
Seroprevalence of Strongyloides stercoralis in Patients about to Receive Immunosuppressive Treatment in Gran Canaria (Spain)

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
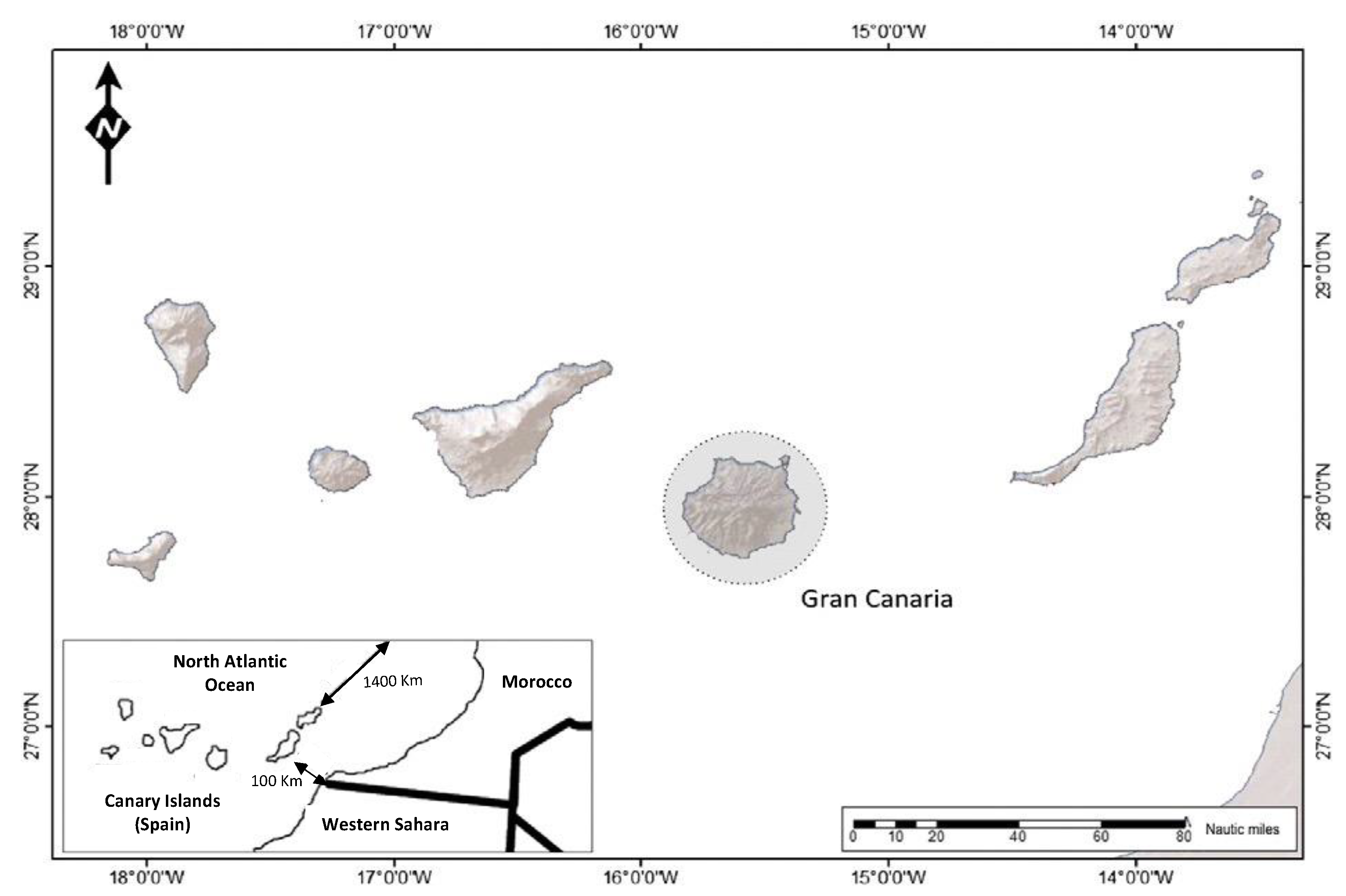
2.1. Study Site
2.2. Ethics Approval Statement
2.3. Study Design and Pupulation
2.4. Variables
- (i)
- Patient demographics: sex (male and female), age, country of origin (Spain, rest of Europe, Africa, America, and Asia), place of residence and occupation.
- (ii)
- Type of patient: pre-biological treatment or pre-kidney transplant
- (iii)
- Underlying pathology
- (iv)
- Presence of eosinophilia, defined as a total eosinophil count ≥450/µL and relative eosinophilia, defined as the percentage of eosinophils >5% but eosinophil count < 450/µL
2.5. Serological Study
2.6. Data Analysis
3. Results
3.1. Study Group
3.2. Control Group
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jourdan, P.M.; Lamberton, P.H.L.; Fenwick, A.; Addiss, D.G. Soil-transmitted helminth infections. Lancet 2018, 391, 252–265. [Google Scholar] [CrossRef] [PubMed]
- Bethony, J.; Brooker, S.; Albonico, M.; Geiger, S.M.; Loukas, A.; Diemert, D.; Hotez, P.J. Soil-transmitted helminth infections: Ascariasis, trichuriasis, and hookworm. Lancet 2006, 367, 1521–1532. [Google Scholar] [CrossRef] [PubMed]
- Schär, F.; Trostdorf, U.; Giardina, F.; Khieu, V.; Muth, S.; Marti, H.; Vounatsou, P.; Odermatt, P. Strongyloides stercoralis: Global Distribution and Risk Factors. PLoS Negl. Trop. Dis. 2013, 7, e2288. [Google Scholar] [CrossRef] [PubMed]
- Buonfrate, D.; Bisanzio, D.; Giorli, G.; Odermatt, P.; Fürst, T.; Greenaway, C.; French, M.; Reithinger, R.; Gobbi, F.; Montresor, A.; et al. The Global Prevalence of Strongyloides stercoralis Infection. Pathogens 2020, 9, 468. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Perez, A.; Lopez-Velez, R. Is strongyloidiasis endemic in Spain? PLoS Negl. Trop. Dis. 2015, 9, e0003482. [Google Scholar] [CrossRef] [PubMed]
- Barroso, M.; Salvador, F.; Sánchez-Montalvá, A.; Bosch-Nicolau, P.; Molina, I. Strongyloides stercoralis infection: A systematic review of endemic cases in Spain. PLoS Negl. Trop. Dis. 2019, 13, e0007230. [Google Scholar] [CrossRef] [PubMed]
- Mejia, R.; Nutman, T.B. Screening, prevention, and treatment for hyperinfection syndrome and disseminated infections caused by Strongyloides stercoralis. Curr. Opin. Infect. Dis. 2012, 25, 458–463. [Google Scholar] [CrossRef]
- Pardo Moreno, G.; Rodríguez Rodríguez, R.; Campillos Páez, M.T. Strongyloides stercoralis: Risk factors for disseminated infection. Med. Clin. 2003, 121, 662–664. [Google Scholar] [CrossRef]
- Ramos-Sesma, V.; Navarro, M.; Llenas-García, J.; Gil-Anguita, C.; Torrús-Tendero, D.; Wikman-Jorgensen, P.; Amador-Prous, C.; Ventero-Martín, M.-P.; Garijo-Sainz, A.-M.; García-López, M.; et al. Strongyloidiasis among Latin American Migrants in Spain: A Community-Based Approach. Pathogens 2020, 9, 511. [Google Scholar] [CrossRef]
- Eslahi, A.V.; Badri, M.; Nahavandi, K.H.; Houshmand, E.; Dalvand, S.; Riahi, S.M.; Johkool, M.G.; Asadi, N.; Ahangari, S.A.H.; Taghipour, A.; et al. Prevalence of strongyloidiasis in the general population of the world: A systematic review and meta-analysis. Pathog. Glob. Health 2021, 115, 7–20. [Google Scholar] [CrossRef]
- Siddiqui, A.A.; Berk, S.L. Diagnosis of Strongyloides stercoralis infection. Clin. Infect. Dis. 2001, 33, 1040–1047. [Google Scholar] [CrossRef] [PubMed]
- Requena-Méndez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Muñoz, J. The laboratory diagnosis and follow up of strongyloidiasis: A systematic review. PLoS Negl. Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef] [PubMed]
- Luvira, V.; Chantawat, N.; Naaglor, T.; Dekumyoy, P.; Mungthin, M.; Trakulhun, K.; Phiboonbanakit, D.; Pakdee, W. Comparative Diagnosis of Strongyloidiasis in Immunocompromised Patients. Am. J. Trop. Med. Hyg. 2016, 95, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Nadir, E.; Grossman, T.; Ciobotaro, P.; Attali, M.; Barkan, D.; Bardenstein, R.; Zimhony, O. Real-time PCR for Strongyloides stercoralis-associated meningitis. Diagn. Microbiol. Infect. Dis. 2016, 84, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Verweij, J.J.; Canales, M.; Polman, K.; Ziem, J.; Brienen, E.A.; Polderman, A.M.; van Lieshout, L. Molecular diagnosis of Strongyloides stercoralis in faecal samples using real-time PCR. Trans. R Soc. Trop. Med. Hyg. 2009, 103, 342–346. [Google Scholar] [CrossRef] [PubMed]
- Schär, F.; Odermatt, P.; Khieu, V.; Panning, M.; Duong, S.; Muth, S.; Marti, H.; Kramme, S. Evaluation of real-time PCR for Strongyloides stercoralis and hookworm as diagnostic tool in asymptomatic schoolchildren in Cambodia. Acta Trop. 2013, 126, 89–92. [Google Scholar] [CrossRef]
- Becker, S.L.; Piraisoody, N.; Kramme, S.; Marti, H.; Silué, K.D.; Panning, M.; von Müller, L. Real-time PCR for detection of Strongyloides. stercoralis in human stool samples from Côte d’Ivoire: Diagnostic accuracy, inter-laboratory comparison and patterns of hookworm co-infection. Acta Trop. 2015, 150, 210–217. [Google Scholar] [CrossRef]
- Meurs, L.; Polderman, A.M.; Vinkeles Melchers, N.V.; Brienen, E.A.; Verweij, J.J.; Groosjohan, B.; van Lieshout, L. Diagnosing Polyparasitism in a High-Prevalence Setting in Beira, Mozambique: Detection of Intestinal Parasites in Fecal Samples by Microscopy and Real-Time PCR. PLoS Negl. Trop. Dis. 2017, 11, e0005310. [Google Scholar] [CrossRef]
- Buonfrate, D.; Mendez, A.R.; Angheben, A.; Cinquini, M.; Cruciani, M.; Fittipaldo, A.V.; Giorli, G.; Gobbi, F.; Piubelli, C.; Bisoffi, Z. Accuracy of molecular biology techniques for the diagnosis of Strongyloides stercoralis infection-A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006229. [Google Scholar] [CrossRef]
- Autier, B.; Gangneux, J.P.; Robert-Gangneux, F. Evaluation of the Allplex™ GI-Helminth(I) Assay, the first marketed multiplex PCR for helminth diagnosis. Parasite 2021, 28, 33. [Google Scholar] [CrossRef]
- Bisoffi, Z.; Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Gobbo, M.; Bonafini, S.; Angheben, A.; et al. Diagnostic accuracy of five serologic tests for Strongyloides stercoralis infection. PLoS Negl. Trop. Dis. 2014, 8, e2640. [Google Scholar] [CrossRef] [PubMed]
- Kalantari, N.; Chehrazi, M.; Ghaffari, S.; Gorgani-Firouzjaee, T. Serological assays for the diagnosis of Strongyloides stercoralis infection: A systematic review and meta-analysis of diagnostic test accuracy. Trans. R Soc. Trop. Med. Hyg. 2020, 114, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Carnino, L.; Schwob, J.M.; Gétaz, L.; Nickel, B.; Neumayr, A.; Eperon, G. A Practical Approach to Screening for Strongyloides stercoralis. Trop. Med. Infect. Dis. 2021, 6, 203. [Google Scholar] [CrossRef]
- Ahmad, H.; Balachandra, D.; Arifin, N.; Nolan, T.J.; Lok, J.B.; Khan, A.H.; Yunus, M.H.; Noordin, R. Diagnostic Potential of an IgE-ELISA in Detecting Strongyloidiasis. Am. J. Trop. Med. Hyg. 2020, 103, 2288–2293. [Google Scholar] [CrossRef]
- Anderson, N.W.; Klein, D.M.; Dornink, S.M.; Jespersen, D.J.; Kubofcik, J.; Nutman, T.B.; Merrigan, S.D.; Couturier, M.R.; Theel, E.S. Comparison of three immunoassays for detection of antibodies to Strongyloides stercoralis. Clin. Vaccine Immunol. 2014, 21, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Fradejas, I.; Herrero-Martínez, J.M.; Lizasoaín, M.; Rodríguez de Las Parras, E.; Pérez-Ayala, A. Comparative study of two commercial tests for Strongyloides. stercoralis serologic diagnosis. Trans. R Soc. Trop. Med. Hyg. 2018, 112, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Alcaraz, C.O.; Adell, R.I.; Sánchez, P.S.; Blasco MJ, V.; Sánchez, O.A.; Auñón, A.S.; Calabuig, D.R. Characteristics and geographical profile of strongyloidiasis in healthcare area 11 of the Valencian community (Spain). J. Infect. 2004, 49, 152–158. [Google Scholar] [CrossRef]
- Novo-Veleiro, I.; Martin-Sánchez, A.M.; Elcuaz Romano, R.; Afonso-Rodriguez, O.; García Bardeci, D.; Bordes Benitez, A.; Carranza-Rodriguez, C.; Hernández-Cabrera, M.; Alvela-Suárez, L.; Pérez-Arellano, J.L. Parasitic diseases in Gran Canaria (Spain). Multicenter prospective study for one year. Rev. Ibero-Lat. Parasitol. 2012, 1, 34–41. [Google Scholar]
- McDonald, H.H.; Moore, M. Strongyloides stercoralis Hyperinfection. N. Engl. J. Med. 2017, 376, 2376. [Google Scholar] [CrossRef]
- Dykie, A.; Wijesinghe, T.; Rabson, A.B.; Madugula, K.; Farinas, C.; Wilson, S.; Jain, P. Human T-cell Leukemia Virus Type 1 and Strongyloides. stercoralis: Partners in Pathogenesis. Pathogens 2020, 9, 904. [Google Scholar] [CrossRef]
- Salvador, F.; Ribera, E.; Crespo, M.; Falcó, V.; Curran, A.; Ocaña, I.; Eynde, E.V.D.; Molina, I.; Pahissa, A.; Navarro, J.; et al. Tropical diseases screening in immigrant patients with human immunodeficiency virus infection in Spain. Am. J. Trop. Med. Hyg. 2013, 88, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Vilela, E.G.; Clemente, W.T.; Mira RR, L.; Torres HO, G.; Veloso, L.F.; Fonseca, L.P.; Lima, A.S. Strongyloides stercoralis hyperinfection syndrome after liver transplantation: Case report and literature review. Transpl. Infect. Dis. 2009, 11, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.W.; Abt, P.L.; Rosenbach, M.A.; Bleicher, M.B.; Levine, M.S.; Mehta, J.; Montgomery, S.P.; Hasz, R.D.; Bono, B.R.; Tetzlaff, M.T.; et al. Donor-derived Strongyloides. stercoralis infections in renal transplant recipients. Transplantation 2011, 91, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.T.; Fernandez-Ruiz, M.; Grossi, P.A.; Hernandez-Jimenez, P.; Lopez-Medrano, F.; Mularoni, A.; Aguado, J.M. Reactivation of latent infections in solid organ transplant recipients from sub-Saharan Africa: What should be remembered? Transpl. Rev. 2021, 35, 100632. [Google Scholar] [CrossRef] [PubMed]
- Keiser, P.B.; Nutman, T.B. Strongyloides stercoralis in the Immunocompromised Population. Clin. Microbiol. Rev. 2004, 17, 208–217. [Google Scholar] [CrossRef]
- Camargo, L.F.A.; Kamar, N.; Gotuzzo, E.; Wright, A.J. Schistosomiasis and Strongyloidiasis Recommendations for Solid-Organ Transplant Recipients and Donors. Transplantation 2018, 102 (Suppl. S2), S27–S34. [Google Scholar] [CrossRef]
- Clemente, W.T.; Pierrotti, L.C.; Abdala, E.; Morris, M.I.; Azevedo, L.S.; López-Vélez, R.; Aguado, J.M. Recommendations for Management of Endemic Diseases and Travel Medicine in Solid-Organ Transplant Recipients and Donors: Latin America. Transplantation 2018, 102, 193–208. [Google Scholar] [CrossRef]
- Winnicki, W.; Eder, M.; Mazal, P.; Mayer, F.J.; Sengölge, G.; Wagner, L. Prevalence of Strongyloides stercoralis infection and hyperinfection syndrome among renal allograft recipients in Central Europe. Sci. Rep. 2018, 8, 15406. [Google Scholar] [CrossRef]
- Chatani, B.; Selvaggi, G.; Garcia, J.; Gonzalez, I.A. Describing universal Strongyloides serologic screening among pediatric intestinal and liver transplant recipients. Pediatr Transp. 2021, 25, e14039. [Google Scholar] [CrossRef]
- Kottkamp, A.C.; Filardo, T.D.; Holzman, R.S.; Aguero-Rosenfeld, M.; Neumann, H.J.; Mehta, S.A. Prevalence of strongyloidiasis among cardiothoracic organ transplant candidates in a non-endemic region: A single-center experience with universal screening. Transpl. Infect. Dis. 2021, 23, e13614. [Google Scholar] [CrossRef]
- Baddley, J.W.; Cantini, F.; Goletti, D.; Gómez-Reino, J.J.; Mylonakis, E.; San-Juan, R.; Fernández-Ruiz, M.; Torre-Cisneros, J. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the safety of targeted and biological therapies: An infectious diseases perspective (Introduction). Clin. Microbiol. Infect. 2018, 24 (Suppl. S2), S10–S20. [Google Scholar] [CrossRef] [PubMed]
- Boatright, M.D.; Wang, B.W. Clinical infection with Strongyloides stercoralis following etanercept use for rheumatoid arthritis. Arthritis Rheum. 2005, 52, 1336–1337. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, M.; Sinyagovskiy, P.; Mohamed, W.; Abdelghani, A. Pulmonary strongyloidiasis causing septic shock in a patient with Crohn’s disease. Respir. Med. Case Rep. 2018, 24, 52–54. [Google Scholar] [CrossRef]
- Krishnamurthy, R.; Dincer, H.E.; Whittemore, D. Strongyloides stercoralis hyperinfection in a patient with rheumatoid arthritis after anti-TNF-alpha therapy. J. Clin. Rheumatol. 2007, 13, 150–152. [Google Scholar] [CrossRef]
- Hashiba, Y.; Umekita, K.; Minami, H.; Kawano, A.; Nagayasu, E.; Maruyama, H.; Hidaka, T.; Okayama, A. Strongyloides stercoralis colitis in a patient positive for human T-cell leukaemia virus with rheumatoid arthritis during an anti-rheumatic therapy: A case report. Mod. Rheumatol. Case Rep. 2021, 5, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Maurice, M.M.; van der Graaff, W.L.; Leow, A.; Breedveld, F.C.; van Lier, R.A.; Verweij, C.L. Treatment with monoclonal anti-tumor necrosis factor alpha antibody results in an accumulation of Th1 CD4+ T cells in the peripheral blood of patients with rheumatoid arthritis. Arthritis Rheum. 1999, 42, 2166–2173. [Google Scholar] [CrossRef] [PubMed]
- Lier, A.J.; Tuan, J.J.; Davis, M.W.; Paulson, N.; McManus, D.; Campbell, S.; Peaper, D.R.; Topal, J.E. Case Report: Disseminated Strongyloidiasis in a Patient with COVID-19. Am. J. Trop. Med. Hyg. 2020, 103, 1590–1592. [Google Scholar] [CrossRef]
- Incani, R.N.; Hernández, M.; González, M.E. Hyperinfection by Strongyloides stercoralis probably associated with Rituximab in a patient with mantle cell lymphoma and hyper eosinophilia. Rev. Inst. Med. Trop. 2010, 52, 221–224. [Google Scholar] [CrossRef]
- Stewart, D.M.; Ramanathan, R.; Mahanty, S.; Fedorko, D.P.; Janik, J.E.; Morris, J.C. Disseminated Strongyloides. stercoralis infection in HTLV-1-associated adult T-cell leukemia/lymphoma. Acta Haematol. 2011, 126, 63–67. [Google Scholar] [CrossRef]
- Gibson, M.; Lowe, P.M. Considerations in pre-treatment testing for Strongyloides stercoralis in an Australian cohort of 159 patients receiving biological therapies. Australas J. Dermatol. 2020, 61, 378–379. [Google Scholar] [CrossRef]
- González-Ramos, J.; Alonso-Pacheco, M.L.; Mora-Rillo, M.; Herranz-Pinto, P. Need to screen for Chagas disease and Strongyloides infestation in non-endemic countries prior to treatment with biologics. Actas Dermosifiliogr. 2017, 108, 373–375. [Google Scholar] [CrossRef] [PubMed]
- Muhi, S.; Ko, D.K.; McGuinness, S.L.; Biggs, B.A.; Mahanty, S.; Delany, C. Mixed-method analysis of screening for Strongyloides stercoralis prior to immunosuppression: A problem of limited bandwidth? Intern. Med. J. 2022, 52, 790–799. [Google Scholar] [CrossRef] [PubMed]
- Monge-Maillo, B.; Navarro, M.; Rodríguez, E.; Rincón, J.M.R.; Tojeiro, S.C.; Sanchez, S.J.; del Corral, M.J.C.; López-Vélez, R. Community screening campaign for Strongyloides stercoralis among Latin American immigrants in Spain. Clin. Microbiol. Infect. 2018, 24, 1220–1221. [Google Scholar] [PubMed]


{kind=link}
| Island | Women | Men | N (%) |
|---|---|---|---|
| Gran Canaria | 142 | 109 | 251 (39.1%) |
| Tenerife | 97 | 75 | 172 (26.8%) |
| La Palma | 37 | 44 | 81 (12.6%) |
| La Gomera | 22 | 22 | 44 (6.9%) |
| Lanzarote | 23 | 10 | 33 (5.1%) |
| Fuerteventura | 20 | 11 | 31 (4.8%) |
| El Hierro | 17 | 13 | 30 (4.7%) |
| Total | 358 | 284 | 642 |
| Baseline Pathology | N = 208 |
|---|---|
| Crohn’s disease | 57 (27.5%) |
| Psoriasis | 45 (21.6%) |
| Multiple sclerosis | 40 (19.2%) |
| Rheumatoid arthritis | 16 (7.7%) |
| Ulcerative colitis | 12 (5.8%) |
| Hidradenitis | 10 (4.8%) |
| Ankylosing spondylitis | 7 (3.4%) |
| Atopic dermatitis | 3 (1.5%) |
| Uveitis | 3 (1.5%) |
| Others | 15 (7.2%) |
| Immunosuppressive Treatment (204) N (%) | Kidney Transplant (48) N (%) | |
|---|---|---|
| Relative eosinophilia | ||
| <5% | 173/204 (85.0) | 35/48 (73.0) |
| >5% | 31/204 (15.0) | 13/48 (27.0) |
| Absolute Eosinophilia | ||
| <450 | 189/204 (92.6) | 42/48 (87,5) |
| >450 | 15/204 (7.4) | 6/48 (12.5) |
| Age | Sex | Country of Birth | Baseline Pathology | Eosinophilia (Absolute and Relative) | S. stercoralis IgG (DU) | Toxocara canis | Echinococcus granulosus | |
|---|---|---|---|---|---|---|---|---|
| Case 1 | 40 | Female | Spain | Crohn’s disease | No | 14 | Negative | Negative |
| Case 2 | 32 | Male | Spain | Multiple sclerosis | No | 23 | Negative | Negative |
| Case 3 | 70 | Male | Morocco | Lung cancer | No | 12 | Negative | Negative |
| Case 4 | 35 | Male | Spain | Crohn’s disease | No | 17 | Negative | Negative |
| Case 5 | 37 | Female | Equatorial Guinea | Kidney transplant | No | 21 | Negative | Negative |
| Case 6 | 31 | Female | Spain | Crohn’s disease | No | 15 | Negative | Negative |
| Case 7 | 40 | Male | Spain | Crohn’s disease | No | 117 | Negative | Negative |
| Case 8 | 37 | Male | Spain | Psoriasis | No | 12 | Negative | Negative |
| Case 9 | 37 | Female | Spain | Multiple sclerosis | No | 67 | Negative | Negative |
| Case 10 | 29 | Female | Spain | Crohn’s disease | No | 18 | Negative | Negative |
| Case 11 | 62 | Female | Spain | Hydradenitis | No | 55 | Negative | Negative |
| Case 12 | 74 | Female | Spain | Kidney transplant | No | 68 | Negative | Negative |
| Age | Sex | Country of Birth | Eosinophilia (Absolute and Relative) | S. stercoralis IgG (DU) | Toxocara canis | Echinococcus granulosus | |
|---|---|---|---|---|---|---|---|
| Case 1 | 13 | Female | Spain | No | 20 | Negative | Negative |
| Case 2 | 15 | Female | Spain | No | 18 | Negative | Negative |
| Case 3 | 17 | Male | Spain | No | 35 | Negative | Negative |
| Case 4 | 41 | Male | Spain | No | 22 | Negative | Negative |
| Case 5 | 43 | Female | Spain | No | 14 | Negative | Negative |
| Case 6 | 57 | Female | Spain | No | 45 | Negative | Negative |
| Case 7 | 62 | Female | Spain | No | 18 | Negative | Negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carranza-Rodríguez, C.; López-Delgado, L.; Granados-Magan, Á.; Pérez-Arellano, J.-L. Seroprevalence of Strongyloides stercoralis in Patients about to Receive Immunosuppressive Treatment in Gran Canaria (Spain). Trop. Med. Infect. Dis. 2023, 8, 181. https://doi.org/10.3390/tropicalmed8030181
Carranza-Rodríguez C, López-Delgado L, Granados-Magan Á, Pérez-Arellano J-L. Seroprevalence of Strongyloides stercoralis in Patients about to Receive Immunosuppressive Treatment in Gran Canaria (Spain). Tropical Medicine and Infectious Disease. 2023; 8(3):181. https://doi.org/10.3390/tropicalmed8030181
Chicago/Turabian StyleCarranza-Rodríguez, Cristina, Laura López-Delgado, Álvaro Granados-Magan, and José-Luis Pérez-Arellano. 2023. "Seroprevalence of Strongyloides stercoralis in Patients about to Receive Immunosuppressive Treatment in Gran Canaria (Spain)" Tropical Medicine and Infectious Disease 8, no. 3: 181. https://doi.org/10.3390/tropicalmed8030181
APA StyleCarranza-Rodríguez, C., López-Delgado, L., Granados-Magan, Á., & Pérez-Arellano, J.-L. (2023). Seroprevalence of Strongyloides stercoralis in Patients about to Receive Immunosuppressive Treatment in Gran Canaria (Spain). Tropical Medicine and Infectious Disease, 8(3), 181. https://doi.org/10.3390/tropicalmed8030181