
Efficacy Assessment of Autodissemination Using Pyriproxyfen-Treated Ovitraps in the Reduction of Dengue Incidence in Parañaque City, Philippines: A Spatial Analysis

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Sites, and Population
2.1.1. Participant Inclusion Criteria
2.1.2. Participant Exclusion Criteria
2.2. Data Collection
2.2.1. Control and Intervention Ovitrap Set-Up
2.2.2. Outcome Measurements
2.2.3. Sample Size Calculations
2.3. Data Analysis
2.3.1. Spatial Statistics
2.3.2. Analyzing Patterns
2.3.3. Mapping Clusters
3. Results
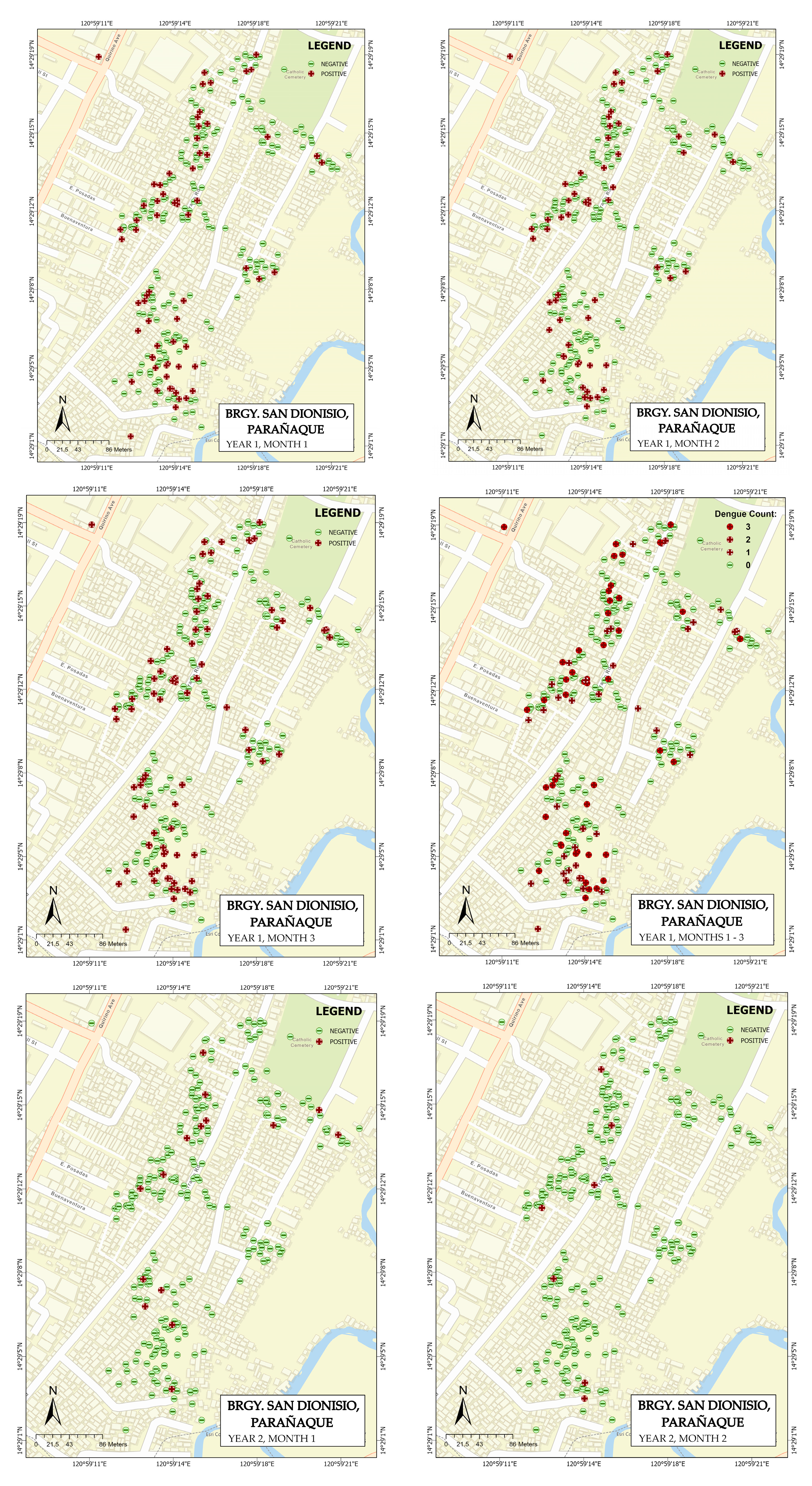
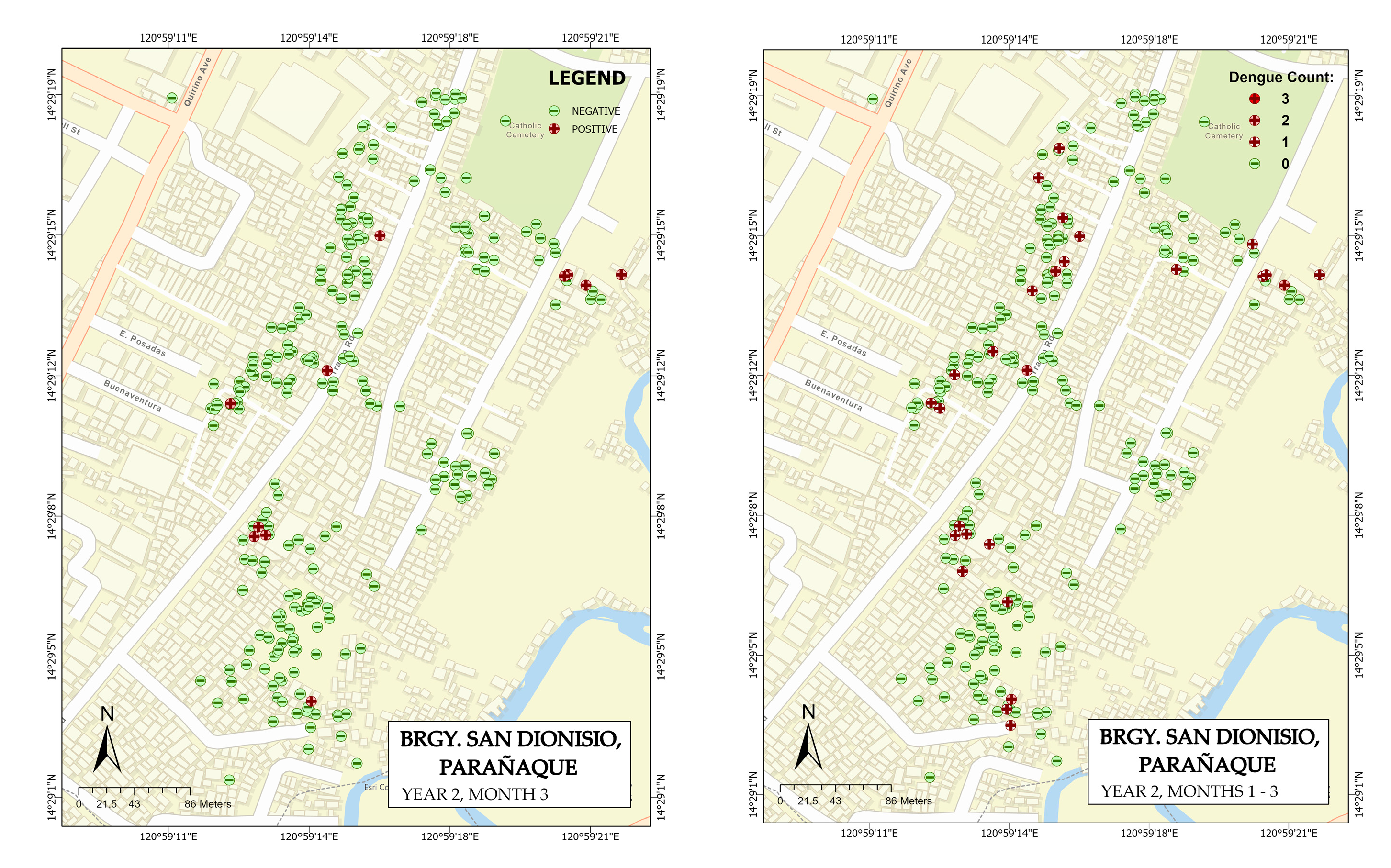
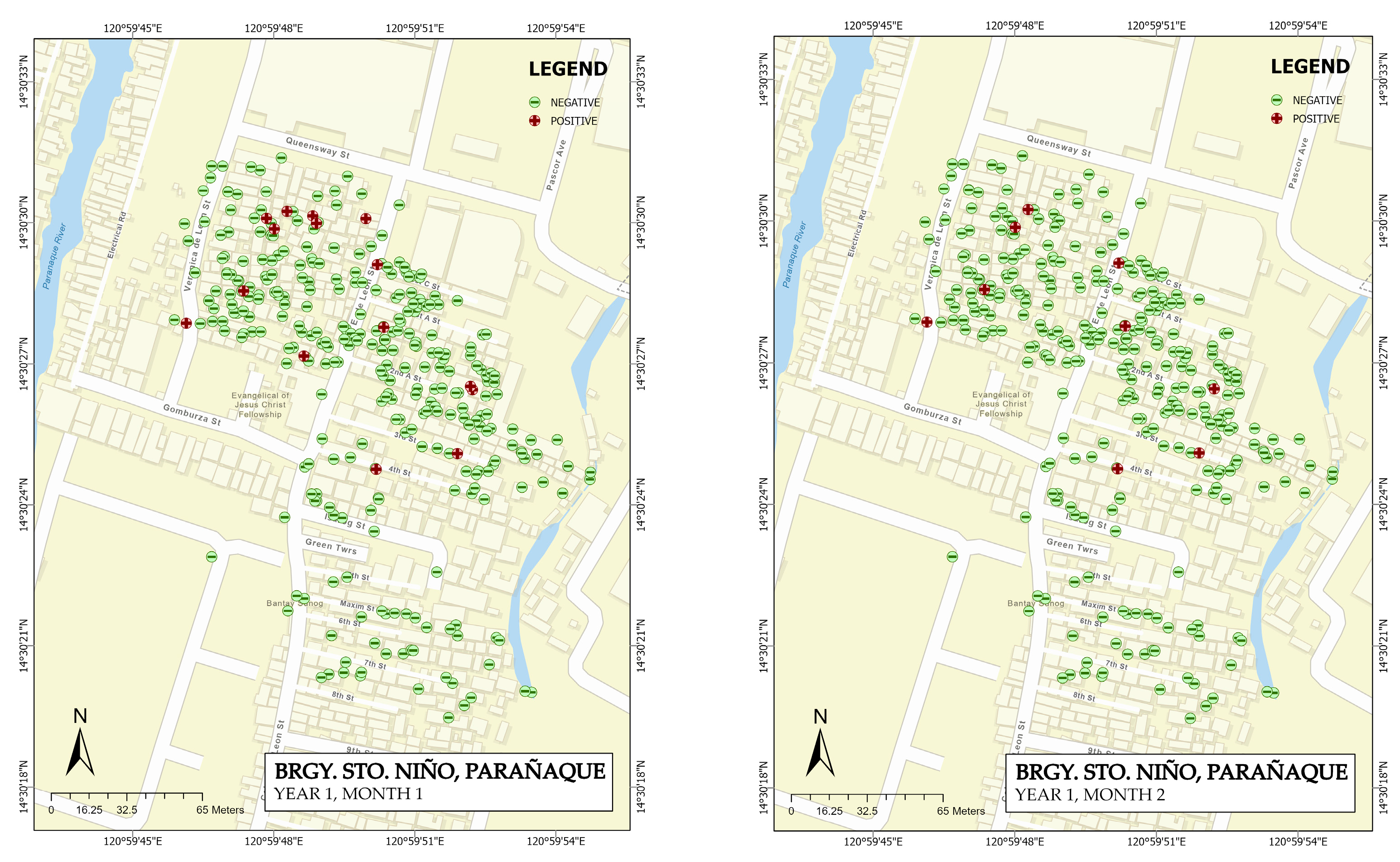
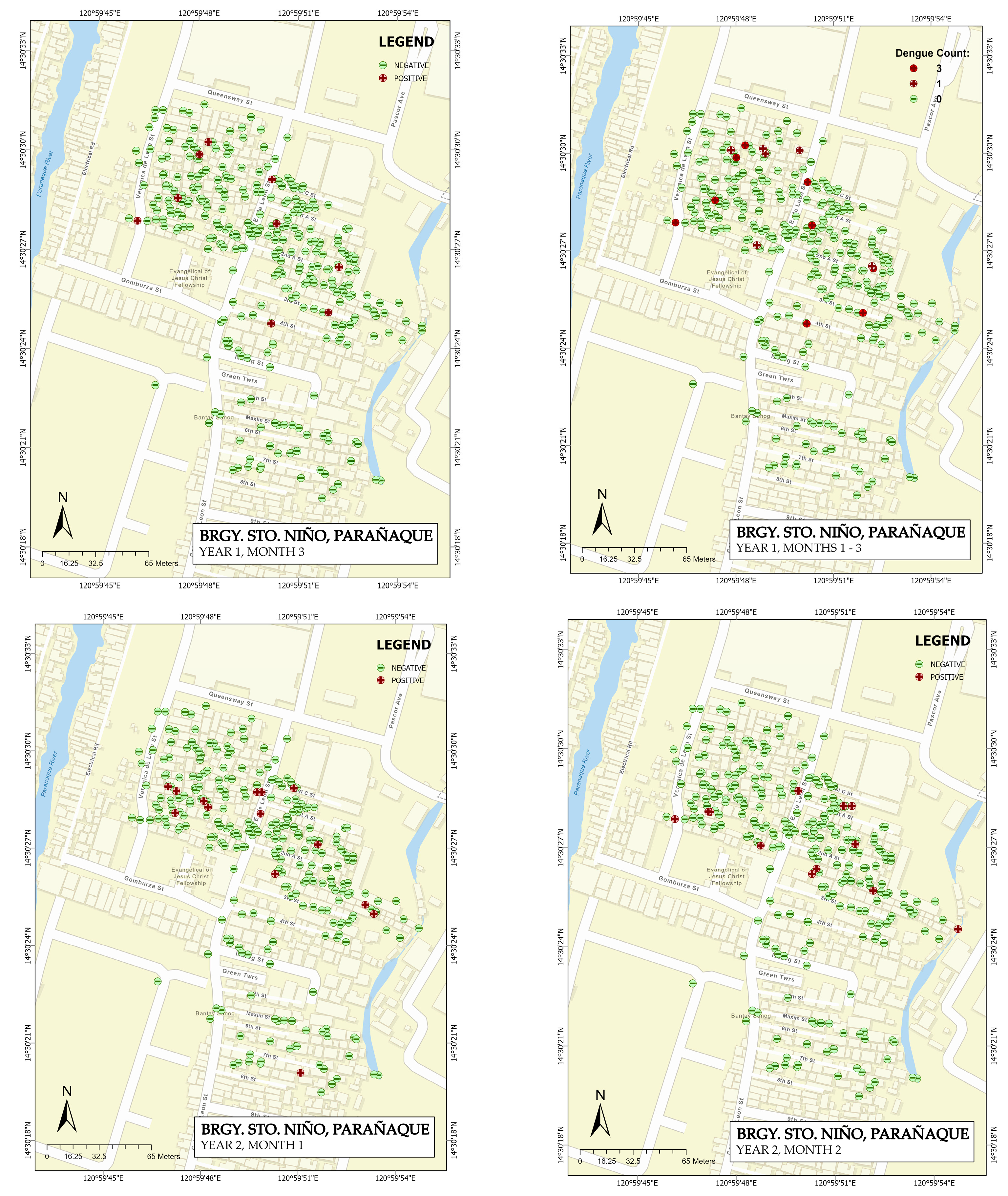
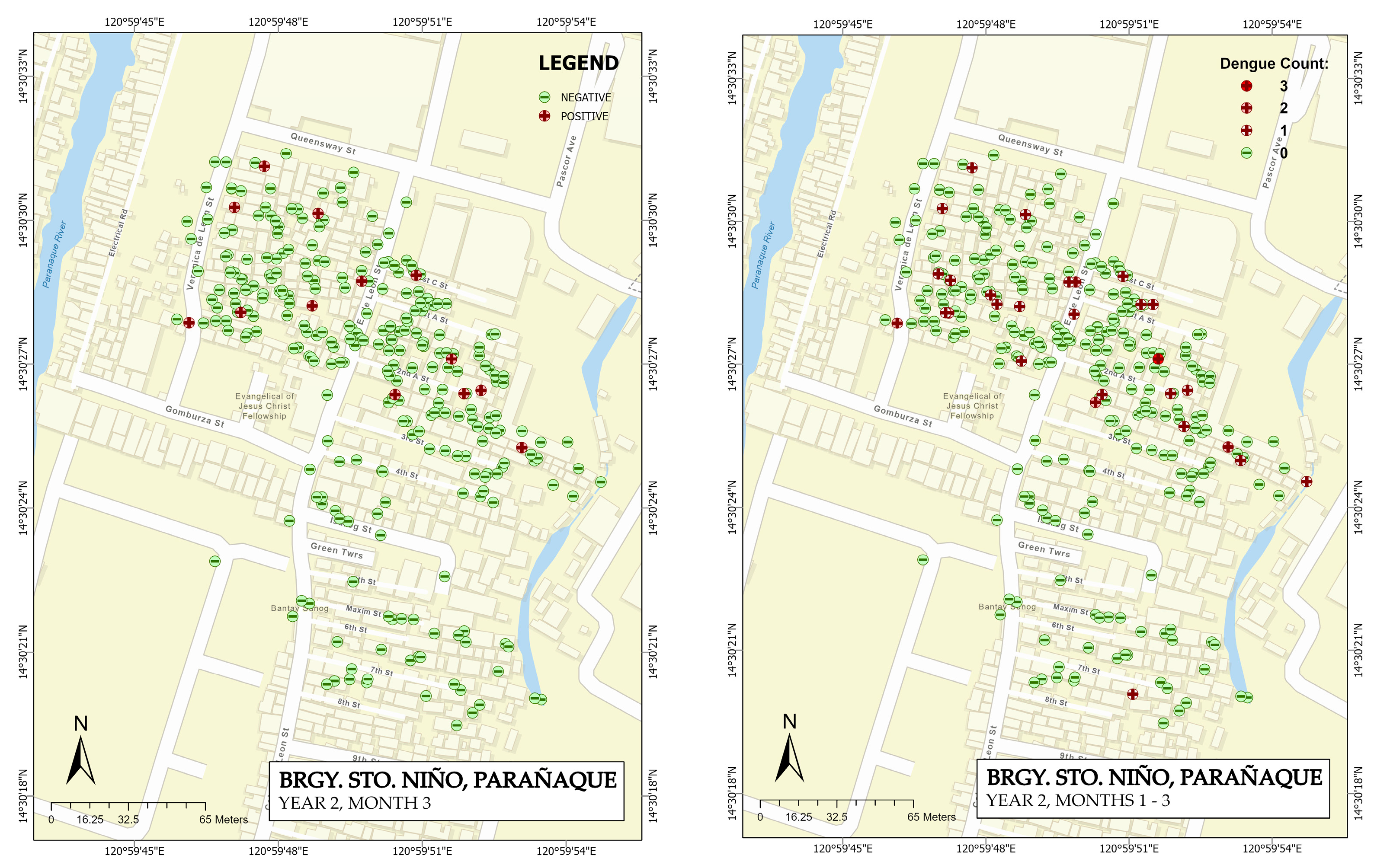
3.1. Map Generation
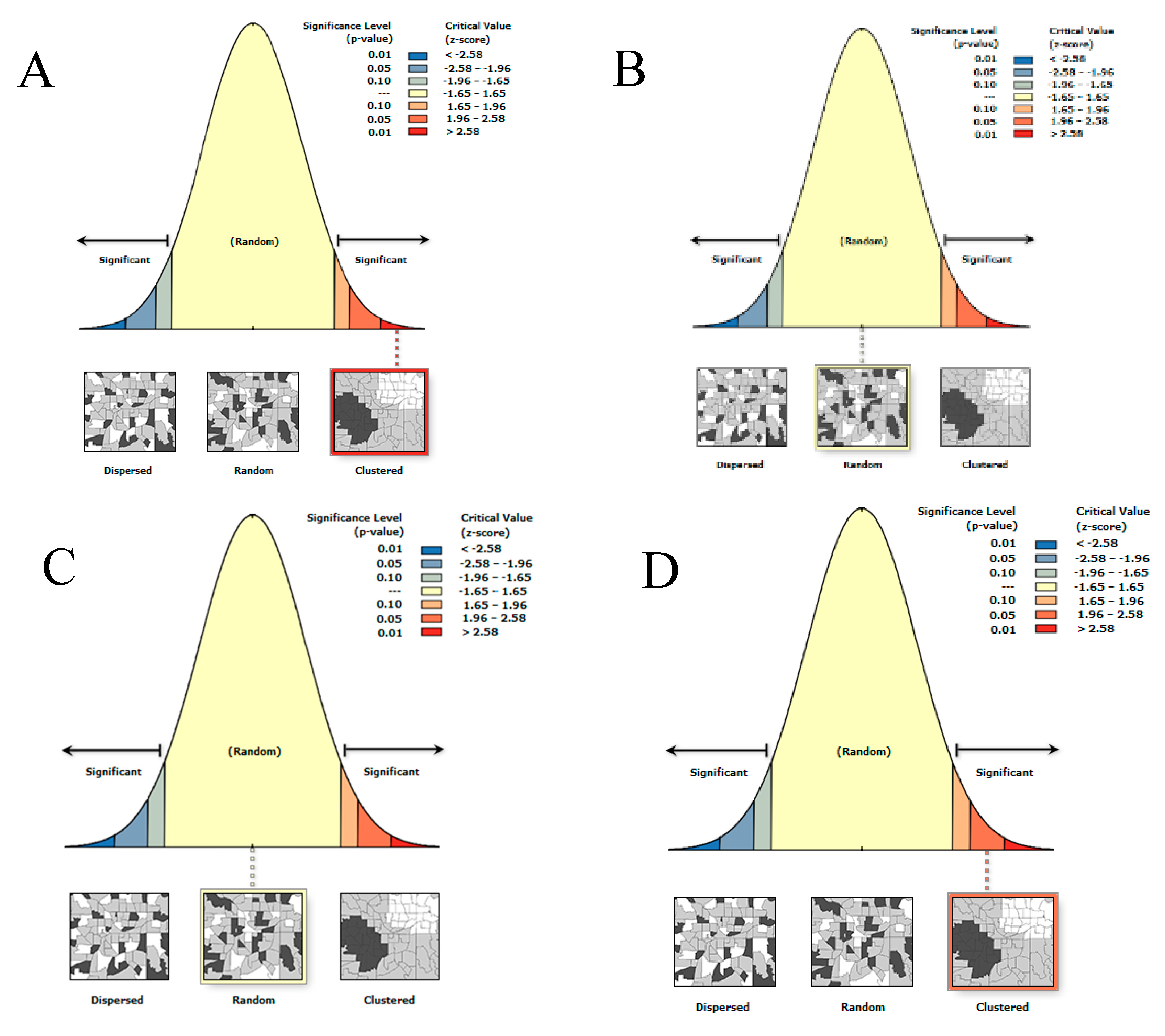
3.2. Global Moran’s I Spatial Autocorrelation
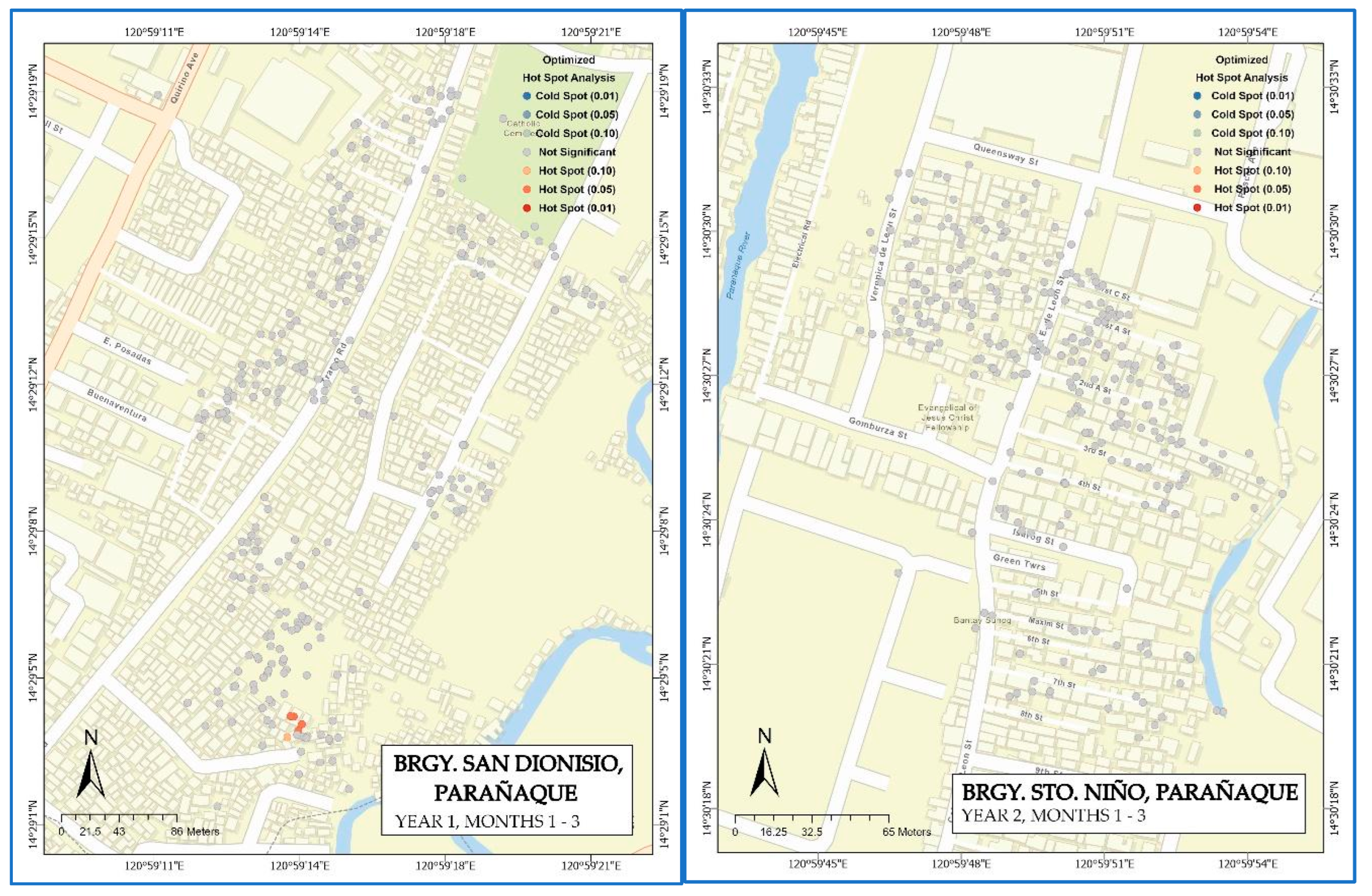
3.3. Optimized Hotspot Analysis of Clustered Years
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnson, B.W.; Russell, B.J.; Lanciotti, R.S. Serotype-specific detection of dengue viruses in a fourplex real-time reverse transcriptase PCR assay. J. Clin. Microbiol. 2005, 43, 4977–4983. [Google Scholar] [CrossRef] [PubMed]
- Read, M.C. Dengue and dengue haemorrhagic fever. Lancet 1998, 352, 971–977. [Google Scholar]
- Rigau-Pérez, J.G. Severe dengue: The need for new case definitions. Lancet Infect. Dis. 2006, 6, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Banu, S.; Guo, Y.; Hu, W.; Dale, P.; Mackenzie, J.S.; Mengersen, K.; Tong, S. Impacts of El Niño southern oscillation and Indian Ocean dipole on dengue incidence in Bangladesh. Sci. Rep. 2015, 5, 16105. [Google Scholar] [CrossRef]
- Ebi, K.L.; Nealon, J. Dengue in a changing climate. Environ. Res. 2016, 151, 115–123. [Google Scholar] [CrossRef]
- Murray, N.E.A.; Quam, M.B.; Wilder-Smith, A. Epidemiology of dengue: Past, present and future prospects. Clin. Epidemiol. 2013, 5, 299. [Google Scholar]
- Iguchi, J.A.; Seposo, X.T.; Honda, Y. Meteorological factors affecting dengue incidence in Davao, Philippines. BMC Public Health 2018, 18, 629. [Google Scholar] [CrossRef]
- Buonsenso, D.; Barone, G.; Onesimo, R.; Calzedda, R.; Chiaretti, A.; Valentini, P. The re-emergence of dengue virus in non-endemic countries: A case series. BMC Res. Notes 2014, 7, 596. [Google Scholar] [CrossRef]
- Seposo, X.T. Dengue at the time of COVID-19 in the Philippines. West. Pac. Surveill. Response J. WPSAR 2021, 12, 38. [Google Scholar] [CrossRef]
- Mahmud, M.A.F.; Abdul Mutalip, M.H.; Lodz, N.A.; Muhammad, E.N.; Yoep, N.; Hasim, M.H.; Abdul Rahim, F.A.; Aik, J.; Rajarethinam, J.; Muhamad, N.A. The Application of Environmental Management Methods in Combating Dengue: A Systematic Review. Int. J. Environ. Health Res. 2022, 1–20. Available online: https://www.tandfonline.com/doi/full/10.1080/09603123.2022.2076815 (accessed on 18 September 2022). [CrossRef]
- Santos, A.P. Philippines: Worst Dengue Outbreak in Years Kills over a Thousand. Aljazeera. Available online: https://www.aljazeera.com (accessed on 17 September 2019).
- Edillo, F.; Ymbong, R.R.; Bolneo, A.A.; Hernandez, R.J.; Fuentes, B.L.; Cortes, G.; Cabrera, J.; Lazaro, J.E.; Sakuntabhai, A. Temperature, season, and latitude influence development-related phenotypes of Philippine Aedes aegypti (Linnaeus): Implications for dengue control amidst global warming. Parasites Vectors 2022, 15, 74. [Google Scholar] [CrossRef] [PubMed]
- Bravo, L.; Roque, V.G.; Brett, J.; Dizon, R.; L’Azou, M. Epidemiology of dengue disease in the Philippines (2000–2011): A systematic literature review. PLoS Negl. Trop. Dis. 2014, 8, e3027. [Google Scholar] [CrossRef] [PubMed]
- Ligsay, A.; Telle, O.; Paul, R. Challenges to Mitigating the Urban Health Burden of Mosquito-Borne Diseases in the Face of Climate Change. Int. J. Environ. Res. Public Health 2021, 18, 5035. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.S.; Overgaard, H.J.; Pientong, C.; Mayxay, M.; Ekalaksananan, T.; Aromseree, S.; Phanthanawiboon, S.; Zafar, S.; Shipin, O.; Paul, R.E. Knowledge, attitudes, and practices on climate change and dengue in Lao People’s Democratic Republic and Thailand. Environ. Res. 2021, 193, 110509. [Google Scholar] [CrossRef]
- Fe, E. Community-based dengue vector control: Experiences in behavior change in Metropolitan Manila. Philipp. Pathog. Glob. Health 2012, 106, 455–460. [Google Scholar]
- World Health Organization & UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases. (2017). Framework for a national Vector Control Needs Assessment. World Health Organization. Available online: https://apps.who.int/iris/handle/10665/259405 (accessed on 1 October 2022).
- Devine, G.J.; Overgaard, H.J.; Paul, R.E. Global vector control guidelines–the need for co-creation. Trends Parasitol. 2019, 35, 267–270. [Google Scholar] [CrossRef]
- Mamun, M.A.; Misti, J.M.; Griffiths, M.D.; Gozal, D. The dengue epidemic in Bangladesh: Risk factors and actionable items. Lancet 2019, 394, 2149–2150. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Renhorn, K.-E.; Tissera, H.; Abu Bakar, S.; Alphey, L.; Kittayapong, P.; Lindsay, S.; Logan, J.; Hatz, C.; Reiter, P. DengueTools: Innovative tools and strategies for the surveillance and control of dengue. Glob. Health Action 2012, 5, 17273. [Google Scholar] [CrossRef]
- Chaki, P.P.; Govella, N.J.; Shoo, B.; Hemed, A.; Tanner, M.; Fillinger, U.; Killeen, G.F. Achieving high coverage of larval-stage mosquito surveillance: Challenges for a community-based mosquito control programme in urban Dar es Salaam, Tanzania. Malar. J. 2009, 8, 311. [Google Scholar] [CrossRef]
- Reiter, P. Oviposition, dispersal, and survival in Aedes aegypti: Implications for the efficacy of control strategies. Vector-Borne Zoonotic Dis. 2007, 7, 261–273. [Google Scholar] [CrossRef]
- Pell, J.; Macaulay, E.; Wilding, N. A pheromone trap for dispersal of the pathogen Zoophthora radicans Brefeld.(Zygomycetes: Entomophthorales) amongst populations of the diamondback moth, Plutella xylostella L. (Lepidoptera: Yponomeutidae). Biocontrol Sci. Technol. 1993, 3, 315–320. [Google Scholar] [CrossRef]
- Gross, H.R.; Hamm, J.J.; Carpenter, J.E. Design and application of a hive-mounted device that uses honey bees (Hymenoptera: Apidae) to disseminate Heliothis nuclear polyhedrosis virus. Environ. Entomol. 1994, 23, 492–501. [Google Scholar] [CrossRef]
- Itoh, T.; Kawada, H.; Abe, A.; Eshita, Y.; Rongsriyam, Y.; Igarashi, A. Utilization of bloodfed females of Aedes aegypti as a vehicle for the transfer of the insect growth regulator pyriproxyfen to larval habitats. J. Am. Mosq. Control Assoc. 1994, 10, 344–347. [Google Scholar] [PubMed]
- Abad-Franch, F.; Zamora-Perea, E.; Luz, S.L. Mosquito-disseminated insecticide for citywide vector control and its potential to block arbovirus epidemics: Entomological observations and modeling results from Amazonian Brazil. PLoS Med. 2017, 14, e1002213. [Google Scholar] [CrossRef]
- Seixas, G.; Paul, R.E.; Pires, B.; Alves, G.; de Jesus, A.; Silva, A.-C.; Devine, G.J.; Sousa, C.A. An evaluation of efficacy of the auto-dissemination technique as a tool for Aedes aegypti control in Madeira, Portugal. Parasites Vectors 2019, 12, 202. [Google Scholar] [CrossRef]
- Ligsay, A.D.; Tambio, K.J.M.; Aytona, M.J.M.; Alejandro, G.J.D.; Regencia, Z.J.G.; Baja, E.S.; Paul, R.E.L. Assessing Entomological and Epidemiological Efficacy of Pyriproxyfen-Treated Ovitraps in the Reduction of Aedes Species: A Quasi-Experiment on Dengue Infection Using Saliva Samples. Int. J. Environ. Res. Public Health 2022, 19, 3026. [Google Scholar] [CrossRef]
- Devine, G. Auto-dissemination of pyriproxyfen for the control of containerinhabiting mosquitoes—A progress review. Outlooks Pest Manag. 2016, 27, 164–167. [Google Scholar] [CrossRef]
- Gaugler, R.; Suman, D.; Wang, Y. An autodissemination station for the transfer of an insect growth regulator to mosquito oviposition sites. Med. Vet. Entomol. 2012, 26, 37–45. [Google Scholar] [CrossRef]
- Alvarado-Castro, V.; Paredes-Solís, S.; Nava-Aguilera, E.; Morales-Pérez, A.; Alarcón-Morales, L.; Balderas-Vargas, N.A.; Andersson, N. Assessing the effects of interventions for Aedes aegypti control: Systematic review and meta-analysis of cluster randomised controlled trials. BMC Public Health 2017, 17, 21–38. [Google Scholar] [CrossRef]
- Maoz, D.; Ward, T.; Samuel, M.; Müller, P.; Runge-Ranzinger, S.; Toledo, J.; Boyce, R.; Velayudhan, R.; Horstick, O. Community effectiveness of pyriproxyfen as a dengue vector control method: A systematic review. PLoS Negl. Trop. Dis. 2017, 11, e0005651. [Google Scholar] [CrossRef]
- Tsunoda, T.; Kawada, H.; Huynh, T.T.; Luu, L.L.; Le, S.H.; Tran, H.N.; Vu, H.T.; Le, H.M.; Hasebe, F.; Tsuzuki, A.; et al. Field trial on a novel control method for the dengue vector, Aedes aegypti by the systematic use of Olyset® Net and pyriproxyfen in Southern Vietnam. Parasit Vectors 2013, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Ocampo, C.B.; Mina, N.J.; Carabalí, M.; Alexander, N.; Osorio, L. Reduction in dengue cases observed during mass control of Aedes (Stegomyia) in street catch basins in an endemic urban area in Colombia. Acta Trop. 2014, 132, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Perez, M.; Consunji, R.; Rolloque, A.; Alcantara, M. Accessing local Government support for assessing the safety of homes in Paranaque city. Inj. Prev. 2010, 16, A36. [Google Scholar] [CrossRef]
- Alera, M.T.; Srikiatkhachorn, A.; Velasco, J.M.; Tac-An, I.A.; Lago, C.B.; Clapham, H.E.; Fernandez, S.; Levy, J.W.; Thaisomboonsuk, B.; Klungthong, C. Incidence of dengue virus infection in adults and children in a prospective longitudinal cohort in the Philippines. PLoS Negl. Trop. Dis. 2016, 10, e0004337. [Google Scholar] [CrossRef]
- Andries, A.-C.; Duong, V.; Ong, S.; Ros, S.; Sakuntabhai, A.; Horwood, P.; Dussart, P.; Buchy, P. Evaluation of the performances of six commercial kits designed for dengue NS1 and anti-dengue IgM, IgG and IgA detection in urine and saliva clinical specimens. BMC Infect. Dis. 2016, 16, 201. [Google Scholar] [CrossRef]
- Andries, A.-C.; Duong, V.; Ly, S.; Cappelle, J.; Kim, K.S.; Lorn Try, P.; Ros, S.; Ong, S.; Huy, R.; Horwood, P. Value of routine dengue diagnostic tests in urine and saliva specimens. PLoS Negl. Trop. Dis. 2015, 9, e0004100. [Google Scholar] [CrossRef]
- Mitchell, A. The ESRI Guide to GIS Analysis; Environmental Systems Research: Redlands, CA, USA, 2005; Volume 2. [Google Scholar]
- Scott, L.M.; Janikas, M.V. Spatial statistics in ArcGIS. In Handbook of Applied Spatial Analysis; Springer: Berlin/Heidelberg, Germany, 2010; pp. 27–41. [Google Scholar]
- Krivoruchko, K. Spatial Statistical Data Analysis for GIS Users; Esri Press: Redlands, CA, USA, 2011. [Google Scholar]
- Ord, J.K.; Getis, A. Local spatial autocorrelation statistics: Distributional issues and an application. Geogr. Anal. 1995, 27, 286–306. [Google Scholar] [CrossRef]
- Getis, A. Spatial autocorrelation. In Handbook of Applied Spatial Analysis; Springer: Berlin/Heidelberg, Germany, 2010; pp. 255–278. [Google Scholar]
- Pasaribu, A.P.; Tsheten, T.; Yamin, M.; Maryani, Y.; Fahmi, F.; Clements, A.C.; Gray, D.J.; Wangdi, K. Spatio-temporal patterns of dengue incidence in Medan city, North Sumatera, Indonesia. Trop. Med. Infect. Dis. 2021, 6, 30. [Google Scholar] [CrossRef]
- L’Azou, M.; Moureau, A.; Sarti, E.; Nealon, J.; Zambrano, B.; Wartel, T.A.; Villar, L.; Capeding, M.R.; Ochiai, R.L. Symptomatic dengue in children in 10 Asian and Latin American countries. N. Engl. J. Med. 2016, 374, 1155–1166. [Google Scholar] [CrossRef]
- Salazar, F.; Angeles, J.; Sy, A.K.; Inobaya, M.T.; Aguila, A.; Toner, T.; Bangs, M.J.; Thomsen, E.; Paul, R.E. Efficacy of the In2Care® auto-dissemination device for reducing dengue transmission: Study protocol for a parallel, two-armed cluster randomised trial in the Philippines. Trials 2019, 20, 269. [Google Scholar] [CrossRef]
- Thammavong, P.; Boyer, S.; Luangamath, P.; Phommavanh, N.; Vungkyly, V.; Nilaxay, S.; Lakeomany, K.; Brey, P.; Grandadam, M.; Marcombe, S. Small-scale field assessment against the dengue vector Aedes aegypti using the auto-dissemination approach in an urban area of Vientiane, Lao PDR. PLoS ONE 2022, 17, e0270987. [Google Scholar] [CrossRef] [PubMed]
- Buckner, E.A.; Williams, K.F.; Marsicano, A.L.; Latham, M.D.; Lesser, C.R. Evaluating the vector control potential of the In2Care® mosquito trap against Aedes aegypti and Aedes albopictus under semifield conditions in Manatee County, Florida. J. Am. Mosq. Control Assoc. 2017, 33, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Pathan, A.I.; Gandhi, P.J.; Agnihotri, P.; Patel, D. GIS-Based Geospatial Assessment of Novel Corona Virus (COVID-19) in One of the Promising Industrial States of India—A Case of Gujarat. Handb. Intell. Comput. Optim. Sustain. Dev. 2022, 849–868. [Google Scholar]
- Fradelos, E.C.; Papathanasiou, I.V.; Mitsi, D.; Tsaras, K.; Kleisiaris, C.F.; Kourkouta, L. Health based geographic information systems (GIS) and their applications. Acta Inform. Med. 2014, 22, 402. [Google Scholar] [CrossRef]
- Delavaran, H.; Kazemi, H.; Kamkar, B.; Gherekhloo, J. Development of a new model for health assessment in agroecosystems. Environ. Monit. Assess. 2022, 194, 78. [Google Scholar] [CrossRef]
- Garcia, F.B.; delas Llagas, L.A. An Examination of the Spatial Factors of Dengue Cases in Quezon City, Philippines: A Geographic Information System (GIS)-Based Approach. Acta Med. Philipp. 2011, 45, 53–62. [Google Scholar]
- Khalid, B.; Ghaffar, A. Environmental risk factors and hotspot analysis of dengue distribution in Pakistan. Int. J. Biometeorol. 2015, 59, 1721–1746. [Google Scholar] [CrossRef]
- Mutheneni, S.R.; Mopuri, R.; Naish, S.; Gunti, D.; Upadhyayula, S.M. Spatial distribution and cluster analysis of dengue using self organizing maps in Andhra Pradesh, India, 2011–2013. Parasite Epidemiol. Control 2018, 3, 52–61. [Google Scholar] [CrossRef]
- Wang, C.; Yang, W.; Fan, J.; Wang, F.; Jiang, B.; Liu, Q. Spatial and temporal patterns of dengue in Guangdong province of China. Asia Pac. J. Public Health 2015, 27, NP844–NP853. [Google Scholar] [CrossRef]
- Phanitchat, T.; Zhao, B.; Haque, U.; Pientong, C.; Ekalaksananan, T.; Aromseree, S.; Thaewnongiew, K.; Fustec, B.; Bangs, M.J.; Alexander, N. Spatial and temporal patterns of dengue incidence in northeastern Thailand 2006–2016. BMC Infect. Dis. 2019, 19, 743. [Google Scholar] [CrossRef]
- Abd Majid, N.; Muhamad Nazi, N.; Mohamed, A.F. Distribution and spatial pattern analysis on dengue cases in Seremban District, Negeri Sembilan, Malaysia. Sustainability 2019, 11, 3572. [Google Scholar] [CrossRef]
- Jeefoo, P.; Tripathi, N.K.; Souris, M. Spatio-temporal diffusion pattern and hotspot detection of dengue in Chachoengsao province, Thailand. Int. J. Environ. Res. Public Health 2011, 8, 51–74. [Google Scholar] [CrossRef] [PubMed]
- Al-Azab, A.M.; Al-ghamdi, K.M.; Shaheen, M.A.; Zaituon, A.A. The biological effects of sumilarv and flubex on dengue fever vector Aedes aegypti in Jeddah Governorate Saudi Arabia. Biosci. Biotechnol. Res. Asia 2013, 10, 235–240. [Google Scholar] [CrossRef]
- Berti, J.; Manzo, D.; Ramos, M.; Guerra, L.A. Eficacia y actividad residual del regulador de crecimiento pyriproxyfen sobre larvas de Aedes aegypti (Diptera: Culicidae) en condiciones de laboratorio. Boletín de Malariol. y Salud Ambient. 53 2013, 1, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Darriet, F.; Marcombe, S.; Etienne, M.; Yébakima, A.; Agnew, P.; Yp-Tcha, M.-M.; Corbel, V. Field evaluation of pyriproxyfen and spinosad mixture for the control of insecticide resistant Aedes aegypti in Martinique (French West Indies). Parasites Vectors 2010, 3, 88. [Google Scholar] [CrossRef]
- Lau, K.W.; Chen, C.D.; Lee, H.L.; Norma-Rashid, Y.; Sofian-Azirun, M. Evaluation of insect growth regulators against field-collected Aedes aegypti and Aedes albopictus (Diptera: Culicidae) from Malaysia. J. Med. Entomol. 2015, 52, 199–206. [Google Scholar] [CrossRef]
- Andrighetti, M.T.M.; Cerone, F.; Rigueti, M.; Galvani, K.C.; Macoris, M.d.L.d.G. Effect of Pyriproxyfen in Aedes Aegypti Populations with Different Levels of Susceptibility to the Organophosphate Temephos. Dengue Bull. 2008, 32, 186–198. [Google Scholar]
- Schafrick, N.H.; Milbrath, M.O.; Berrocal, V.J.; Wilson, M.L.; Eisenberg, J.N. Spatial clustering of Aedes aegypti related to breeding container characteristics in Coastal Ecuador: Implications for dengue control. Am. J. Trop. Med. Hyg. 2013, 89, 758. [Google Scholar] [CrossRef]
- Harrington, L.C.; Scott, T.W.; Lerdthusnee, K.; Coleman, R.C.; Costero, A.; Clark, G.G.; Jones, J.J.; Kitthawee, S.; Kittayapong, P.; Sithiprasasna, R. Dispersal of the dengue vector Aedes aegypti within and between rural communities. Am. J. Trop. Med. Hyg. 2005, 72, 209–220. [Google Scholar] [CrossRef]
- Misslin, R.; Telle, O.; Daudé, E.; Vaguet, A.; Paul, R.E. Urban climate versus global climate change—What makes the difference for dengue? Ann. N. Y. Acad. Sci. 2016, 1382, 56–72. [Google Scholar] [CrossRef]
- Romeo-Aznar, V.; Paul, R.; Telle, O.; Pascual, M. Mosquito-borne transmission in urban landscapes: The missing link between vector abundance and human density. Proc. R. Soc. B 2018, 285, 20180826. [Google Scholar] [CrossRef] [PubMed]
- Telle, O.; Nikolay, B.; Kumar, V.; Benkimoun, S.; Pal, R.; Nagpal, B.; Paul, R.E. Social and environmental risk factors for dengue in Delhi city: A retrospective study. PLoS Negl. Trop. Dis. 2021, 15, e0009024. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, B.; Karki, R.; Misslin, R.; Nakhapakorn, K.; Daudé, E.; Paul, R.E. Importance of Public Transport Networks for Reconciling the Spatial Distribution of Dengue and the Association of Socio-Economic Factors with Dengue Risk in Bangkok, Thailand. Int. J. Environ. Res. Public Health 2022, 19, 10123. [Google Scholar] [CrossRef] [PubMed]
- Huits, R.; Schwartz, E. Fatal outcomes of imported dengue fever in adult travelers from non-endemic areas are associated with primary infections. J. Travel Med. 2021, 28, taab020. [Google Scholar] [CrossRef] [PubMed]
- Thanh Toan, D.T.; Hu, W.; Quang Thai, P.; Ngoc Hoat, L.; Wright, P.; Martens, P. Hot spot detection and spatio-temporal dispersion of dengue fever in Hanoi, Vietnam. Glob. Health Action 2013, 6, 18632. [Google Scholar] [CrossRef]
- Chakravarti, A.; Matlani, M.; Jain, M. Immunodiagnosis of dengue virus infection using saliva. Curr. Microbiol. 2007, 55, 461–464. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics a | Barangays | |
|---|---|---|
| San Dionisio (n = 705) | Sto. Niño (n = 757) | |
| Age, years | 9.9 ± 5.6 | 13.1 ± 7.4 |
| Age categories, years | ||
| 1 to 10 | 61.7 | 43.0 |
| 11 to 20 | 33.2 | 40.3 |
| 21 to 30 | 5.1 | 16.7 |
| Male | 48.8 | 48.3 |
| Barangays | Collection Dates | Serostatus | ||
|---|---|---|---|---|
| Positive | Negative | |||
| San Dionisio | Year 1 | Month 1 | 76 | 598 |
| Month 2 | 65 | 609 | ||
| Month 3 | 103 | 566 | ||
| Year 2 | Month 1 | 16 | 561 | |
| Month 2 | 7 | 570 | ||
| Month 3 | 11 | 567 | ||
| Sto. Niño | Year 1 | Month 1 | 15 | 730 |
| Month 2 | 9 | 736 | ||
| Month 3 | 9 | 736 | ||
| Year 2 | Month 1 | 15 | 630 | |
| Month 2 | 13 | 620 | ||
| Month 3 | 13 | 620 | ||
| Barangays | Date | Moran’s Index | z-Scores | p-Values | Interpretation |
|---|---|---|---|---|---|
| San Dionisio | Year 1 | 0.027112 | 2.74 | 0.01 | clustered |
| Year 2 | 0.004152 | 0.51 | 0.61 | random | |
| Sto. Niño | Year 1 | −0.00263 | −0.18 | 0.86 | random |
| Year 2 | 0.017973 | 2.35 | 0.02 | clustered |
| Parameters | San Dionisio, Year 1 | Sto. Niño, Year 2 |
|---|---|---|
| Initial Data Assessment | 660 input features | 640 input features |
| Data Summary | ||
| Minimum count | 0 | 0 |
| Maximum count | 3 | 3 |
| Mean count | 0.3682 | 0.0625 |
| Standard Deviation | 0.8974 | 0.2945 |
| Locational Outliers | 3 outlier locations | 2 outlier locations |
| Scale of Analysis | 30 m optimal distance | 85 m optimal distance |
| Hotspot Analysis | 10 output features | 0 output features |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ligsay, A.D.; Regencia, Z.J.G.; Tambio, K.J.M.; Aytona, M.J.M.; Generale, A.J.A.; Alejandro, G.J.D.; Tychuaco, J.S.; De las Llagas, L.A.; Baja, E.S.; Paul, R.E.L. Efficacy Assessment of Autodissemination Using Pyriproxyfen-Treated Ovitraps in the Reduction of Dengue Incidence in Parañaque City, Philippines: A Spatial Analysis. Trop. Med. Infect. Dis. 2023, 8, 66. https://doi.org/10.3390/tropicalmed8010066
Ligsay AD, Regencia ZJG, Tambio KJM, Aytona MJM, Generale AJA, Alejandro GJD, Tychuaco JS, De las Llagas LA, Baja ES, Paul REL. Efficacy Assessment of Autodissemination Using Pyriproxyfen-Treated Ovitraps in the Reduction of Dengue Incidence in Parañaque City, Philippines: A Spatial Analysis. Tropical Medicine and Infectious Disease. 2023; 8(1):66. https://doi.org/10.3390/tropicalmed8010066
Chicago/Turabian StyleLigsay, Antonio D., Zypher Jude G. Regencia, Kristan Jela M. Tambio, Michelle Joyce M. Aytona, Alain Jason A. Generale, Grecebio Jonathan D. Alejandro, Jacquiline S. Tychuaco, Lilian A. De las Llagas, Emmanuel S. Baja, and Richard Edward L. Paul. 2023. "Efficacy Assessment of Autodissemination Using Pyriproxyfen-Treated Ovitraps in the Reduction of Dengue Incidence in Parañaque City, Philippines: A Spatial Analysis" Tropical Medicine and Infectious Disease 8, no. 1: 66. https://doi.org/10.3390/tropicalmed8010066
APA StyleLigsay, A. D., Regencia, Z. J. G., Tambio, K. J. M., Aytona, M. J. M., Generale, A. J. A., Alejandro, G. J. D., Tychuaco, J. S., De las Llagas, L. A., Baja, E. S., & Paul, R. E. L. (2023). Efficacy Assessment of Autodissemination Using Pyriproxyfen-Treated Ovitraps in the Reduction of Dengue Incidence in Parañaque City, Philippines: A Spatial Analysis. Tropical Medicine and Infectious Disease, 8(1), 66. https://doi.org/10.3390/tropicalmed8010066