
A Cross-Sectional Survey on the Malaria Control and Prevention Knowledge, Attitudes, and Practices of Caregivers of Children Under-5 in the Western Area of Sierra Leone

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
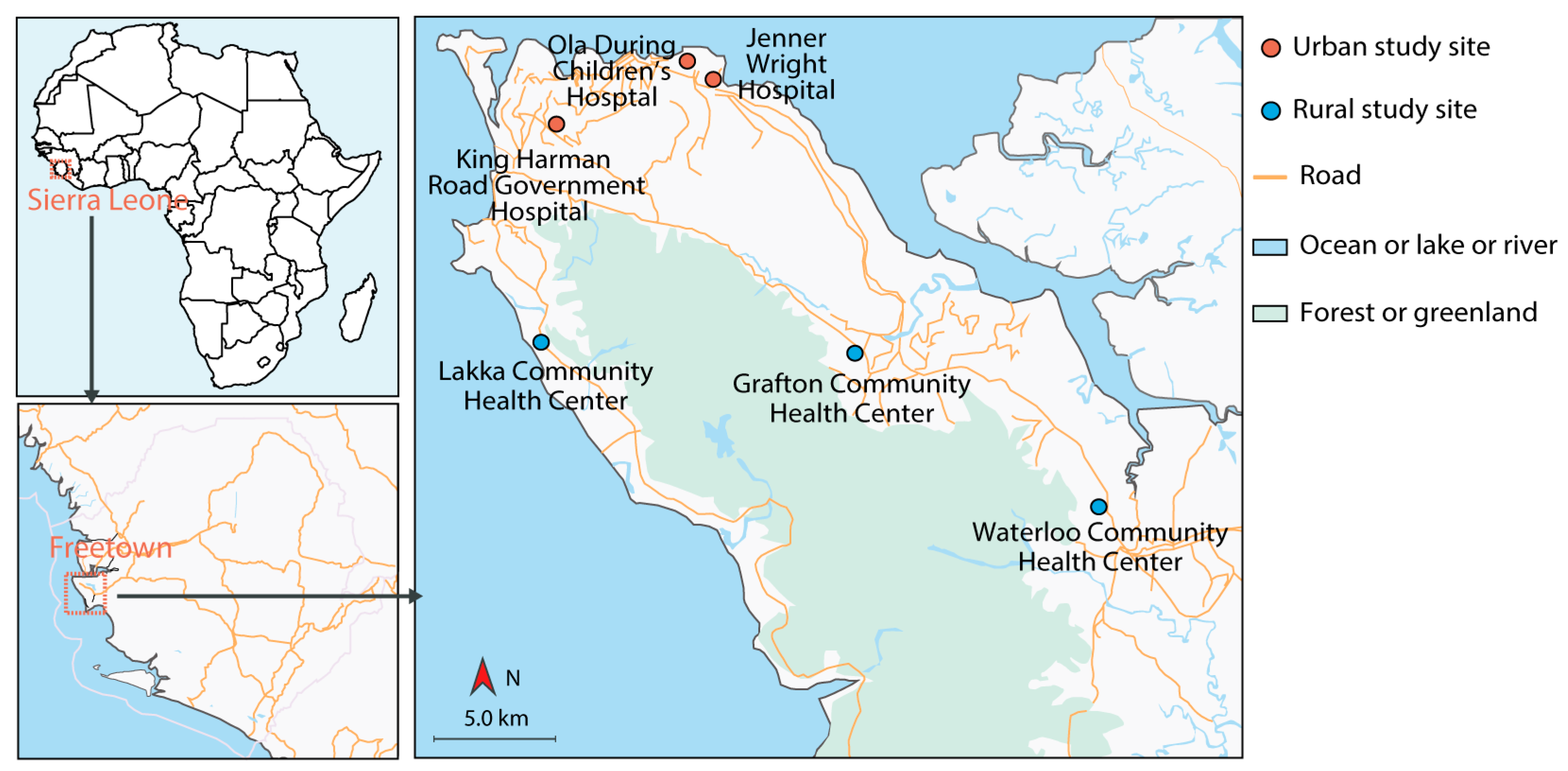
2.1. Setting
2.2. Study Population and Eligibility Criteria
2.3. Sample Size
2.4. Survey Questionnaire
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Socio-Demographic Characteristics of the Caregivers
3.2. Knowledge
3.3. Attitudes
3.4. Practices
3.5. Correlations among Knowledge, Attitudes, and Practices
3.6. Effects of Socio-Demographic Characteristics on KAPs
4. Discussion
4.1. Knowledge
4.2. Attitudes
4.3. Practices
4.4. Correlation among Malaria Related KAPs
4.5. Correlation between Caregivers’ Socio-Demographic Characteristics and KAPs
5. Conclusions
6. Limitations of this Study
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Malaria Report 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- DePina, A.J.; Dia, A.K.; Martins, A.; Ferreira, M.C.; Moreira, A.L.; Leal, S.V.; Pires, C.M.; Moreira, J.M.G.; Tavares, M.F.; da Moura, A.J.F.; et al. Knowledge, attitudes and practices about malaria in Cabo Verde: A country in the pre-elimination context. BMC Public Health 2019, 19, 850. [Google Scholar] [CrossRef] [PubMed]
- Government of Sierra Leone Ministry of Health and Sanitation National Malaria Control Programme. Guidelines for Case Management of Malaria in Sierra Leone, 4th ed.; WHO Africa: Freetown, Sierra Leone, 2015. [Google Scholar]
- NMCP; INFORM; LSHTM. Sierra Leone: A Profile of Malaria Control and Epidemiology; London School of Hygiene and Tropical Medicine: London, UK, 2015. [Google Scholar]
- Tabbabi, A. Socio-economic impact of malaria in Africa. ASMI 2018, 1, 32–34. [Google Scholar]
- Government of Sierra Leone Ministry of Health and Sanitation. Sierra Leone Malaria Control Strategic Plan 2016–2020; WHO Africa: Freetown, Sierra Leone, 2015.
- World Health Organization. A Framework for Malaria Elimination; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. Global Technical Strategy for Malaria 2016–2030, 2021 Update; World Health Organization: Geneva, Switzerland, 2021; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- Catholic Relief Services (CRS); College of Medicine and Allied Health Sciences; University of Sierra Leone (COMAHS); ICF International; National Malaria Control Programme (Sierra Leone); Roll Back Malaria Partnership; Statistics Sierra Leone. Sierra Leone Malaria Indicator Survey 2016; ICF International: Fairfax, WV, USA, 2017. [Google Scholar]
- Oladimeji, K.E.; Tsoka-Gwegweni, J.M.; Ojewole, E.; Yunga, S.T. Knowledge of malaria prevention among pregnant women and non-pregnant mothers of children aged under 5 years in Ibadan, South West Nigeria. Malar. J. 2019, 18, 92. [Google Scholar] [CrossRef]
- Hlongwana, K.W.; Mabaso, M.L.; Kunene, S.; Govender, D.; Maharaj, R. Community knowledge, attitudes and practices (KAPs) on malaria in Swaziland: A country earmarked for malaria elimination. Malar. J. 2009, 8, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khairy, S.; Al-Surimi, K.; Ali, A.; Shubily, H.M.; Walaan, N.A.; Househ, M.; Walaan, N.A.; Househ, M.; El-Metwally, A. Knowledge, attitude and practice about malaria in south-western Saudi Arabia: A household-based cross-sectional survey. J. Infect. Public Health 2017, 10, 499–506. [Google Scholar] [CrossRef]
- Yaya, S.; Bishwajit, G.; Ekholuenetale, M.; Shah, V.; Kadio, B.; Udenigwe, O. Knowledge of prevention, cause, symptom and practices of malaria among women in Burkina Faso. PLoS ONE 2017, 12, e0180508. [Google Scholar]
- Shimaponda-Mataa, N.M.; Tembo-Mwase, E.; Gebreslasie, M.; Mukaratirwa, S. Knowledge, attitudes and practices in the control and prevention of malaria in four endemic provinces of Zambia. SAJID 2016, 32, 29–39. [Google Scholar]
- Kassam, R.; Sekiwunga, R.; MacLeod, D.; Tembe, J.; Liow, E. Patterns of treatment-seeking behaviors among caregivers of febrile young children: A Ugandan multiple case study. BMC Public Health 2016, 16, 160. [Google Scholar] [CrossRef] [Green Version]
- Cochran, W.G. Sampling Techniques, 3rd ed.; John Wiley & Sons: New York, NY, USA, 1977; pp. 72–76. [Google Scholar]
- U.S. President’s Malaria Initiative. Sierra Leone Malaria Operational Plan; FY 2018 & FY 2019; U.S. President’s Malaria Initiative: Freetown, Sierra Leone, 2020.
- Gupta, R.K.; Raina, S.K.; Shora, T.N.; Jan, R.; Sharma, R.; Hussain, S. A household survey to assess community knowledge, attitude and practices on malaria in a rural population of Northern India. JFMPC 2016, 5, 101–107. [Google Scholar]
- Janet, K.; Catherine, A.; Folake, O.; Precious, O.; Yewande, D.A. Knowledge, attitudes and practices of mothers of under-five regarding prevention of malaria in children: Evidence from ogun state, Nigeria. IOSR-JHSS 2016, 21, 1–7. [Google Scholar] [CrossRef]
- Onarheim, S.A.; Andrew, Y.K.; Bjørn, B. Education and knowledge helps combating malaria, but not degedege: A cross-sectional study in Rufiji, Tanzania. Malar. J. 2014, 13, 200. [Google Scholar] [CrossRef] [Green Version]
- WHO: Malaria Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/malaria (accessed on 16 June 2012).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988; 567p. [Google Scholar]
- Collins, C.; Xu, J.; Tang, S. Schistosomiasis control and the health system in P.R. China. Infect. Dis. Poverty 2012, 1, 8. [Google Scholar] [CrossRef] [Green Version]
- Mazigo, H.D.; Obasy, E.; Mauka, W.; Manyiri, P.; Zinga, M.; Kweka, E.J.; Mnyone, L.L.; Heukelbach, J. Knowledge, attitudes, and practices about malaria and its control in rural northwest Tanzania. Malar. Res. Treat. 2010, 2010, 794261. [Google Scholar] [CrossRef] [Green Version]
- Smithson, P.; Florey, L.; Salgado, S.R.; Hershey, C.L.; Masanja, H.; Bhattarai, A.; Mwita, A.; McElroy, P.D. Tanzania Malaria Impact Evaluation Research Group. Impact of malaria control on mortality and anemia among Tanzanian children less than five years of age, 1999–2010. PLoS ONE 2015, 10, e0141112. [Google Scholar]
- Nejati, J.; Moosa-Kazemi, S.H.; Saghafipour, A.; Soofi, K. Knowledge, attitude and practice (KAP) on malaria, from high malaria burden rural communities, southeastern Iran. J. Parasit. Dis. 2018, 42, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Govere, J.; Durrheim, D.; Grange, K.; Mabuza, A.; Booman, M. Community knowledge and perceptions about malaria and practices influencing malaria control in Mpumalanga Province, South Africa. S. Afr. Med. J. 2000, 90, 611–618. [Google Scholar]
- Obol, J.; Lagoro, K.; Garimoi, O.C. Knowledge and misconceptions about malaria among pregnant women in a post-conflict internally displaced persons’ camps in Gulu district, northern Uganda. Malar. Res. Treat. 2011, 2011, 107987–107994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathania, M.M.; Kimera, S.I.; Silayo, R.S. Knowledge and awareness of malaria and mosquito biting behaviour in selected sites within Morogoro and Dodoma regions Tanzania. Malar. J. 2016, 15, 287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dujing, S.L. Malaria in Children under 5 Years in the Gushegu District Hospital before and after Indoor Residual Spraying in Northern Ghana. Master’s Thesis, University of Ghana, Accra, Ghana, July 2015. [Google Scholar]
- Nyirakanani, C.; Chibvongodze, R.; Habtu, M.; Masika, M.; Mukoko, D.; Njunwa, K.J. Prevalence and risk factors of asymptomatic malaria among under-five children in Huye District, Southern Rwanda. Tanzan. J. Health Res. 2018, 20, 1–7. [Google Scholar]
- O’Donnell, A.J.; Rund, S.S.C.; Reece, S.E. Time-of-day of blood-: Effects on mosquito life history and malaria transmission. Parasites Vectors 2019, 12, 301. [Google Scholar] [CrossRef]
- Pigeault, R.; Caudron, Q.; Nicot, A.; Rivero, A.; Gandon, S. Timing malaria transmission with mosquito fluctuations. Evol. Lett. 2018, 2, 378–389. [Google Scholar] [CrossRef] [Green Version]
- Statistics Sierra Leone (SSL) and ICF International. Sierra Leone Demographic and Health Survey 2013; SSL and ICF International: Freetown, Sierra Leone; Rockville, ML, USA, 2014. [Google Scholar]
- Htwe, E.P. Caregivers’ Malaria Preventive Practices for Under-Five Children and Its Association in Ngapudaw High-Risk Township, Ayeyarwady Region-Myanmar. Master’s Thesis, Chulalongkorn University, Bangkok, Thailand, 2017. [Google Scholar]
- Lungu, E.A.; Obse, A.G.; Darker, C.; Biesma, R. What influences where they seek care? Caregivers’ preferences for under-five child healthcare services in urban slums of Malawi: A discrete choice experiment. PLoS ONE 2018, 13, e0189940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Guidelines for the Treatment of Malaria, 3rd ed.; WHO Press: Geneva, Switzerland, 2015. [Google Scholar]
- Taylor, C.; Florey, L.; Ye, Y. Equity trends in ownership of insecticide-treated nets in 19 sub-Saharan African countries. Bull. World Health Organ. 2017, 95, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Tizifa, T.A.; Kabaghe, A.N.; McCann, R.S.; van den Berg, H.; Van Vugt, M.; Phiri, K.S. Prevention efforts for malaria. Curr. Trop. Med. Rep. 2018, 5, 41–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gachelin, G.; Garner, P.; Ferroni, E.; Verhave, J.P.; Opinel, A. Evidence and strategies for malaria prevention and control: A historical analysis. Malar. J. 2018, 17, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mpimbaza, A.; Ndeezi, G.; Katahoire, A.; Rosenthal, P.J.; Karamagi, C. Demographic, socioeconomic, and geographic factors leading to severe malaria and delayed care seeking in Ugandan children: A case-control study. Am. J. Trop. Med. Hyg. 2017, 97, 1513–1523. [Google Scholar] [CrossRef]
- Adinan, J.; Damian, D.J.; Mosha, N.R.; Mboya, I.B.; Mamseri, R.; Msuya, S.E. Individual and contextual factors associated with appropriate healthcare seeking behavior among febrile children in Tanzania. PLoS ONE 2017, 12, e0175446. [Google Scholar] [CrossRef] [Green Version]
- Measure Evaluation. Capacity of Sierra Leone’s National Malaria Control Programme for Monitoring and Evaluation: Baseline Assessment; University of North Carolina: Chapel Hill, NC, USA, 2019. [Google Scholar]
- Thandar, M.M.; Kyaw, M.P.; Jimba, M.; Yasuoka, J. Caregivers’ treatment-seeking behaviour for children under age five in malaria-endemic areas of rural Myanmar: A cross-sectional study. Malar. J. 2015, 14, 1. [Google Scholar] [CrossRef] [Green Version]
- Elfaki, A.E.M.; Elnimeiri, M.K.M.; Elfakey, W.E.M. Management seeking behavior of malaria among mothers of under-five year’s children in Damazin Locality, Blue Nile State, Sudan. IJPSI 2017, 6, 14–19. [Google Scholar]
- Beeson, J.G.; Boeuf, P.; Fowkes, F.J. Maximizing antimalarial efficacy and the importance of dosing strategies. BMC Med. 2015, 13, 110. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.K.; Haq, S.; Dhiman, R.C. Studies on knowledge, attitude and practices in malaria endemic tribal areas of Bihar and Jharkhand, India. J. Trop. Dis. Public Health 2013, 1, 110. [Google Scholar]
- Israel, O.K.; Fawole, O.I.; Adebowale, A.S.; Ajayi, I.O.; Yusuf, O.B.; Oladimeji, A.; Ajumobi, O. Caregivers’ knowledge and utilization of long-lasting insecticidal nets among under-five children in Osun State, Southwest, Nigeria. Malar. J. 2018, 17, 231. [Google Scholar] [CrossRef] [PubMed]
- Eseigbe, E.E.; Anyiam, J.O.; Ogunrinde, G.O.; Wammanda, R.D.; Zoaka, H.A. Health care seeking behavior among caregivers of sick children WHO had cerebral malaria in northwestern Nigeria. Malar. Res. Treat. 2012, 2012, 954975. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F. Social implications of malaria and their relationships with poverty. Mediterr. J. Hematol. Infect. Dis. 2012, 4, e2012048. [Google Scholar] [CrossRef] [PubMed]
- Davies, M. Women’s Perceptions of Malaria in the Western Rural Areas of Sierra Leone. Ph.D. Thesis, Walden University, Minneapolis, MN, USA, August 2018. [Google Scholar]
- Orimadegun, A.E.; Ilesanmi, K.S. Mothers’ understanding of childhood malaria and practices in rural communities of Ise-Orun, Nigeria: Implications for malaria control. J. Fam. Med. Prim. Care 2015, 4, 226–231. [Google Scholar] [CrossRef]
- Mitiku, I.; Assefa, A. Caregivers’ perception of malaria and treatment-seeking behaviour for under five children in Mandura District, West Ethiopia: A cross-sectional study. Malar. J. 2017, 16, 144. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | Variables | Frequency | Percentage (%) |
|---|---|---|---|
| Age (years) | 15–20 | 68 | 19.4 |
| 21–25 | 128 | 36.6 | |
| 26–30 | 95 | 27.1 | |
| >30 | 59 | 16.9 | |
| Gender | Male | 10 | 2.9 |
| Female | 340 | 97.1 | |
| Religion | Christian | 111 | 31.7 |
| Muslim | 239 | 68.3 | |
| Relationship | Mother | 324 | 92.6 |
| Father | 10 | 2.9 | |
| Others a | 16 | 4.6 | |
| Children under-5 | =1 | 218 | 62.3 |
| ≥2 | 132 | 37.8 | |
| Other children above-5 | =0 | 159 | 45.4 |
| ≥1 | 191 | 54.6 | |
| District | Urban | 173 | 49.4 |
| Rural | 177 | 50.6 | |
| Marital status | Single | 68 | 19.4 |
| Married | 245 | 70.0 | |
| Consensual union | 37 | 10.6 | |
| Education | None | 95 | 27.1 |
| Primary b | 30 | 8.6 | |
| Secondary c | 198 | 56.6 | |
| University | 27 | 7.7 | |
| Occupational status | Unemployed | 162 | 46.3 |
| Employed | 155 | 44.3 | |
| Student | 33 | 9.4 |
| Variables | Spearman Rank Test | Univariate Logistic Regression Analysis | ||
|---|---|---|---|---|
| rs | p | OR (95% CI) | p | |
| Knowledge-Attitudes | 0.13 | 0.019 * | 1.98 (1.21–3.25) | 0.007 ** |
| Knowledge-Practices | 0.05 | 0.333 | 1.19 (0.74–1.90) | 0.476 |
| Attitudes-Practices | 0.45 | 0.000 *** | 7.91 (4.33–15.54) | 0.000 *** |
| Variables | Knowledge | Attitudes | Practices | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Age (Years) (Group Age of 15–20 as the reference) | ||||||
| 21–25 | 1.31 (0.71–2.42) | 0.384 | 0.39 (0.19–0.76) | 0.007 ** | 0.90 (0.49–1.63) | 0.715 |
| 26–30 | 1.73 (1.25–8.11) | 0.107 | 1.04 (0.47–2.24) | 0.927 | 1.00 (0.54–1.88) | 0.991 |
| >30 | 3.03 (1.35–7.28) | 0.009 ** | 0.83 (0.36–1.94) | 0.670 | 1.00 (0.49–2.02) | 0.995 |
| Gender (Male as the reference) | ||||||
| Female | - | - | 2.66 (0.72–9.75) | 0.129 | 7.11 (1.11–111.28) | 0.064 |
| Religion (Group Muslim as the reference) | ||||||
| Christian | 2.20 (1.29–3.86) | 0.005 ** | 1.63 (0.97–2.80) | 0.072 | 0.73 (0.46–1.15) | 0.173 |
| Relationship (Mother as the reference) | ||||||
| Father | - | - | 0.36 (0.10–1.33) | 0.114 | 0.14 (0.01–0.74) | 0.061 |
| Others | 1.91 (0.60–8.45) | 0.322 | 0.47 (0.17–1.34) | 0.140 | 0.56 (0.17–1.58) | 0.294 |
| Children under-5 (Group having 1 child under-5 as the reference) | ||||||
| ≥2 | 1.03 (0.64–1.66) | 0.909 | 1.06 (0.66–1.73) | 0.814 | 1.49 (0.96–2.31) | 0.074 |
| Children above-5 (Group having no child above-5 as the reference) | ||||||
| ≥1 | 0.83 (0.52–1.32) | 0.431 | 1.09 (0.68–1.74) | 0.723 | 1.13 (0.74–1.73) | 0.574 |
| District (Group Urban as the reference) | ||||||
| Rural | 1.15 (0.73–1.83) | 0.544 | 1.83 (1.14–2.96) | 0.012 * | 1.24 (0.81–1.90) | 0.317 |
| Marital status (Group Single as the reference) | ||||||
| Married | 0.70 (0.36–1.28) | 0.257 | 1.05 (0.57–1.89) | 0.869 | 0.87 (0.51–1.50) | 0.619 |
| Consensual union | 0.73 (0.30–1.82) | 0.488 | 0.72 (0.30–1.71) | 0.445 | 0.54 (0.23–1.23) | 0.149 |
| Education (Group No education as the reference) | ||||||
| Primary | 1.10 (0.48–2.64) | 0.823 | 2.23 (0.87–6.50) | 0.112 | 0.68 (0.29–1.55) | 0.366 |
| Secondary | 1.94 (1.15–3.28) | 0.013 * | 1.45 (0.86–2.44) | 0.164 | 0.71 (0.43–1.16) | 0.167 |
| University | 2.81 (1.04–8.96) | 0.055 | 4.46 (1.42–19.73) | 0.021 * | 0.70 (0.29–1.66) | 0.424 |
| Occupational status (Group Unemployed as the reference) | ||||||
| Employed | 1.56 (0.97–2.54) | 0.071 | 0.97 (0.59–1.59) | 0.908 | 1.14 (0.73–1.78) | 0.556 |
| Student | 3.04 (1.20–9.33) | 0.030 * | 0.75 (0.34–1.71) | 0.474 | 0.22 (0.07–0.56) | 0.003 ** |
| KAPs | Variables | OR (95% CI) | p |
|---|---|---|---|
| Knowledge | Age (Years) (Group Age of 15–20 as the reference) | ||
| 21–25 | 1.44 (0.74–2.80) | 0.277 | |
| 26–30 | 2.14 (1.02–4.55) | 0.046 * | |
| >30 | 4.83 (1.95–12.69) | 0.001 *** | |
| Religion (Group Muslim as the reference) | |||
| Christian | 2.28 (1.30–4.14) | 0.005 ** | |
| Education (Group No education as the reference) | |||
| Primary | 0.99 (0.41–2.45) | 0.978 | |
| Secondary | 2.34 (1.32–4.19) | 0.004 ** | |
| University | 1.55 (0.53–5.25) | 0.445 | |
| Occupation status (Group Unemployed as the reference) | |||
| Employed | 1.26 (0.75–2.12) | 0.391 | |
| Student | 2.98 (1.12–9.48) | 0.041 * | |
| Attitudes | Age (Years) (Group Age of 15–20 as the reference) | ||
| 21–25 | 0.40 (0.19–0.79) | 0.01 ** | |
| 26–30 | 1.03 (0.45–2.32) | 0.94 | |
| >30 | 1.12 (0.44–2.89) | 0.814 | |
| District (Group Urban as the reference) | |||
| Rural | 1.97 (1.20–3.28) | 0.008 ** | |
| Education (Group No education as the reference) | |||
| Primary | 2.26 (0.83–7.08) | 0.132 | |
| Secondary | 1.86 (1.05–3.30) | 0.034 * | |
| University | 5.53 (1.67–25.54) | 0.011 * | |
| Relationship (Mother as the reference) | |||
| Father | 0.19 (0.04–0.80) | 0.022 * | |
| Others | 0.48 (0.16–1.47) | 0.187 | |
| Practices | Relationship (Mother as the reference) | ||
| Father | 0.11 (0.01–0.60) | 0.037 * | |
| Others | 0.60 (0.17–1.88) | 0.396 | |
| Religion (Group Muslim as the reference) | |||
| Christian | 0.64 (0.39–1.06) | 0.083 | |
| Occupational status (Group Unemployed as the reference) | |||
| Employed | 1.44 (0.90–2.30) | 0.127 | |
| Student | 0.22 (0.07–0.59) | 0.005 ** | |
| Marital status (Group Single as the reference) | |||
| Married | 0.53 (0.28–0.97) | 0.043 * | |
| Consensual union | 0.37 (0.15–0.89) | 0.029 * | |
| Children under-5 (Group having 1 child under-5 as the reference) | |||
| ≥2 | 1.46 (0.92–2.34) | 0.109 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koroma, J.M.; Wang, Y.; Guo, X.; Zhang, X.; Ngobeh, J.J.K.; Gabir, A.M.E.A.; Li, Z.; Li, L.; Wu, R.; Zhou, X. A Cross-Sectional Survey on the Malaria Control and Prevention Knowledge, Attitudes, and Practices of Caregivers of Children Under-5 in the Western Area of Sierra Leone. Trop. Med. Infect. Dis. 2022, 7, 120. https://doi.org/10.3390/tropicalmed7070120
Koroma JM, Wang Y, Guo X, Zhang X, Ngobeh JJK, Gabir AMEA, Li Z, Li L, Wu R, Zhou X. A Cross-Sectional Survey on the Malaria Control and Prevention Knowledge, Attitudes, and Practices of Caregivers of Children Under-5 in the Western Area of Sierra Leone. Tropical Medicine and Infectious Disease. 2022; 7(7):120. https://doi.org/10.3390/tropicalmed7070120
Chicago/Turabian StyleKoroma, Joan Mabinty, Yuji Wang, Xiang Guo, Xiaoqing Zhang, Jone Jama Kpanda Ngobeh, Ahmed Mohamed Elamin Ali Gabir, Ziyao Li, Li Li, Rangke Wu, and Xiaohong Zhou. 2022. "A Cross-Sectional Survey on the Malaria Control and Prevention Knowledge, Attitudes, and Practices of Caregivers of Children Under-5 in the Western Area of Sierra Leone" Tropical Medicine and Infectious Disease 7, no. 7: 120. https://doi.org/10.3390/tropicalmed7070120
APA StyleKoroma, J. M., Wang, Y., Guo, X., Zhang, X., Ngobeh, J. J. K., Gabir, A. M. E. A., Li, Z., Li, L., Wu, R., & Zhou, X. (2022). A Cross-Sectional Survey on the Malaria Control and Prevention Knowledge, Attitudes, and Practices of Caregivers of Children Under-5 in the Western Area of Sierra Leone. Tropical Medicine and Infectious Disease, 7(7), 120. https://doi.org/10.3390/tropicalmed7070120