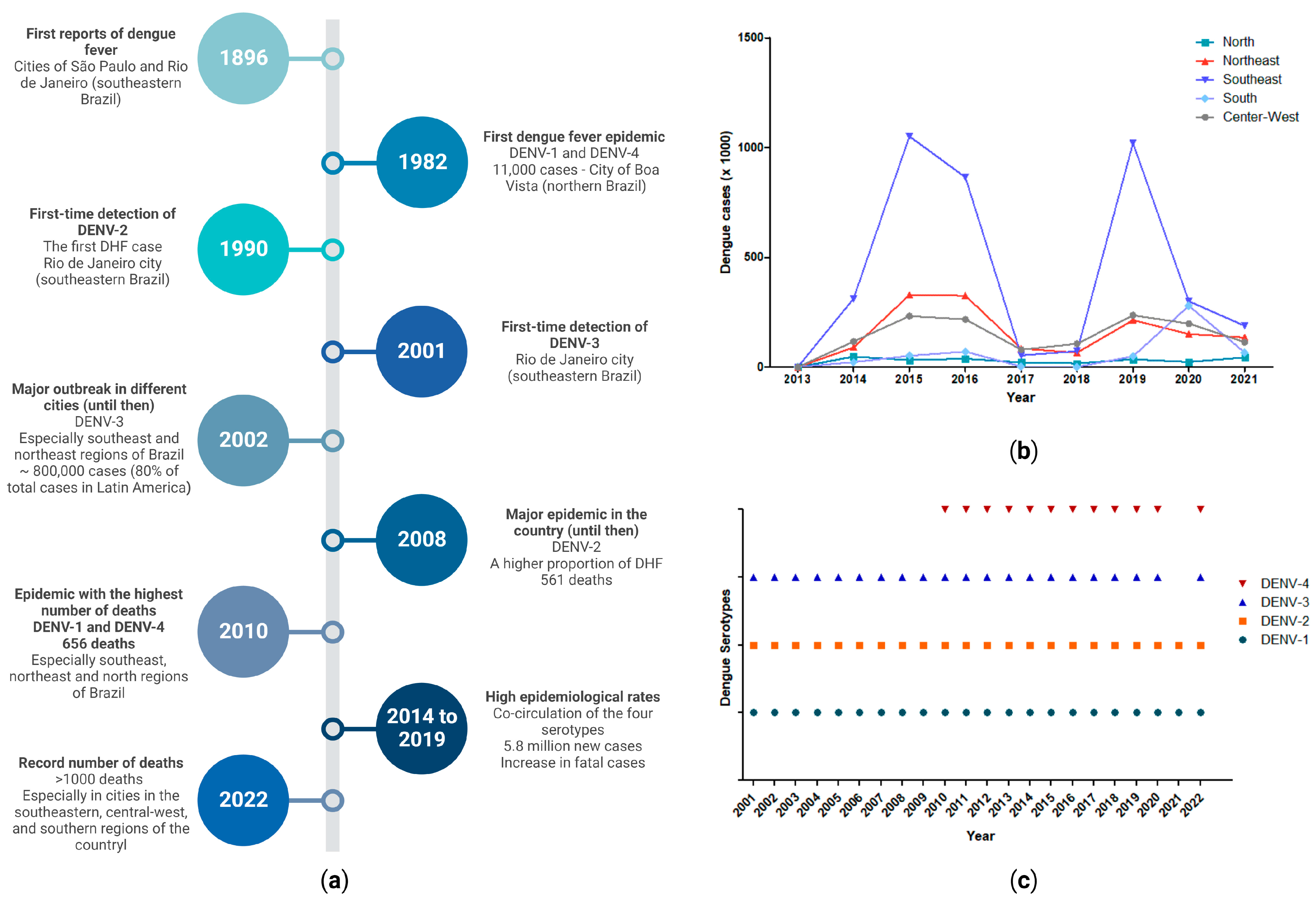
5.1. Epidemiologic Issues: Focus in Brazil
5.2. Economic Burden: Focus in Brazil
5.3. Disease Control: Focus in Brazil
6. Considerations and Perspectives for Dengue: Focus on Epidemiology
6.1. General Perspectives and Challenges Regarding Dengue
6.2. Perspectives on Economic Epidemiology
6.3. Perspectives on Technological Advancement and Support of Epidemiological Elucidation
6.4. Perspective on Dengue and Wastewater-Based Epidemiology
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Viglietta, M.; Bellone, R.; Blisnick, A.A.; Failloux, A.-B. Vector Specificity of Arbovirus Transmission. Front. Microbiol. 2021, 12, 3446. [Google Scholar] [CrossRef] [PubMed]
- Araújo, N.J.S.; Macêdo, M.J.F.; de Morais, L.P.; da Cunha, F.A.B.; de Matos, Y.M.L.S.; de Almeida, R.S.; Braga, M.F.B.M.; Coutinho, H.D.M. Control of arboviruses vectors using biological control by Wolbachia pipientis: A short review. Arch. Microbiol. 2022, 204, 376. [Google Scholar] [CrossRef] [PubMed]
- Torres-Flores, J.M.; Reyes-Sandoval, A.; Salazar, M.I. Dengue Vaccines: An Update. Biodrugs 2022, 36, 325. [Google Scholar] [CrossRef]
- Alagarasu, K.; Patil, J.A.; Kakade, M.B.; More, A.M.; Yogesh, B.; Newase, P.; Jadhav, S.M.; Parashar, D.; Kaur, H.; Gupta, N.; et al. Serotype and genotype diversity of dengue viruses circulating in India: A multi-centre retrospective study involving the Virus Research Diagnostic Laboratory Network in 2018. Int. J. Infect. Dis. 2021, 111, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, M.S.; Rasotgi, V.; Jain, S.; Gupta, V. Discovery of fifth serotype of dengue virus (DENV-5): A new public health dilemma in dengue control. Med. J. Armed Forces India 2015, 71, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Normile, D. Surprising New Dengue Virus Throws a Spanner in Disease Control Efforts. Science 2013, 342, 415. [Google Scholar] [CrossRef] [PubMed]
- Paixão, E.S.; Teixeira, M.G.; Rodrigues, L.C. Zika, chikungunya and dengue: The causes and threats of new and re-emerging arboviral diseases. BMJ Glob. Health 2018, 3, e000530. [Google Scholar] [CrossRef]
- Barreto, M.L.; Teixeira, M.G. Dengue no Brasil: Situação epidemiológica e contribuições para uma agenda de pesquisa. Estud. Avançados 2008, 22, 53–72. [Google Scholar] [CrossRef]
- Gwee, X.W.S.; Chua, P.E.Y.; Pang, J. Global dengue importation: A systematic review. BMC Infect. Dis. 2021, 21, 1078. [Google Scholar]
- Buchs, A.; Conde, A.; Frank, A.; Gottet, C.; Hedrich, N.; Lovey, T.; Shindleman, H.; Schlagenhauf, P. The threat of dengue in Europe. New Microbes New Infect. 2022, 49–50, 101061. [Google Scholar] [CrossRef]
- Berberian, G.; Pérez, G.; Mangano, A.; Borgnia, D.; Buchovsky, A.; Costa, M.; Fabbri, C.; Luppo, V.; Luppo, A.S.; Deschutter, V.; et al. Dengue beyond the tropics: A time-series study at a children’s hospital in the City of Buenos Aires. Arch Argent Pediatr. 2022, 120, 384–390. [Google Scholar] [CrossRef]
- Manna, S.; Satapathy, P.; Bora, I.; Padhi, B.K. Dengue outbreaks in South Asia amid Covid-19: Epidemiology, transmission, and mitigation strategies. Front. Public Health 2022, 10, 4918. [Google Scholar] [CrossRef] [PubMed]
- Xavier, L.L.; Honório, N.A.; Pessanha, J.F.M.; Peiter, P.C. Analysis of climate factors and dengue incidence in the metropolitan region of Rio de Janeiro, Brazil. PLoS ONE 2021, 16, e0251403. [Google Scholar] [CrossRef]
- do Carmo, R.F.; Silva Júnior, J.V.J.; Pastor, A.F.; de Souza, C.D.F. Spatiotemporal dynamics, risk areas and social determinants of dengue in Northeastern Brazil, 2014–2017: An ecological study. Infect. Dis. Poverty 2020, 9, 153. [Google Scholar] [CrossRef]
- da Silva, J.C.B.; Machado, C.J.S. Associations between Dengue And Socio-Environmental Variables in Capitals of the Brazilian Northeast by Cluster Analysis. Ambient. Soc. 2018, 21, 1332. [Google Scholar] [CrossRef]
- Ortiz Guerrero, L.M.; Carreño Parra, L.M.; Márquez Gómez, M.A. Análisis de contenido en mensajes impresos sobre enfermedades de transmisión vectorial en un municipio de Colombia. Nova 2020, 18, 77–94. [Google Scholar] [CrossRef]
- Angelo, M.; Ramalho, W.M.; Gurgel, H.; Belle, N.; Pilot, E. Dengue Surveillance System in Brazil: A Qualitative Study in the Federal District. Int. J. Environ. Res. Public Health 2020, 17, 2062. [Google Scholar] [CrossRef]
- von dem Knesebeck, O. Concepts of social epidemiology in health services research. BMC Health Serv. Res. 2015, 15, 357. [Google Scholar] [CrossRef]
- Tsheten, T.; Gray, D.J.; Clements, A.C.A.; Wangdi, K. Epidemiology and challenges of dengue surveillance in the WHO South-East Asia Region. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 583–599. [Google Scholar] [CrossRef]
- Islam, M.T.; Quispe, C.; Herrera-Bravo, J.; Sarkar, C.; Sharma, R.; Garg, N.; Fredes, L.I.; Martorell, M.; Alshehri, M.M.; Sharifi-Rad, J.; et al. Production, Transmission, Pathogenesis, and Control of Dengue Virus: A Literature-Based Undivided Perspective. Biomed Res. Int. 2021, 2021, 4224816. [Google Scholar] [CrossRef]
- Agha, S.B.; Tchouassi, D.P. Urbanization of Aedes mosquito populations and evolution of arboviral disease risk in Africa. Curr. Opin. Insect Sci. 2022, 54, 100988. [Google Scholar] [CrossRef]
- OPAS Dengue. Available online: https://www.paho.org/pt/topicos/dengue (accessed on 9 January 2023).
- Martins, I.C.; Ricardo, R.C.; Santos, N.C. Dengue, West Nile, and Zika Viruses: Potential Novel Antiviral Biologics Drugs Currently at Discovery and Preclinical Development Stages. Pharmaceutics 2022, 14, 2535. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.M.; Adams, L.E.; Durbin, A.P.; Muñoz-Jordán, J.L.; Poehling, K.A.; Sánchez-González, L.M.; Volkman, H.R.; Paz-Bailey, G. Dengue: A Growing Problem with New Interventions. Pediatrics 2022, 149, e2021055522. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, P.; Sabeena, S.P.; Varma, M.; Arunkumar, G. Current Understanding of the Pathogenesis of Dengue Virus Infection. Curr. Microbiol. 2021, 78, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Leowattana, W.; Leowattana, T. Dengue hemorrhagic fever and the liver. World J. Hepatol. 2021, 13, 1968–1976. [Google Scholar] [CrossRef]
- Murugesan, A.; Manoharan, M. Dengue Virus. In Emerging and Reemerging Viral Pathogens; Elsevier: Amsterdam, The Netherlands, 2020; pp. 281–359. ISBN 9780128194003. [Google Scholar]
- Guerra-Gomes, I.C.; Gois, B.M.; Peixoto, R.F.; Oliveira, C.A.; Maciel, B.L.L.; Sarmento, M.I.F.; Pachá, A.S.C.; Araújo, J.M.G.; Amaral, I.P.G.; Keesen, T.S.L. Molecular and clinical epidemiological surveillance of dengue virus in Paraíba, Northeast Brazil. Rev. Soc. Bras. Med. Trop. 2017, 50, 19–26. [Google Scholar] [CrossRef]
- Wong, P.-F.; Wong, L.-P.; AbuBakar, S. Diagnosis of severe dengue: Challenges, needs and opportunities. J. Infect. Public Health 2020, 13, 193–198. [Google Scholar] [CrossRef]
- Guanche Garcell, H.; Gutiérrez García, F.; Ramirez Nodal, M.; Ruiz Lozano, A.; Pérez Díaz, C.R.; González Valdés, A.; Gonzalez Alvarez, L. Clinical relevance of Zika symptoms in the context of a Zika Dengue epidemic. J. Infect. Public Health 2020, 13, 173–176. [Google Scholar] [CrossRef]
- Belaunzarán-Zamudio, P.F.; Mateja, A.; Guerra-de-Blas, P.d.C.; Rincón-León, H.A.; Navarro-Fuentes, K.; Ruiz-Hernández, E.; Caballero-Sosa, S.; Camas-Durán, F.; Priego-Smith, Z.; Nájera-Cancino, J.G.; et al. Comparison of clinical characteristics of Zika and dengue symptomatic infections and other acute illnesses of unidentified origin in Mexico. PLoS Negl. Trop. Dis. 2021, 15, e0009133. [Google Scholar] [CrossRef]
- Malavige, G.N.; Jeewandara, C.; Ogg, G.S. Dengue and COVID-19: Two sides of the same coin. J. Biomed. Sci. 2022, 29, 48. [Google Scholar] [CrossRef]
- Zulfa, R.; Lo, W.-C.; Cheng, P.-C.; Martini, M.; Chuang, T.-W. Updating the Insecticide Resistance Status of Aedes aegypti and Aedes albopictus in Asia: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 306. [Google Scholar] [CrossRef]
- Zeyaullah, M.; Muzammil, K.; AlShahrani, A.M.; Khan, N.; Ahmad, I.; Alam, M.S.; Ahmad, R.; Khan, W.H. Preparedness for the Dengue Epidemic: Vaccine as a Viable Approach. Vaccines 2022, 10, 1940. [Google Scholar] [CrossRef]
- Silva, N.M.; Santos, N.C.; Martins, I.C. Dengue and Zika Viruses: Epidemiological History, Potential Therapies, and Promising Vaccines. Trop. Med. Infect. Dis. 2020, 5, 150. [Google Scholar] [CrossRef] [PubMed]
- Waickman, A.T.; Newell, K.; Endy, T.P.; Thomas, S.J. Biologics for dengue prevention: Up-to-date. Expert Opin. Biol. Ther. 2023, 23, 73–87. [Google Scholar] [CrossRef]
- Takeda Takeda’s Dengue Vaccine Approved for Use in Brazil. Available online: https://www.takeda.com/newsroom/newsreleases/2023/takedas-qdenga-approved-in-brazil (accessed on 6 April 2023).
- Takeda New Dengue Vaccine Approved in Indonesia for Use Regardless of Prior Dengue Exposure. Available online: https://www.takeda.com/newsroom/newsreleases/2022/takedas-qdenga-dengue-tetravalent-vaccine-live-attenuated-approved-in-indonesia-for-use-regardless-of-prior-dengue-exposure (accessed on 6 April 2023).
- Takeda Takeda’s Dengue Vaccine Approved for Use in European Union. Available online: https://www.takeda.com/newsroom/newsreleases/2022/takedas-qdenga-dengue-tetravalent-vaccine-live-attenuated-approved-for-use-in-european-union (accessed on 6 April 2023).
- Biswal, S.; Borja-Tabora, C.; Martinez Vargas, L.; Velásquez, H.; Theresa Alera, M.; Sierra, V.; Johana Rodriguez-Arenales, E.; Yu, D.; Wickramasinghe, V.P.; Duarte Moreira, E.; et al. Efficacy of a tetravalent dengue vaccine in healthy children aged 4–16 years: A randomised, placebo-controlled, phase 3 trial. Lancet 2020, 395, 1423–1433. [Google Scholar] [CrossRef]
- Biswal, S.; Reynales, H.; Saez-Llorens, X.; Lopez, P.; Borja-Tabora, C.; Kosalaraksa, P.; Sirivichayakul, C.; Watanaveeradej, V.; Rivera, L.; Espinoza, F.; et al. Efficacy of a Tetravalent Dengue Vaccine in Healthy Children and Adolescents. N. Engl. J. Med. 2019, 381, 2009–2019. [Google Scholar] [CrossRef] [PubMed]
- Lasluisa, D.; Barrios, E.; Vasilieva, O. Optimal Strategies for Dengue Prevention and Control during Daily Commuting between Two Residential Areas. Processes 2019, 7, 197. [Google Scholar] [CrossRef]
- Lima, E.P.; Goulart, M.O.F.; Rolim Neto, M.L. Meta-analysis of studies on chemical, physical and biological agents in the control of Aedes aegypti. BMC Public Health 2015, 15, 858. [Google Scholar] [CrossRef]
- Dias, Í.K.R.; Martins, R.M.G.; Sobreira, C.L.d.S.; Rocha, R.M.G.S.; Lopes, M.d.S.V. Ações educativas de enfrentamento ao Aedes Aegypti: Revisão integrativa. Cien. Saude Colet. 2022, 27, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Gan, S.J.; Leong, Y.Q.; bin Barhanuddin, M.F.H.; Wong, S.T.; Wong, S.F.; Mak, J.W.; Ahmad, R.B. Dengue fever and insecticide resistance in Aedes mosquitoes in Southeast Asia: A review. Parasit. Vectors 2021, 14, 315. [Google Scholar] [CrossRef] [PubMed]
- Waltz, E. First genetically modified mosquitoes released in the United States. Nature 2021, 593, 175–176. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.-H.; Gamez, S.; Raban, R.R.; Marshall, J.M.; Alphey, L.; Li, M.; Rasgon, J.L.; Akbari, O.S. Combating mosquito-borne diseases using genetic control technologies. Nat. Commun. 2021, 12, 4388. [Google Scholar] [CrossRef] [PubMed]
- Pinto, S.B.; Riback, T.I.S.; Sylvestre, G.; Costa, G.; Peixoto, J.; Dias, F.B.S.; Tanamas, S.K.; Simmons, C.P.; Dufault, S.M.; Ryan, P.A.; et al. Effectiveness of Wolbachia-infected mosquito deployments in reducing the incidence of dengue and other Aedes-borne diseases in Niterói, Brazil: A quasi-experimental study. PLoS Negl. Trop. Dis. 2021, 15, e0009556. [Google Scholar] [CrossRef] [PubMed]
- Meghani, Z. Regulation of genetically engineered (GE) mosquitoes as a public health tool: A public health ethics analysis. Global. Health 2022, 18, 21. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Insecticide Use for Vector-Borne Disease Control; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Suwantika, A.A.; Kautsar, A.P.; Supadmi, W.; Zakiyah, N.; Abdulah, R.; Ali, M.; Postma, M.J. Cost-Effectiveness of Dengue Vaccination in Indonesia: Considering Integrated Programs with Wolbachia-Infected Mosquitos and Health Education. Int. J. Environ. Res. Public Health 2020, 17, 4217. [Google Scholar] [CrossRef]
- Knerer, G.; Currie, C.S.M.; Brailsford, S.C. Reducing dengue fever cases at the lowest budget: A constrained optimization approach applied to Thailand. BMC Public Health 2021, 21, 807. [Google Scholar] [CrossRef]
- Zeng, Z.; Zhan, J.; Chen, L.; Chen, H.; Cheng, S. Global, regional, and national dengue burden from 1990 to 2017: A systematic analysis based on the global burden of disease study 2017. EClinicalMedicine 2021, 32, 100712. [Google Scholar] [CrossRef]
- Messina, J.P.; Brady, O.J.; Golding, N.; Kraemer, M.U.G.; Wint, G.R.W.; Ray, S.E.; Pigott, D.M.; Shearer, F.M.; Johnson, K.; Earl, L.; et al. The current and future global distribution and population at risk of dengue. Nat. Microbiol. 2019, 4, 1508–1515. [Google Scholar] [CrossRef]
- Messina, J.P.; Brady, O.J.; Scott, T.W.; Zou, C.; Pigott, D.M.; Duda, K.A.; Bhatt, S.; Katzelnick, L.; Howes, R.E.; Battle, K.E.; et al. Global spread of dengue virus types: Mapping the 70 year history. Trends Microbiol. 2014, 22, 138–146. [Google Scholar] [CrossRef]
- Champagne, C.; Paul, R.; Ly, S.; Duong, V.; Leang, R.; Cazelles, B. Dengue modeling in rural Cambodia: Statistical performance versus epidemiological relevance. Epidemics 2019, 26, 43–57. [Google Scholar] [CrossRef]
- ECDC Dengue Worldwide Overview. Available online: https://www.ecdc.europa.eu/en/dengue-monthly (accessed on 15 March 2023).
- CDC Dengue around the World. Available online: https://www.cdc.gov/dengue/areaswithrisk/around-the-world.html (accessed on 15 March 2023).
- Kolimenakis, A.; Heinz, S.; Wilson, M.L.; Winkler, V.; Yakob, L.; Michaelakis, A.; Papachristos, D.; Richardson, C.; Horstick, O. The role of urbanisation in the spread of Aedes mosquitoes and the diseases they transmit—A systematic review. PLoS Negl. Trop. Dis. 2021, 15, e0009631. [Google Scholar] [CrossRef]
- Gupta, B.P.; Tuladhar, R.; Kurmi, R.; Manandhar, K. Das Dengue periodic outbreaks and epidemiological trends in Nepal. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 6. [Google Scholar] [CrossRef]
- Imad, H.A.; Phadungsombat, J.; Nakayama, E.E.; Chatapat, L.; Pisutsan, P.; Matsee, W.; Piyaphanee, W.; Nguitragool, W.; Shioda, T. A Cluster of Dengue Cases in Travelers: A Clinical Series from Thailand. Trop. Med. Infect. Dis. 2021, 6, 152. [Google Scholar] [CrossRef]
- Bhatia, S.; Bansal, D.; Patil, S.; Pandya, S.; Ilyas, Q.M.; Imran, S. A Retrospective Study of Climate Change Affecting Dengue: Evidences, Challenges and Future Directions. Front. Public Health 2022, 10, 1418. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.-L.; Tseng, W.-C.; Chen, C.-C.; Liao, S.-Y. Estimating the Threshold Effects of Climate on Dengue: A Case Study of Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 1392. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.J.; Carlson, C.J.; Mordecai, E.A.; Johnson, L.R. Global expansion and redistribution of Aedes-borne virus transmission risk with climate change. PLoS Negl. Trop. Dis. 2019, 13, e0007213. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A. Risk of Dengue in Travelers: Implications for Dengue Vaccination. Curr. Infect. Dis. Rep. 2018, 20, 50. [Google Scholar] [CrossRef]
- Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A.; Stanaway, J.D. The global economic burden of dengue: A systematic analysis. Lancet Infect. Dis. 2016, 16, 935–941. [Google Scholar] [CrossRef]
- Hung, T.M.; Van Hao, N.; Yen, L.M.; McBride, A.; Dat, V.Q.; van Doorn, H.R.; Loan, H.T.; Phong, N.T.; Llewelyn, M.J.; Nadjm, B.; et al. Direct Medical Costs of Tetanus, Dengue, and Sepsis Patients in an Intensive Care Unit in Vietnam. Front. Public Health 2022, 10, 1665. [Google Scholar] [CrossRef]
- Xu, M.; Chang, N.; Tu, T.; Sun, J.; Jiang, J.; Xia, Y.; Tang, W.; Ji, H.; Zhao, X.; Zhu, J.; et al. Economic burden of dengue fever in China: A retrospective research study. PLoS Negl. Trop. Dis. 2022, 16, e0010360. [Google Scholar] [CrossRef]
- Shepard, D.S.; Undurraga, E.A.; Halasa, Y.A. Economic and Disease Burden of Dengue in Southeast Asia. PLoS Negl. Trop. Dis. 2013, 7, e2055. [Google Scholar] [CrossRef]
- Lee, J.-S.; Mogasale, V.; Lim, J.K.; Ly, S.; Lee, K.S.; Sorn, S.; Andia, E.; Carabali, M.; Namkung, S.; Lim, S.-K.; et al. A multi-country study of the economic burden of dengue fever based on patient-specific field surveys in Burkina Faso, Kenya, and Cambodia. PLoS Negl. Trop. Dis. 2019, 13, e0007164. [Google Scholar] [CrossRef]
- Suaya, J.A.; Shepard, D.S.; Siqueira, J.B.; Martelli, C.T.; Lum, L.C.S.; Tan, L.H.; Kongsin, S.; Jiamton, S.; Garrido, F.; Montoya, R.; et al. Cost of Dengue Cases in Eight Countries in the Americas and Asia: A Prospective Study. Am. J. Trop. Med. Hyg. 2009, 80, 846–855. [Google Scholar] [CrossRef] [PubMed]
- Baly, A.; Toledo, M.E.; Rodriguez, K.; Benitez, J.R.; Rodriguez, M.; Boelaert, M.; Vanlerberghe, V.; Van der Stuyft, P. Costs of dengue prevention and incremental cost of dengue outbreak control in Guantanamo, Cuba. Trop. Med. Int. Health 2012, 17, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Halasa-Rappel, Y.A.; Baurin, N.; Coudeville, L.; Shepard, D.S. Cost-effectiveness of dengue vaccination in ten endemic countries. Vaccine 2018, 36, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, R.C.; Carrasquilla, G.; Porras, A.; Galera-Gelvez, K.; Yescas, J.G.L.; Rueda-Gallardo, J.A. The Burden of Dengue and the Financial Cost to Colombia, 2010–2012. Am. J. Trop. Med. Hyg. 2016, 94, 1065. [Google Scholar] [CrossRef]
- Canyon, D. V Historical analysis of the economic cost of dengue in Australia. J Vector Borne Dis 2008, 45, 245–248. [Google Scholar]
- Guzzetta, G.; Trentini, F.; Poletti, P.; Baldacchino, F.A.; Montarsi, F.; Capelli, G.; Rizzoli, A.; Rosà, R.; Merler, S.; Melegaro, A. Effectiveness and economic assessment of routine larviciding for prevention of chikungunya and dengue in temperate urban settings in Europe. PLoS Negl. Trop. Dis. 2017, 11, e0005918. [Google Scholar] [CrossRef]
- da Oliveira, L.N.S.; Itria, A.; Lima, E.C. Cost of illness and program of dengue: A systematic review. PLoS ONE 2019, 14, e0211401. [Google Scholar] [CrossRef]
- Gutiérrez-Bugallo, G.; Boullis, A.; Martinez, Y.; Hery, L.; Rodríguez, M.; Bisset, J.A.; Vega-Rúa, A. Vector competence of Aedes aegypti from Havana, Cuba, for dengue virus type 1, chikungunya, and Zika viruses. PLoS Negl. Trop. Dis. 2020, 14, e0008941. [Google Scholar] [CrossRef]
- Lopez-Gatell, H.; Hernandez-Avila, M.; Hernández Avila, J.E.; Alpuche-Aranda, C.M. Dengue in Latin America: A Persistent and Growing Public Health Challenge; Springer: Vienna, Austria, 2015; pp. 203–224. ISBN 9783709114223. [Google Scholar]
- PAHO Reported Cases of Dengue Fever in The Americas. Available online: https://www3.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en/dengue-nacional-en/252-dengue-pais-ano-en.html (accessed on 18 January 2023).
- Tapia-Conyer, R.; Betancourt-Cravioto, M.; Méndez-Galván, J. Dengue: An escalating public health problem in Latin America. Paediatr. Int. Child Health 2012, 32, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Shepard, D.S.; Coudeville, L.; Halasa, Y.A.; Zambrano, B.; Dayan, G.H. Economic Impact of Dengue Illness in the Americas. Am. J. Trop. Med. Hyg. 2011, 84, 200–207. [Google Scholar] [CrossRef] [PubMed]
- San Martín, J.L.; Brathwaite Dick, O.; del Diego, J.; Montoya, R.H.; Dayan, G.H.; Zambrano, B. The History of Dengue Outbreaks in the Americas. Am. J. Trop. Med. Hyg. 2012, 87, 584–593. [Google Scholar] [CrossRef]
- Nunez-Avellaneda, D.; Tangudu, C.; Barrios-Palacios, J.; Machain-Williams, C.; Alarcón-Romero, L.D.C.; Zubillaga-Guerrero, M.I.; Nunez-Avellaneda, S.; McKeen, L.A.; Canche-Aguilar, I.; Loaeza-Díaz, L.; et al. Co-Circulation of All Four Dengue Viruses and Zika Virus in Guerrero, Mexico, 2019. Vector-Borne Zoonotic Dis. 2021, 21, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Laserna, A.; Barahona-Correa, J.; Baquero, L.; Castañeda-Cardona, C.; Rosselli, D. Economic impact of dengue fever in Latin America and the Caribbean: A systematic review. Rev. Panam. Salud Pública 2018, 42, e111. [Google Scholar] [CrossRef]
- del Castillo Signor, L.C.; Edwards, T.; Escobar, L.E.; Mencos, Y.; Matope, A.; Castaneda-Guzman, M.; Adams, E.R.; Cuevas, L.E. Epidemiology of dengue fever in Guatemala. PLoS Negl. Trop. Dis. 2020, 14, e0008535. [Google Scholar] [CrossRef]
- Douglas, K.O.; Dutta, S.K.; Martina, B.; Anfasa, F.; Samuels, T.A.; Gittens-St. Hilaire, M. Dengue Fever and Severe Dengue in Barbados, 2008–2016. Trop. Med. Infect. Dis. 2020, 5, 68. [Google Scholar] [CrossRef]
- Flamand, C.; Quenel, P.; Ardillon, V.; Carvalho, L.; Bringay, S.; Teisseire, M. The Epidemiologic Surveillance of Dengue-Fever in French Guiana: When Achievements Trigger Higher Goals. Stud. Health Technol. Inform. 2011, 169, 629–633. [Google Scholar] [CrossRef]
- Teixeira, M.G.; Lima, M.B.; Guerra, Z. Epidemiologia e medidas de prevenção do Dengue. Inf. Epidemiol. Sus. 1999, 8, 5–33. [Google Scholar]
- Flamand, C.; Fritzell, C.; Prince, C.; Abboud, P.; Ardillon, V.; Carvalho, L.; Demar, M.; Boukhari, R.; Papaix-Puech, M.; Elenga, N.; et al. Epidemiological assessment of the severity of dengue epidemics in French Guiana. PLoS ONE 2017, 12, e0172267. [Google Scholar] [CrossRef]
- Chen, Y.; Li, N.; Lourenço, J.; Wang, L.; Cazelles, B.; Dong, L.; Li, B.; Liu, Y.; Jit, M.; Bosse, N.I.; et al. Measuring the effects of COVID-19-related disruption on dengue transmission in southeast Asia and Latin America: A statistical modelling study. Lancet Infect. Dis. 2022, 22, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, C. Pandemic May Be Masking Cases of Arbovirus Diseases, Indicates Seminar. Available online: https://portal.fiocruz.br/en/news/pandemic-may-be-masking-cases-arbovirus-diseases-indicates-seminar (accessed on 17 January 2023).
- Bardach, A.E.; García-Perdomo, H.A.; Alcaraz, A.; Tapia López, E.; Gándara, R.A.R.; Ruvinsky, S.; Ciapponi, A. Interventions for the control of Aedes aegypti in Latin America and the Caribbean: Systematic review and meta-analysis. Trop. Med. Int. Health 2019, 24, 530–552. [Google Scholar] [CrossRef] [PubMed]
- Sarti, E.; Cox, H.; Besada-Lombana, S.; Tapia-Maruri, L. Dengue Awareness in Latin American Populations: A Questionnaire Study. Infect. Dis. Ther. 2015, 4, 199–211. [Google Scholar] [CrossRef]
- Cabrera, M.; Leake, J.; Naranjo-Torres, J.; Valero, N.; Cabrera, J.C.; Rodríguez-Morales, A.J. Dengue Prediction in Latin America Using Machine Learning and the One Health Perspective: A Literature Review. Trop. Med. Infect. Dis. 2022, 7, 322. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.C.; Wilson, M.E.; Bloom, D.E. Disease and economic burdens of dengue. Lancet Infect. Dis. 2017, 17, e70–e78. [Google Scholar] [CrossRef] [PubMed]
- Tiga, D.C.; Undurraga, E.A.; Ramos-Castañeda, J.; Martínez-Vega, R.A.; Tschampl, C.A.; Shepard, D.S. Persistent Symptoms of Dengue: Estimates of the Incremental Disease and Economic Burden in Mexico. Am. J. Trop. Med. Hyg. 2016, 94, 1085–1089. [Google Scholar] [CrossRef]
- de Aguiar, D.F.; de Barros, E.N.C.; Ribeiro, G.S.; Brasil, P.; Mourao, M.P.G.; Luz, K.; Aoki, F.H.; Freitas, A.R.R.; Calvet, G.A.; Oliveira, E.; et al. A prospective, multicentre, cohort study to assess the incidence of dengue illness in households from selected communities in Brazil (2014–2018). Int. J. Infect. Dis. 2021, 108, 443–453. [Google Scholar] [CrossRef]
- Codeco, C.T.; Oliveira, S.S.; Ferreira, D.A.C.; Riback, T.I.S.; Bastos, L.S.; Lana, R.M.; Almeida, I.F.; Godinho, V.B.; Cruz, O.G.; Coelho, F.C. Fast expansion of dengue in Brazil. Lancet Reg. Health-Am. 2022, 12, 100274. [Google Scholar] [CrossRef]
- Böhm, A.W.; dos Costa, C.S.; Neves, R.G.; Flores, T.R.; Nunes, B.P. Tendência da incidência de dengue no Brasil, 2002–2012. Epidemiol. Serviços Saúde 2016, 25, 725–733. [Google Scholar] [CrossRef]
- Santos, C.H.; de Sousa, F.Y.; Ramos de Lima, L.; Stival, M.M. Perfil Epidemiológico do Dengue em Anápolis-GO, 2001–2007. Rev. Patol. Trop. 2010, 38, 249–260. [Google Scholar] [CrossRef]
- de Figueiredo, M.L.G.; Alfonso, H.L.; Amarilla, A.A.; Figueiredo, L.T.M.; Aquino, V.H.; da Costa, C.A.; Luz, S.L.B. Detection of DENV-4 genotype I from mosquitoes collected in the city of Manaus, Brazil. Virol. J. 2013, 10, 60. [Google Scholar] [CrossRef]
- Coelho, I.C.B.; Haguinet, F.; Colares, J.K.B.; Coelho, Z.C.B.; Araújo, F.M.C.; Dias Schwarcz, W.; Duarte, A.C.; Borges, B.; Minguet, C.; Guignard, A. Dengue Infection in Children in Fortaleza, Brazil: A 3-Year School-Based Prospective Cohort Study. Am. J. Trop. Med. Hyg. 2020, 103, 100–111. [Google Scholar] [CrossRef] [PubMed]
- DATASUS DENGUE-Notificações Registradas No Sistema de Informação de Agravos de Notificação-Brasil. Available online: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinannet/cnv/denguebbr.def (accessed on 10 March 2023).
- PAHO Dengue Serotypes. Available online: https://www3.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en/dengue-nacional-en/517-dengue-serotypes-en.html (accessed on 10 March 2023).
- Alves, J.A.; Santos, J.R.; de Mendonça, E.N.; Abud, A.C.; Nunes, M.d.a.S.; Fakhouri, R.; Inagaki, A.D.; Marchioro, M.; Antoniolli, A.R. Epidemiological aspects of dengue in Aracaju, State of Sergipe, Brazil. Rev. Soc. Bras. Med. Trop. 2011, 44, 670–673. [Google Scholar] [CrossRef] [PubMed]
- Junior, J.B.S.; Massad, E.; Lobao-Neto, A.; Kastner, R.; Oliver, L.; Gallagher, E. Epidemiology and costs of dengue in Brazil: A systematic literature review. Int. J. Infect. Dis. 2022, 122, 521–528. [Google Scholar] [CrossRef]
- Oneda, R.M.; Basso, S.R.; Frasson, L.R.; Mottecy, N.M.; Saraiva, L.; Bassani, C. Epidemiological profile of dengue in Brazil between the years 2014 and 2019. Rev. Assoc. Med. Bras. 2021, 67, 731–735. [Google Scholar] [CrossRef]
- Guzzetta, G.; Marques-Toledo, C.A.; Rosà, R.; Teixeira, M.; Merler, S. Quantifying the spatial spread of dengue in a non-endemic Brazilian metropolis via transmission chain reconstruction. Nat. Commun. 2018, 9, 2837. [Google Scholar] [CrossRef] [PubMed]
- Vilela, A.P.P.; Miranda, D.P.J.; Andrade, E.H.P.; Abrahão, J.S.; Araújo, V.E.M.; Zibaoui, H.M.; Oliveira, J.G.; Rosa, J.C.C.; Figueiredo, L.B.; Kroon, E.G.; et al. Spatial–Temporal Co-Circulation of Dengue Virus 1, 2, 3, and 4 Associated with Coinfection Cases in a Hyperendemic Area of Brazil: A 4-Week Survey. Am. J. Trop. Med. Hyg. 2016, 94, 1080–1084. [Google Scholar] [CrossRef]
- Brito, A.F.; Machado, L.C.; Oidtman, R.J.; Siconelli, M.J.L.; Tran, Q.M.; Fauver, J.R.; de Carvalho, R.D.O.; Dezordi, F.Z.; Pereira, M.R.; de Castro-Jorge, L.A.; et al. Lying in wait: The resurgence of dengue virus after the Zika epidemic in Brazil. Nat. Commun. 2021, 12, 2619. [Google Scholar] [CrossRef]
- Martelli, C.M.T.; Siqueira, J.B.; Parente, M.P.P.D.; de Sene Amancio Zara, A.L.; Oliveira, C.S.; Braga, C.; Pimenta, F.G.; Cortes, F.; Lopez, J.G.; Bahia, L.R.; et al. Economic Impact of Dengue: Multicenter Study across Four Brazilian Regions. PLoS Negl. Trop. Dis. 2015, 9, e0004042. [Google Scholar] [CrossRef]
- Godói, I.P.; Da Silva, L.V.D.; Sarker, A.R.; Megiddo, I.; Morton, A.; Godman, B.; Alvarez-Madrazo, S.; Bennie, M.; Guerra-Junior, A.A. Economic and epidemiological impact of dengue illness over 16 years from a public health system perspective in Brazil to inform future health policies including the adoption of a dengue vaccine. Expert Rev. Vaccines 2018, 17, 1123–1133. [Google Scholar] [CrossRef]
- Durham, D.P.; Ndeffo Mbah, M.L.; Medlock, J.; Luz, P.M.; Meyers, L.A.; Paltiel, A.D.; Galvani, A.P. Dengue dynamics and vaccine cost-effectiveness in Brazil. Vaccine 2013, 31, 3957–3961. [Google Scholar] [CrossRef]
- Castro Rodriguez, R.; Rueda-Gallardo, J.; Avella Niño, M.; Lopez, J.; Caicedo Navas, A. Costo-Efectividad De La Vacuna Contra El Dengue 2014. Value Health 2015, 18, A871–A872. [Google Scholar] [CrossRef]
- Godói, I.P.; Santos, A.S.; Reis, E.A.; Lemos, L.L.P.; Brandão, C.M.R.; Alvares, J.; Acurcio, F.A.; Godman, B.; Guerra Júnior, A.A. Consumer Willingness to Pay for Dengue Vaccine (CYD-TDV, Dengvaxia®) in Brazil; Implications for Future Pricing Considerations. Front. Pharmacol. 2017, 8, 41. [Google Scholar] [CrossRef] [PubMed]
- Crépey, P.; Boiron, L.; Araujo, R.R.; Lopez, J.G.; Petitjean, A.; de Albuquerque Luna, E.J. Impact of quadrivalent influenza vaccines in Brazil: A cost-effectiveness analysis using an influenza transmission model. BMC Public Health 2020, 20, 1374. [Google Scholar] [CrossRef]
- Shim, E. Cost-Effectiveness of Dengue Vaccination Programs in Brazil. Am. J. Trop. Med. Hyg. 2017, 96, 1227–1234. [Google Scholar] [CrossRef]
- da Silva Augusto, L.G.; Gurgel, A.M.; Costa, A.M.; Diderichsen, F.; Lacaz, F.A.; Parra-Henao, G.; Rigotto, R.M.; Nodari, R.; Santos, S.L. Aedes aegypti control in Brazil. Lancet 2016, 387, 1052–1053. [Google Scholar] [CrossRef] [PubMed]
- Preto, C.; Maron de Mello, A.; Cesário Pereira Maluf, E.M.; Teixeira Krainski, E.; Graeff, G.; de Sousa, G.A.; da Silva, L.R.; Vieira da Costa-Ribeiro, M.C.; da Cruz Magalhães Buffon, M.; Shimakura, S.E.; et al. Vaccination coverage and adherence to a dengue vaccination program in the state of Paraná, Brazil. Vaccine 2021, 39, 711–719. [Google Scholar] [CrossRef]
- Donateli, C.P.; do Einloft, A.B.N.; Coutinho Junior, A.L.; Cotta, R.M.M.; Costa, G.D. da Endemic Disease Control Agents’ perception on the fight against Aedes aegypti and the prevention of arbovirus infections in Brazil. PLoS Negl. Trop. Dis. 2019, 13, e0007741. [Google Scholar] [CrossRef] [PubMed]
- Araújo, H.; Carvalho, D.; Ioshino, R.; Costa-da-Silva, A.; Capurro, M. Aedes aegypti Control Strategies in Brazil: Incorporation of New Technologies to Overcome the Persistence of Dengue Epidemics. Insects 2015, 6, 576–594. [Google Scholar] [CrossRef]
- Luna, E.; Figueiredo, G.; Levi, J.; Campos, S.; Felix, A.; Souza, N.; Figueiredo, W.; Costa, A.; Cardoso, M.; Pannuti, C. Data on dengue incidence in South-eastern Brazil, 2014–2018. Data Br. 2020, 29, 105266. [Google Scholar] [CrossRef]
- Paes de Andrade, P.; Aragão, F.J.L.; Colli, W.; Dellagostin, O.A.; Finardi-Filho, F.; Hirata, M.H.; Lira-Neto, A.D.C.; Almeida de Melo, M.; Nepomuceno, A.L.; Gorgônio da Nóbrega, F.; et al. Use of transgenic Aedes aegypti in Brazil: Risk perception and assessment. Bull. World Health Organ. 2016, 94, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Rahman, R.U.; Cosme, L.V.; Costa, M.M.; Carrara, L.; Lima, J.B.P.; Martins, A.J. Insecticide resistance and genetic structure of Aedes aegypti populations from Rio de Janeiro State, Brazil. PLoS Negl. Trop. Dis. 2021, 15, e0008492. [Google Scholar] [CrossRef]
- Guha-Sapir, D.; Schimmer, B. Dengue fever: New paradigms for a changing epidemiology. Emerg. Themes Epidemiol. 2005, 2, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kuno, G. Emergence of the Severe Syndrome and Mortality Associated with Dengue and Dengue-Like Illness: Historical Records (1890 to 1950) and Their Compatibility with Current Hypotheses on the Shift of Disease Manifestation. Clin. Microbiol. Rev. 2009, 22, 186–201. [Google Scholar] [CrossRef]
- Gubler, D.J. Dengue, Urbanization and Globalization: The Unholy Trinity of the 21st Century. Trop. Med. Health 2011, 39, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Faruk, M.O.; Jannat, S.N.; Rahman, M.S. Impact of environmental factors on the spread of dengue fever in Sri Lanka. Int. J. Environ. Sci. Technol. 2022, 19, 10637–10648. [Google Scholar] [CrossRef]
- The Lancet Looking for a volunteer to help fight dengue fever. Lancet 2007, 370, 458. [CrossRef]
- Andrioli, D.C.; Busato, M.A.; Lutinski, J.A. Spatial and temporal distribution of dengue in Brazil, 1990–2017. PLoS ONE 2020, 15, e0228346. [Google Scholar] [CrossRef]
- WHO Neglected Tropical Diseases. Available online: https://www.who.int/news-room/questions-and-answers/item/neglected-tropical-diseases (accessed on 19 January 2023).
- Horstick, O.; Tozan, Y.; Wilder-Smith, A. Reviewing Dengue: Still a Neglected Tropical Disease? PLoS Negl. Trop. Dis. 2015, 9, e0003632. [Google Scholar] [CrossRef]
- Bärnighausen, T.; Bloom, D.E.; Cafiero, E.T.; O’Brien, J.C. Valuing the broader benefits of dengue vaccination, with a preliminary application to Brazil. Semin. Immunol. 2013, 25, 104–113. [Google Scholar] [CrossRef]
- das Sousa, F.C.A.; Soares, H.V.A.; Lemos, L.E.A.S.; Reis, D.M.; da Silva, W.C.; de Rodrigues, L.A.S. Perfil epidemiológico de doenças negligenciadas de notificação compulsória no Brasil com análise dos investimentos governamentais nessa área. Res. Soc. Dev. 2020, 9, e62911610. [Google Scholar] [CrossRef]
- McAdams, D. The Blossoming of Economic Epidemiology. Annu. Rev. Econom. 2021, 13, 539–570. [Google Scholar] [CrossRef]
- Perrings, C.; Castillo-Chavez, C.; Chowell, G.; Daszak, P.; Fenichel, E.P.; Finnoff, D.; Horan, R.D.; Kilpatrick, A.M.; Kinzig, A.P.; Kuminoff, N.V.; et al. Merging Economics and Epidemiology to Improve the Prediction and Management of Infectious Disease. Ecohealth 2014, 11, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, J. Health Economics; Hyde, T., Tu, P., Eds.; Palgrave Macmillan: New York, NY, USA, 2014; ISBN 9781137029966. [Google Scholar]
- Philipson, T. Economic epidemiology and infectious diseases. In Handbook of Health Economics; Elsevier B.V.: Amsterdam, The Netherlands, 2000; Volume 1, pp. 1761–1799. [Google Scholar]
- Macinko, J.; Harris, M.J.; Rocha, M.G. Brazil’s National Program for Improving Primary Care Access and Quality (PMAQ). J. Ambul. Care Manag. 2017, 40, S4–S11. [Google Scholar] [CrossRef]
- Raude, J.; Peretti-Watel, P.; Ward, J.; Flamand, C.; Verger, P. Are Perceived Prevalences of Infection also Biased and How? Lessons from Large Epidemics of Mosquito-Borne Diseases in Tropical Regions. Med. Decis. Mak. 2018, 38, 377–389. [Google Scholar] [CrossRef]
- Broadbent, A.; Grote, T. Can Robots Do Epidemiology? Machine Learning, Causal Inference, and Predicting the Outcomes of Public Health Interventions. Philos. Technol. 2022, 35, 14. [Google Scholar] [CrossRef]
- de Saldanha, R.F.; Bastos, R.R.; Barcellos, C. Microdatasus: Pacote para download e pré-processamento de microdados do Departamento de Informática do SUS (DATASUS). Cad. Saude Publica 2019, 35. [Google Scholar] [CrossRef]
- de Morais, A.; de Konstantyner, T.C.R.O.; Fazenda, Á.L.; Sala, A.; Martins, C.B. Rtabnetsp: Pacote R para extração de indicadores de saúde do estado de São Paulo. Epidemiol. Serviços Saúde 2021, 30, 2021. [Google Scholar] [CrossRef]
- Corpuz, M.V.A.; Buonerba, A.; Vigliotta, G.; Zarra, T.; Ballesteros, F.; Campiglia, P.; Belgiorno, V.; Korshin, G.; Naddeo, V. Viruses in wastewater: Occurrence, abundance and detection methods. Sci. Total Environ. 2020, 745, 140910. [Google Scholar] [CrossRef]
- Fonseca, M.S.; Machado, B.A.S.; de Rolo, C.A.; Hodel, K.V.S.; dos Almeida, E.S.; de Andrade, J.B. Evaluation of SARS-CoV-2 concentrations in wastewater and river water samples. Case Stud. Chem. Environ. Eng. 2022, 6, 100214. [Google Scholar] [CrossRef]
- Mousazadeh, M.; Ashoori, R.; Paital, B.; Kabdaşlı, I.; Frontistis, Z.; Hashemi, M.; Sandoval, M.A.; Sherchan, S.; Das, K.; Emamjomeh, M.M. Wastewater Based Epidemiology Perspective as a Faster Protocol for Detecting Coronavirus RNA in Human Populations: A Review with Specific Reference to SARS-CoV-2 Virus. Pathogens 2021, 10, 1008. [Google Scholar] [CrossRef] [PubMed]
- Thakali, O.; Raya, S.; Malla, B.; Tandukar, S.; Tiwari, A.; Sherchan, S.P.; Sherchand, J.B.; Haramoto, E. Pilot study on wastewater surveillance of dengue virus RNA: Lessons, challenges, and implications for future research. Environ. Chall. 2022, 9, 100614. [Google Scholar] [CrossRef]
- Ishtiaq, F. India must scale up wastewater analysis for health surveillance. Nat. India 2022. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Country | New Cases Reported in 2022 | Level of Infection Risk |
|---|---|---|
| Asia | ||
| Afghanistan | 1266 | Sporadic/Uncertain |
| Bangladesh | 82,743 | Frequent/Continuous |
| Cambodia | 12,591 | Frequent/Continuous |
| China | 537 | Risk varies based on region |
| India | 110,473 | Risk varies based on region |
| Indonesia | 125,888 | Frequent/Continuous |
| Malaysia | 64,078 | Frequent/Continuous |
| Nepal | 54,784 | Frequent/Continuous |
| Pakistan | 78,554 | Risk varies based on region |
| Philippines | 220,705 | Frequent/Continuous |
| Singapore | 31,883 | Sporadic/Uncertain |
| Thailand | 33,489 | Frequent/Continuous |
| Vietnam | 367,729 | Frequent/Continuous |
| Africa | ||
| Kenya | 34 | Frequent/Continuous |
| São Tomé and Príncipe | 1161 | Sporadic/Uncertain |
| Somalia | 5350 | Frequent/Continuous |
| Sudan | 4800 | Frequent/Continuous |
| American | ||
| Brazil | 2,363,490 | Frequent/Continuous |
| Colombia | 69,497 | Frequent/Continuous |
| Mexico | 59,918 | Risk varies based on region |
| Nicaragua | 97,541 | Frequent/Continuous |
| Peru | 72,851 | Risk varies based on region |
| Australia and the Pacific | ||
| Australia | 407 | Frequent/Continuous |
| Fiji | 1960 | Frequent/Continuous |
| Vanuatu | 148 | Sporadic/Uncertain |
| Europe | ||
| France | 272 | Sporadic/Uncertain |
| Region | Country | Dengue-Related Costs (in USD) | Reference |
|---|---|---|---|
| Asia | Vietnam | The average cost for the ICU per inpatient is between 64.4 and 4250 | [67] |
| China | Total economic costs in 2019: ~460 million | [68] | |
| Indonesia | The aggregate cost of illness in 2010: >300 million The average cost per capita: >1.3 | [69] | |
| Thailand | The aggregate cost of illness in 2010: >290 million The average cost per capita: >4.34 | ||
| Singapore | The aggregate cost of illness in 2010: >67 million The average cost per capita: >12.65 | ||
| Cambodia | The aggregate cost of illness in 2010: >16 million The average cost per capita: >0.11 | ||
| Africa | Burkina Faso | The average cost of illness per inpatient: 26 The average economic costs per episode, considering outpatients: 13 | [70] |
| Kenya | The average economic costs per episode considering outpatients: 33 | ||
| America | El Salvador | The aggregate annual cost of illness: 1.7 million | [71] |
| Venezuela | The aggregate annual cost of illness: 10.2 million | ||
| Guatemala | The aggregate annual cost of illness: 1.2 million | ||
| Panama | The aggregate annual cost of illness: 0.9 million | ||
| Cuba | The average cost per hospitalized case: >296 | [72] | |
| Puerto Rico | The average cost per capita: 31.52 | [73] | |
| Honduras | The average cost per capita: 2.12 | ||
| Colombia | The total financial cost of the illness: 131.7 million | [74] | |
| Brazil | The annual aggregated cost of illness: 1014.3 million The average cost per dengue case: 531.63 | [66] | |
| Oceania | Australia | Total annual cost of illness: >2.7 million | [75] |
| Europe | Italy | The average cost per dengue case: ~290 | [76] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lessa, C.L.S.; Hodel, K.V.S.; Gonçalves, M.d.S.; Machado, B.A.S. Dengue as a Disease Threatening Global Health: A Narrative Review Focusing on Latin America and Brazil. Trop. Med. Infect. Dis. 2023, 8, 241. https://doi.org/10.3390/tropicalmed8050241
Lessa CLS, Hodel KVS, Gonçalves MdS, Machado BAS. Dengue as a Disease Threatening Global Health: A Narrative Review Focusing on Latin America and Brazil. Tropical Medicine and Infectious Disease. 2023; 8(5):241. https://doi.org/10.3390/tropicalmed8050241
Chicago/Turabian StyleLessa, Carlos Letacio Silveira, Katharine Valéria Saraiva Hodel, Marilda de Souza Gonçalves, and Bruna Aparecida Souza Machado. 2023. "Dengue as a Disease Threatening Global Health: A Narrative Review Focusing on Latin America and Brazil" Tropical Medicine and Infectious Disease 8, no. 5: 241. https://doi.org/10.3390/tropicalmed8050241
APA StyleLessa, C. L. S., Hodel, K. V. S., Gonçalves, M. d. S., & Machado, B. A. S. (2023). Dengue as a Disease Threatening Global Health: A Narrative Review Focusing on Latin America and Brazil. Tropical Medicine and Infectious Disease, 8(5), 241. https://doi.org/10.3390/tropicalmed8050241