
Strongyloides stercoralis: A Neglected but Fatal Parasite

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
3. Epidemiology
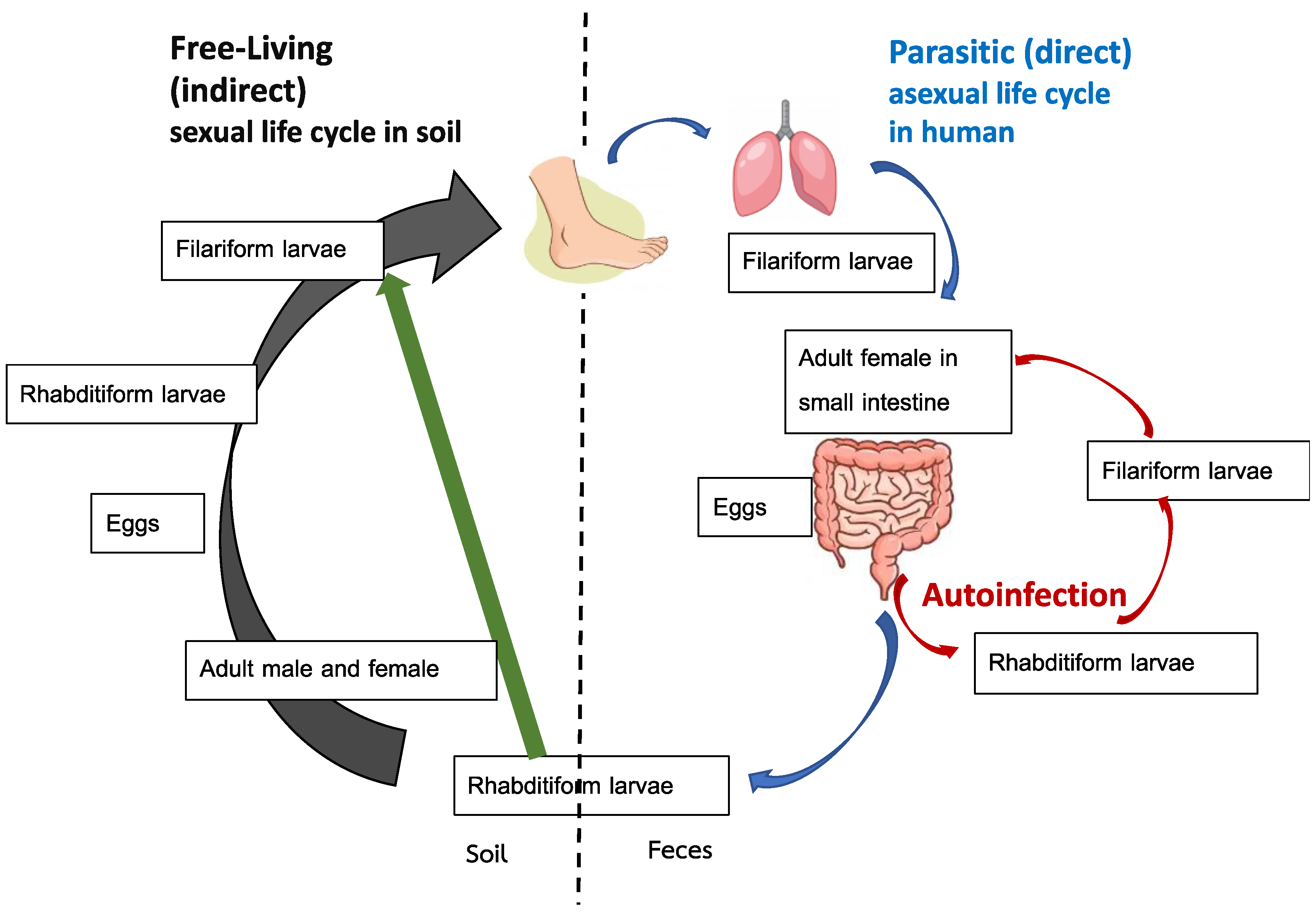
4. Life Cycle
5. Laboratory Diagnosis
6. Clinical Syndromes
6.1. Acute Strongyloidiasis
6.2. Chronic Strongyloidiasis
6.3. Hyperinfection Syndrome
6.4. Disseminated Infection
7. Strongyloidiasis in Immunocompromised Patients
8. Management
8.1. Management of Uncomplicated Strongyloidiasis
8.2. Management of Complicated Strongyloidiasis
8.3. Follow-Up after Treatment
9. Screening and Prevention
10. Strongyloidiasis and COVID-19
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schär, F.; Trostdorf, U.; Giardina, F.; Khieu, V.; Muth, S.; Marti, H.; Vounatsou, P.; Odermatt, P. Strongyloides stercoralis: Global Distribution and Risk Factors. PLoS Negl. Trop. Dis. 2013, 7, e2288. [Google Scholar] [CrossRef] [PubMed]
- Tamarozzi, F.; Martello, E.; Giorli, G.; Fittipaldo, A.; Staffolani, S.; Montresor, A.; Bisoffi, Z.; Buonfrate, D. Morbidity Associated with Chronic Strongyloides stercoralis Infection: A Systematic Review and Meta-Analysis. Am. J. Trop. Med. Hyg. 2019, 100, 1305–1311. [Google Scholar] [CrossRef]
- Bisoffi, Z.; Buonfrate, D.; Montresor, A.; Requena-Méndez, A.; Muñoz, J.; Krolewiecki, A.J.; Gotuzzo, E.; Mena, M.A.; Chiodini, P.L.; Anselmi, M.; et al. Strongyloides stercoralis: A plea for action. PLoS Negl. Trop. Dis. 2013, 7, e2214. [Google Scholar] [CrossRef]
- Keiser, P.B.; Nutman, T.B. Strongyloides stercoralis in the Immunocompromised Population. Clin. Microbiol. Rev. 2004, 17, 208–217. [Google Scholar] [CrossRef]
- Caumes, E.; Keystone, J.S. Acute strongyloidiasis: A rarity. Chronic strongyloidiasis: A time bomb! J. Travel Med. 2011, 18, 71–72. [Google Scholar] [CrossRef]
- Krolewiecki, A.; Nutman, T.B. Strongyloidiasis: A Neglected Tropical Disease. Infect. Dis. Clin. North Am. 2019, 33, 135–151. [Google Scholar] [CrossRef] [PubMed]
- Montes, M.; Sawhney, C.; Barros, N. Strongyloides stercoralis: There but not seen. Curr. Opin. Infect. Dis. 2010, 23, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Asundi, A.; Beliavsky, A.; Liu, X.J.; Akaberi, A.; Schwarzer, G.; Bisoffi, Z.; Requena-Méndez, A.; Shrier, I.; Greenaway, C. Prevalence of strongyloidiasis and schistosomiasis among migrants: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e236–e248. [Google Scholar] [CrossRef]
- Genta, R.M. Global prevalence of strongyloidiasis: Critical review with epidemiologic insights into the prevention of disseminated disease. Rev. Infect. Dis. 1989, 11, 755–767. [Google Scholar] [CrossRef] [PubMed]
- Buonfrate, D.; Bisanzio, D.; Giorli, G.; Odermatt, P.; Fürst, T.; Greenaway, C.; French, M.; Reithinger, R.; Gobbi, F.; Montresor, A.; et al. The Global Prevalence of Strongyloides stercoralis Infection. Pathogens 2020, 9, 468. [Google Scholar] [CrossRef] [PubMed]
- Román-Sánchez, P.; Pastor-Guzmán, A.; Moreno-Guillén, S.; Igual-Adell, R.; Suñer-Generoso, S.; Tornero-Estébanez, C. High prevalence of Strongyloides stercoralis among farm workers on the Mediterranean coast of Spain: Analysis of the predictive factors of infection in developed countries. Am. J. Trop. Med. Hyg. 2003, 69, 336–340. [Google Scholar] [CrossRef]
- Boggild, A.K.; Libman, M.; Greenaway, C.; McCarthy, A.E. CATMAT statement on disseminated strongyloidiasis: Prevention, assessment and management guidelines. Can. Commun. Dis. Rep. 2016, 42, 12–19. [Google Scholar] [CrossRef]
- Leung, E.; McIntyre, M.; Andany, N.; Ciccotelli, W.A.; Graham, C.; Jüni, P.; Langford, B.; McCarthy, A.E.; Nott, C.; Gold, W.L.; et al. Ivermectin to Prevent Disseminated Strongyloides Infection in Patients with COVID-19. Sci. Briefs Ont. COVID-19 Sci. Advis. Table 2021, 2, 1–7. [Google Scholar] [CrossRef]
- Ganesh, S.; Cruz, R.J., Jr. Strongyloidiasis: A multifaceted disease. Gastroenterol. Hepatol. 2011, 7, 194–196. [Google Scholar]
- Sing, A.; Leitritz, L.; Bogner, J.R.; Heesemann, J. First-glance diagnosis of Strongyloides stercoralis autoinfection by stool microscopy. J. Clin. Microbiol. 1999, 37, 1610–1611. [Google Scholar] [CrossRef]
- Luvira, V.; Watthanakulpanich, D.; Pittisuttithum, P. Management of Strongyloides stercoralis: A puzzling parasite. Int. Health 2014, 6, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, A.A.; Berk, S.L. Diagnosis of Strongyloides stercoralis infection. Clin. Infect. Dis. 2001, 33, 1040–1047. [Google Scholar] [CrossRef]
- Mendes, T.; Minori, K.; Ueta, M.; Miguel, D.C.; Allegretti, S.M. Strongyloidiasis Current Status with Emphasis in Diagnosis and Drug Research. J. Parasitol. Res. 2017, 2017, 5056314. [Google Scholar] [CrossRef] [PubMed]
- Requena-Méndez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Muñoz, J. The Laboratory Diagnosis and Follow Up of Strongyloidiasis: A Systematic Review. PLoS Negl. Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef] [PubMed]
- Roxby, A.C.; Gottlieb, G.S.; Limaye, A.P. Strongyloidiasis in transplant patients. Clin. Infect. Dis. 2009, 49, 1411–1423. [Google Scholar] [CrossRef]
- Hays, R.; Thompson, F.; Esterman, A.; McDermott, R. Strongyloides stercoralis, Eosinophilia, and Type 2 Diabetes Mellitus: The Predictive Value of Eosinophilia in the Diagnosis of S. stercoralis Infection in an Endemic Community. Open Forum Infect. Dis. 2016, 3, ofw029. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Pérez, A.; Soriano-Pérez, M.J.; Salvador, F.; Gomez-Junyent, J.; Villar-Garcia, J.; Santin, M.; Muñoz, C.; González-Cordón, A.; Salas-Coronas, J.; Sulleiro, E.; et al. Clinical Features Associated with Strongyloidiasis in Migrants and the Potential Impact of Immunosuppression: A Case Control Study. Pathogens 2020, 9, 507. [Google Scholar] [CrossRef] [PubMed]
- Loutfy, M.R.; Wilson, M.; Keystone, J.S.; Kain, K.C. Serology and eosinophil count in the diagnosis and management of strongyloidiasis in a non-endemic area. Am. J. Trop. Med. Hyg. 2002, 66, 749–752. [Google Scholar] [CrossRef] [PubMed]
- Vargas, P.; Krolewiecki, A.J.; Echazú, A.; Juarez, M.; Cajal, P.; Gil, J.F.; Caro, N.; Nasser, J.; Lammie, P.; Cimino, R.O. Serologic Monitoring of Public Health Interventions against Strongyloides stercoralis. Am. J. Trop. Med. Hyg. 2017, 97, 166–172. [Google Scholar] [CrossRef]
- Buonfrate, D.; Sequi, M.; Mejia, R.; Cimino, R.O.; Krolewiecki, A.J.; Albonico, M.; Degani, M.; Tais, S.; Angheben, A.; Requena-Mendez, A.; et al. Accuracy of Five Serologic Tests for the Follow up of Strongyloides stercoralis Infection. PLoS Negl. Trop. Dis. 2015, 9, e0003491. [Google Scholar] [CrossRef]
- Ramanathan, R.; Nutman, T. Strongyloides stercoralis infection in the immunocompromised host. Curr. Infect. Dis. Rep. 2008, 10, 105–110. [Google Scholar] [CrossRef]
- Luvira, V.; Trakulhun, K.; Mungthin, M.; Naaglor, T.; Chantawat, N.; Pakdee, W.; Phiboonbanakit, D.; Dekumyoy, P. Comparative Diagnosis of Strongyloidiasis in Immunocompromised Patients. Am. J. Trop. Med. Hyg. 2016, 95, 401–404. [Google Scholar] [CrossRef]
- Dekumyoy, P.; Somtana, K.; Jantanawiwat, P.; Nuamtanong, S.; Sa-nguankiat, S.; Nuchfaong, S.; Janyapoon, K.; Chindanond, D. Improved antigens for IgG-ELISA diagnosis of strongyloidiasis. Southeast Asian J. Trop. Med. Public Health 2002, 33 (Suppl. 3), 53–59. [Google Scholar]
- Yunus, M.H.; Arifin, N.; Balachandra, D.; Anuar, N.S.; Noordin, R. Lateral Flow Dipstick Test for Serodiagnosis of Strongyloidiasis. Am. J. Trop. Med. Hyg. 2019, 101, 432–435. [Google Scholar] [CrossRef]
- Sadaow, L.; Sanpool, O.; Rodpai, R.; Boonroumkaew, P.; Maleewong, W.; Intapan, P.M. Development of immunochromatographic device as a point-of-care tool for serodiagnosis of human strongyloidiasis cases. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 465–470. [Google Scholar] [CrossRef]
- Boonroumkaew, P.; Sadaow, L.; Sanpool, O.; Rodpai, R.; Thanchomnang, T.; Phupiewkham, W.; Intapan, P.M.; Maleewong, W. Effectiveness of Strongyloides Recombinant IgG Immunoreactive Antigen in Detecting IgG and IgG4 Subclass Antibodies for Diagnosis of Human Strongyloidiasis Using Rapid Immunochromatographic Tests. Diagnostics 2020, 10, 615. [Google Scholar] [CrossRef] [PubMed]
- Noordin, R.; Anuar, N.S.; Juri, N.M.; Wongphutorn, P.; Ruantip, S.; Kopolrat, K.Y.; Worasith, C.; Sithithaworn, J.; Sithithaworn, P. Evaluation of a Rapid IgG4 Lateral Flow Dipstick Test to Detect Strongyloides stercoralis Infection in Northeast Thailand. Am. J. Trop. Med. Hyg. 2021, 105, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Watts, M.R.; Kim, R.; Ahuja, V.; Robertson, G.J.; Sultana, Y.; Wehrhahn, M.C.; Bradbury, R.S.; Gilbert, G.L.; Lee, R.; Loeffelholz, M.J. Comparison of Loop-Mediated Isothermal Amplification and Real-Time PCR Assays for Detection of Strongyloides Larvae in Different Specimen Matrices. J. Clin. Microbiol. 2019, 57, e01173-18. [Google Scholar] [CrossRef] [PubMed]
- Robertson, G.J.; Koehler, A.V.; Gasser, R.B.; Watts, M.; Norton, R.; Bradbury, R.S. Application of PCR-Based Tools to Explore Strongyloides Infection in People in Parts of Northern Australia. Trop. Med. Infect. Dis. 2017, 2, 62. [Google Scholar] [CrossRef] [PubMed]
- Formenti, F.; La Marca, G.; Perandin, F.; Pajola, B.; Romano, M.; Santucci, B.; Silva, R.; Giorli, G.; Bisoffi, Z.; Buonfrate, D. A diagnostic study comparing conventional and real-time PCR for Strongyloides stercoralis on urine and on faecal samples. Acta Trop. 2019, 190, 284–287. [Google Scholar] [CrossRef]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Cinquini, M.; Cruciani, M.; Fittipaldo, A.; Giorli, G.; Gobbi, F.; Piubelli, C.; Bisoffi, Z. Accuracy of molecular biology techniques for the diagnosis of Strongyloides stercoralis infection-A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006229. [Google Scholar] [CrossRef]
- Pattison, D.A.; Speare, R. Strongyloidiasis in personnel of the Regional Assistance Mission to Solomon Islands (RAMSI). Med. J. Aust. 2008, 189, 203–206. [Google Scholar] [CrossRef]
- Greaves, D.; Coggle, S.; Pollard, C.; Aliyu, S.H.; Moore, E.M. Strongyloides stercoralis infection. BMJ 2013, 347, f4610. [Google Scholar] [CrossRef]
- Kling, K.; Kuenzli, E.; Blum, J.; Neumayr, A. Acute strongyloidiasis in a traveller returning from South East Asia. Travel Med. Infect. Dis. 2016, 14, 535–536. [Google Scholar] [CrossRef]
- Geri, G.; Rabbat, A.; Mayaux, J.; Zafrani, L.; Chalumeau-Lemoine, L.; Guidet, B.; Azoulay, E.; Pène, F. Strongyloides stercoralis hyperinfection syndrome: A case series and a review of the literature. Infection 2015, 43, 691–698. [Google Scholar] [CrossRef]
- Vasquez-Rios, G.; Pineda-Reyes, R.; Pineda-Reyes, J.; Marin, R.; Ruiz, E.F.; Terashima, A. Strongyloides stercoralis hyperinfection syndrome: A deeper understanding of a neglected disease. J. Parasit. Dis. 2019, 43, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Weiser, J.A.; Scully, B.E.; Bulman, W.A.; Husain, S.; Grossman, M.E. Periumbilical parasitic thumbprint purpura: Strongyloides hyperinfection syndrome acquired from a cadaveric renal transplant. Transpl. Infect. Dis. 2011, 13, 58–62. [Google Scholar] [CrossRef]
- Fardet, L.; Genereau, T.; Poirot, J.L.; Guidet, B.; Kettaneh, A.; Cabane, J. Severe strongyloidiasis in corticosteroid-treated patients: Case series and literature review. J. Infect. 2007, 54, 18–27. [Google Scholar] [CrossRef]
- Nabha, L.; Krishnan, S.; Ramanathan, R.; Mejia, R.; Roby, G.; Sheikh, V.; McAuliffe, I.; Nutman, T.; Sereti, I. Prevalence of Strongyloides stercoralis in an urban US AIDS cohort. Pathog. Glob. Health 2012, 106, 238–244. [Google Scholar] [CrossRef]
- Rafiei, R.; Rafiei, A.; Rahdar, M.; Keikhaie, B. Seroepidemiology of Strongyloides stercoralis amongst immunocompromised patients in Southwest Iran. Parasite Epidemiol. Control 2016, 1, 229–232. [Google Scholar] [CrossRef]
- Getaz, L.; Castro, R.; Zamora, P.; Kramer, M.; Gareca, N.; Torrico-Espinoza, M.D.C.; Macias, J.; Lisarazu-Velasquez, S.; Rodriguez, G.; Valencia-Rivero, C.; et al. Epidemiology of Strongyloides stercoralis infection in Bolivian patients at high risk of complications. PLoS Negl. Trop. Dis. 2019, 13, e0007028. [Google Scholar] [CrossRef]
- Winnicki, W.; Eder, M.; Mazal, P.; Mayer, F.J.; Sengölge, G.; Wagner, L. Prevalence of Strongyloides stercoralis infection and hyperinfection syndrome among renal allograft recipients in Central Europe. Sci. Rep. 2018, 8, 15406. [Google Scholar] [CrossRef]
- Abanyie, F.A.; Gray, E.B.; Delli Carpini, K.W.; Yanofsky, A.; McAuliffe, I.; Rana, M.; Chin-Hong, P.V.; Barone, C.N.; Davis, J.L.; Montgomery, S.P.; et al. Donor-derived Strongyloides stercoralis infection in solid organ transplant recipients in the United States, 2009-2013. Am. J. Transplant. 2015, 15, 1369–1375. [Google Scholar] [CrossRef]
- Hoy, W.E.; Roberts, N.J., Jr.; Bryson, M.F.; Bowles, C.; Lee, J.C.K.; Rivero, A.J.; Ritterson, A.L. Transmission of Strongyloidiasis by Kidney Transplant?: Disseminated Strongyloidiasis in Both Recipients of Kidney Allografts From a Single Cadaver Donor. JAMA 1981, 246, 1937–1939. [Google Scholar] [CrossRef]
- Schad, G.A. Cyclosporine may eliminate the threat of overwhelming strongyloidiasis in immunosuppressed patients. J. Infect. Dis. 1986, 153, 178. [Google Scholar] [CrossRef]
- Schwartz, B.S.; Mawhorter, S.D. Parasitic infections in solid organ transplantation. Am. J. Transplant. 2013, 13 (Suppl. 4), 280–303. [Google Scholar] [CrossRef]
- Marcos, L.A.; Terashima, A.; Canales, M.; Gotuzzo, E. Update on strongyloidiasis in the immunocompromised host. Curr. Infect. Dis. Rep. 2011, 13, 35–46. [Google Scholar] [CrossRef]
- Pungpak, S.; Bunnag, D.; Chindanond, D.; Radmoyos, B. Albendazole in the treatment of strongyloidiasis. Southeast Asian J. Trop. Med. Public Health 1987, 18, 207–210. [Google Scholar]
- Archibald, L.K.; Beeching, N.J.; Gill, G.V.; Bailey, J.W.; Bell, D.R. Albendazole is effective treatment for chronic strongyloidiasis. Q. J. Med. 1993, 86, 191–195. [Google Scholar]
- Pitisuttithum, P.; Supanaranond, W.; Chindanond, D. A randomized comparative study of albendazole and thiabendazole in chronic strongyloidiasis. Southeast Asian J. Trop. Med. Public Health 1995, 26, 735–738. [Google Scholar]
- Shikiya, K.; Zaha, O.; Niimura, S.; Uehara, T.; Ohshiro, J.; Kinjo, F.; Saito, A.; Asato, R. Clinical study on ivermectin against 125 strongyloidiasis patients. Kansenshogaku Zasshi 1994, 68, 13–20. [Google Scholar] [CrossRef]
- Datry, A.; Hilmarsdottir, I.; Mayorga-Sagastume, R.; Lyagoubi, M.; Gaxotte, P.; Biligui, S.; Chodakewitz, J.; Neu, D.; Danis, M.; Gentilini, M. Treatment of Strongyloides stercoralis infection with ivermectin compared with albendazole: Results of an open study of 60 cases. Trans. R Soc. Trop. Med. Hyg. 1994, 88, 344–345. [Google Scholar] [CrossRef]
- Gann, P.H.; Neva, F.A.; Gam, A.A. A randomized trial of single- and two-dose ivermectin versus thiabendazole for treatment of strongyloidiasis. J. Infect. Dis. 1994, 169, 1076–1079. [Google Scholar] [CrossRef]
- Toma, H.; Sato, Y.; Shiroma, Y.; Kobayashi, J.; Shimabukuro, I.; Takara, M. Comparative studies on the efficacy of three anthelminthics on treatment of human strongyloidiasis in Okinawa, Japan. Southeast Asian J. Trop. Med. Public Health 2000, 31, 147–151. [Google Scholar]
- Igual-Adell, R.; Oltra-Alcaraz, C.; Soler-Company, E.; Sanchez-Sanchez, P.; Matogo-Oyana, J.; Rodriguez-Calabuig, D. Efficacy and safety of ivermectin and thiabendazole in the treatment of strongyloidiasis. Expert Opin. Pharmacother. 2004, 5, 2615–2619. [Google Scholar] [CrossRef]
- Suputtamongkol, Y.; Kungpanichkul, N.; Silpasakorn, S.; Beeching, N.J. Efficacy and safety of a single-dose veterinary preparation of ivermectin versus 7-day high-dose albendazole for chronic strongyloidiasis. Int. J. Antimicrob. Agents 2008, 31, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Bisoffi, Z.; Buonfrate, D.; Angheben, A.; Boscolo, M.; Anselmi, M.; Marocco, S.; Monteiro, G.; Gobbo, M.; Bisoffi, G.; Gobbi, F. Randomized clinical trial on ivermectin versus thiabendazole for the treatment of strongyloidiasis. PLoS Negl. Trop. Dis. 2011, 5, e1254. [Google Scholar] [CrossRef] [PubMed]
- Suputtamongkol, Y.; Premasathian, N.; Bhumimuang, K.; Waywa, D.; Nilganuwong, S.; Karuphong, E.; Anekthananon, T.; Wanachiwanawin, D.; Silpasakorn, S. Efficacy and safety of single and double doses of ivermectin versus 7-day high dose albendazole for chronic strongyloidiasis. PLoS Negl. Trop. Dis. 2011, 5, e1044. [Google Scholar] [CrossRef]
- Barda, B.; Sayasone, S.; Phongluxa, K.; Xayavong, S.; Keoduangsy, K.; Odermatt, P.; Puchkov, M.; Huwyler, J.; Hattendorf, J.; Keiser, J. Efficacy of Moxidectin Versus Ivermectin Against Strongyloides stercoralis Infections: A Randomized, Controlled Noninferiority Trial. Clin. Infect. Dis. 2017, 65, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Buonfrate, D.; Salas-Coronas, J.; Munoz, J.; Maruri, B.T.; Rodari, P.; Castelli, F.; Zammarchi, L.; Bianchi, L.; Gobbi, F.; Cabezas-Fernandez, T.; et al. Multiple-dose versus single-dose ivermectin for Strongyloides stercoralis infection (Strong Treat 1 to 4): A multicentre, open-label, phase 3, randomised controlled superiority trial. Lancet Infect. Dis. 2019, 19, 1181–1190. [Google Scholar] [CrossRef]
- Hofmann, D.; Sayasone, S.; Sengngam, K.; Chongvilay, B.; Hattendorf, J.; Keiser, J. Efficacy and safety of ascending doses of moxidectin against Strongyloides stercoralis infections in adults: A randomised, parallel-group, single-blinded, placebo-controlled, dose-ranging, phase 2a trial. Lancet Infect. Dis. 2021, 21, 1151–1160. [Google Scholar] [CrossRef]
- Prichard, R.K.; Geary, T.G. Perspectives on the utility of moxidectin for the control of parasitic nematodes in the face of developing anthelmintic resistance. Int. J. Parasitol. Drugs Drug Resist. 2019, 10, 69–83. [Google Scholar] [CrossRef]
- Buonfrate, D.; Requena-Mendez, A.; Angheben, A.; Munoz, J.; Gobbi, F.; Van Den Ende, J.; Bisoffi, Z. Severe strongyloidiasis: A systematic review of case reports. BMC Infect. Dis. 2013, 13, 78. [Google Scholar] [CrossRef]
- Mejia, R.; Nutman, T.B. Screening, prevention, and treatment for hyperinfection syndrome and disseminated infections caused by Strongyloides stercoralis. Curr. Opin. Infect. Dis. 2012, 25, 458–463. [Google Scholar] [CrossRef]
- Hamilton, K.W.; Abt, P.L.; Rosenbach, M.A.; Bleicher, M.B.; Levine, M.S.; Mehta, J.; Montgomery, S.P.; Hasz, R.D.; Bono, B.R.; Tetzlaff, M.T.; et al. Donor-derived Strongyloides stercoralis infections in renal transplant recipients. Transplantation 2011, 91, 1019–1024. [Google Scholar] [CrossRef]
- Barrett, J.; Broderick, C.; Soulsby, H.; Wade, P.; Newsholme, W. Subcutaneous ivermectin use in the treatment of severe Strongyloides stercoralis infection: Two case reports and a discussion of the literature. J. Antimicrob. Chemother. 2016, 71, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Turner, S.A.; Maclean, J.D.; Fleckenstein, L.; Greenaway, C. Parenteral administration of ivermectin in a patient with disseminated strongyloidiasis. Am. J. Trop. Med. Hyg. 2005, 73, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Donadello, K.; Cristallini, S.; Taccone, F.S.; Lorent, S.; Vincent, J.L.; de Backer, D.; Jacobs, F. Strongyloides disseminated infection successfully treated with parenteral ivermectin: Case report with drug concentration measurements and review of the literature. Int. J. Antimicrob. Agents 2013, 42, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Sithithaworn, P.; Srisawangwong, T.; Tesana, S.; Daenseekaew, W.; Sithithaworn, J.; Fujimaki, Y.; Ando, K. Epidemiology of Strongyloides stercoralis in north-east Thailand: Application of the agar plate culture technique compared with the enzyme-linked immunosorbent assay. Trans. R Soc. Trop. Med. Hyg. 2003, 97, 398–402. [Google Scholar] [CrossRef]
- Carnino, L.; Schwob, J.-M.; Gétaz, L.; Nickel, B.; Neumayr, A.; Eperon, G. A Practical Approach to Screening for Strongyloides stercoralis. Trop. Med. Infect. Dis. 2021, 6, 203. [Google Scholar] [CrossRef]
- Requena-Méndez, A.; Buonfrate, D.; Gomez-Junyent, J.; Zammarchi, L.; Bisoffi, Z.; Muñoz, J. Evidence-Based Guidelines for Screening and Management of Strongyloidiasis in Non-Endemic Countries. Am. J. Trop. Med. Hyg. 2017, 97, 645–652. [Google Scholar] [CrossRef]
- Gómez-Junyent, J.; Paredes, D.; Hurtado, J.C.; Requena-Méndez, A.; Ruiz, A.; Valls, M.E.; Vila, J.; Muñoz, J. High seroprevalence of Strongyloides stercoralis among individuals from endemic areas considered for solid organ transplant donation: A retrospective serum-bank based study. PLoS Negl. Trop. Dis. 2018, 12, e0007010. [Google Scholar] [CrossRef]
- Pierrotti, L.C.; Kotton, C.N. Transplantation in the Tropics: Lessons on Prevention and Management of Tropical Infectious Diseases. Curr. Infect. Dis. Rep. 2015, 17, 34. [Google Scholar] [CrossRef]
- Santiago, M.; Leitao, B. Prevention of Strongyloides hyperinfection syndrome: A rheumatological point of view. Eur. J. Intern. Med. 2009, 20, 744–748. [Google Scholar] [CrossRef]
- Hayes, J.; Nellore, A. Management of Strongyloides in Solid Organ Transplant Recipients. Infect. Dis. Clin. North Am. 2018, 32, 749–763. [Google Scholar] [CrossRef]
- Forrer, A.; Khieu, V.; Schindler, C.; Schär, F.; Marti, H.; Char, M.C.; Muth, S.; Odermatt, P. Ivermectin Treatment and Sanitation Effectively Reduce Strongyloides stercoralis Infection Risk in Rural Communities in Cambodia. PLoS Negl. Trop. Dis. 2016, 10, e0004909. [Google Scholar] [CrossRef] [PubMed]
- Hays, R.; Esterman, A.; McDermott, R. Control of chronic Strongyloides stercoralis infection in an endemic community may be possible by pharmacological means alone: Results of a three-year cohort study. PLoS Negl. Trop. Dis. 2017, 11, e0005825. [Google Scholar] [CrossRef] [PubMed]
- Barda, B.; Albonico, M.; Buonfrate, D.; Ame, S.M.; Ali, S.; Speich, B.; Keiser, J. Side Benefits of Mass Drug Administration for Lymphatic Filariasis on Strongyloides stercoralis Prevalence on Pemba Island, Tanzania. Am. J. Trop. Med. Hyg. 2017, 97, 681–683. [Google Scholar] [CrossRef] [PubMed]
- Kearns, T.M.; Currie, B.J.; Cheng, A.C.; McCarthy, J.; Carapetis, J.R.; Holt, D.C.; Page, W.; Shield, J.; Gundjirryirr, R.; Mulholland, E.; et al. Strongyloides seroprevalence before and after an ivermectin mass drug administration in a remote Australian Aboriginal community. PLoS Negl. Trop. Dis. 2017, 11, e0005607. [Google Scholar] [CrossRef]
- Group, R.C.; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Pereira, C.V.M.; Mastandrea, G.R.A.; Medeiros, A.C.C.d.S.; Gryschek, R.C.B.; Paula, F.M.d.; Corral, M.A. COVID-19 and strongyloidiasis: What to expect from this coinfection? Clinics (Sao Paulo) 2021, 76, e3528. [Google Scholar] [CrossRef]
- Stauffer, W.M.; Alpern, J.D.; Walker, P.F. COVID-19 and Dexamethasone: A Potential Strategy to Avoid Steroid-Related Strongyloides Hyperinfection. JAMA 2020, 324, 623–624. [Google Scholar] [CrossRef]
- Feria, L.; Torrado, M.; Anton-Vazquez, V. Reactivation of Strongyloides stercoralis in patients with SARS-CoV-2 pneumonia receiving dexamethasone. Med. Clin. (Barc) 2022, 158, 242–243. [Google Scholar] [CrossRef]
- Gautam, D.; Gupta, A.; Meher, A.; Siddiqui, F.; Singhai, A. Corticosteroids in Covid-19 pandemic have the potential to unearth hidden burden of strongyloidiasis. IDCases 2021, 25, e01192. [Google Scholar] [CrossRef]
- Lier, A.J.; Tuan, J.J.; Davis, M.W.; Paulson, N.; McManus, D.; Campbell, S.; Peaper, D.R.; Topal, J.E. Case Report: Disseminated Strongyloidiasis in a Patient with COVID-19. Am. J. Trop. Med. Hyg. 2020, 103, 1590–1592. [Google Scholar] [CrossRef]
- Marchese, V.; Crosato, V.; Gulletta, M.; Castelnuovo, F.; Cristini, G.; Matteelli, A.; Castelli, F. Strongyloides infection manifested during immunosuppressive therapy for SARS-CoV-2 pneumonia. Infection 2021, 49, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Pintos-Pascual, I.; López-Dosil, M.; Castillo-Núñez, C.; Múñez-Rubio, E. Eosinophilia and abdominal pain after severe pneumonia due to COVID 19. Enferm. Infecc. Microbiol. Clin. (Engl. Ed.) 2021, 39, 478–480. [Google Scholar] [CrossRef] [PubMed]
- De Wilton, A.; Nabarro, L.E.; Godbole, G.S.; Chiodini, P.L.; Boyd, A.; Woods, K. Risk of Strongyloides Hyperinfection Syndrome when prescribing dexamethasone in severe COVID-19. Travel Med. Infect. Dis. 2021, 40, 101981. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Advantages | Disadvantages |
|---|---|---|
| Stool concentration | -Practical in clinical setting -Able to detect other parasites | -Variation in sensitivity (operator dependent) |
| Baermann funnel | -Quantify parasite burden and suitability for low parasite load | -Requires large amount of stool |
| Stool culture | -High sensitivity | -Cannot detect other parasites -Requires fresh stool, time consuming -Limited availability |
| Serology | -More sensitive than fecal-based methods, suitable for screening and diagnosis based on well-prepared antigens -Can be used in both endemic area residents and immigrants -Screening prior to immunosuppressive treatment -Seroepidemiological studies -Use in follow-up studies (decrease 6–12 months after treatment) | -Low sensitivity in patients with impaired immunity and low immune response -Limited specificity for cross-reactivity with other helminth infections (such as filariasis, ascariasis and schistosomiasis) based on antigen used and detected immunoglobulin |
| Molecular | -Applicable to other clinical specimens -High specificity (with limited sensitivity), suitable for confirmation tests | -Limited availability -Variation in sensitivity and specificity depending on techniques used |
| Study | Population | Study Design | Follow-Up Period | Regimens | Cure/Total N (%) | Remarks | |
|---|---|---|---|---|---|---|---|
| Pungpak S, et al., 1987 [53] | Thai adults without co-morbidity | Controlled trial, open label | 15, 30 days | Albendazole 400 mg/day for 3 days | 8/11 (72.2) | ||
| Albendazole 400 mg/day for 3 days with repeated regimen 1 week later | 19/19 (100) | ||||||
| Archibald LK, et al., 1993 [54] | British ex-Far East prisoners of World War II | Prospective cohort | 6–9 months, using stool tests and/or serology | Albendazole 400 mg twice daily for 3 days | 35/47 (75) | - | |
| Pitisuttithum P, et al., 1995 [55] | Thai adults without co-morbidity | RCT, open label | 3 weeks | Albendazole 400 mg twice daily for 5 days | 18/23 (94.7) | p = 0.183 | |
| Thiabendazole 1 g twice daily for 5 days | 12/12 (100.0) | ||||||
| Shikiya K, et al., 1994 [56] | Japanese patients | Prospective study | No data | Ivermectin 6 mg in 2 doses, 2 weeks interval | 108/125 (86.4) | - | |
| Datry A, et al., 1994 [57] | French adults without co-morbidity | RCT, open label | 3 months | Ivermectin 150–200 µg/kg, single dose | 24/29 (82.8) | p < 0.01 | |
| Albendazole 400 mg/day for 3 days | 9/24 (37.5) | ||||||
| Gann PH, et al., 1994 [58] | Southeast Asian refugees in the United States | RCT, open label | ≥3 months | Ivermectin 200 µg/kg, single dose | 16/16 (100) | - | |
| Ivermectin 200 µg/kg/day for 2 consecutive days | 17/18 (94.4) | ||||||
| Thiabendazole 50 mg/kg/day for 3 days | 18/19 (94.7) | ||||||
| Toma H, et al., 2000 [59] | Japanese adults, positive rate of HTLV-1 infection was 29.4% | Controlled trial, open label | 1 year | Pyrvinium pamoate 5 mg/kg/day for 3 days | 14/60 (23.3) | -p < 0.001; pyrvinium pamoate vs. albendazole -p < 0.001; albendazole vs. ivermectin -Significantly decreased cure rate in HTLV-1 infection subjects | |
| Albendazole, 400 mg/day for 3 days | 65/84 (77.4) | ||||||
| Ivermectin, 6 mg in a single dose | 65/67 (97.0) | ||||||
| Igual-Adell R, et al., 2004 [60] | Spanish adults | Retrospect-ive study | 3 months | Ivermectin 200 µg/kg, single dose | 17/22 (77.3) | - | |
| Ivermectin 200 µg/kg/day for 2 consecutive days | 35/35 (100) | ||||||
| Thiabendazole 50 mg/kg/day for 5 days | 25/31 (78) | ||||||
| Suputtamongkol Y, et al., 2008 [61] | Thai adult patients with concomitant medical illness | RCT, open label | 4 weeks | Veterinary (parenteral formulation) ivermectin 200 µg/kg, orally, single dose | 16/21 (76.2) | p = 0.029 | |
| Albendazole 800 mg/day for 7 days | 8/21 (38.1) | ||||||
| Bisoffi Z, et al., 2011 [62] | Italian and immigrant adults without co-morbidity | RCT, open label, phase III | 3–6 months, Using both stool tests and serology | Ivermectin 200 µg/kg, single dose | 60/106 (56.6) | p = 0.53 | |
| Thiabendazole 50 mg/kg/day for 2 days | 48/92 (52.2) | ||||||
| Suputtamongkol Y, et al., 2011 [63] | Thai adult patients with concomitant medical illness | RCT, open label | 1 year | Ivermectin 200 µg/kg, single dose | 30/31 (96.8) | p = 0.006; albendazole vs. ivermectin | |
| Ivermectin 200 µg/kg/day, two doses, given 2 weeks apart | 27/29 (93.1) | ||||||
| Albendazole 800 mg/day for 7 days | 19/30 (63.3) | ||||||
| Barda B, et al., 2017 [64] | Loa healthy people aged > 12 years | Non-inferior, RCT, single-blind, phase II | 21 days | Moxidectin 8 mg, single dose | 59/63 (93.7) | ||
| Ivermectin 200 µg/kg, single dose | 59/62 (95.2) | ||||||
| Buonfrate D, et al., 2019 [65] | European aged > 5 years and weight > 15 kg without immunosuppr-ession | Multileft, superior RCT, open label, phase III | 1 year using stool tests and/or serology | Ivermectin 200 µg/kg/day, 4 doses (day 1, 2, 15, 16) | 102/118 (86) | p = 0.75 Early terminated trial from futility | |
| Ivermectin 200 µg/kg, single dose | 96/113 (85) | ||||||
| Hofmann D, et al., 2021 [66] | Loa adult (aged 18–65 years) community members | Single-blinded, RCT, parallel-group, placebo-controlled, dose-ranging, phase 2a trial | 28 days after treatment | Cure/total N (%) | Predicted cure rate% (95% CI) | ||
| Moxidectin 2 mg, single dose | 22/30 (73) | 75% (59–87) | -Stratify participants based on baseline -S. stercoralis infection intensities: light, moderate, heavy | ||||
| Moxidectin 4 mg, single dose | 26/29 (90) | 83% (76–88) | |||||
| Moxidectin 6 mg, single dose | 27/32 (84) | 86% (79–90) | |||||
| Moxidectin 8 mg, single dose | 24/29 (83) | 87% (80–92) | |||||
| Moxidectin 10 mg, single dose | 29/30 (97) | 88% (80–93) | |||||
| Moxidectin 12 mg, single dose | 26/30 (87) | 88% (80–93) | |||||
| Placebo | 4/29 (14) | 14% (5–31) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luvira, V.; Siripoon, T.; Phiboonbanakit, D.; Somsri, K.; Watthanakulpanich, D.; Dekumyoy, P. Strongyloides stercoralis: A Neglected but Fatal Parasite. Trop. Med. Infect. Dis. 2022, 7, 310. https://doi.org/10.3390/tropicalmed7100310
Luvira V, Siripoon T, Phiboonbanakit D, Somsri K, Watthanakulpanich D, Dekumyoy P. Strongyloides stercoralis: A Neglected but Fatal Parasite. Tropical Medicine and Infectious Disease. 2022; 7(10):310. https://doi.org/10.3390/tropicalmed7100310
Chicago/Turabian StyleLuvira, Viravarn, Tanaya Siripoon, Danabhand Phiboonbanakit, Kollawat Somsri, Dorn Watthanakulpanich, and Paron Dekumyoy. 2022. "Strongyloides stercoralis: A Neglected but Fatal Parasite" Tropical Medicine and Infectious Disease 7, no. 10: 310. https://doi.org/10.3390/tropicalmed7100310
APA StyleLuvira, V., Siripoon, T., Phiboonbanakit, D., Somsri, K., Watthanakulpanich, D., & Dekumyoy, P. (2022). Strongyloides stercoralis: A Neglected but Fatal Parasite. Tropical Medicine and Infectious Disease, 7(10), 310. https://doi.org/10.3390/tropicalmed7100310