
The Impact of COVID-19 on Tuberculosis Program Performance in the Kingdom of Lesotho

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Population
2.3. Data Collection
2.4. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Tuberculosis Report 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Ortblad, K.F.; Salomon, J.A.; Barnighausen, T.; Atun, R. Stopping tuberculosis: A biosocial model for sustainable development. Lancet 2015, 386, 2354–2362. [Google Scholar] [CrossRef] [PubMed]
- Sumner, A.; Hoy, C.; Ortiz-Juarez, E. Estimates of the Impact of COVID-19 on Global Poverty. WIDER Working Paper 2020/43; UNU-WIDER: Helsinki, Finland, 2020. [Google Scholar] [CrossRef]
- Saunders, M.J.; Evans, C.A. COVID-19, tuberculosis and poverty: Preventing a perfect storm. Eur. Respir. J. 2020, 56, 2001348. [Google Scholar] [CrossRef] [PubMed]
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Hamlet, A.; Smith, J.; Winskill, P.; Verity, R.; et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef] [PubMed]
- Sands, P. HIV, tuberculosis, and malaria: How can the impact of COVID-19 be minimised? Lancet Glob. Health 2020, 8, e1102–e1103. [Google Scholar] [CrossRef]
- WHO. Impact of the COVID-19 Pandemic on TB Detection and Mortality in 2020; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Glaziou, P. Predicted impact of the COVID-19 pandemic on global tuberculosis deaths in 2020. medRixv 2020. [Google Scholar] [CrossRef]
- We Did a Rapid Assessment: The TB Response Is Heavily Impacted by the COVID-19 Pandemic; Stop TB Partnership: Geneva, Switzerland, 2020.
- Alimuddin, Z.; Marais, B.J.; McHugh, T.D. COVID-19 and tuberculosis—Threats and opportunities. Int. J. Tuberc. Lung Dis. 2020, 24, 757–760. [Google Scholar] [CrossRef]
- Reid, M.J.A.; Arinaminpathy, N.; Bloom, A.; Bloom, B.R.; Boehme, C.; Chaisson, R.; Chin, D.P.; Churchyard, G.; Cox, H.; Ditiu, L.; et al. Building a tuberculosis-free world: The Lancet Commission on tuberculosis. Lancet 2019, 393, 1331–1384. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Tuberculosis Report 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- The Impact of COVID-19 on the TB Epidemic: A Community Perspective; Stop TB Partnership, Civil Society-Led TB/COVID-19 Working Group: Geneva, Switzerland, 2020.
- Togun, T.; Kampmann, B.; Stoker, N.G.; Lipman, M. Anticipating the impact of the COVID-19 pandemic on TB patients and TB control programmes. Ann. Clin. Microbiol. Antimicrob. 2020, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Columbia University. Lesotho Population Based HIV Impact Assessment; Columbia University: New York, NY, USA, 2020. [Google Scholar]
- United Nations Statistics Division. Demographic Year Book. 2012. Available online: https://unstats.un.org/unsd/demographic/products/dyb/dyb2012 (accessed on 15 December 2022).
- Lesotho Ministry of Health and Social Welfare Services. National Health Strategic Plan 2017–2022 (Final Draft). 2016; pp. 1–78. Available online: http://www.nationalplanningcycles.org/sites/default/files/planning_cycle_repository/lesotho/lesotho_revised_nhsp_2017-22_final_draft1.pdf (accessed on 16 February 2023).
- WHO. Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Oluoch-Aridi, J.; Chelagat, T.; Nyikuri, M.M.; Onyango, J.; Guzman, D.; Makanga, C.; Miller-Graff, L.; Dowd, R. COVID-19 Effect on Access to Maternal Health Services in Kenya. Front. Glob. Womens Health 2020, 1, 599267. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Xia, Y.; Chen, H.; Wang, N.; Du, X.; Chen, W.; Li, T.; Huan, S.; Sun, M.; Chen, M.; et al. The impact of the COVID-19 epidemic on tuberculosis control in China. Lancet Reg. Health West Pac. 2020, 3, 100032. [Google Scholar] [CrossRef]
- Odume, B.; Falokun, V.; Chukwuogo, O.; Ogbudebe, C.; Useni, S.; Nwokoye, N.; Aniwada, E.; Olusola Faleye, B.; Okekearu, I.; Nongo, D.; et al. Impact of COVID-19 on TB active case finding in Nigeria. Public Health Action 2020, 10, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Thekkur, P.; Tweya, H.; Phiri, S.; Mpunga, J.; Kalua, T.; Kumar, A.M.V.; Satyanarayana, S.; Shewade, H.D.; Khogali, M.; Zachariah, R.; et al. Assessing the Impact of COVID-19 on TB and HIV Programme Services in Selected Health Facilities in Lilongwe, Malawi: Operational Research in Real Time. Trop. Med. Infect. Dis. 2021, 6, 81. [Google Scholar] [CrossRef] [PubMed]
- Mbithi, I.; Thekkur, P.; Chakaya, J.M.; Onyango, E.; Owiti, P.; Njeri, N.C.; Kumar, A.M.V.; Satyanarayana, S.; Shewade, H.D.; Khogali, M.; et al. Assessing the Real-Time Impact of COVID-19 on TB and HIV Services: The Experience and Response from Selected Health Facilities in Nairobi, Kenya. Trop. Med. Infect. Dis. 2021, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Lakoh, S.; Jiba, D.F.; Baldeh, M.; Adekanmbi, O.; Barrie, U.; Seisay, A.L.; Deen, G.F.; Salata, R.A.; Yendewa, G.A. Impact of COVID-19 on Tuberculosis Case Detection and Treatment Outcomes in Sierra Leone. Trop. Med. Infect. Dis. 2021, 6, 154. [Google Scholar] [CrossRef] [PubMed]
- Thekkur, P.; Takarinda, K.C.; Timire, C.; Sandy, C.; Apollo, T.; Kumar, A.M.V.; Satyanarayana, S.; Shewade, H.D.; Khogali, M.; Zachariah, R.; et al. Operational Research to Assess the Real-Time Impact of COVID-19 on TB and HIV Services: The Experience and Response from Health Facilities in Harare, Zimbabwe. Trop. Med. Infect. Dis. 2021, 6, 94. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.S.; Rego, S.; Rajal, J.B.; Bond, V.; Fatima, R.K.; Isani, A.K.; Sutherland, J.; Kranzer, K. Mitigating the impact of COVID-19 on tuberculosis and HIV services: A cross-sectional survey of 669 health professionals in 64 low and middle-income countries. PLoS ONE 2021, 16, e0244936. [Google Scholar] [CrossRef]
- WHO. Programmatic Innovations to Address Challenges in Tuberculosis Prevention and Care during the COVID-19 Pandemic; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]


{kind=link}
| Indicators | Definitions |
|---|---|
| Outpatient department (OPD) visits | Visits consulted at the outpatient department in facilities excludes patients for antenatal care visit, deliveries, postnatal care visit, tuberculosis, anteretroviral therapy, pediatrics (under 5), HIV testing, and other clients not seen for acute or chronic illness. |
| Presumed TB cases | A patient who presents with symptoms or signs suggestive of TB. |
| Diagnosed TB cases | Any bacteriologically confirmed or clinically diagnosed case of TB. |
| Cases of TB/HIV co-infection | Any person with a bacteriologically confirmed or clinically diagnosed case of TB who has a positive result from HIV testing conducted at the time of TB diagnosis or other documented evidence of enrolment in HIV care. |
| Percentage of patients with successful TB treatment outcomes | The number of TB patients who successfully completed TB treatment or were cured of TB disease out of the number of TB patients who started treatment. |
| Percentage of TB patients who died during treatment | The number of TB patients who died for any reason during the course of TB treatment out of these patients who started treatment. |
| Percentage of TB patients with unknown treatment outcomes | The number of TB patients for whom no treatment outcome was assigned out of the patients who started TB treatment. This includes cases transferred out to another treatment unit as well as cases for whom the treatment outcome is unknown to the reporting unit. |
| Indicator | Monthly Value During Baseline, Median (IQR) | Cumulative Predicated Value during Pandemic, Median (IQR) | Cumulative Observed Value during Pandemic | Cumulative Deviation from Expected, 95% PI | Cumulative Proportion Deviation from Expected, 95% PI |
|---|---|---|---|---|---|
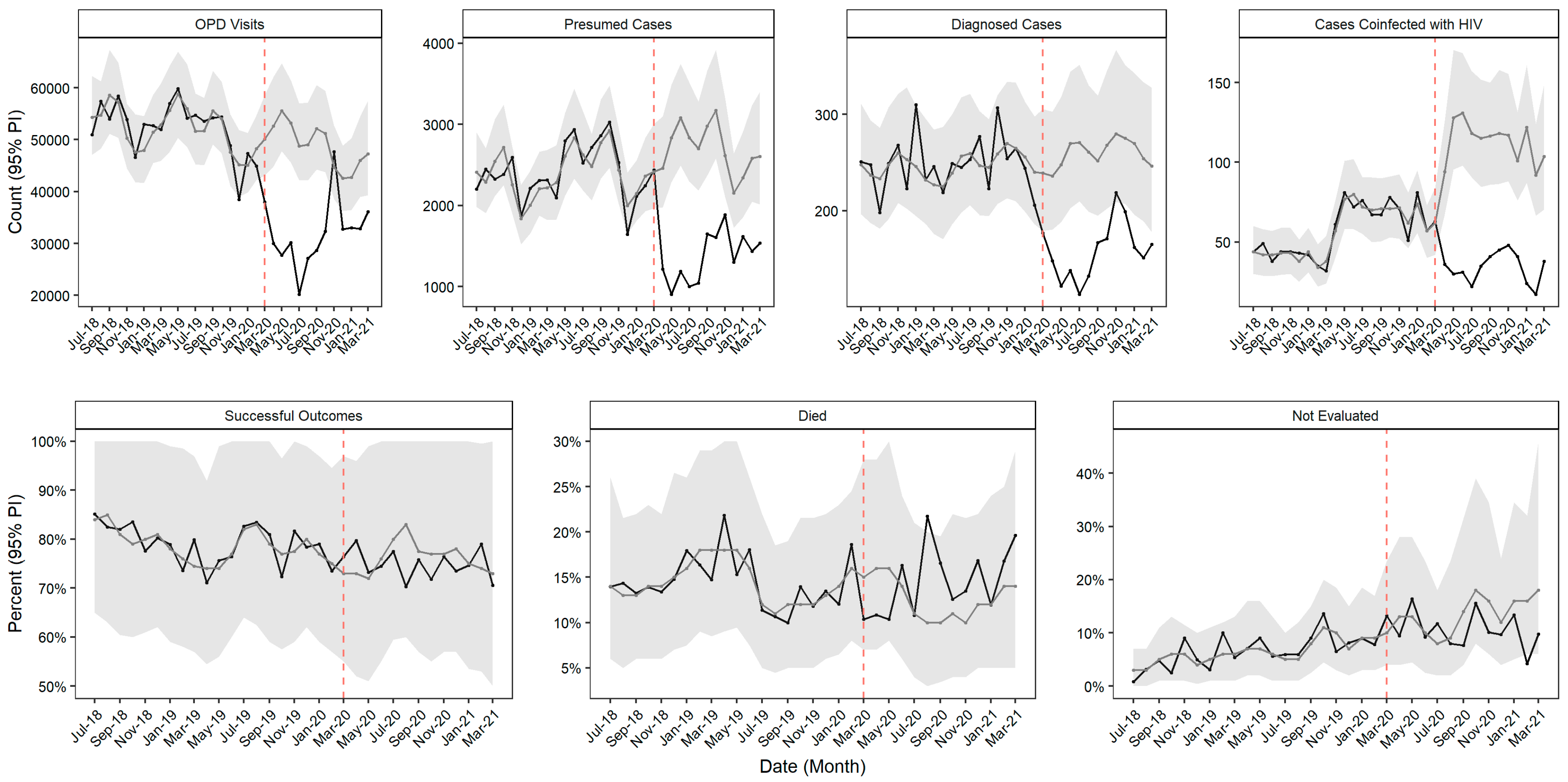
| Outpatient department visits | 53,748 (50,455, 54,482) | 638,178 (584,386, 695,632) | 416,445 | −221,733.0 (−279,186.7, −167,940.9) | −34.7% (−40.1%, −28.7%) |
| Presumed TB cases | 2357 (2209, 2626) | 34,947 (30,892, 39,422) | 18,837 | −16,109.5 (−20,585.4, −12,054.5) | −46.1% (−52.2%, −39.0%) |
| Diagnosed TB cases | 249 (230, 257) | 3367 (2881, 3909) | 2064 | −1303.0 (−1844.8, −817.3) | −38.7% (−47.2%, −28.4%) |
| Cases of TB/HIV co-infection | 54 (44, 71) | 1427 (1177, 1721) | 471 | −955.5 (−1250.2, −705.5) | −67.0% (−72.6%, −60.0%) |
| Percentage of patients with successful treatment outcomes | 80 (76, 82) | 995 (841, 1174) | 974 | −21.0 (−200.0, 132.5) | −2.1% (−17.0%, 15.8%) |
| Percentage of TB patients who died during treatment | 14 (13, 16) | 170 (112, 245) | 188 | 18.2 (−56.8, 76.7) | 10.7% (−23.2%, 68.8%) |
| Percentage of TB patients with unknown treatment outcomes | 6 (5, 9) | 177 (101, 310) | 138 | −38.7 (−171.7, 37.3) | −21.9% (−55.4%, 36.9%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andom, A.T.; Fejfar, D.; Yuen, C.M.; Ndayizigiye, M.; Mugunga, J.C.; Mukherjee, J.S. The Impact of COVID-19 on Tuberculosis Program Performance in the Kingdom of Lesotho. Trop. Med. Infect. Dis. 2023, 8, 165. https://doi.org/10.3390/tropicalmed8030165
Andom AT, Fejfar D, Yuen CM, Ndayizigiye M, Mugunga JC, Mukherjee JS. The Impact of COVID-19 on Tuberculosis Program Performance in the Kingdom of Lesotho. Tropical Medicine and Infectious Disease. 2023; 8(3):165. https://doi.org/10.3390/tropicalmed8030165
Chicago/Turabian StyleAndom, Afom T., Donald Fejfar, Courtney M. Yuen, Melino Ndayizigiye, Jean Claude Mugunga, and Joia S. Mukherjee. 2023. "The Impact of COVID-19 on Tuberculosis Program Performance in the Kingdom of Lesotho" Tropical Medicine and Infectious Disease 8, no. 3: 165. https://doi.org/10.3390/tropicalmed8030165
APA StyleAndom, A. T., Fejfar, D., Yuen, C. M., Ndayizigiye, M., Mugunga, J. C., & Mukherjee, J. S. (2023). The Impact of COVID-19 on Tuberculosis Program Performance in the Kingdom of Lesotho. Tropical Medicine and Infectious Disease, 8(3), 165. https://doi.org/10.3390/tropicalmed8030165