
Economic and Social Costs of Noma: Design and Application of an Estimation Model to Niger and Burkina Faso

 , ,
, ,
Abstract
1. Introduction
2. Methods
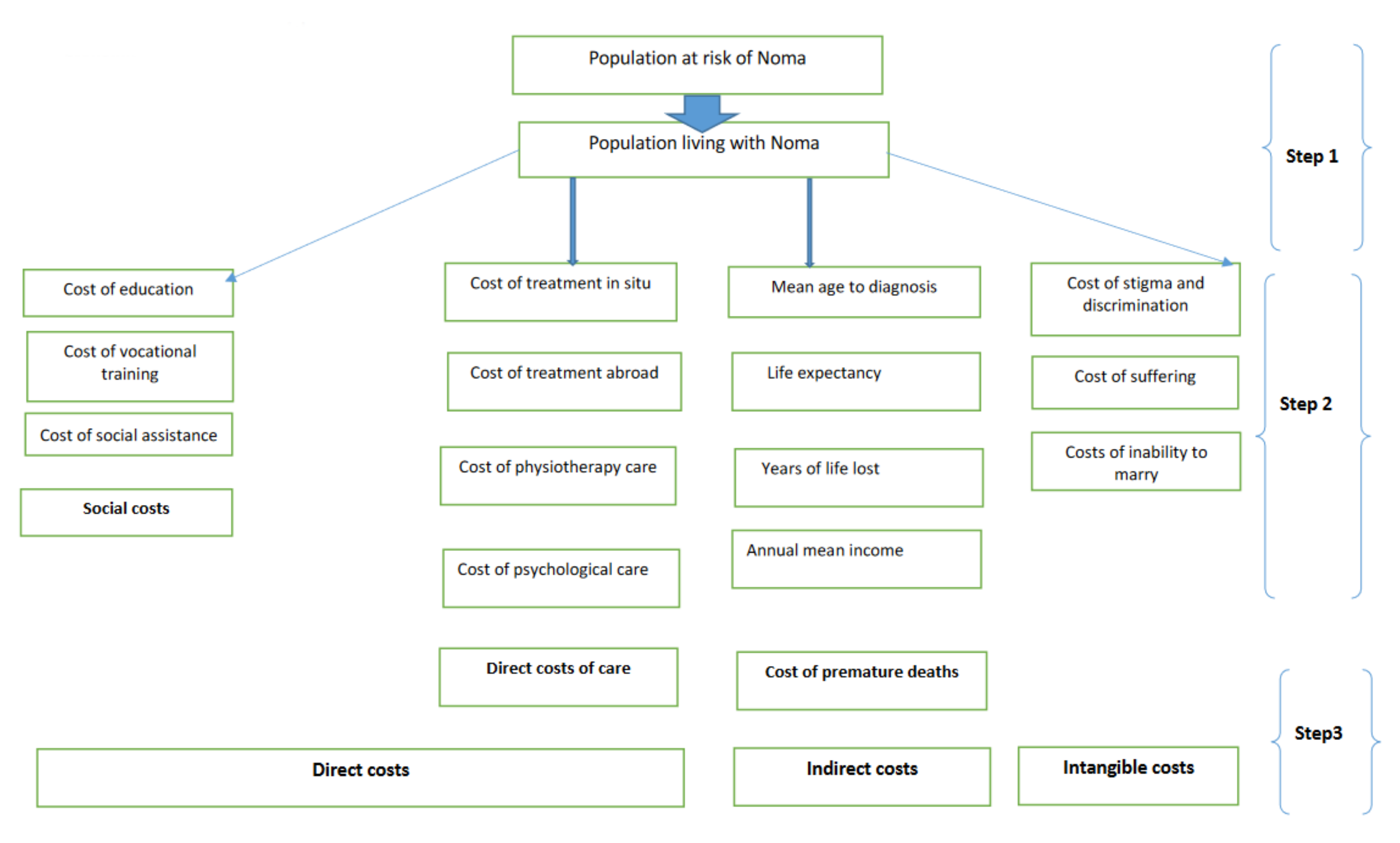
2.1. Model Design and Data Sources
2.1.1. Estimation of Noma Prevalence in Burkina and Niger (Step 1)
2.1.2. Identification of the Socio-Economic Indicators Used in The Model (Step 2)
2.1.3. Estimating the Economic and Social Costs of Noma (Step 3)
3. Results
3.1. Application of the Estimation Model to Burkina Faso and Niger
3.1.1. Prevalence of Noma
3.1.2. Health and Socio-Demographic Indicators
3.1.3. Economic and Social Costs of Noma in Burkina Faso and Niger
4. Discussion
- An apparent “gap” in research on noma, with the majority of work devoted to West Africa in general and to the countries belonging to the “noma belt” in particular;
- A predominance of clinical studies in the epidemiology of noma, with a critical lack of population-based studies, even though these are necessary to understand the extent of the condition;
- An apparent dearth of studies on the role and importance of social structures both in the emergence of noma and in the strategies to combat it;
- Widening the scope of research to include states where prevalence levels are not known and where there are no health data on the subject in existence;
- Testing the proposed noma cost estimation model by applying it to different contexts and different health and social systems;
- Orienting cost studies towards understanding the distribution of costs by paying agent (households, state, NGOs);
- Incorporating social sciences, in particular, political economics, sociology, history, anthropology, political epidemiology and human rights into the research and activities to combat noma;
- Encouraging and educating states that are already committed, not very committed or still in denial to invest in the prevention and fight against noma, thus avoiding the enormous costs of their inaction;
- Training health professionals, including traditional practitioners, in the diagnosis and care of people with noma and in the collection, management and use of social and health data on noma cases occurring in the community or received in consultation;
- Sharing good practices in prevention and care, and in the rehabilitation of noma survivors;
- Aiming in the long term at completely eradicating this disease of shame and collective irresponsibility towards our children.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Lead Organizations are the University of Geneva, Switzerland; The University of York, UK; The Swiss Tropical and Public Health Institute, Basel, Switzerland.
- Funders Organisations are Swiss Network for International Studies, Geneva, Switzerland; Hilfsaktion Noma e.V. Regensburg, Germany; Service de la Solidarité Internationale- Geneva, Switzerland; Noma-Hilfe-Schweiz, Zurich–Switzerland; Winds of Hope, Lausanne, Switzerland.
- Partners Organisations are Foundation Sentinelles, Lausanne, Switzerland; Hilfsaktion Noma e.V. Regensburg, Germany; Health Frontiers Laos, Vientiane, Laos; Médecins Sans Frontières, Geneva, Switzerland; SongES, Niamey, Niger; International No Noma Federation, Lausanne, Switzerland.
- Academics Partners are the Centre Interfacultaire en Droits de l’Enfant, University of Geneva, Switzerland; Centre de recherche en santé, Burkina Faso; Geneva Health Forum, Geneva, Switzerland.
- Governmental Bodies are the Ministry of Health, Ouagadougou, Burkina Faso
- Programme National de lutte contre les maladies bucco-dentaires et le noma, Niamey, Niger.
- Intergovernmental Partners are the United Nations Human Rights Council Advisory Committee; the United Nations Children’s Fund (UNICEF), Niger; the World Health Organisation, Geneva.
- Special Thanks to Valérie Elsig from Sentinelles Foundation for her support to this study.
References
- Ashok, N.; Tarakji, B.; Darwish, S.; Rodrigues, J.C.; Altamimi, M.A. A Review on Noma: A Recent Update. Glob. J. Health Sci. 2015, 8, 53–59. [Google Scholar] [CrossRef]
- Shaye, D.A.; Rabbels, J.; Adetunji, A.S.; Magee, A.; Vo, D.; Winters, R. Evaluation of the Noma Disease Burden Within the Noma Belt. JAMA Facial Plast. Surg. 2018, 20, 332–333. [Google Scholar] [CrossRef] [PubMed]
- Ibikunle, A.; Adeniyi, S.; Taiwo, A.; Braimah, R.; Gbotolorun, O.; Ogbeide, M.; Yekini, L.; Adeyemi, F. Pattern of tissue destruction among patients diagnosed with cancrum oris (Noma) at a Northwestern Nigerian Hospital, Sokoto. Saudi J. Oral Sci. 2017, 4, 101–105. [Google Scholar] [CrossRef]
- Bourgeois, D.M.; Leclercq, M.H. The World Health Organization initiative on noma. Oral Dis. 1999, 5, 172–174. [Google Scholar] [CrossRef] [PubMed]
- Tonna, J.E.; Lewin, M.R.; Mensh, B. A case and review of noma. PLoS Negl. Trop. Dis. 2010, 4, e869. [Google Scholar] [CrossRef] [PubMed]
- Wamba, A. Causes and pathogenesis of noma in Zinder (Niger): A socio-anthropological study. Med. Sante Trop. 2013, 23, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Wali, I.M.; Regmi, K. People living with facial disfigurement after having had noma disease: A systematic review of the literature. J. Health Psychol. 2017, 22, 1243–1255. [Google Scholar] [CrossRef] [PubMed]
- Srour, M.L.; Baratti-Mayer, D. Why is noma a neglected-neglected tropical disease? PLoS Negl. Trop. Dis. 2020, 14, e0008435. [Google Scholar] [CrossRef] [PubMed]
- Srour, M.L.; Marck, K.W.; Baratti-Mayer, D. Noma: Neglected, forgotten and a human rights issue. Int. Health 2015, 7, 149–150. [Google Scholar] [CrossRef]
- Srour, M.L.; Farley, E.; Mpinga, E.K. Lao Noma Survivors: A Case Series, 2002–2020. Am. J. Trop. Med. Hyg. 2022, 106, 1269. [Google Scholar] [CrossRef]
- Baratti-Mayer, D.; Pittet, B.; Montandon, D.; Bolivar, I.; Bornand, J.-E.; Hugonnet, S.; Jaquinet, A.; Schrenzel, J.; Pittet, D. Noma: An “infectious” disease of unknown aetiology. Lancet Infect. Dis. 2003, 3, 419–431. [Google Scholar] [CrossRef]
- Aluko-Olokun, B. Face of Noma and Extreme Poverty: Development of an Economic Index Derivable From Health Data. J. Craniofac. Surg. 2017, 28, 1342–1343. [Google Scholar] [CrossRef] [PubMed]
- WHO-Afro. Le Noma, une priorité pour la région africaine de l’OMS. 2006. Available online: https://docplayer.fr/20810794-Le-noma-une-priorite-pour-la-region-africaine-de-l-oms.html (accessed on 24 June 2022).
- Berthold, P. Noma: A forgotten disease. Dent. Clin. N. Am. 2003, 47, 559–574. [Google Scholar] [CrossRef]
- Ravinetto, R. Noma: Time to Address a Collective Moral Failure. Am. J. Trop. Med. Hyg. 2017, 96, 263–264. [Google Scholar] [CrossRef][Green Version]
- Simon, P.; Buta, E.; Gueorguieva, R.; Kong, G.; Morean, M.E.; Camenga, D.R.; Bold, K.W.; Krishnan-Sarin, S. Transitions across tobacco use profiles among adolescents: Results from the Population Assessment of Tobacco and Health (PATH) study waves 1 and 2. Addiction 2020, 115, 740–747. [Google Scholar] [CrossRef]
- Ordioni, N. Pauvreté et inégalités de droits en Afrique: Une perspective “genrée”. Mondes En Développement 2005, 129, 93–106. [Google Scholar] [CrossRef]
- Fieger, A.; Marck, K.W.; Busch, R.; Schmidt, A. An estimation of the incidence of noma in north-west Nigeria. Trop. Med. Int. Health TM IH 2003, 8, 402–407. [Google Scholar] [CrossRef]
- World Health Organisation. International Classification of Diseases 11th Revisions—DA0C.31: Noma. Available online: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/340823130 (accessed on 10 August 2021).
- Tall, F.; Ki-Zerbo, G.; Ouedraogo, I.; Guigma, Y. Le noma de l’enfant en milieu hospitalier de Bobo-Dioulasso: Aspects épidémiologiques, cliniques et prise en charge. Odonto-Stomatol. Trop. 2001, 96, 147. [Google Scholar]
- Kopp, P. Le Coût Social des Drogues en France; OFDT: Paris, France, 2015. [Google Scholar]
- Rice, D.P. Cost of illness studies: What is good about them? Inj. Prev. 2000, 6, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Verhaeghe, N.; Lievens, D.; Annemans, L.; Vander Laenen, F.; Putman, K. The health-related social costs of alcohol in Belgium. BMC Public Health 2017, 17, 958. [Google Scholar] [CrossRef]
- Baratti-Mayer, D.; Gayet-Ageron, A.; Hugonnet, S.; François, P.; Pittet-Cuenod, B.; Huyghe, A.; Bornand, J.-E.; Gervaix, A.; Montandon, D.; Schrenzel, J.; et al. Risk factors for noma disease: A 6-year, prospective, matched case-control study in Niger. Lancet Glob. Health 2013, 1, e87–e96. [Google Scholar] [CrossRef]
- Millogo, M.; Konsem, T.; Ouedraogo, D.; Ouoba, K.; Zwetyenga, N. HIV and noma in Burkina Faso. Rev. Stomatol. Chir. Maxillofac. 2012, 113, 433–436. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. GNI per Capita, Atlas Method—Burkina Faso. Available online: https://data.worldbank.org/indicator/NY.GNP.PCAP.CD?locations=BF (accessed on 8 August 2021).
- The World Bank. GNI per Capita, Atlas Method—Niger. Available online: https://data.worldbank.org/indicator/NY.GNP.PCAP.CD?locations=NE (accessed on 8 August 2021).
- Federal Statistical Office of Switzerland. Life Expectancy. Available online: https://www.bfs.admin.ch/bfs/en/home/statistics/population/births-deaths/life-expectancy.html (accessed on 8 August 2021).
- University of Shebrooke. Perspective Monde. Available online: https://perspective.usherbrooke.ca/bilan/BMEncyclopedie/BMEncycloListePays.jsp (accessed on 8 August 2021).
- Country Economy. Human Development Index. 2020. Available online: https://fr.countryeconomy.com/demographie/idh (accessed on 8 August 2021).
- NSD-S HUB; ACRST. Terrorism in the Sahel: Facts and Figures; NATO: Naples, Italy, 2020. [Google Scholar]
- Farley, E.; Bala, H.M.; Lenglet, A.; Mehta, U.; Abubakar, N.; Samuel, J.; de Jong, A.; Bil, K.; Oluyide, B.; Fotso, A.; et al. ‘I treat it but I don’t know what this disease is’: A qualitative study on noma (cancrum oris) and traditional healing in northwest Nigeria. Int. Health 2020, 12, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Farley, E.; Mehta, U.; Srour, M.L.; Lenglet, A. Noma (cancrum oris): A scoping literature review of a neglected disease (1843 to 2021). PLoS Negl. Trop. Dis. 2021, 15, e0009844. [Google Scholar] [CrossRef]
- Farley, E.; Oyemakinde, M.J.; Schuurmans, J.; Ariti, C.; Saleh, F.; Uzoigwe, G.; Bil, K.; Oluyide, B.; Fotso, A.; Amirtharajah, M.; et al. The prevalence of noma in northwest Nigeria. BMJ Glob. Health 2020, 5, e002141. [Google Scholar] [CrossRef]
- Bello, S.A.; Adeoye, J.A.; Oketade, I.; Akadiri, O.A. Estimated incidence and Prevalence of noma in north central Nigeria, 2010–2018: A retrospective study. PLoS Negl. Trop. Dis. 2019, 13, e0007574. [Google Scholar] [CrossRef]
- Baratti-Mayer, D.; Daou, B.M.; Gayet-Ageron, A.; Jeannot, E.; Pittet-Cuenod, B. Sociodemographic Characteristics of Traditional Healers and Their Knowledge of Noma: A Descriptive Survey in Three Regions of Mali. Int. J. Environ. Res. Public Health 2019, 16. [Google Scholar] [CrossRef]
- Konsem, T.; Millogo, M.; Assouan, C.; Ouedraogo, D. Evoluting form of cancrum oris, about 55 cases collected at the Academic Hospital Yalgado Ouedraogo of Ouagadougou. Bull. Soc. Pathol. Exot. 2014, 107, 74–78. [Google Scholar] [CrossRef]
- Bonkoungou, P.; Sawadogo, A.; Balaka, B.; Tall, F. The child’s noma in an hospital center in Burkina Faso: Clinical features and course. Mali Med. 2005, 20, 40–42. [Google Scholar]
- Isanaka, S.; Menzies, N.A.; Sayyad, J.; Ayoola, M.; Grais, R.F.; Doyon, S. Cost analysis of the treatment of severe acute malnutrition in West Africa. Matern. Child Nutr. 2017, 13, e12398. [Google Scholar] [CrossRef] [PubMed]
- Zoungrana, B.; Sawadogo, P.S.; Somda, N.S.; Tapsoba, F.; Tankoano, A.; Savadogo, A. Effectiveness and cost of management of severe acute malnutrition with complications in Kaya, Burkina Faso. Pan Afr. Med. J. 2019, 34, 145. [Google Scholar] [CrossRef] [PubMed]
- Sicuri, E.; Vieta, A.; Lindner, L.; Constenla, D.; Sauboin, C. The economic costs of malaria in children in three sub-Saharan countries: Ghana, Tanzania and Kenya. Malar J. 2013, 12, 307. [Google Scholar] [CrossRef] [PubMed]
- Sauerborn, R.; Shepard, D.S.; Ettling, M.B.; Brinkmann, U.; Nougtara, A.; Diesfeld, H.J. Estimating the direct and indirect economic costs of malaria in a rural district of Burkina Faso. Trop. Med. Parasitol. 1991, 42, 219–223. [Google Scholar]
- Population Data. Niger. Available online: https://www.populationdata.net/pays/niger/ (accessed on 8 August 2021).
- Population Data. Burkina Faso. Available online: https://en.populationdata.net/countries/burkina-faso/ (accessed on 8 August 2021).
- Idigbe, E.O.; Enwonwu, C.O.; Falkler, W.A.; Ibrahim, M.M.; Onwujekwe, D.; Afolabi, B.M.; Savage, K.O.; Meeks, V.I. Living conditions of children at risk for noma: Nigerian experience. Oral Dis. 1999, 5, 156–162. [Google Scholar] [CrossRef]
- Fujii, D.E.M.; Tokioka, A.B.; Lichton, A.I.; Hishinuma, E. Ethnic differences in prediction of violence risk with the HCR-20 among psychiatric inpatients. Psychiatr. Serv. 2005, 56, 711–716. [Google Scholar] [CrossRef]
- Zwetyenga, N.; See, L.A.; Szwebel, J.; Beuste, M.; Aragou, M.; Oeuvrard, C.; Martin, D.; Emparanza, A. Noma. Rev. Stomatol. Chir. Maxillofac. Chir. Orale 2015, 116, 261–279. [Google Scholar] [CrossRef]
- Prado-Calleros, H.M.; Castillo-Ventura, B.B.; Jimenez-Escobar, I.; Ramirez-Hinojosa, J.P.; Lopez-Gomez, A.; Garcia-de-la-Cruz, M.; Dayan-Nurko, M. Noma and Noma-like disease in HIV/AIDS patients, a comorbid interaction: A systematic review. J. Infect. Dev. Ctries. 2018, 12, 89–96. [Google Scholar] [CrossRef]
- Adeniyi, S.A.; Awosan, K.J. Pattern of noma (cancrum oris) and its risk factors in Northwestern Nigeria: A hospital-based retrospective study. Ann. Afr. Med. 2019, 18, 17–22. [Google Scholar] [CrossRef]
- Farley, E.; Lenglet, A.; Ariti, C.; Jiya, N.M.; Adetunji, A.S.; van der Kam, S.; Bil, K. Risk factors for diagnosed noma in northwest Nigeria: A case-control study, 2017. PLoS Negl Trop. Dis. 2018, 12, e0006631. [Google Scholar] [CrossRef]
- Makoutodé, P. Coût de la prise en charge des cas d’ulcère de Buruli au Centre de Dépistage et de Traitement de l’ulcère de Buruli d’Allada au Bénin. In Réunion Annuelle de l’Initiative Mondiale contre l’Ulcère de Buruli; World Health Organisation: Geneva, Switzerland, 2009. [Google Scholar]
- Bouassalo, K.M.; Mossi, E.K.; Padaro, E.; Gunepin, M.; Weber, E. Chronic lymphocytic leukemia revealed by a rare complication: Noma. First description from Togo. J. Oral Med. Oral Surg. 2019, 25, 31. [Google Scholar] [CrossRef]
- Denloye, O.O.; Aderinokun, G.A.; Lawoyin, J.O.; Bankole, O.O. Reviewing trends in the incidence of cancrum oris in Ibadan, Nigeria. West. Afr. J. Med. 2003, 22, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Ministère de la santé. Enquête nutritionnelle; Ministère de la Santé: Ouagadougou, Burkina Faso, 2020. [Google Scholar]
- Adefolaju, T. Traditional and Orthodox Medical Systems in Nigeria: The Imperative of a Synthesis. Am. J. Health Res. 2014, 2, 118–124. [Google Scholar] [CrossRef]
- Sittoni, T.; Maina, S. Impacts Économiques d’un Mauvais Assainissement en Afrique; Water and Sanitation Program: Washington, DC, USA, 2012. [Google Scholar]
- Langendorf, C.; Roederer, T.; de Pee, S.; Brown, D.; Doyon, S.; Mamaty, A.A.; Toure, L.W.; Manzo, M.L.; Grais, R.F. Preventing acute malnutrition among young children in crises: A prospective intervention study in Niger. PLoS Med. 2014, 11, e1001714. [Google Scholar] [CrossRef]
- Ministère de la santé publique. Comptes de la Santé 2016; Ministère de la Santé Publique: Niamey, Niger, 2018. [Google Scholar]
- Présidence du Faso. Note au Premier Ministre relative à l’élaboration du budget 2017; Présidence du Faso: Ouagadougou, Burkina Faso, 2016. [Google Scholar]
- IEPP-UNESCO. République du Niger. Analyse du secteur de l’Education; IEPP-UNESCO: Dakar, Senegal, 2020. [Google Scholar]
- Kouyate, B.; Sie, A.; Ye, M.; De Allegri, M.; Muller, O. The great failure of malaria control in Africa: A district perspective from Burkina Faso. PLoS Med. 2007, 4, e127. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, S.; Harati, R.; Lall, S.V.; Dikhanov, Y.M.; Hamadeh, N.; Oliver, W.V.; Rissanen, M.O.; Yamanaka, M. Comparing Costs of Living across World Cities. World Bank Econ. Rev. 2020, 34, S79–S88. [Google Scholar] [CrossRef]
- Mudogo, C.M. Vulnerability of Urban Poor Women and Children to the Triple. Burden of Malnutrition: A Scoping Review of the Sub-Saharan Africa Environment. Glob. J. Med. Res. Nutr. Food Sci. 2017, 17, 9–16. [Google Scholar]


{kind=link}
| Indicators | Burkina Faso | Niger |
|---|---|---|
| Surface area in km2 | 270,764 | 1,266,491 |
| Population (inhabitants)/2019 | 20,870,060 | 23,310,179 |
| Density (number of inhabitants per km2) | 77.08 | 18.40 |
| Mean annual income USD/2018 | 750.00 | 570.00 |
| Life expectancy at birth/2018 | 61.20 | 62.00 |
| Mortality rate < age 5 in ‰/2018 | 92.20 | 84.00 |
| Urbanization rate in %/2020 | 31.00 | 17.00 |
| Human Development Index/2019 | 0.452 | 0.394 |
| HDI rank in 2019 | 182/189 | 189/189 |
| Indicators | Burkina Faso | Niger |
|---|---|---|
| Total population | 20,244,080 | 22,442,948 |
| Population at risk of noma | 14,939,063 | 16,540,452 |
| Potential noma cases | 95,610 | 105,858 |
| Potential noma cases receiving treatment | 9561 | 10,585 |
| Indicators | Burkina Faso | Niger | Sources |
|---|---|---|---|
| Life expectancy at birth (years) | 61.20 | 62.00 | [43,44] |
| Mean age of mortality from noma (years) | 6.00 | 6.00 | [35,49,50] |
| Years of life lost | 55.20 | 56.00 | [35,48] |
| Mortality rate (without treatment) in % | 90.00 | 90.00 | [8,47] |
| Mean annual income per inhabitant in USD | 750.00 | 570.00 | [26,27] |
| Cost Category | Population | Mean Cost per Person in USD | Total Costs in USD | Data Sources |
|---|---|---|---|---|
| 1. Direct costs | 9561 | 28,179,901 | ||
| Costs of treatment | 9561 | 345 | 3,298,545 | A. |
| Costs of surgery | 5737 | 400 | 2,294,800 | B1. |
| Costs of accommodation | 5737 | 765 | 4,388,805 | B2. |
| Costs of psychological management | 5737 | 65 | 372,905 | B3. |
| Costs of physiotherapy | 5737 | 254 | 1,457,198 | B4. |
| Costs of assist. W. Income-gen. Activities | 5737 | 245 | 1,406,398 | B5. |
| Costs of schooling/vocational training | 1950 | 175 | 341,250 | B6. |
| Costs of care abroad | 172 | 85,000 | 14,620,000 | B7. |
| 2. Indirect costs | ||||
| Costs of loss of production | 25,870 | 750 | 19,402,500 | C1. |
| Costs related to premature death | 86,049 | 750 × 55.2 | 3,562,428,600 | C2. |
| Costs of inability to marry | 13,356 | 1000 | 13,365,000 | C3. |
| 3. Intangible costs | NN | NN | NN |
| Cost Category | Population | Mean Cost per Person in USD | Total Costs in USD | Data Sources |
|---|---|---|---|---|
| 1. Direct costs | 10,585 | 30,746,063 | ||
| Costs of treatment | 10,585 | 345 | 3,651,825 | A. |
| Costs of surgery | 6372 | 400 | 2,548,800 | B1. |
| Costs of accommodation | 6372 | 765 | 4,874,580 | B2. |
| Costs of psychological management | 6372 | 65 | 414,180 | B3. |
| Costs of physiotherapy | 6372 | 254 | 1,618,488 | B4. |
| Costs of assist. W. Income-gen. activities | 6372 | 245 | 1,561,140 | B5. |
| Costs of schooling/vocational training. | 2166 | 175 | 379,050 | B6. |
| Costs of care abroad | 185 | 85,000 | 15,725,000 | B7. |
| 2. Indirect costs | ||||
| Costs of loss of production | 28,581 | 570 | 16,291,170 | C1. |
| Costs related to premature death | 95,272 | 570 × 56 | 3,041,082,240 | C2. |
| Costs of inability to marry | 14,820 | 1000 | 14,820,000 | C3. |
| 3. Intangible costs | NN | NN | NN |
| Cost Categories | Burkina Faso Populations/Costs in US Dollars | Niger Populations/Costs in US Dollars | ||
|---|---|---|---|---|
| 1. Direct costs | 9561 | 28,179,901 | 10,585 | 30,746,063 |
| Costs of treatment | 9561 | 3,298,545 | 10,585 | 3,651,825 |
| Costs of surgery | 5737 | 2,294,800 | 6372 | 2,548,800 |
| Costs of accommodation | 5737 | 4,388,805 | 6372 | 4,874,580 |
| Costs of psychological care | 5737 | 372,905 | 6372 | 414,180 |
| Costs of physiotherapy | 5737 | 1,457,198 | 6372 | 1,618,488 |
| Costs of schooling/vocational training | 1950 | 341,250 | 2166 | 379,050 |
| Costs of assist. W. Income-gen. Activities | 5737 | 1,406,398 | 6372 | 1,561,140 |
| Costs of care abroad | 172 | 14,620,000 | 185 | 15,725,000 |
| 2. Indirect costs | ||||
| Costs of loss of production | 28,581 | 19,402,500 | 28,581 | 16,291,170 |
| Costs related to premature death | 95,272 | 3,562,428,600 | 95,272 | 3,041,082,240 |
| Costs of inability to marry | 14,820 | 13,365,000 | 14,820 | 14,820,000 |
| 3. Intangible costs | NN | NN | NN | NN |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mpinga, E.K.; Srour, M.L.; Moussa, M.-S.A.; Dupuis, M.; Kagoné, M.; Grema, M.S.M.; Zacharie, N.-B.; Baratti-Mayer, D. Economic and Social Costs of Noma: Design and Application of an Estimation Model to Niger and Burkina Faso. Trop. Med. Infect. Dis. 2022, 7, 119. https://doi.org/10.3390/tropicalmed7070119
Mpinga EK, Srour ML, Moussa M-SA, Dupuis M, Kagoné M, Grema MSM, Zacharie N-B, Baratti-Mayer D. Economic and Social Costs of Noma: Design and Application of an Estimation Model to Niger and Burkina Faso. Tropical Medicine and Infectious Disease. 2022; 7(7):119. https://doi.org/10.3390/tropicalmed7070119
Chicago/Turabian StyleMpinga, Emmanuel Kabengele, Margaret Leila Srour, Marie-Solène Adamou Moussa, Marc Dupuis, Moubassira Kagoné, Maïna Sani Malam Grema, Ngoyi-Bukonda Zacharie, and Denise Baratti-Mayer. 2022. "Economic and Social Costs of Noma: Design and Application of an Estimation Model to Niger and Burkina Faso" Tropical Medicine and Infectious Disease 7, no. 7: 119. https://doi.org/10.3390/tropicalmed7070119
APA StyleMpinga, E. K., Srour, M. L., Moussa, M.-S. A., Dupuis, M., Kagoné, M., Grema, M. S. M., Zacharie, N.-B., & Baratti-Mayer, D. (2022). Economic and Social Costs of Noma: Design and Application of an Estimation Model to Niger and Burkina Faso. Tropical Medicine and Infectious Disease, 7(7), 119. https://doi.org/10.3390/tropicalmed7070119