

Monkeypox Disease: An Emerging Public Health Concern in the Shadow of COVID-19 Pandemic: An Update


Abstract
1. Introduction
2. Taxonomy
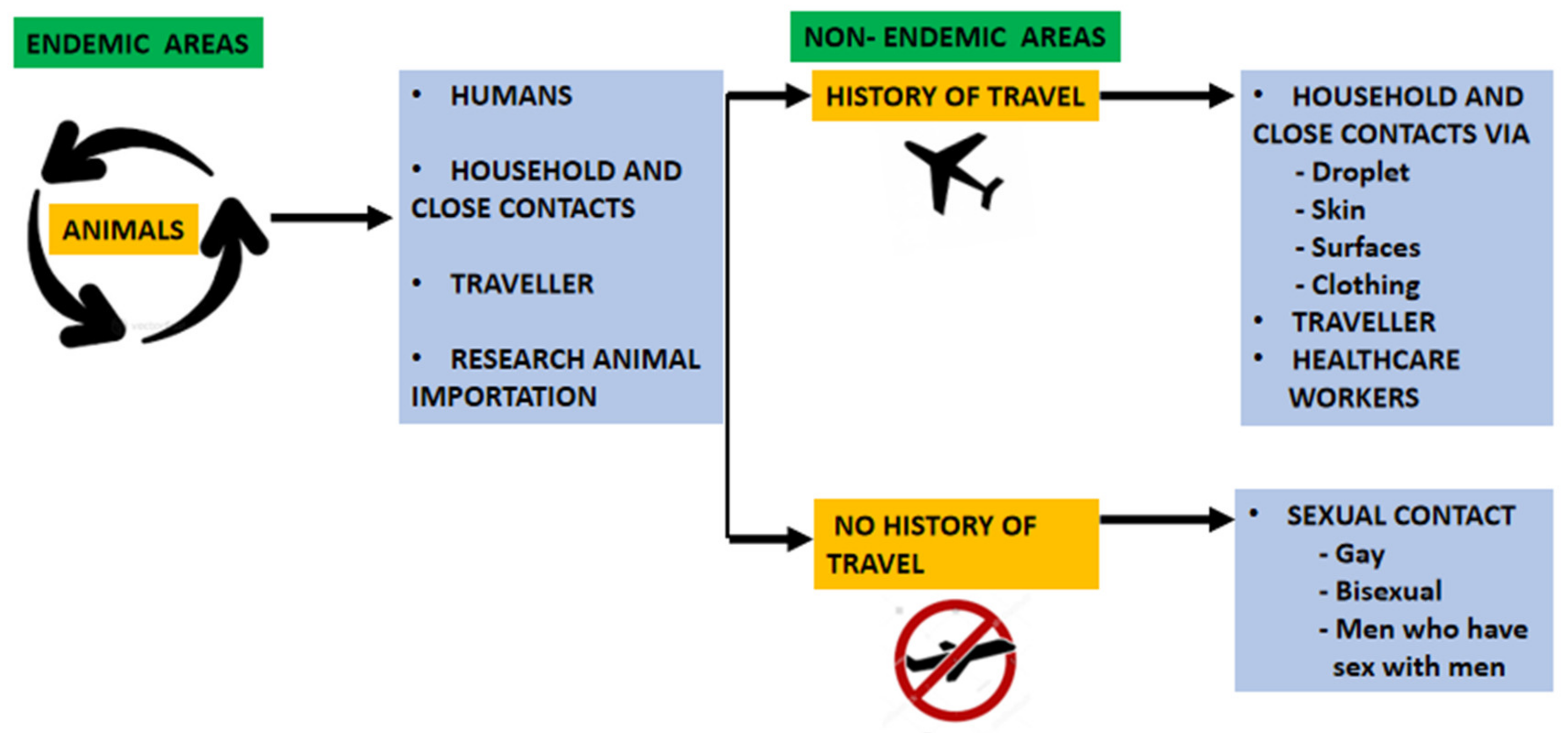
3. Transmission
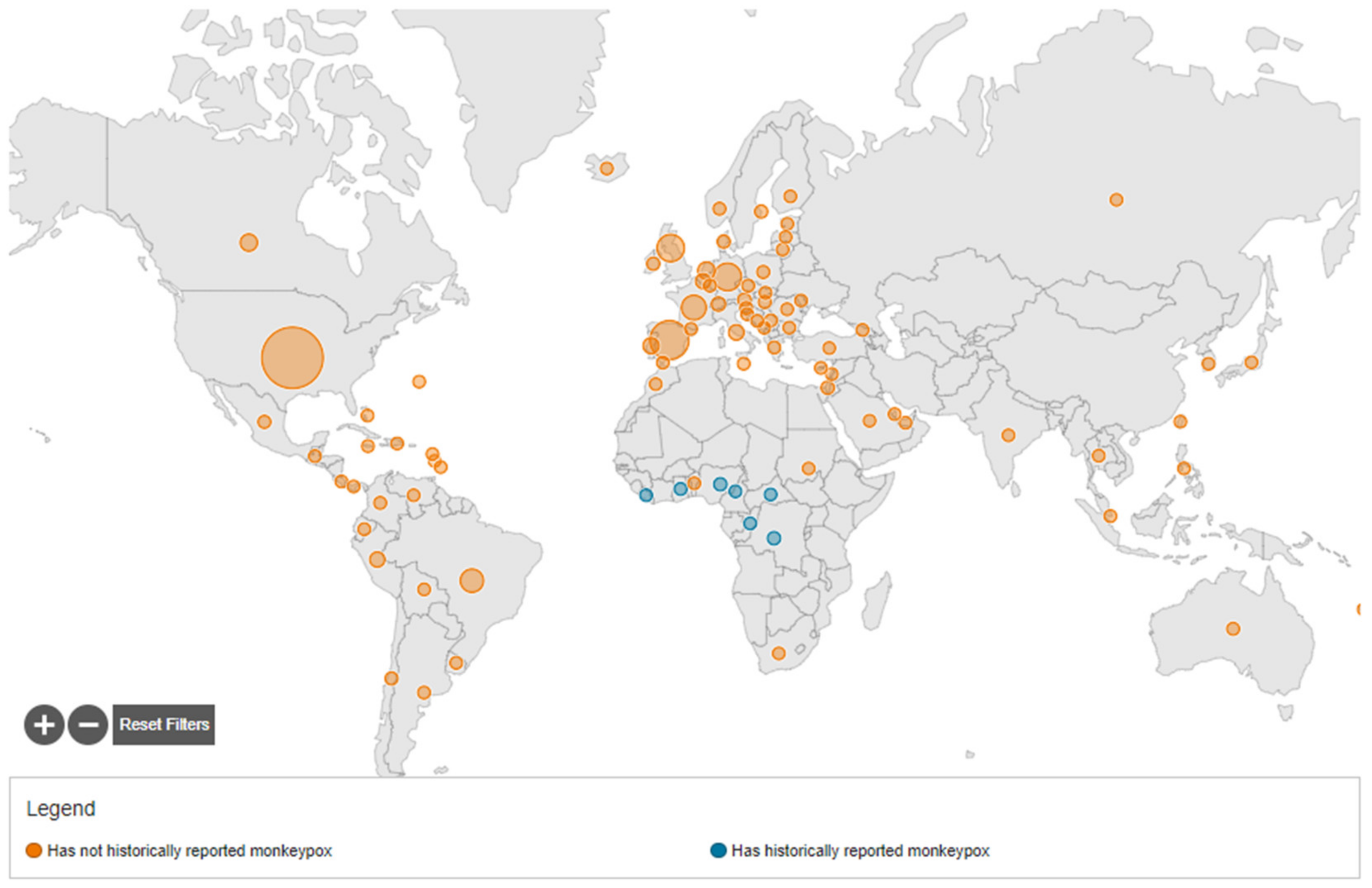
4. Epidemiology
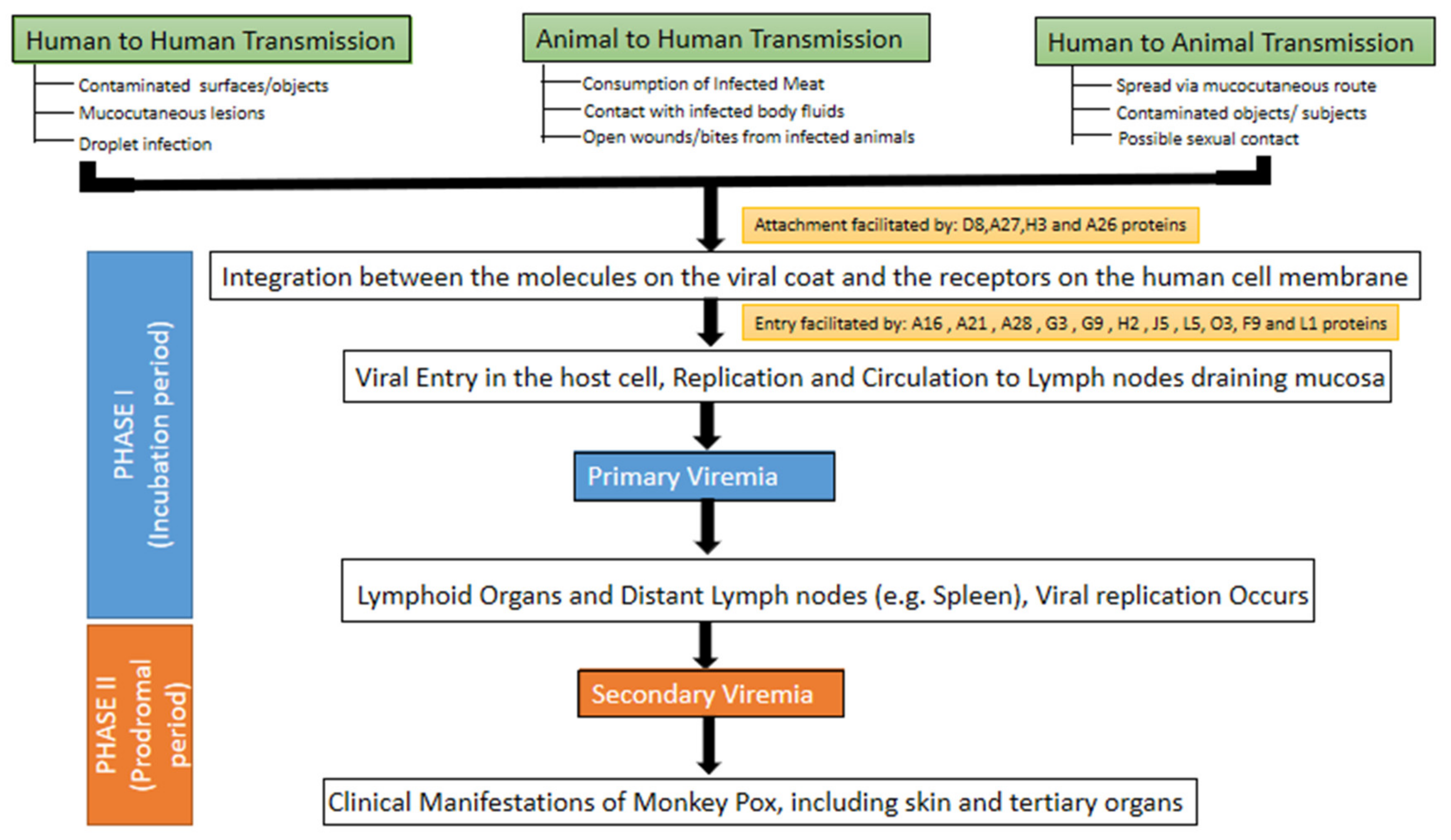
5. Pathogenesis
6. Clinical Features
7. Orofacial Features
8. Diagnosis
9. Differential Diagnosis
10. Prevention
11. Treatment
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, X.; Zhu, Z.; He, Y.; Lim, J.W.; Lane, B.; Wang, H.; Peng, Q.; Sun, L.; Lu, H. Monkeypox claims new victims: The outbreak in men who have sex with men. Infect. Dis. Poverty 2022, 11, 84. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.; White, A. Monkeypox virus emerges from the shadow of its more infamous cousin: Family biology matters. Emerg. Microbes Infect. 2022, 11, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Cheema, A.Y.; Ogedegbe, O.J.; Munir, M.; Alugba, G.; Ojo, T.K. Monkeypox: A Review of Clinical Features, Diagnosis, and Treatment. Cureus 2022, 14, e26756. [Google Scholar] [CrossRef] [PubMed]
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The changing epidemiology of human monkeypox—A potential threat? A systematic review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef]
- Heymann, D.L.; Simpson, K. The evolving epidemiology of human monkeypox: Questions still to be answered. J. Infect. Dis. 2021, 223, 1839–1841. [Google Scholar] [CrossRef]
- Adler, H.; Gould, S.; Hine, P.; Snell, L.B.; Wong, W.; Houlihan, C.F.; Osborne, J.C.; Rampling, T.; Beadsworth, M.B.J.; Duncan, C.J.; et al. Clinical features and management of human monkeypox: A retrospective observational study in the UK. Lancet Infect. Dis. 2022, 22, 1153–1162. [Google Scholar] [CrossRef]
- Patel, A.; Bilinska, J.; Tam, J.C.H.; Fontoura, D.D.S.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C.; et al. Clinical features and novel presentations of human monkeypox in a central London centre during the 2022 outbreak: Descriptive case series. BMJ 2022, 378, e072410. [Google Scholar] [CrossRef]
- Alshahrani, N.Z.; Alzahrani, F.; Alarifi, A.M.; Algethami, M.R.; Alhumam, M.N.; Ayied, H.A.M.; Awan, A.Z.; Almutairi, A.F.; Bamakhrama, S.A.; Almushari, B.S.; et al. Assessment of Knowledge of Monkeypox Viral Infection among the General Population in Saudi Arabia. Pathogens 2022, 11, 904. [Google Scholar] [CrossRef]
- Cabanillas, B.; Valdelvira, R.; Akdis, C.A. Monkeypox outbreak in Europe, UK, North America, and Australia: A changing trend of a zoonotic disease. Allergy 2022, 77, 2284–2286. [Google Scholar] [CrossRef]
- Nuzzo, J.B.; Borio, L.L.; Gostin, L.O. The WHO Declaration of Monkeypox as a Global Public Health Emergency. JAMA 2022, 328, 615–617. [Google Scholar] [CrossRef]
- Pittman, P.R.; Martin, J.W.; Kingebeni, P.M.; Tamfum, J.-J.M.; Wan, Q.; Reynolds, M.G.; Quinn, X.; Norris, S.; Townsend, M.B.; Satheshkumar, P.S.; et al. Clinical characterization of human monkeypox infections in the Democratic Republic of the Congo. MedRxiv 2022. [Google Scholar] [CrossRef]
- Brown, K.; Leggat, P.A. Human Monkeypox: Current State of Knowledge and Implications for the Future. Trop. Med. Infect. Dis. 2016, 1, 8. [Google Scholar] [CrossRef]
- Singhal, T.; Kabra, S.K.; Lodha, R. Monkeypox: A Review. Indian J. Pediatr. 2022, 89, 955–960. [Google Scholar] [CrossRef]
- Seang, S.; Burrel, S.; Todesco, E.; Leducq, V.; Monsel, G.; Le Pluart, D.; Cordevant, C.; Pourcher, V.; Palich, R. Evidence of human-todog transmission of monkeypox virus. Lancet 2022, 400, 658–659. [Google Scholar] [CrossRef]
- Zachary, K.C.; Shenoy, E.S. Monkeypox transmission following exposure in healthcare facilities in nonendemic settings: Low risk but limited literature. Infect Control. Hosp. Epidemiol. 2022, 43, 920–924. [Google Scholar] [CrossRef]
- Essbauer, S.; Pfeffer, M.; Meyer, H. Zoonotic poxviruses. Vet. Microbiol. 2010, 140, 229–236. [Google Scholar] [CrossRef]
- Okyay, R.A.; Bayrak, E.; Kaya, E.; Sahin, A.R.; Kocyigit, B.F.; Tasdogan, A.M.; Avci, A.; Sumbul, H.E. Another Epidemic in the Shadow of Covid 19 Pandemic: A Review of Monkeypox. Eurasian J. Med. Oncol. 2022, 6, 95–99. [Google Scholar] [CrossRef]
- Beer, E.M.; Rao, V.B. A systematic review of the epidemiology of human monkeypox outbreaks and implications for outbreak strategy. PLoS Negl. Trop. Dis. 2019, 13, e0007791. [Google Scholar] [CrossRef]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibiet, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Mahzoum, K.; Dardas, L.A.; Al-Tammemi, A.B.; Al-Majali, L.; Al-Naimat, H.; Jardaneh, L.; AlHadidi, F.; Al-Salahat, K.; Al-Ajlouni, E.; et al. Knowledge of Human Monkeypox and Its Relation to Conspiracy Beliefs among Students in Jordanian Health Schools: Filling the Knowledge Gap on Emerging Zoonotic Viruses. Medicina 2022, 58, 924. [Google Scholar] [CrossRef]
- Al-Tammemi, A.B.; Albakri, R.; Alabsi, S. The Outbreak of Human Monkeypox in 2022: A Changing Epidemiology or an Impending Aftereffect of Smallpox Eradication? Front. Trop. Dis. 2022, 3, 951380. [Google Scholar] [CrossRef]
- Sklenovská, N.; Van Ranst, M. Emergence of Monkeypox as the Most Important Orthopoxvirus Infection in Humans. Front. Public Health 2018, 6, 241. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L. Monkeypox: WHO declares a public health emergency of international concern. BMJ 2022, 378, o1874. [Google Scholar] [CrossRef] [PubMed]
- Science Media Centre. Expert Reaction to WHO Declaring the Global Monkeypox Outbreak A Public Health Emergency of International Concern. Available online: https://www.sciencemediacentre.org/expert-reaction-to-who-declaring-the-global-monkeypox-outbreak-a-public-health-emergency-of-international-concern-pheic/ (accessed on 1 October 2022).
- Lahariya, C. Re-emerging diseases and epidemic threats: Ten ‘areas of actions’ (AA-10) and a case for global solidarity. J. Vector Borne Dis. 2017, 54, 1–3. [Google Scholar]
- Lahariya, C.; Thakur, A.; Dudeja, N. Monkeypox Disease Outbreak (2022): Epidemiology, Challenges, and the Way Forward. Indian Pediatr. 2022, 59, 636–642. [Google Scholar] [CrossRef]
- Jamil, H.; Tariq, W.; Tahir, M.J.; Mahfooz, R.S.; Asghar, M.S.; Ahmed, A. Human monkeypox expansion from the endemic to non-endemic regions: Control measures. Ann. Med. Surg. 2022, 79, 104048. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Kong, J.D.; Mahroum, N.; Tsigalou, C.; Khamisy-Farah, R.; Converti, M.; Wu, J. Epidemiological trends and clinical features of the ongoing monkeypox epidemic: A preliminary pooled data analysis and literature review. J. Med. Virol. 2022. [CrossRef]
- Bragazzi, N.L.; Khamisy-Farah, R.; Tsigalou, C.; Mahroum, N.; Converti, M. Attaching a stigma to the LGBTQI+ community should be avoided during the monkeypox epidemic. J. Med. Virol. 2022, 1–2. [Google Scholar] [CrossRef]
- Lapa, D.; Carletti, F.; Mazzotta, V.; Matusali, G.; Pinnetti, C.; Meschi, S.; Gagliardini, R.; Colavita, F.; Mondi, A.; Minosse, C.; et al. Monkeypox virus isolation from a semen sample collected in the early phase of infection in a patient with prolonged seminal viral shedding. Lancet Infect. Dis. 2022, 22, 1267–1269. [Google Scholar] [CrossRef]
- Magnus, P.V.; Andersen, E.K.; Petersen, K.B.; Andersen, A.B. A pox-like disease in Cynomolgus Monkeys. Acta Pathol. Microbiol. Scand. 1959, 46, 156–176. [Google Scholar] [CrossRef]
- Simpson, K.; Heymann, D.; Brown, C.S.; Edmunds, W.J.; Elsgaard, J.; Fine, P.; Hochrein, H.; Hoff, N.A.; Green, A.; Ihekweazu, C.; et al. Human monkeypox—after 40 years, an unintended consequence of smallpox eradication. Vaccine 2020, 38, 5077–5081. [Google Scholar] [CrossRef]
- Gong, Q.; Wang, C.; Chuai, X.; Chiu, S. Monkeypox virus: A re-emergent threat to humans. Virol. Sin. 2022, 37, 477–482. [Google Scholar] [CrossRef]
- Mauldin, M.R.; McCollum, A.M.; Nakazawa, Y.J.; Mandra, A.; Whitehouse, E.R.; Davidson, W.; Zhao, H.; Gao, J.; Li, Y.; Doty, J.; et al. Exportation of monkeypox virus from the African continent. J. Infect. Dis. 2022, 225, 1367–1376. [Google Scholar] [CrossRef]
- Hobson, G.; Adamson, J.; Adler, H.; Firth, R.; Gould, S.; Houlihan, C.; Johnson, C.; Porter, D.; Rampling, T.; Ratcliffe, L.; et al. Family cluster of three cases of monkeypox imported from Nigeria to the United Kingdom, May 2021. Eurosurveillance 2021, 26, 2100745. [Google Scholar] [CrossRef]
- Harris, E. What to Know About Monkeypox. JAMA 2022, 327, 2278–2279. [Google Scholar] [CrossRef]
- Duque, M.P.; Ribeiro, S.; Martins, J.V.; Casaca, P.; Leite, P.P.; Tavares, M.; Mansinho, K.; Duque, L.M.; Fernandes, C.; Cordeiro, R.; et al. Ongoing monkeypox virus outbreak, Portugal, 29 April to 23 May 2022. Eurosurveillance 2022, 27, 2200424. [Google Scholar] [CrossRef]
- Vivancos, R.; Anderson, C.; Blomquist, P.; Balasegaram, S.; Bell, A.; Bishop, L.; Brown, C.S.; Chow, Y.; Edeghere, O.; Florence, I.; et al. Community transmission of monkeypox in the United Kingdom, April to May 2022. Eurosurveillance 2022, 27, 2200422. [Google Scholar] [CrossRef]
- 2022 Monkeypox Outbreak Global Map. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 23 September 2022).
- India confirms first case of monkeypox in WHO South-East Asia Region. Available online: https://www.who.int/southeastasia/news/detail/15-07-2022-india-confirms-first-case-of-monkeypox-in-who-south-east-asia-region (accessed on 2 August 2022).
- Alkhalil, A.; Hammamieh, R.; Hardick, J.; Ichou, M.A.; Jett, M.; Ibrahim, S. Gene expression profiling of monkeypox virus-infected cells reveals novel interfaces for host-virus interactions. Virol. J. 2010, 7, 173. [Google Scholar] [CrossRef]
- Moss, B. Poxvirus cell entry: How many proteins does it take? Viruses 2012, 4, 688–707. [Google Scholar] [CrossRef]
- Moore, M.J.; Zahra, F. Monkeypox [Updated 2022 Jul 16]. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kabuga, A.I.; Zowalaty, M.E.E. A review of the monkeypox virus and a recent outbreak of skin rash disease in Nigeria. J. Med. Virol. 2019, 91, 533–540. [Google Scholar] [CrossRef]
- Hutson, C.L.; Carroll, D.S.; Gallardo-Romero, N.; Drew, C.; Zaki, S.R.; Nagy, T.; Hughes, C.; Olson, V.A.; Sanders, J.; Patel, N.; et al. Comparison of Monkeypox Virus Clade Kinetics and Pathology within the Prairie Dog Animal Model Using a Serial Sacrifice Study Design. Biomed Res. Int. 2015, 2015, 965710. [Google Scholar] [CrossRef]
- Titanji, B.K.; Tegomoh, B.; Nematollahi, S.; Konomos, M.; Kulkarni, P.A. Monkeypox: A Contemporary Review for Healthcare Professionals. Open Forum Infect. Dis. 2022, 9, ofac310. [Google Scholar] [CrossRef]
- Clinical Management and Infection Prevention and Control for Monkeypox: Interim Rapid Response Guidance, 10 June 2022. Available online: https://www.who.int/publications/i/item/WHO-MPX-Clinical-and-IPC-2022.1 (accessed on 15 September 2022).
- Reynolds, M.G.; McCollum, A.M.; Nguete, B.; Shongo-Lushima, R.; Petersen, B.W. Improving the Care and Treatment of Monkeypox Patients in Low-Resource Settings: Applying Evidence from Contemporary Biomedical and Smallpox Biodefense Research. Viruses 2017, 9, 380. [Google Scholar] [CrossRef] [PubMed]
- Alakunle, E.F.; Okeke, M.I. Monkeypox virus: A neglected zoonotic pathogen spreads globally. Nat. Rev. Microbiol. 2022, 20, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Kaler, J.; Hussain, A.; Flores, G.; Kheiri, S.; Desrosiers, D. Monkeypox: A Comprehensive Review of Transmission, Pathogenesis, and Manifestation. Cureus 2022, 14, e26531. [Google Scholar] [CrossRef] [PubMed]
- Tiecco, G.; Degli Antoni, M.; Storti, S.; Tomasoni, L.R.; Castelli, F.; Quiros-Roldan, E. Monkeypox, a Literature Review: What Is New and Where Does This concerning Virus Come From? Viruses 2022, 14, 1894. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S. Monkeypox. Br. Dent. J. 2022, 232, 760. [Google Scholar] [CrossRef]
- Huhn, G.D.; Bauer, A.M.; Yorita, K.; Graham, M.B.; Sejvar, J.; Likos, A.; Damon, I.K.; Reynolds, M.G.; Kuehnert, M.J. Clinical characteristics of human monkeypox, and risk factors for severe disease. Clin. Infect. Dis. 2005, 41, 1742–1751. [Google Scholar] [CrossRef]
- Guidelines for Collecting and Handling Specimens for Monkeypox Testing. Available online: https://www.cdc.gov/poxvirus/monkeypox/clinicians/prep-collection-specimens.html (accessed on 16 September 2022).
- Ministry of Health and Family Welfare, Government of India. Guidelines for Management of Monkeypox Disease. Available online: https://main.mohfw.gov.in/sites/default/files/Guidelines%20for%20Management%20of%20Monkeypox%20Disease.pdf (accessed on 15 September 2022).
- Weinstein, R.A.; Nalca, A.; Rimoin, A.W.; Bavari, S.; Whitehouse, C.A. Reemergence of Monkeypox: Prevalence, Diagnostics, and Countermeasures. Clin. Infect. Dis. 2005, 41, 1765–1771. [Google Scholar] [CrossRef]
- The Threat. Available online: https://www.cdc.gov/smallpox/bioterrorism/public/threat.html (accessed on 12 September 2022).
- McCollum, A.M.; Damon, I.K. Human monkeypox. Clin. Infect. Dis. 2014, 58, 260–267. [Google Scholar] [CrossRef]
- Breman, J.G.; Henderson, D.A. Diagnosis and management of smallpox. N. Engl. J. Med. 2002, 346, 1300–1308. [Google Scholar] [CrossRef]
- Monkeypox. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 15 September 2022).
- Infection Prevention and Control of Monkeypox in Healthcare Settings. Available online: https://www.cdc.gov/poxvirus/monkeypox/clinicians/infection-control-healthcare.htm (accessed on 15 September 2022).
- Monkeypox, COVID-19 & Other Global Health Issues Virtual Press conference transcript - 27 July 2022. Available online: https://www.who.int/publications/m/item/monkeypox--covid-19---other-global-health-issues-virtual-press-conference-transcript---27-july-2022 (accessed on 16 September 2022).
- Rao, A.K.; Petersen, B.W.; Whitehill, F.; Razeq, J.H.; Isaacs, S.N.; Merchlinsky, M.J.; Campos-Outcalt, D.; Morgan, R.L.; Damon, I.; Sánchez, P.J.; et al. Use of JYNNEOS (Smallpox and Monkeypox Vaccine, Live, Nonreplicating) for Preexposure Vaccination of Persons at Risk for Occupational Exposure to Orthopoxviruses: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 734–742, Erratum in MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 886. [Google Scholar] [CrossRef]
- Turner, W.; Mandia, J.; Keltner, C.; Haynes, R.; Faestel, P.; Mease, L. Monkeypox in patient immunized with ACAM2000 smallpox vaccine during 2022 outbreak. Emerg. Infect. Dis. 2022, 28. Epub ahead of print. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Interim Clinical Guidance for Treatment of Monkeypox. Available online: https://www.cdc.gov/poxvirus/monkeypox/clinicians/treatment.html (accessed on 27 July 2022).




{kind=link}
{kind=link}
{kind=link}
| Diagnostic Tests | Description | Specimen Used |
|---|---|---|
| Polymerase chain reaction (PCR) | It is based on the nucleic acid amplification test (NAAT) that demonstrates monkeypox DNA (deoxyribonucleic acid); real-time PCR is currently the gold standard. | Lesion exudate/crust sample |
| Viral culture | The virus is cultured and isolated from a patient specimen. | Lesion exudate |
| Electron microscopy | Morphologically demonstrate the pox viruses. | Biopsy, scab lesion, vesicular exudate |
| Immunohistochemistry | Demonstrates Orthopoxvirus-specific antigens. | Biopsy |
| Anti-Orthopoxvirus immunoglobulin G (IgG) and immunoglobulin M (IgM) tests | Evaluate a recent or previous exposure to Orthopoxvirus. | Blood sample |
| Disease Features | Monkeypox | Smallpox | Chickenpox |
|---|---|---|---|
| HISTORY | |||
| Mode of infection | Previous outbreaks-
| Respiratory droplet infection and by contact with skin exanthem | Airborne disease, spread by coughing/sneezing, and by contact with skin exanthem |
| 2022 Outbreak Possible sexual route as this outbreak witnessed cases, particularly in gay and bisexual men, and men who have sex with men | |||
| INCUBATION PERIOD | |||
| 7 to 17 days | 7 to 17 days | 10 to 21 days | |
| PRODROMAL PHASE (mild or absent in the 2022 monkeypox outbreak) | |||
| Yes (1–4 days) | Yes (2–4 days) | Yes (0–2 days) | |
| CLINICAL EVALUATION | |||
| Fever | 1–3 days before rash | 2–4 days before rash | 1–2 days before rash |
| Moderate fever 38.5–40.5 °C | High fever, often more than 40 °C | Mild/no fever Usually less than 38.8 °C | |
| Malaise | Moderate | Moderate | Mild |
| Lymphadenopathy | Moderate | Absent | Absent |
| Headache | Moderate | Severe | Mild |
| CUTANEOUS EXANTHEM | |||
| Rash development | Slow | Rapid | Rapid |
| Appearance | Umbilicated | Umbilicated | Dewdrop |
| Pattern | Centrifugal | Centrifugal | Centripetal |
| Evolution | Previous monkeypox outbreaks: monomorphic (single stage of development) | Monomorphic | Pleomorphic |
| 2022 monkeypox outbreak: pleomorphic (different stage of development) | |||
| Distribution | Previous monkeypox outbreaks: denser on the face, palms and soles, and mucous membranes | Starts on the face, followed by spreading to arms and legs, and hands and feet. | Starts on the chest, back, and face, and then spread over the entire body, including inside the mouth, eyelids, or genital area |
| 2022 monkeypox outbreak: usually limited to the genital, perigenital, and perianal sites, with mild or absent prodromal features | |||
| Depth (mm) | Superficial–deep (2–6 mm) | Deep (4–6 mm) | Superficial (2–4 mm) |
| Peeling/Desquamation of rash | 22–24 day | 14–21 days | 6–14 days |
| COMPLICATIONS | |||
| Encephalitis | Less than 1% | Less than 1% | Less than 1% |
| Pneumonitis | Yes up to 12% | Possible | Yes up to 16% |
| Eye complications | Yes up to 5% | Yes up to 9% | None |
| Secondary Soft tissue infections | Yes | Yes | Yes |
| Component of Management | Signs/Symptoms | Treatment Protocol |
|---|---|---|
| Protection of compromised skin and mucous membranes | Skin exanthem |
|
| Genital lesions |
| |
| Conjunctivitis |
| |
| Symptomatic relief | Fever |
|
| Itching/Pruritus |
| |
| Nausea and vomiting |
| |
| Headache/malaise |
| |
| Nutritional support, fluid and electrolytes balance | Dehydration can occur in association with poor appetite, nausea, vomiting, and diarrhoea |
|
| Complication | Management |
|---|---|
| Skin exfoliation |
|
| Necrotizing soft tissue infection |
|
| Ocular lesions |
|
| Acute respiratory distress syndrome |
|
| Severe dehydration and hypovolaemic shock |
|
| Sepsis and septic shock |
|
| Encephalitis |
|
| Nutritional considerations |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasan, S.; Saeed, S. Monkeypox Disease: An Emerging Public Health Concern in the Shadow of COVID-19 Pandemic: An Update. Trop. Med. Infect. Dis. 2022, 7, 283. https://doi.org/10.3390/tropicalmed7100283
Hasan S, Saeed S. Monkeypox Disease: An Emerging Public Health Concern in the Shadow of COVID-19 Pandemic: An Update. Tropical Medicine and Infectious Disease. 2022; 7(10):283. https://doi.org/10.3390/tropicalmed7100283
Chicago/Turabian StyleHasan, Shamimul, and Shazina Saeed. 2022. "Monkeypox Disease: An Emerging Public Health Concern in the Shadow of COVID-19 Pandemic: An Update" Tropical Medicine and Infectious Disease 7, no. 10: 283. https://doi.org/10.3390/tropicalmed7100283
APA StyleHasan, S., & Saeed, S. (2022). Monkeypox Disease: An Emerging Public Health Concern in the Shadow of COVID-19 Pandemic: An Update. Tropical Medicine and Infectious Disease, 7(10), 283. https://doi.org/10.3390/tropicalmed7100283