Factors Affecting Continued Participation in Tuberculosis Contact Investigation in a Low-Income, High-Burden Setting

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
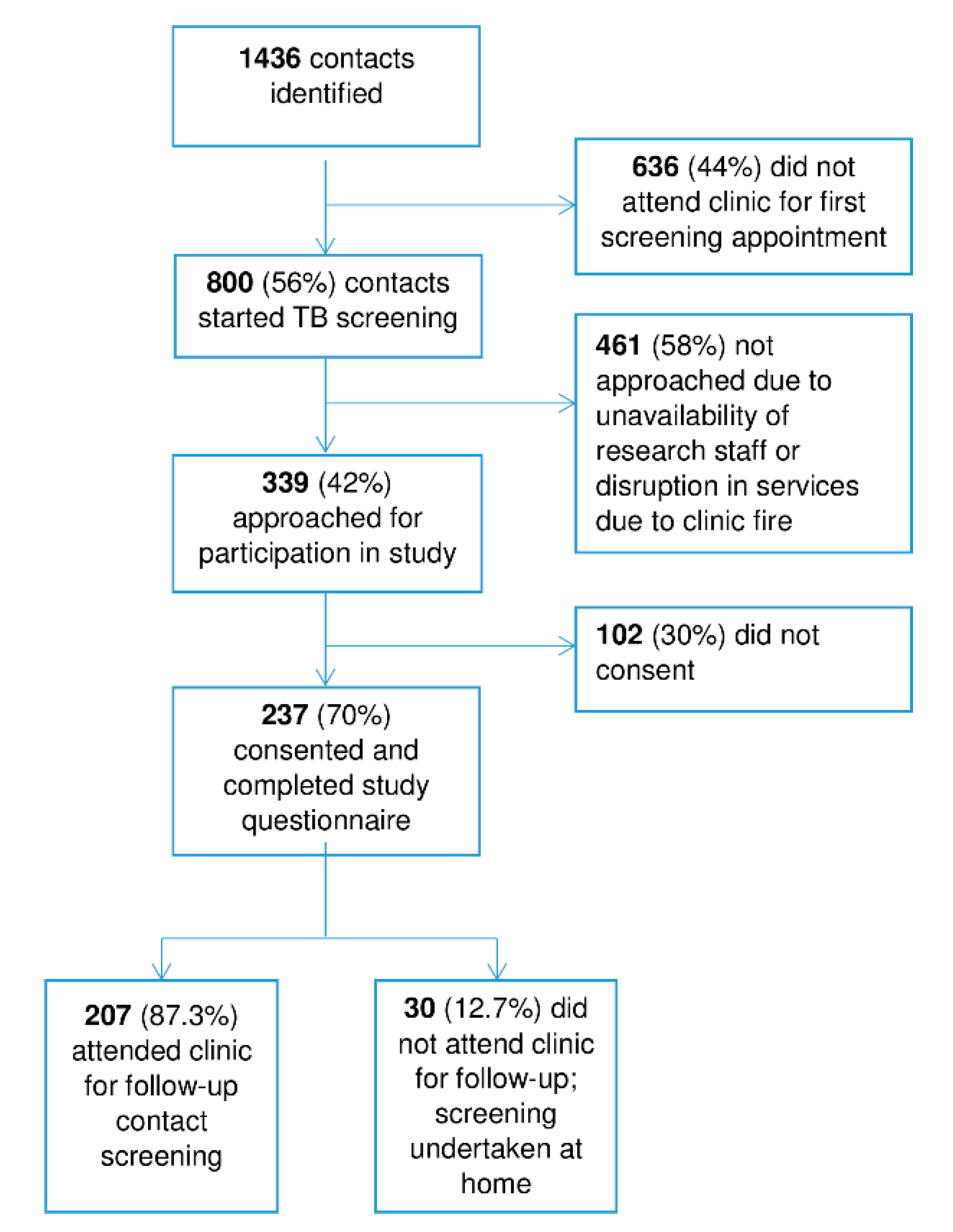
2.1. Design, Setting, and Explanation of Processes
2.2. Participants
2.3. Data Collection
2.4. Definitions
2.5. Analyses
2.6. Ethics
3. Results
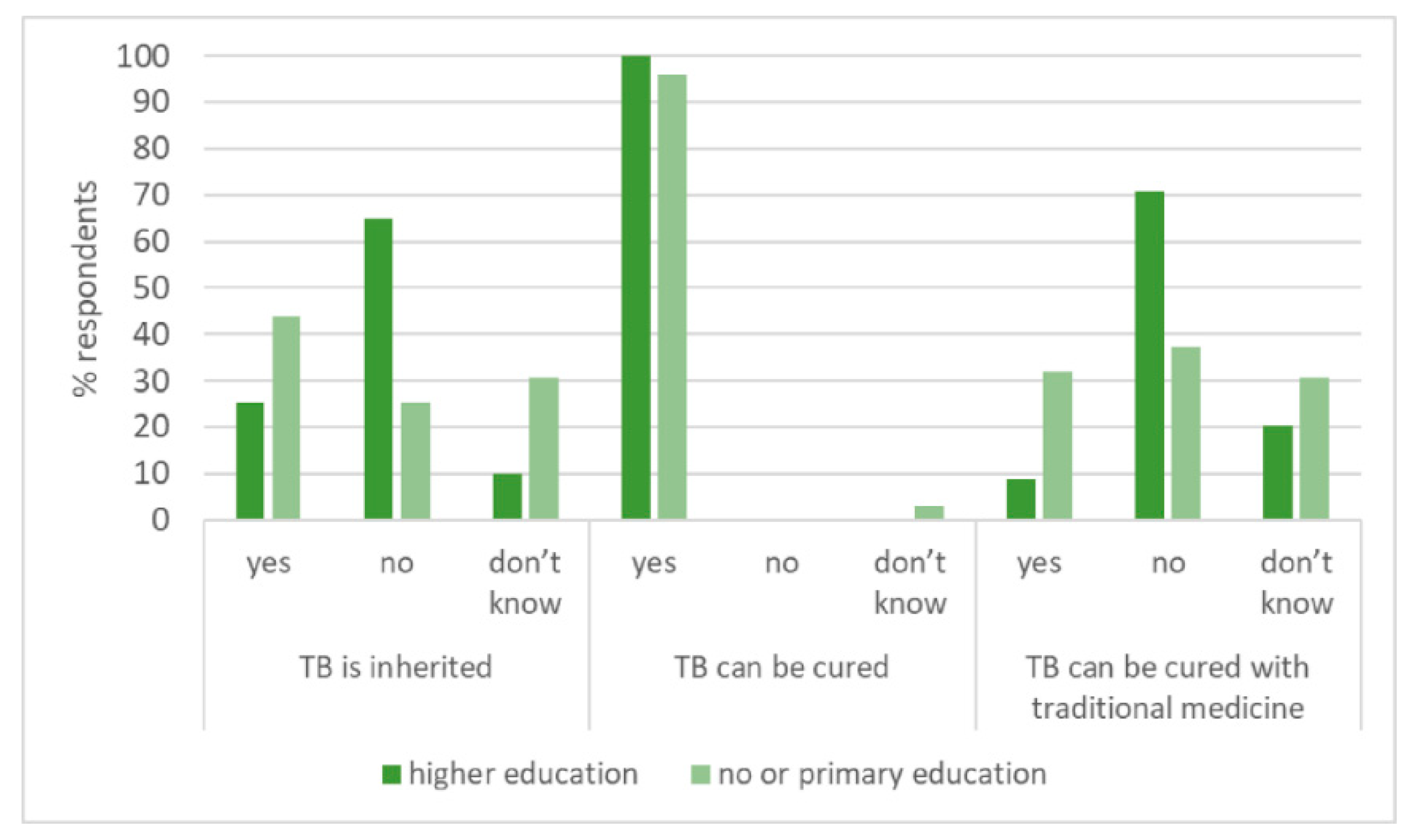
3.1. Knowledge, Attitudes and Practices
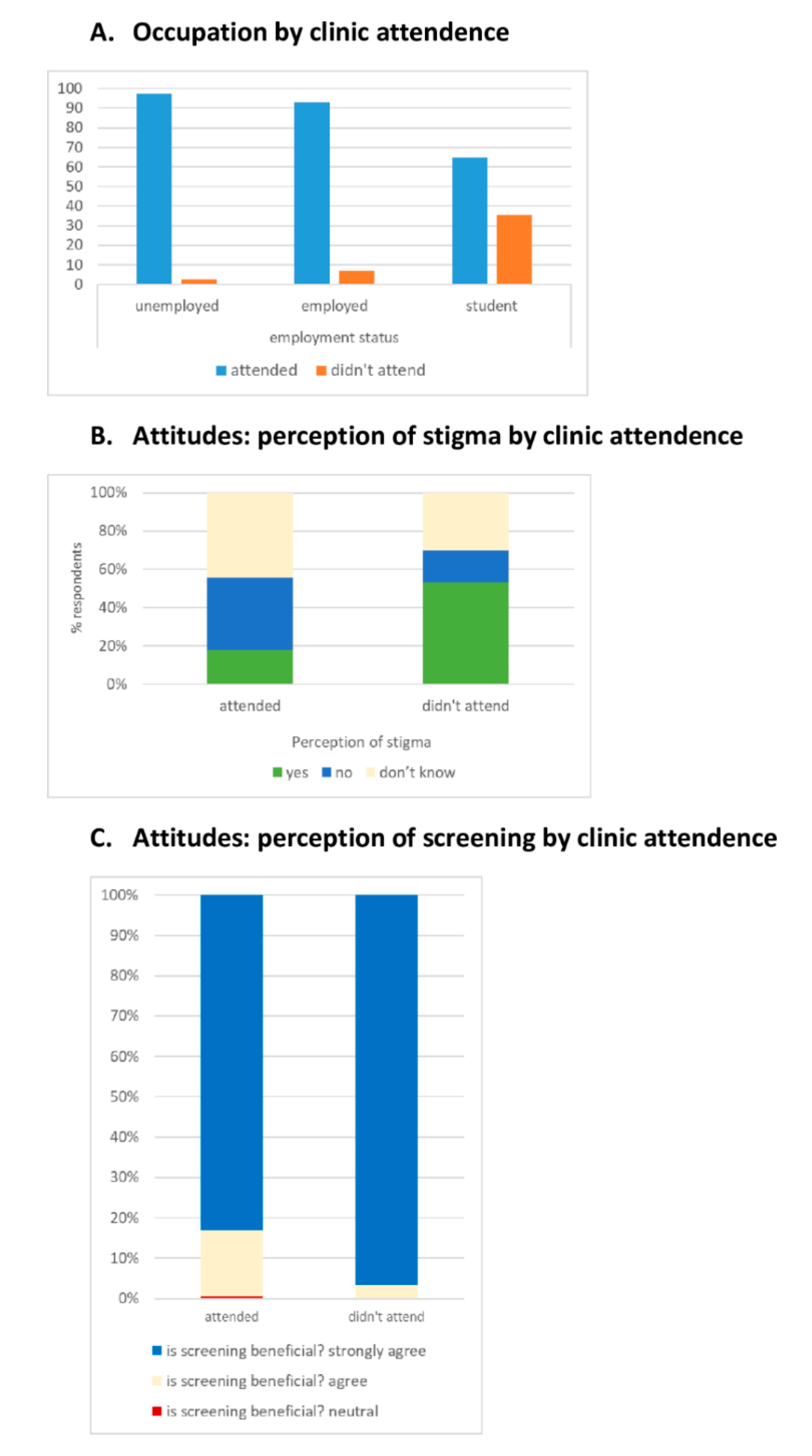
3.2. Associations with Attendance
3.3. Interviews with Non-Attenders
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2019; WHO Press: Geneva, Switzerland, 2019. [Google Scholar]
- Fox, G.J.; Nhung, N.V.; Sy, D.N.; Hoa, N.L.; Anh, L.T.; Anh, N.T.; Hoa, N.B.; Dung, N.H.; Buu, T.N.; Loi, N.T.; et al. Household-Contact Investigation for Detection of Tuberculosis in Vietnam. N. Engl. J. Med. 2018, 378, 221–229. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Latent Tuberculosis Infection: Updated and Consolidated Guidelines for Programmatic Management; WHO Press: Geneva, Switzerland, 2018. [Google Scholar]
- Fox, G.J.; Dobler, C.; Marais, B.; Denholm, J. Preventive therapy for latent tuberculosis infection—The promise and the challenges. Int. J. Infect. Dis. 2017, 56, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Mandalakas, A.M.; Hesseling, A.C.; Gie, R.P.; Schaaf, H.S.; Marais, B.J.; Sinanovic, E. Modelling the cost-effectiveness of strategies to prevent tuberculosis in child contacts in a high-burden setting. Thorax 2012, 68, 247–255. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Control. 2016. Available online: http://www.who.int/tb/publications/global_report/en/ (accessed on 24 August 2017).
- Dony, J.F.; Ahmad, J.; Tiong, Y.K. Epidemiology of tuberculosis and leprosy, Sabah, Malaysia. Tuberculosis 2004, 84, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Sabait, M.; Mohammad, W.M.Z.W.; Abdullah, M.R.; Omar, J. Challenges and Opportunities to Improve Tuberculosis Screening among Immigrant Plantation Workers in Sabah, Malaysia. Int. J. Public Health Sci. 2016, 5, 41. [Google Scholar]
- Ministry of Health Malaysia. Manual Sistem Maklumat Tibi Kebangsaan. In National Tuberculosis Information System [TBIS] Manual; National Information System Development Committee Dcd, Ed.; Ministry of Health Malaysia: Putrajaya, Malaysia, 2002. [Google Scholar]
- Menzies School of Health Research. The Topical Disease Research Regional Collaborative Initiative. 2016. Available online: https://www.menzies.edu.au/page/Research/Projects/Tuberculosis/The_Tropical_Disease_Research_Regional_Collaborative_Initiative/ (accessed on 11 June 2020).
- Fox, G.J.; Loan, L.P.; Nhung, N.V.; Loi, N.T.; Sy, D.N.; Britton, W.J.; Marks, G. Barriers to adherence with tuberculosis contact investigation in six provinces of Vietnam: A nested case–control study. BMC Infect. Dis. 2015, 15, 103. [Google Scholar] [CrossRef] [PubMed]
- Lestari, T.; Graham, S.M.; Boogard, C.V.D.; Triasih, R.; Poespoprodjo, J.R.; Ubra, R.R.; Kenangalem, E.; Mahendradhata, Y.; Anstey, N.M.; Bailie, R.; et al. Bridging the knowledge-practice gap in tuberculosis contact management in a high-burden setting: A mixed-methods protocol for a multicenter health system strengthening study. Implement. Sci. 2019, 14, 31. [Google Scholar] [CrossRef] [PubMed]
- Hulley, S.B.; Cummins, S.R.; Browner, W.S.; Grady, D.; Hearst, N.; Newman, T.B. Designing Clinical Research: An Epidemiological Approach, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Ayé, R.; Wyss, K.; Abdualimova, H.; Saidaliev, S. Illness costs to households are a key barrier to access diagnostic and treatment services for tuberculosis in Tajikistan. BMC Res. Notes 2010, 3, 340. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. The End TB Strategy: Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015; WHO Press: Geneva, Switzerland, 2014. [Google Scholar]
- Mangesho, P.; Shayo, E.; Makunde, W.H.; Keto, G.B.S.; I Mandara, C.; Kamugisha, M.L.; Kilale, A.M.; Ishengoma, D.R.S. Community knowledge, attitudes and practices towards tuberculosis and its treatment in Mpwapwa district, central Tanzania. Tanzania Health Res. Bull. 2007, 9, 38–43. [Google Scholar]
- Tornee, S.; Kaewkungwal, J.; Fungladda, W.; Silachamroon, U.; Akarasewi, P.; Sunakorn, P. Factors associated with the household contact screening adherence of tuberculosis patients. Southeast Asian J. Trop. Med. Public Health 2005, 36, 331–340. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All | Attended | Did not Attend | p |
|---|---|---|---|---|
| Number | 237 | 207 (87.3%) | 30 (12.7%) | |
| Age (median, range) | 28 (17–66) | 30.5 (17–66) | 17 (17–53) | 0.001 |
| Sex | ||||
| Male: number (%) | 76 (32.1) | 72 (94.7%) | 4 (5.3%) | |
| Female: number (%) | 161 (67.9%) | 135 (83.9%) | 26 (16.2%) | 0.021 |
| Nationality | ||||
| Malaysian | 174 (73.4) | 146 (83.9%) | 28 (16.1%) | |
| Non-Malaysian | 63 (26.6) | 61 (96.8%) | 2 (3.2%) | 0.007 |
| Ethnicity | ||||
| Sabah Indigenous (Bumiputera) | 140 (59.1) | 116 (82.9%) | 24 (17.1%) | |
| Malay | 4 (1.7) | 3 (75.0%) | 1 (25.0%) | |
| Chinese Malaysian | 16 (6.8) | 15 (93.8%) | 1 (6.3%) | |
| Indian Malaysian | 1 (0.4) | 1 (100.0%) | 0 (0.0%) | |
| Migrants | 76 (32.1) | 72 (94.7%) | 4 (5.3%) | 0.11 |
| Level of education | ||||
| Bachelors’ and above | 7 (3.0) | 4 (57.4%) | 3 (42.9%) | |
| Diploma | 24 (10.1) | 18 (75.0%) | 6 (25.0%) | |
| High school | 25 (10.5) | 25 (100.0%) | 0 (0.0%) | |
| Middle school | 106 (44.8) | 87 (82.1%) | 19 (17.9%) | |
| Primary school | 20 (8.4) | 20 (100.0%) | 0 (0.0%) | |
| No formal education | 55 (23.2) | 53 (96.4%) | 2 (3.6%) | <0.001 |
| Current main job | ||||
| Unemployed | 9 (3.8) | 9 (100.0%) | 0 (0.0%) | |
| Housewife | 29 (12.2) | 28 (96.6%) | 1 (3.5%) | |
| Self-employed | 72 (30.4) | 72 (100.0%) | 0 (0.0%) | |
| Private employee | 50 (21.1) | 45 (90.0%) | 5 (10.0%) | |
| Government employee | 20 (8.4) | 16 (80.0%) | 4 (20.0%) | |
| Student | 54 (22.8) | 35 (64.8%) | 19 (35.2%) | |
| Other | 3 (1.3) | 2 (66.7%) | 1 (33.3%) | <0.001 |
| Relationship to TB index case | ||||
| Parent | 42 (17.7) | 42 (100.0%) | 0 (0.0%) | |
| Spouse | 40 (16.9) | 39 (97.5%) | 1 (2.5%) | |
| Child | 15 (6.3) | 15 (100.0%) | 0 (0.0%) | |
| Sibling | 20 (8.4) | 20 (100.0%) | 0 (0.0%) | |
| Other relative | 45 (19.0) | 45 (100.0%) | 0 (0.0%) | |
| Other | 75 (31.6) | 46 (61.3%) | 29 (36.7%) | <0.001 |
| Marital status | ||||
| Married | 118 (49.8) | 111 (94.1%) | 7 (5.9%) | |
| Single | 119 (50.2) | 96 (807%) | 23 (19.3%) | 0.003 |
| Monthly income (Malaysian Ringgit, RM *) | ||||
| <RM 710 | 65 (27.4) | 46 (70.7%) | 19 (29.2%) | |
| RM 710–RM 1000 | 61 (25.7) | 59 (96.7%) | 2 (3.3%) | |
| RM 1001–RM 2000 | 77 (32.5) | 76 (98.7%) | 1 (1.3%) | |
| RM 2001–RM 3000 | 16 (6.8) | 16 (100.0%) | 0 (0.0%) | |
| >RM 3000 | 18 (7.6) | 10 (55.6%) | 8 (44.4%) | <0.001 |
| Number of contacts in household: median (range) | 6 (1–15) | 5 (2–15) | 6.5 (1–12) | 0.02 |
| Characteristics (n = 237) | Frequency (%) | ||
|---|---|---|---|
| TB is commonly associated with the following symptoms: | Yes | No | Don’t know |
| Cough | 232 (97.9) | 3 (1.3) | 2 (0.8) |
| Leg pain | 91 (38.4) | 86 (36.3) | 60 (25.3) |
| Weight loss | 194 (81.9) | 21 (8.9) | 22 (9.3) |
| Night sweats | 160 (67.5) | 30 (12.7) | 47 (19.8) |
| Coughing up blood | 231 (97.5) | 4 (1.7) | 2 (0.8) |
| Fever | 156 (65.8) | 38 (16.0) | 43 (18.2) |
| TB can be transmitted by: | |||
| Sneezing | 214 (90.3) | 15 (6.3) | 8 (3.4) |
| Sharing utensils | 182 (76.8) | 41 (17.3) | 14 (5.9) |
| Sleeping in the same room | 187 (78.9) | 38 (16.0) | 12 (5.1) |
| Sharing a toilet | 139 (58.6) | 70 (29.5) | 28 (11.8) |
| Sexual intercourse | 138 (58.2) | 65 (27.4) | 34 (14.3) |
| TB is caused by: | True | False | Don’t Know |
| An infection | 232 (97.9) | 2 (0.8) | 3 (1.3) |
| Unhygienic environment | 228 (96.2) | 3 (1.3) | 6 (2.5) |
| Inherited from parents | 74 (31.2) | 124 (52.3) | 39 (16.5) |
| The following people have higher TB risk: | |||
| Smokers | 213 (81.9) | 14 (5.9) | 10 (4.2) |
| Children | 194 (81.9) | 12 (5.1) | 31 (13.1) |
| People with HIV/AIDS | 208 (87.8) | 4 (1.7) | 25 (10.5) |
| Pregnant women | 154 (65.0) | 23 (9.7) | 60 (25.3) |
| Treatment and cure of TB: | |||
| TB can be completely cured if a patient takes treatment. | 234 (98.7) | 0 (0.0) | 3 (1.3) |
| Traditional medicine can be used to cure TB | 38 (16.0) | 143 (60.3) | 56 (23.7) |
| Question | Frequency (%) |
|---|---|
| Number | 237 |
| Perceive that TB is stigmatised (‘Do you think that there is discrimination against people with TB?’) | |
| Yes | 53 (22.4) |
| No | 83 (35.0) |
| Don’t know | 101 (42.6) |
| Believe that own risk of TB is higher than the general population | |
| Much lower risk | 2 (0.8) |
| Lower risk | 5 (2.1) |
| Similar risk | 22 (9.3) |
| Higher risk | 79 (33.3) |
| Much higher risk | 129 (54.5) |
| Believe TB screening is beneficial for their family | |
| Neither agree nor disagree | 1 (0.4) |
| Agree | 35 (14.8) |
| Strongly agree | 201 (84.8) |
| What would you do if you had symptoms of TB? | |
| Go to health facility | 232 (97.9) |
| Go to pharmacy | 4 (1.7) |
| Go to traditional healer | 1 (0.4) |
| When would you to go to a health facility if you had TB symptoms? | |
| When symptoms that look like TB signs last for 3–4 weeks | 56 (23.6) |
| As soon as I realise that my symptoms might be related to TB | 181 (76.4) |
| Number | 30 |
| I didn’t attend the clinic appointment because: | |
| The distance to travel from my home to preventative district health centre is too far | 1 (3.3) |
| I am worried about discrimination from other people toward myself and my family | 2 (6.7) |
| It is time-consuming. It was difficult to get time off work or study | 27 (90.0) |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| Odds Ratio * | 95% CI | p Value | Odds Ratio * | 95% CI | p Value | |
| Age | 0.19 | 1.03–1.15 | 0.001 | ** | - | - |
| Male (1: male, 0: female) | 3.47 | 1.16–10.31 | 0.026 | 0.49 | 0.06–3.93 | 0.505 |
| Malaysian (1: Malaysian, 0: non-Malaysian) | 0.17 | 0.04–0.74 | 0.018 | 0.74 | 0.26–21.35 | 0.863 |
| Low educational status (1: low education, 0: higher education) | 7.63 | 1.77–32.93 | 0.006 | 0.35 | 0.01–11.95 | 0.559 |
| Student (1: non-student, 0: student) | 8.49 | 3.71–19.4 | <0.001 | 0.40 | 0.01–19.37 | 0.640 |
| Close relative (1: close relative, 0: other) | 101.5 | 13.5–765.3 | <0.001 | 41.77 | 3.28–531.22 | 0.004 |
| Married (1: married, 0: single) | 3.80 | 1.56–9.24 | 0.003 | 0.43 | 0.59–1.09 | 0.396 |
| Income status (1: income>1000 RM, 0: income <1000 RM) | 2.36 | 1.03–5.38 | 0.042 | 1.82 | 0.06–51.4 | 0.729 |
| Household occupancy (continuous variable between 1 and 15) | 0.83 | 0.70–0.97 | 0.020 | 0.81 | 0.60–1.09 | 0.159 |
| Perception of stigma (1: yes, 0: no) | 0.15 | 0.05–0.44 | 0.001 | ** | - | - |
| Whether the respondent would delay clinic attendance if TB symptoms were present (1: go quickly, 0: delay 3–4 weeks) | 0.46 | 0.15–1.38 | 0.164 | - | - | - |
| Distance to clinic (1: 0-9km, 0: ≥10km) | 0.33 | 0.07–1.44 | 0.140 | - | - | - |
| How the respondent was informed (1: letter, phone, visit, 0: notification to work/school) | 128.05 | 37.45–437.89 | <0.001 | 89.3 | 11.1–149.10 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goroh, M.M.D.; van den Boogaard, C.H.A.; Ibrahim, M.Y.; Tha, N.O.; Swe; Robinson, F.; Lukman, K.A.; Jeffree, M.S.; William, T.; Ralph, A.P. Factors Affecting Continued Participation in Tuberculosis Contact Investigation in a Low-Income, High-Burden Setting. Trop. Med. Infect. Dis. 2020, 5, 124. https://doi.org/10.3390/tropicalmed5030124
Goroh MMD, van den Boogaard CHA, Ibrahim MY, Tha NO, Swe, Robinson F, Lukman KA, Jeffree MS, William T, Ralph AP. Factors Affecting Continued Participation in Tuberculosis Contact Investigation in a Low-Income, High-Burden Setting. Tropical Medicine and Infectious Disease. 2020; 5(3):124. https://doi.org/10.3390/tropicalmed5030124
Chicago/Turabian StyleGoroh, Michelle May D., Christel H.A. van den Boogaard, Mohd Yusof Ibrahim, Naing Oo Tha, Swe, Fredie Robinson, Khamisah Awang Lukman, Mohammad Saffree Jeffree, Timothy William, and Anna P. Ralph. 2020. "Factors Affecting Continued Participation in Tuberculosis Contact Investigation in a Low-Income, High-Burden Setting" Tropical Medicine and Infectious Disease 5, no. 3: 124. https://doi.org/10.3390/tropicalmed5030124
APA StyleGoroh, M. M. D., van den Boogaard, C. H. A., Ibrahim, M. Y., Tha, N. O., Swe, Robinson, F., Lukman, K. A., Jeffree, M. S., William, T., & Ralph, A. P. (2020). Factors Affecting Continued Participation in Tuberculosis Contact Investigation in a Low-Income, High-Burden Setting. Tropical Medicine and Infectious Disease, 5(3), 124. https://doi.org/10.3390/tropicalmed5030124