

Towards Inclusive Diagnostics for Neglected Tropical Diseases: User Experience of a New Digital Diagnostic Device in Low-Income Settings

 , ,
, ,
Abstract
1. Introduction
1.1. Designing for Neglected Tropical Diseases
1.2. Problem Statement
1.3. Aim and Objectives of the Study
2. Materials and Methods
2.1. Study Design
2.2. Tools
2.3. Study Participants and Ethics
2.4. Procedure
2.5. Data Analysis
3. Results
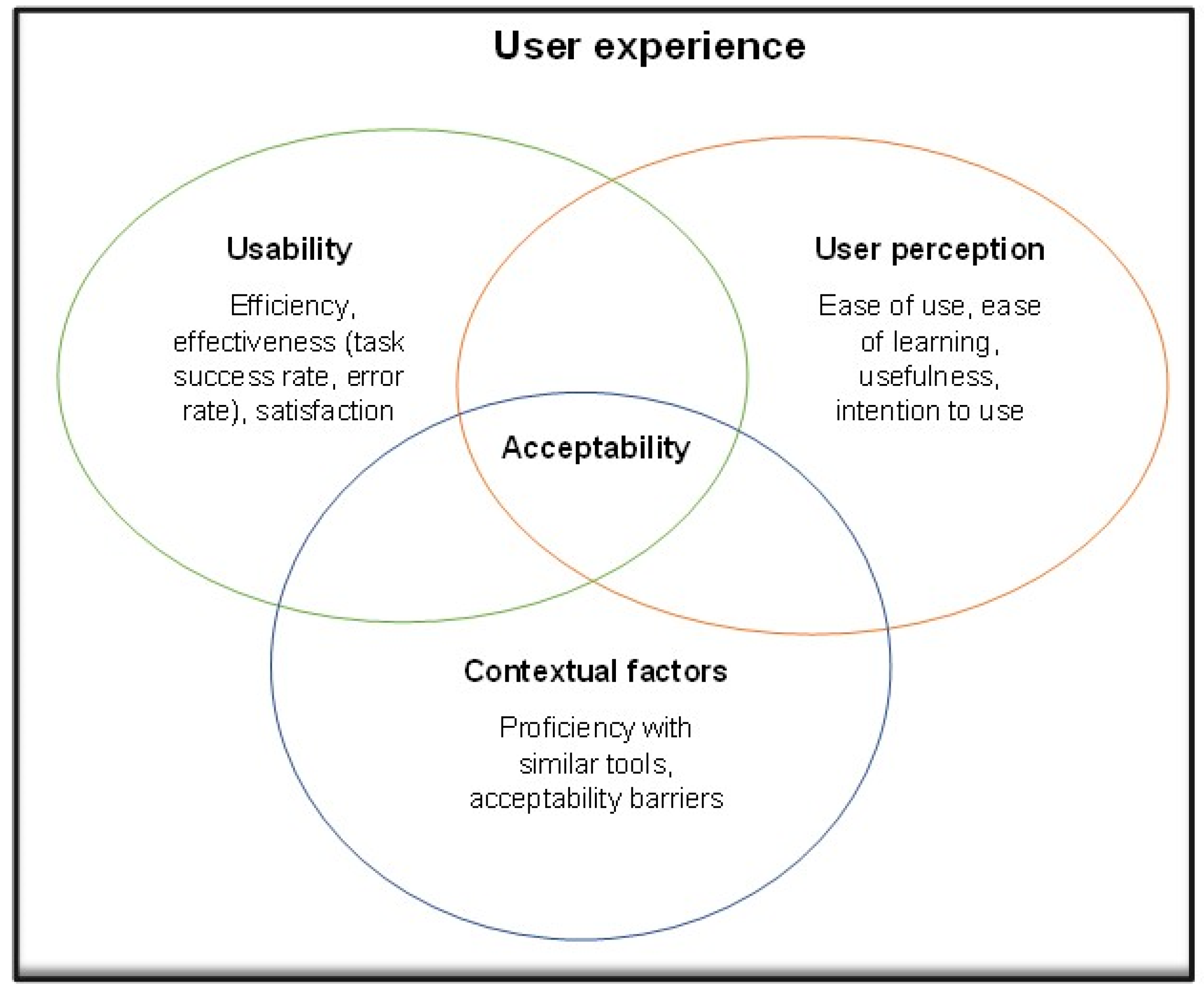
3.1. Usability Results
3.1.1. Efficiency
3.1.2. Effectiveness (Task Success Rate and Error Rate)
3.1.3. Satisfaction
3.2. Contextual Factors
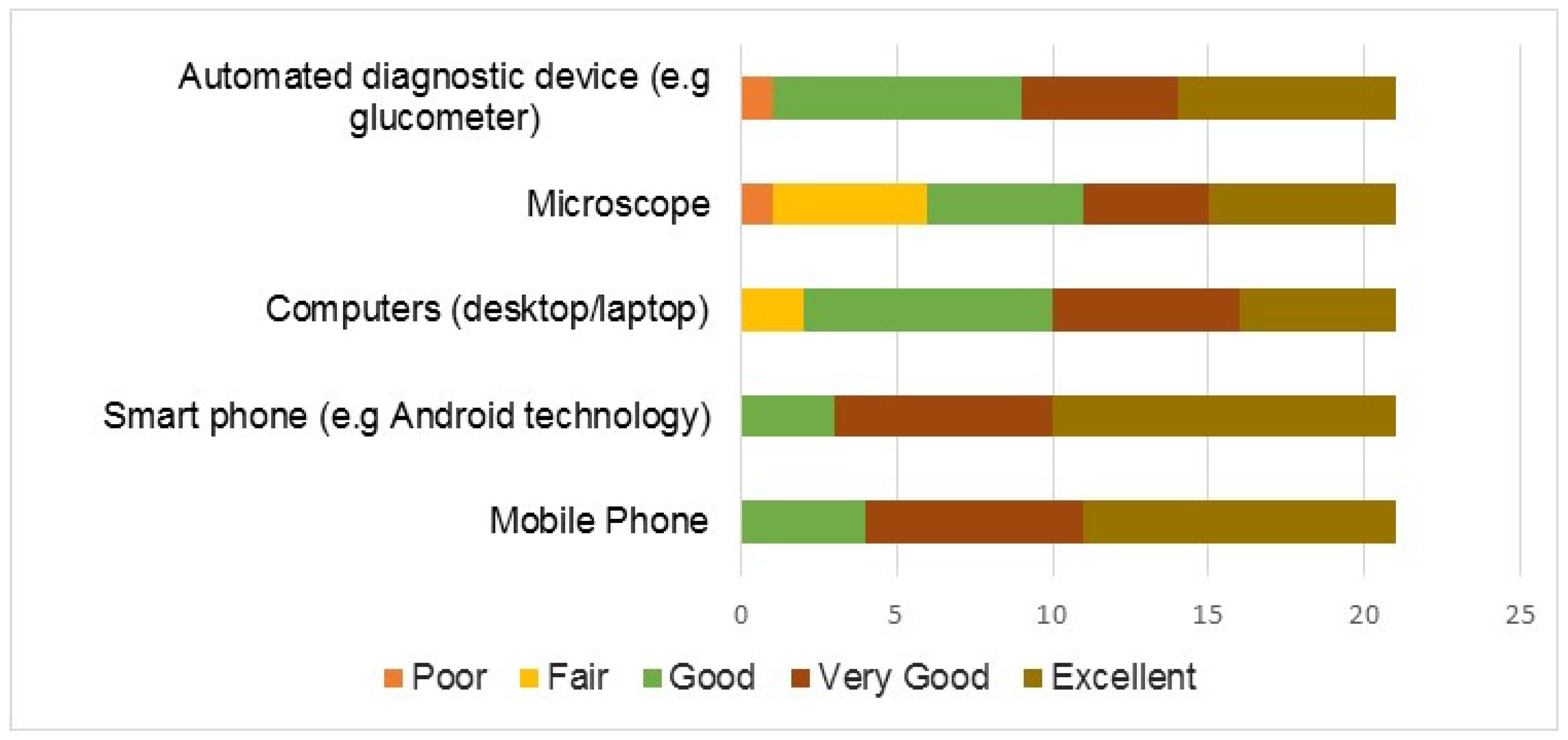
3.2.1. Proficiency with Similar Digital and Optical Devices
3.2.2. Acceptability Barriers
3.3. User Perception
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ending the Neglect to Attain the Sustainable Development Goals—A Road Map for Neglected Tropical Diseases 2021–2030. World Health Organization. 2020. Available online: https://www.who.int/publications/i/item/9789240010352 (accessed on 26 June 2022).
- World Health Organization. Schistosomiasis Fact Sheet. In: World Health Organization [Internet]. 10 May 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/schistosomiasis (accessed on 5 October 2020).
- Adekeye, O.; Dean, L.; Dixon, R. Community Engagement in Neglected Tropical Disease Treatment in Nigeria: Rethinking the Needs of Varying Contexts. 2017. Available online: https://countdown.lstmed.ac.uk/sites/default/files/content/centre_page/attachments/Community Engagement_final.pdf (accessed on 22 June 2022).
- Egan, K.; Devlin, K.; Pandit-Rajani, T. Community Health Systems Catalog Country Profile: Nigeria. Arlington, VA: Advancing Partners & Communities. 2017. Available online: https://www.advancingpartners.org/sites/default/files/catalog/profiles/full_tagged_apc_nigeria_profile.pdf (accessed on 1 June 2022).
- Van, G.-Y.; Onasanya, A.; Van Engelen, J.; Oladepo, O.; Diehl, J.C. Improving Access to Diagnostics for Schistosomiasis Case Management in Oyo State, Nigeria: Barriers and Opportunities. Diagnostics 2020, 10, 328. [Google Scholar] [CrossRef] [PubMed]
- George, E. Occupational Hazard for Pathologists. Am. J. Clin. Pathol. 2010, 133, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Agbana, T.; Onasanya, A. Performance Evaluation of AiDx Assist in the Diagnosis of Lymphatic Filariasis (LF) in Field Settings: A Field Study Conducted by the INSPiRED NWO Project—Dec 2021. 2021. Available online: http://resolver.tudelft.nl/uuid:38561f8e-3b22-413b-87a0-89d26a9466d3 (accessed on 5 November 2022).
- Brown, T. Design Thinking. Harvard Business Review. 1 June 2008. Available online: https://hbr.org/2008/06/design-thinking (accessed on 8 June 2022).
- Privitera, M.B.; Evans, M.; Southee, D. Human factors in the design of medical devices—Approaches to meeting international standards in the European Union and USA. Appl. Ergon. 2017, 59, 251–263. [Google Scholar] [CrossRef] [PubMed]
- Schulze, K.; Krömker, H. A framework to measure user experience of interactive online products. In Proceedings of the 7th International Conference on Methods and Techniques in Behavioral Research, Eindhoven, The Netherlands, 24–27 August 2010. [Google Scholar] [CrossRef]
- ISO 9241-210:2010; Ergonomics of Human-System Interaction—Part 210: Human-Centred Design for Interactive Systems. International Organization for Standardization: Geneva, Switzerland, 2019. Available online: https://www.iso.org/cms/render/live/en/sites/isoorg/contents/data/standard/05/20/52075.html (accessed on 4 May 2022).
- Chamorro-Koc, M.; Popovic, V.; Emmison, M. Context of Use and User’s Experience: An Exploratory Study in the Product Design Domain. In Futureground International Conference; Monash University: Melbourne, Australia, 2004. [Google Scholar]
- Zarour, M.; Alharbi, M. User experience framework that combines aspects, dimensions, and measurement methods. Cogent Eng. 2017, 4, 1421006. [Google Scholar] [CrossRef]
- Parreira, P.; Sousa, L.B.; Marques, I.A.; Santos-Costa, P.; Cortez, S.; Carneiro, F.; Cruz, A.; Salgueiro-Oliveira, A. Usability Assessment of an Innovative Device in Infusion Therapy: A Mix-Method Approach Study. Int. J. Environ. Res. Public Health 2020, 17, 8335. [Google Scholar] [CrossRef]
- Department of Health and Human Services. System Usability Scale (SUS). Department of Health and Human Services. 2013. Available online: https://www.usability.gov/how-to-and-tools/methods/system-usability-scale.html (accessed on 2 February 2022).
- Bailey, R.W.; Wolfson, C.A.; Nall, J.; Koyani, S. Performance-Based Usability Testing: Metrics That Have the Greatest Impact for Improving a System’s Usability. In Human Centered Design; Springer: Berlin/Heidelberg, Germany, 2009; pp. 3–12. [Google Scholar] [CrossRef]
- Center for Devices and Radiological Health. Applying Human Factors and Usability Engineering to Medical Devices: Guidance for Industry and Food and Drug Administration Staff. 2016. Available online: https://www.fda.gov/media/80481/download (accessed on 2 February 2022).
- IEC/TR 62366-2:2016; Medical Devices—Part 2: Guidance on the Application of Usability Engineering to Medical Devices. International Organization for Standardization: Geneva, Switzerland, 2016. Available online: https://www.iso.org/cms/render/live/en/sites/isoorg/contents/data/standard/06/91/69126.html (accessed on 4 May 2022).
- Radomski, A.D.; Bagnell, A.; Curtis, S.; Hartling, L.; Newton, A.S. Examining the Usage, User Experience, and Perceived Impact of an Internet-Based Cognitive Behavioral Therapy Program for Adolescents With Anxiety: Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e15795. [Google Scholar] [CrossRef] [PubMed]
- Kalayou, M.H.; Endehabtu, B.F.; Tilahun, B. The Applicability of the Modified Technology Acceptance Model (TAM) on the Sustainable Adoption of eHealth Systems in Resource-Limited Settings. J. Multidiscip. Health 2020, 13, 1827–1837. [Google Scholar] [CrossRef]
- Marangunić, N.; Granić, A. Technology acceptance model: A literature review from 1986 to 2013. Univ. Access Inf. Soc. 2015, 14, 81–95. [Google Scholar] [CrossRef]
- Melas, C.D.; Zampetakis, L.A.; Dimopoulou, A.; Moustakis, V. Modeling the acceptance of clinical information systems among hospital medical staff: An extended TAM model. J. Biomed. Informatics 2011, 44, 553–564. [Google Scholar] [CrossRef]
- Nguyen, M.; Fujioka, J.; Wentlandt, K.; Onabajo, N.; Wong, I.; Bhatia, R.S.; Bhattacharyya, O.; Stamenova, V. Using the technology acceptance model to explore health provider and administrator perceptions of the usefulness and ease of using technology in palliative care. BMC Palliat. Care 2020, 19, 1–9. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef] [PubMed]
- Spagnolli, A.; Guardigli, E.; Orso, V.; Varotto, A.; Gamberini, L. Measuring User Acceptance of Wearable Symbiotic Devices: Validation Study Across Application Scenarios. In International Workshop on Symbiotic Interaction, Proceedings of the Symbiotic 2015: Symbiotic Interaction, Helsinki, Finland, 30–31 October 2014; Springer: Cham, Switzerland, 2015; pp. 87–98. [Google Scholar]
- Saidi, T.; Douglas, T.S. Critical elements in the design, development and use of medical devices. A systemic perspective of orthopedic devices landscape in low- and middle-income countries. Health Policy Technol. 2021, 11, 100593. [Google Scholar] [CrossRef]
- WHO. Towards Improving Access to Medical Devices through Local Production. 2016. Available online: https://www.who.int/publications-detail-redirect/9789241510141 (accessed on 12 April 2022).
- Ezeh, C.O.; Onyekwelu, K.C.; Akinwale, O.P.; Shan, L.; Wei, H. Urinary schistosomiasis in Nigeria: A 50 year review of prevalence, distribution and disease burden. Parasite 2019, 26, 19. [Google Scholar] [CrossRef]
- Onasanya, A.; Keshinro, M.; Oladepo, O.; Van Engelen, J.; Diehl, J.C. A Stakeholder Analysis of Schistosomiasis Diagnostic Landscape in South-West Nigeria: Insights for Diagnostics Co-creation. Front. Public Health 2020, 8, 564381. [Google Scholar] [CrossRef] [PubMed]
- Sluiter, M.; Onasanya, A.; Oladepo, O.; van Engelen, J.; Keshinro, M.; Agbana, T.; Van, G.-Y.; Diehl, J.C. Target product profiles for devices to diagnose urinary schistosomiasis in Nigeria. In Proceedings of the 2020 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 29 October–1 November 2020; pp. 1–8. [Google Scholar] [CrossRef]
- Samenjo, K.T.; Bengtson, M.; Onasanya, A.; Zambrano, J.C.I.; Oladunni, O.; Oladepo, O.; van Engelen, J.; Diehl, J.-C. Stakeholders’ Perspectives on the Application of New Diagnostic Devices for Urinary Schistosomiasis in Oyo State, Nigeria: A Q-Methodology Approach. Glob. Health Sci. Pract. 2022, 10, e2100780. [Google Scholar] [CrossRef] [PubMed]
- Ward, P.; Dahlberg, P.; Lagatie, O.; Larsson, J.; Tynong, A.; Vlaminck, J.; Zumpe, M.; Ame, S.; Ayana, M.; Khieu, V.; et al. Affordable artificial intelligence-based digital pathology for neglected tropical diseases: A proof-of-concept for the detection of soil-transmitted helminths and Schistosoma mansoni eggs in Kato-Katz stool thick smears. PLoS Neglected Trop. Dis. 2022, 16, e0010500. [Google Scholar] [CrossRef]
- Cunningham, F.C.; Ranmuthugala, G.; Plumb, J.; Georgiou, A.; Westbrook, J.I.; Braithwaite, J. Health professional networks as a vector for improving healthcare quality and safety: A systematic review. BMJ Qual. Saf. 2012, 21, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Tilahun, B.; Gashu, K.D.; Mekonnen, Z.A.; Endehabtu, B.F.; Angaw, D.A. Mapping the role of digital health technologies in the case detection, management, and treatment outcomes of neglected tropical diseases: A scoping review. Trop. Med. Health 2021, 49, 17. [Google Scholar] [CrossRef]
- Frej, A.; Cano, M.; A Ruiz-Postigo, J.; Macharia, P.; Phillips, R.O.; Amoako, Y.A.; Carrion, C. Assessing the Quality of the World Health Organization’s Skin NTDs App as a Training Tool in Ghana and Kenya: Protocol for a Cross-sectional Study. JMIR Res. Protoc. 2022, 11, e39393. [Google Scholar] [CrossRef]
- Davies, J.; Abimiku, A.; Alobo, M.; Mullan, Z.; Nugent, R.; Schneidman, M.; Sikhondze, W.; Onyebujoh, P. Sustainable clinical laboratory capacity for health in Africa. Lancet Glob. Health 2017, 5, e248–e249. [Google Scholar] [CrossRef]
- Petti, C.A.; Polage, C.R.; Quinn, T.C.; Ronald, A.R.; Sande, M.A. Laboratory Medicine in Africa: A Barrier to Effective Health Care. Clin. Infect. Dis. 2006, 42, 377–382. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sex | Count |
| Female | 13 |
| Male | 8 |
| Education | |
| Postgraduate | 5 |
| University Graduate (B.Sc.) | 3 |
| Diploma (OND/HND) | 1 |
| Health Technology School | 12 |
| Years of Experience | |
| 0–4 | 11 |
| 5–9 | 2 |
| 10–14 | 3 |
| 15–19 | 2 |
| 20–24 | 2 |
| ≥25 | 1 |
| Level of Training | |
| Community Health Extension Worker (CHEW) in-training | 11 |
| Laboratory Technologist/Technician | 3 |
| Laboratory Scientist | 7 |
| Category | Turning on the Device (s) | Starting the Application (s) | Putting in a Slide (s) | Reading Result Output (s) | Average Time (s) | Average Error Rate (%) |
|---|---|---|---|---|---|---|
| CHEW in training | 2.5 ± 0.7 | 3.8 ± 1.4 | 2.5 ± 1.0 | 6.5 ± 4.9 | 3.3 ± 2.0 | 2.3% |
| Laboratory Technician | 2.0 ± 0.0 | 4.5 ± 0.7 | 4.0 ± 0.0 | 8.5 ± 2.1 | 7.7 ± 0.7 | 87.5% |
| Laboratory Scientist | 2.5 ± 1.0 | 4.8 ± 3.2 | 2.8 ± 1.4 | 8.0 ± 3.9 | 4.5 ± 4.6 | 9.3% |
| All participants | 2.4 ± 0.8 | 2.8 ± 1.2 | 4.3 ± 2.2 | 7.2 ± 4.3 | 4.2 ± 2.1 | 33% |
| Proficiency in Digital/ Optical Tools | Gender | Level of Education | Level of Training | Years of Experience |
|---|---|---|---|---|
| Mobile phone | 0.83 | 0.69 | 0.07 | 0.58 |
| Smartphone (Android technology) | 0.95 | 0.64 | 0.01 | 0.52 |
| Computer (desktop/laptop) | 0.27 | 0.14 | 0.51 | 0.60 |
| Optical devices (microscope) | 0.11 | 0.14 | 0.00 | 0.01 |
| Automated diagnostic device (e.g., glucometer) | 0.52 | 0.08 | 0.01 | 0.22 |
| Perception Domain | Mean ± S.D | Median | Mode | Cronbach’s Alpha (All Items) |
|---|---|---|---|---|
| Ease of learning | 4.1 ± 1.2 | 5.0 | 5 | 0.9248 |
| Ease of use | 4.3 ± 0.8 | 4.0 | 5 | |
| Usefulness | 4.6 ± 0.5 | 5.0 | 5 | |
| Intention to use | 4.6 ± 0.5 | 5.0 | 5 |
| Variables/Domains | Ease of Learning | EASE OF USE | Usefulness | Intention to Use |
|---|---|---|---|---|
| Gender | W = 54.5, p = 0.85 | W = 50.5, p = 0.90 | W = 63.0, p = 0.34 | W = 47.0, p = 0.66 |
| Highest level of education | W = 32.5, p = 0.10 | W = 39.0, p = 0.23 | W = 49.5, p = 0.70 | W = 63.0, p = 0.44 |
| Level of training | W = 48.5, p = 0.67 | W = 43.5, p = 0.41 | W = 74.0, p = 0.085 | W = 74.0, p = 0.08 |
| Years of Experience | W = 40.0, p = 0.35 | W = 53.5, p = 0.93 | W = 51.5, p = 0.97 | W = 46.0, p = 0.60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onasanya, A.; Bengtson, M.; Agbana, T.; Oladunni, O.; van Engelen, J.; Oladepo, O.; Diehl, J.C. Towards Inclusive Diagnostics for Neglected Tropical Diseases: User Experience of a New Digital Diagnostic Device in Low-Income Settings. Trop. Med. Infect. Dis. 2023, 8, 176. https://doi.org/10.3390/tropicalmed8030176
Onasanya A, Bengtson M, Agbana T, Oladunni O, van Engelen J, Oladepo O, Diehl JC. Towards Inclusive Diagnostics for Neglected Tropical Diseases: User Experience of a New Digital Diagnostic Device in Low-Income Settings. Tropical Medicine and Infectious Disease. 2023; 8(3):176. https://doi.org/10.3390/tropicalmed8030176
Chicago/Turabian StyleOnasanya, Adeola, Michel Bengtson, Temitope Agbana, Opeyemi Oladunni, Jo van Engelen, Oladimeji Oladepo, and Jan Carel Diehl. 2023. "Towards Inclusive Diagnostics for Neglected Tropical Diseases: User Experience of a New Digital Diagnostic Device in Low-Income Settings" Tropical Medicine and Infectious Disease 8, no. 3: 176. https://doi.org/10.3390/tropicalmed8030176
APA StyleOnasanya, A., Bengtson, M., Agbana, T., Oladunni, O., van Engelen, J., Oladepo, O., & Diehl, J. C. (2023). Towards Inclusive Diagnostics for Neglected Tropical Diseases: User Experience of a New Digital Diagnostic Device in Low-Income Settings. Tropical Medicine and Infectious Disease, 8(3), 176. https://doi.org/10.3390/tropicalmed8030176