Discordant Clinical Outcomes in a Monozygotic Dichorionic-Diamniotic Twin Pregnancy with Probable Zika Virus Exposure. Case Report


 ,
, 

Abstract
1. Introduction
2. Materials and Methods
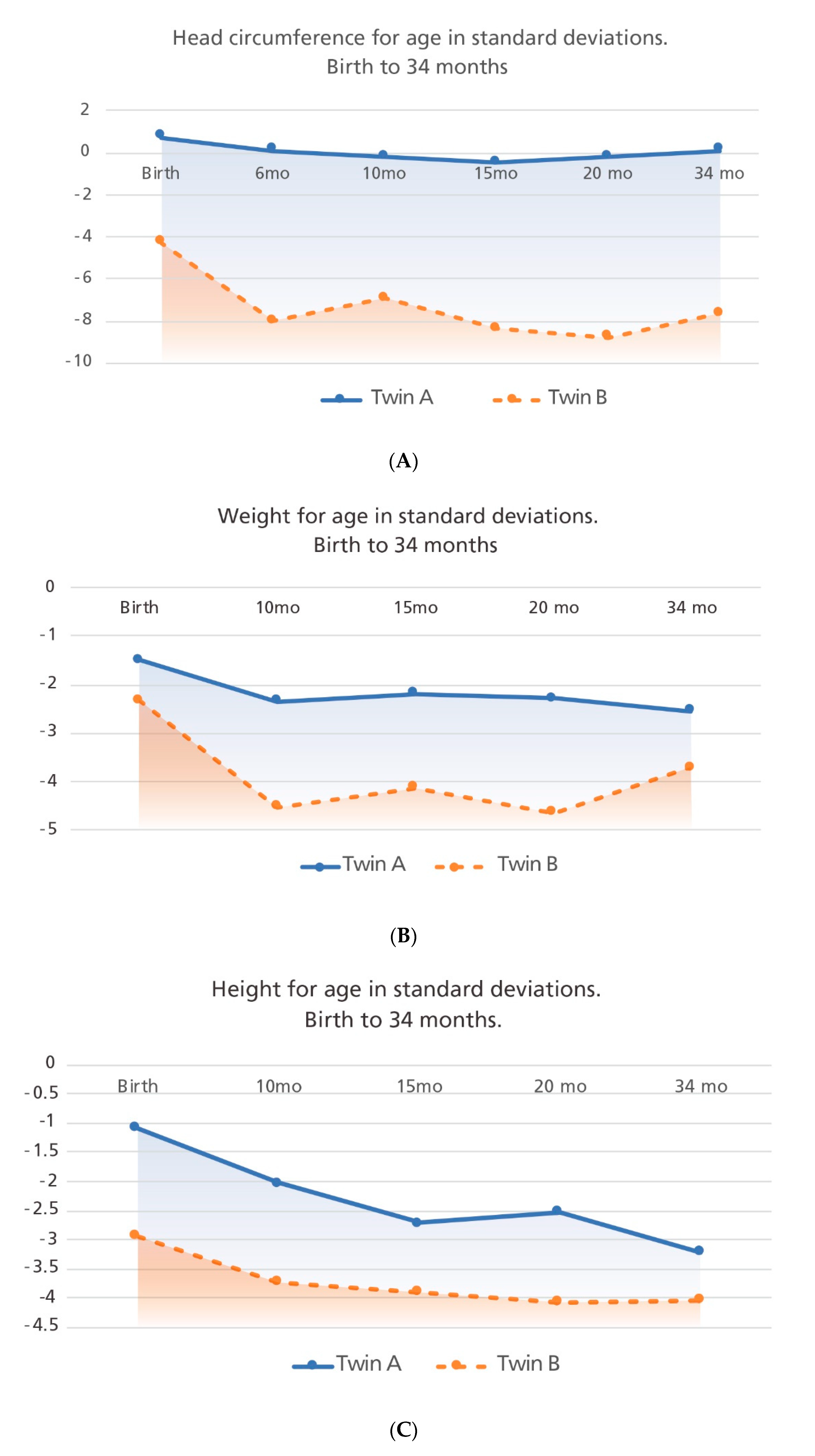
2.1. Anthropometric Evaluations
2.2. Laboratory Testing
2.3. Ethics
3. Case Report
3.1. Pregnancy Information
3.2. Infant Description
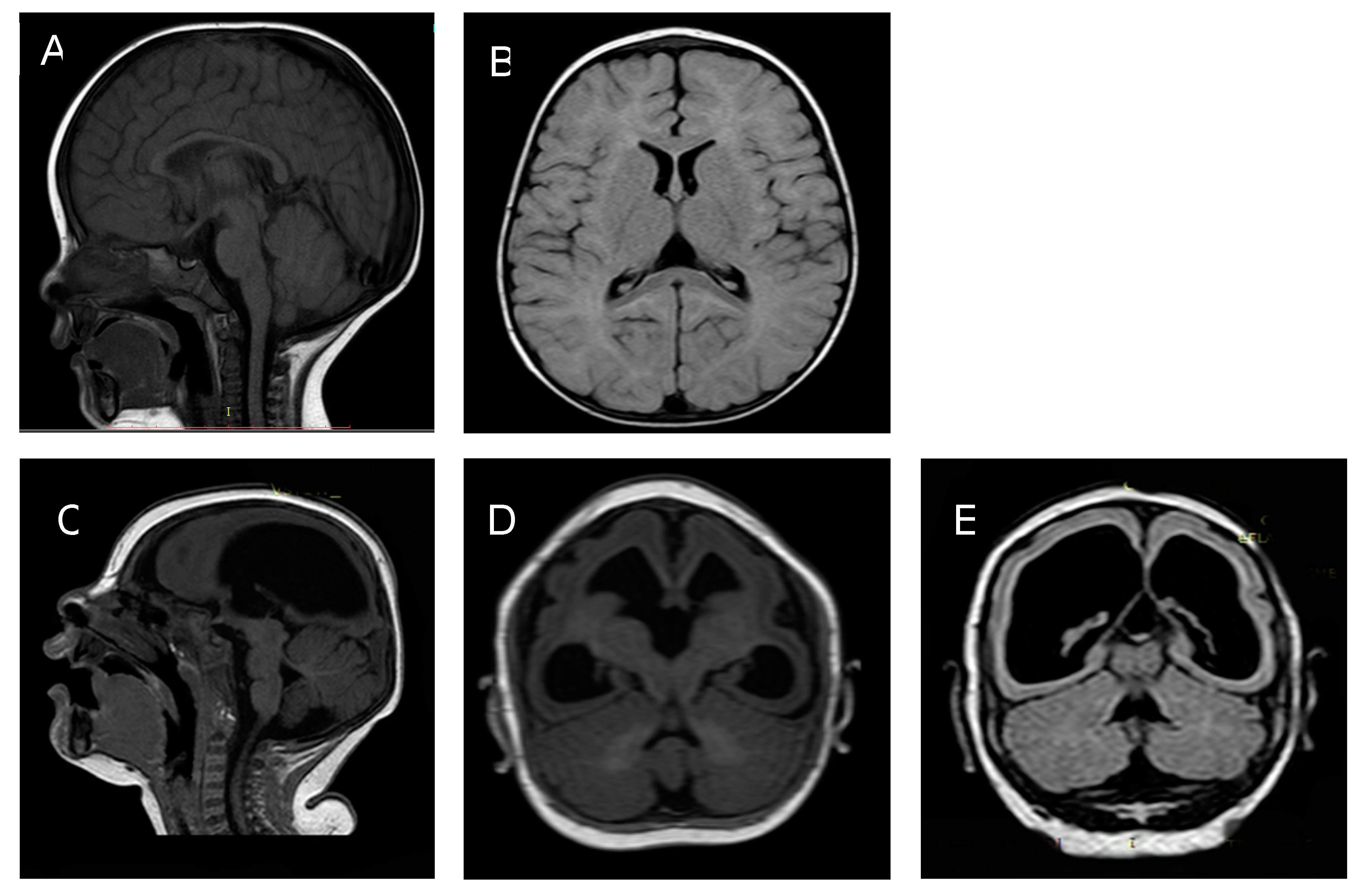
3.2.1. Twin A
3.2.2. Twin B
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
CDC Disclaimer
References
- Lowe, R.; Barcellos, C.; Brasil, P.; Cruz, O.G.; Honório, N.A.; Kuper, H.; Sa Carvalho, M. The Zika virus epidemic in Brazil: From discovery to future implications. Int. J. Environ. Res. Public Health 2018, 15, 96. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Hammack, C.; Ogden, S.C.; Wen, Z.; Qian, X. Zika virus infects human cortical neural precursos and attenuates their growth. Cell Stem Cell 2017, 18, 587–590. [Google Scholar] [CrossRef]
- Ho, C.Y.; Ames, H.M.; Tipton, A.; Vezina, G.; Liu, J.S.; Scafidi, J.; Torii, M.; Rodriguez, F.; du Plessis, A.; DeBiasi, R. Differential neuronal susceptibility and apoptosis in congenital Zika virus infection. Ann. Neurol. 2017, 82, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.M.; Delaney, A.; Jones, A.M.; Carr, C.P.; Liberman, R.F.; Forestieri, N.E.; Tong, V.; Gilboa, S.M.; Honein, M.A.; Moore, C.A.; et al. Updated baseline prevalence of birth defects potentially related to Zika virus infection. Birth Defects Res. 2019, 111, 938–940. [Google Scholar] [CrossRef] [PubMed]
- Cranston, J.S.; Tiene, S.F.; Nielsen-Saines, K.; Vasconcelos, Z.; Pone, M.V.; Pone, S.; Zin, A.; Salles, T.S.; Pereora, J.P., Jr.; Orofino, D.; et al. Association between antenatal exposure to Zika virus and anatomical and neurodevelopmental abnormalities in children. JAMA Netw. Open 2020, 3, e209303. [Google Scholar] [CrossRef]
- Pereira, H.V.F.S.; dos Santos, S.P.; Amâncio, A.P.R.L.; de Oliveira-Szejnfeld, P.S.; Flor, E.O.; de Sales Tavares, J.; Ferreira, R.V.B.; Tovar-Moll, F.; Ramos de Amorim, M.M.; Melo, A. Neurological outcomes of congenital Zika syndrome in toddlers and preschoolers: A case series. Lancet Child Adolesc. Health 2020, 4, 378–387. [Google Scholar] [CrossRef]
- Musso, D.; Ko, A.; Baud, D. Zika virus infection—After the pandemic. N. Engl. J. Med. 2019, 381, 1444–1457. [Google Scholar] [CrossRef]
- Galang, R.R.; Avila, G.A.; Valencia, D.; Daza, M.; Tong, V.T.; Bermúdez, A.J.; Gilboa, S.M.; Rico, A.; Cates, J.; Pacheco, O.; et al. Etiology of microcephaly and central nervous system defects during the Zika epidemic in Colombia. J. Pediatr. 2020, 222, 112–119. [Google Scholar] [CrossRef]
- Ospina, M.L.; Tong, V.T.; Gonzalez, M.; Valencia, D.; Mercado, M.; Gilboa, S.M.; Rodriguez, A.J.; Tinker, S.C.; Rico, A.; Winfield, C.M.; et al. Zika virus disease and pregnancy outcomes in Colombia. N. Engl. J. Med. 2020, 383, 537–545. [Google Scholar] [CrossRef]
- Stirnemann, J.; Villar, J.; Salomon, L.J.; Ohuma, E.; Ruyan, P.; Altman, D.G.; Nosten, F.; Craik, R.; Munim, S.; Ismail, L.C.; et al. International estimated fetal weight standards of the INTERGROWTH-21st Project. Ultrasound Obstet. Gynecol. 2017, 49, 478–486. [Google Scholar] [CrossRef]
- Papageorghiou, A.T.; Ohuma, E.O.; Altman, D.G.; Todros, T.; Ismail, L.C.; Lambert, A.; Jaffer, Y.A.; Bertino, E.; Gravett, M.G.; Purwar, M.; et al. International standards for fetal growth based on serial ultrasound measurements: The Fetal Growth Longitudinal Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 869–879. [Google Scholar] [CrossRef]
- Villar, J.; Ismail, L.C.; Victora, C.G.; Ohuma, E.O.; Bertino, E.; Altman, D.G.; Lambert, A.; Papageorghiou, A.T.; Carvalho, M.; Jaffer, Y.A.; et al. International standards for newborn weight, length, and head circumference by gestational age and sex: The Newborn Cross-Sectional Study of the INTERGROWTH-21st Project. Lancet 2014, 384, 857–868. [Google Scholar] [CrossRef]
- De Onis, M. 4.1 The WHO child growth standards. World Rev. Nutr. Diet. 2015, 113, 278–294. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Salud. Public Health Surveillance Protocol: Zika Virus Disease, Código 895. Available online: https://www.ins.gov.co/buscadoreventos/Lineamientos/PRO%20Zika.pdf (accessed on 16 December 2020).
- Cuevas Ortiz, E.L.; Martínez Ospina, M.L.; Martinez Duran, M.E. Protocolo de Vigilancia en Salud Pública Vigilancia intensificada en salud pública de la microcefalia y otros defectos congénitos del Sistema Nervioso Central. Instituto Nacional de Salud. 2016. Available online: https://www.ins.gov.co/buscador-eventos/Lineamientos/Instructivo%20analisis%20casos%20microcefalia%20y%20otros%20DC%20de%20SNC.pdf (accessed on 16 December 2020).
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Velez, J.O.; Lambert, A.J.; Johnson, A.J.; Stanfield, S.M.; Duffy, M.R. Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 2008, 14, 1232–1239. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Trioplex Real-time RT-PCR Assay: Instructions of Use. 2017; pp. 1–29. Available online: https://www.fda.gov/downloads/medicaldevices/safety/emergencysituations/ucm491592.pdf (accessed on 16 December 2020).
- República de Colombia; Ministerio de la Protección Social. Decreto Número 2323 de 2006, por el Cual se Reglamenta Parcialmente la Ley 09 de 1979, en Relación con la Red Nacional de Laboratorios. Available online: https://www.invima.gov.co/images/pdf/red-nal-laboratorios/decretos/DECRETO_2323_DE_2006.pdf (accessed on 16 December 2020).
- Moore, C.A.; Staples, J.E.; Dobyns, W.B.; Pessoa, A.; Ventura, C.V.; Da Fonseca, E.B.; Marques Ribeiro, E.; Ventura, L.O.; Nogueira Neto, N.; Arena, J.F.; et al. Characterizing the pattern of anomalies in congenital Zika syndrome for pediatric clinicians. JAMA Pediatr. 2017, 171, 288–295. [Google Scholar] [CrossRef]
- del Campo, M.; Feitosa, I.M.L.; Ribeiro, E.M.; Horovitz, D.D.G.; Pessoa, A.L.S.; França, G.V.A.; Garcia-Alix, A.; Doriqui, M.J.R.; Wanderley, H.Y.C.; Sanseverino, M.V.T.; et al. The phenotypic spectrum of congenital Zika syndrome. Am. J. Med. Genet. Part A 2017, 173, 841–857. [Google Scholar] [CrossRef]
- Fernandez, M.P.; Parra Saad, E.; Martinez, M.O.; Corchuelo, S.; Reyes, M.M.; Herrera, M.J.; Parra Saavedra, M.; Rico, A.; Fernandez, A.M.; Lee, R.K.; et al. Ocular histopathologic features of congenital Zika Syndrome. JAMA Ophthalmol. 2017, 135, 1163–1169. [Google Scholar] [CrossRef]
- Lum, F.; Low, D.K.S.; Fan, Y.; Tan, J.J.L.; Lee, B.; Chan, J.K.Y.; Renia, L.; Ginhoux, F.; Ng, L.F.P. Zika Virus infects human fetal brain microglia and induces inflammation. Clin. Infect. Dis. 2017, 64, 914–920. [Google Scholar] [CrossRef]
- Theel, E.S.; Jane Hata, D. Diagnostic testing for Zika virus: A postoutbreak update. J. Clin. Microbiol. 2018, 56, e01972-17. [Google Scholar] [CrossRef]
- Krow-Lucal, E.R.; de Andrade, M.R.; Cananéa, J.N.A.; Moore, C.A.; Leite, P.L.; Biggerstaff, B.J.; Mendes Cabral, C.; Itoh, M.; Percio, J.; Wada, M.Y.; et al. Association and birth prevalence of microcephaly attributable to Zika virus infection among infants in Paraíba, Brazil, in 2015–2016: A case-control study. Lancet Child Adolesc. Health 2018, 2, 205–213. [Google Scholar] [CrossRef]
- Wang, L.N.; Wang, Y.F.; Horne, C.C.; Shiao, L.C. Congenital rubella infection: Escape of one monozygotic twin with two amnions, one chorion, and single placenta. J. Formosan Med. Assoc. 1990, 89, 30–33. [Google Scholar]
- Montgomery, R.C.; Stockdell, K. Congenital rubella in twins. J. Pediatr. 1970, 76, 772–773. [Google Scholar] [CrossRef]
- Lazzarotto, T.; Gabrielli, L.; Foschini, M.P.; Lanari, M.; Guerra, B.; Eusebi, V.; Landini, M.P. Congenital cytomegalovirus infection in twin pregnancies: Viral load in the amniotic fluid and pregnancy outcome. Pediatrics 2003, 112, e153–e157. [Google Scholar] [CrossRef] [PubMed]
- Peyron, F.; Ateba, A.B.; Wallon, M.; Kodjikian, L.; Binquet, C.; Fleury, J.; Garweg, J.G. Congenital toxoplasmosis in twins: A report of fourteen consecutive cases and a comparison with published data. Pediatr. Infect. Dis. J. 2003, 22, 695–701. [Google Scholar] [CrossRef]
- Thapa, R.; Banerjee, P.; Akhtar, N.; Jain, T.S. Discordance for congenital toxoplasmosis in twins. Indian J. Pediatr. 2009, 76, 1069–1070. [Google Scholar] [CrossRef] [PubMed]
- Barton, L.L.; Budd, S.C.; Morfitt, W.S.; Peters, C.J.; Ksiazek, T.G.; Schindler, R.F.; Yoshino, M.T. Congenital lymphocytic choriomeningitis virus infection in twins. Pediatr. Infect. Dis. J. 1993, 12, 942–946. [Google Scholar] [CrossRef]
- Ghannam, A.; Chang, T.; Jantausch, T.; Vezina, G.; Miller, M. Congenital lymphocytic choriomeningitis virus in a member of a twin pregnancy. J. Pediatr. Neurol. 2017, 15, 076–079. [Google Scholar] [CrossRef]
- Sobhani, N.C.; Avvad-Portari, E.; Nascimento, A.C.M.; Machado, H.N.; Lobato, D.S.S.; Pereira, J.P.; Esquivel, M.S.; Vasconcelos, Z.C.; Zin, A.A.; Tsui, I.; et al. Discordant Zika virus findings in twin pregnancies complicated by antenatal Zika Virus exposure: A prospective cohort. J. Infect. Dis. 2020, 221, 1838–1845. [Google Scholar]
- van der Linden, V.; van der Linden, H., Jr.; de Carvalho Leal, M.; Filho, E.L.R.; van der Linden, A.; Aragão, M.d.F.V.V.; Brainer-Lima, A.M.; Di Cavalcanti, D.; Ventura, L.O.; Tabosa Florencia, T.L.; et al. Discordant clinical outcomes of congenital Zika virus infection in twin pregnancies. Arq. Neuro-Psiquiatr. 2017, 75, 381–386. [Google Scholar] [CrossRef]
- Caires-Júnior, L.C.; Goulart, E.; Melo, U.S.; Araujo, B.S.H.; Alvizi, L.; Soares-Schanoski, A.; de Olivera, D.F.; Shigeru Kobayashi, G.; Griesi-Oliveira, K.; Manso Musso, C.; et al. Discordant congenital Zika syndrome twins show differential in vitro viral susceptibility of neural progenitor cells. Nat. Commun. 2018, 9, 475. [Google Scholar] [CrossRef]
- Santos, V.S.; Oliveira, S.J.G.; Gurgel, R.Q.; Lima, D.R.R.; Dos Santos, C.A.; Martins-Filho, P.R.S. Case report: Microcephaly in twins due to the Zika Virus. Am. J. Trop. Med. Hyg. 2017, 97, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Riaz, N.; Wolden, S.L.; Gelblum, D.Y.; Eric, J. Microbial vertical transmission during human pregnancy. Cell Host Microbe 2017, 21, 561–597. [Google Scholar] [CrossRef]
- Benirschke, K. Monozygotic twinning. Surg. Pathol. Clin. 2013, 6, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, B. Histopathological examination of the placenta in twin pregnancies. Apmis 2018, 126, 626–637. [Google Scholar] [CrossRef] [PubMed]
- Czyz, W.; Morahan, J.M.; Ebers, G.C.; Ramagopalan, S.V. Genetic, environmental and stochastic factors in monozygotic twin discordance with a focus on epigenetic differences. BMC Med. 2012, 10, 93. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Hills, S.L.; Oster, A.M.; Porse, C.C.; Danyluk, G.; Cone, M.; Brooks, R.; Scotland, S.; Schiffman, E.; Fredette, C.; et al. Male-to-female sexual transmission of Zika virus-United States, January-April 2016. Clin. Infect. Dis. 2017, 64, 211–213. [Google Scholar] [CrossRef] [PubMed]
- Yarrington, C.D.; Hamer, D.H.; Kuohung, W.; Lee-Parritz, A. Congenital Zika syndrome arising from sexual transmission of Zika virus, a case report. Fertil. Res. Pract. 2019, 5, 1–4. [Google Scholar] [CrossRef]
- Yockey, L.J.; Varela, L.; Rakib, T.; Khoury-Hanold, W.; Fink, S.L.; Stutz, B.; Szigeti-Buck, K.; Van del Pol, A.; Lindenbach, B.; Horvath, T.L.; et al. Vaginal exposure to Zika virus during pregnancy leads to fetal brain infection. Cell 2016, 166, 1247–1256. [Google Scholar] [CrossRef]
- Racicot, K.; Mor, G. Risks associated with viral infections during pregnancy. J. Clin. Investig. 2017, 127, 1591–1599. [Google Scholar] [CrossRef]
- Santos, C.N.O.; Ribeiro, D.R.; Cardoso Alves, J.; Cazzaniga, R.A.; Magalhães, L.S.; De Souza, M.S.F.; Fonseca, A.B.L.; Bispo, A.J.B.; Porto, R.L.S.; Alves Dos Santos, C.; et al. Association between Zika virus microcephaly in newborns with the rs3775291 variant in Toll-Like Receptor 3 and rs1799964 variant at Tumor Necrosis Factor-α Gene. J. Infect. Dis. 2019, 220, 1797–1801. [Google Scholar] [CrossRef]
- Machin, G. Non-identical monozygotic twins, intermediate twin types, zygosity testing, and the non-random nature of monozygotic twinning: A review. Am. J. Med. Genet. Part C Semin. Med. Genet. 2009, 151, 110–127. [Google Scholar] [CrossRef] [PubMed]
- Szylberg, Ł.; Bodnar, M.; Lebioda, A.; Krepska, P.; Kowalewski, A.; Bręborowicz, G.; Marszalek, A. Differences in the expression of TLR-2, NOD2, and NF-κB in placenta between twins. Arch. Immunol. Ther. Exp. 2018, 66, 463–470. [Google Scholar] [CrossRef]
- Egaña-Ugrinovic, G.; Goncé, A.; García, L.; Marcos, M.A.; López, M.; Nadal, A.; Figueras, F. Congenital cytomegalovirus infection among twin pairs. J. Matern. Neonatal. Med. 2016, 29, 3439–3444. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Twin A | Twin B | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| GA by LMP (w/d) | GA by Fetal Biometry (w/d) | EFW g (% for GA) | HC mm (% for GA) | BPD mm (% for GA) | Main Findings | GA by fetal biometry (w/d) | EFW g (% for GA) | HC mm (% for GA) | BPD mm (% for GA) | Main Findings |
| 11/0 | 11/0 | NA | NA | NA | DCDA twin pregnancy | 11/0 | NA | NA | NA | DCDA twin pregnancy |
| 29/4 | 28/2 | 1255 (32.6) | 277 (59.9) | 74 (10.6) | Normal CNS structures, cisterna magna diameter, cerebellar diameter. Normal FD-US. | 25/5 | 883 (<3) | 207 (<3) | 52 (<3) | IUGR, microcephaly enlarged cisterna magna, small cerebellum. Normal FD-US. |
| 31/2 | 30/2 | 1586 (44) | 285 (34) | 78 (10) | Normal FD-US. | 29/0 | 1215 (1) | 225 (<3) | 59 (<3) | IUGR, microcephaly Normal FD-US. |
| 35/2 | 33/4 | 2300 (34) | 309 (26.3) | 86 (12) | Normal FD-US. | 31/6 | 1930 (6) | 258 (<3) | 61 (<3) | IUGR, microcephaly Normal FD-US. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercado, M.; Daza, M.; Moore, C.A.; Valencia, D.; Rico, A.; Álvarez-Diaz, D.A.; Brault, A.C.; Fitzpatrick, K.; Mulkey, S.B. Discordant Clinical Outcomes in a Monozygotic Dichorionic-Diamniotic Twin Pregnancy with Probable Zika Virus Exposure. Case Report. Trop. Med. Infect. Dis. 2020, 5, 188. https://doi.org/10.3390/tropicalmed5040188
Mercado M, Daza M, Moore CA, Valencia D, Rico A, Álvarez-Diaz DA, Brault AC, Fitzpatrick K, Mulkey SB. Discordant Clinical Outcomes in a Monozygotic Dichorionic-Diamniotic Twin Pregnancy with Probable Zika Virus Exposure. Case Report. Tropical Medicine and Infectious Disease. 2020; 5(4):188. https://doi.org/10.3390/tropicalmed5040188
Chicago/Turabian StyleMercado, Marcela, Marcela Daza, Cynthia A. Moore, Diana Valencia, Angelica Rico, Diego A. Álvarez-Diaz, Aaron C. Brault, Kelly Fitzpatrick, and Sarah B. Mulkey. 2020. "Discordant Clinical Outcomes in a Monozygotic Dichorionic-Diamniotic Twin Pregnancy with Probable Zika Virus Exposure. Case Report" Tropical Medicine and Infectious Disease 5, no. 4: 188. https://doi.org/10.3390/tropicalmed5040188
APA StyleMercado, M., Daza, M., Moore, C. A., Valencia, D., Rico, A., Álvarez-Diaz, D. A., Brault, A. C., Fitzpatrick, K., & Mulkey, S. B. (2020). Discordant Clinical Outcomes in a Monozygotic Dichorionic-Diamniotic Twin Pregnancy with Probable Zika Virus Exposure. Case Report. Tropical Medicine and Infectious Disease, 5(4), 188. https://doi.org/10.3390/tropicalmed5040188