Purified Vero Cell Rabies Vaccine (PVRV, Verorab®): A Systematic Review of Intradermal Use Between 1985 and 2019


Abstract
1. Introduction
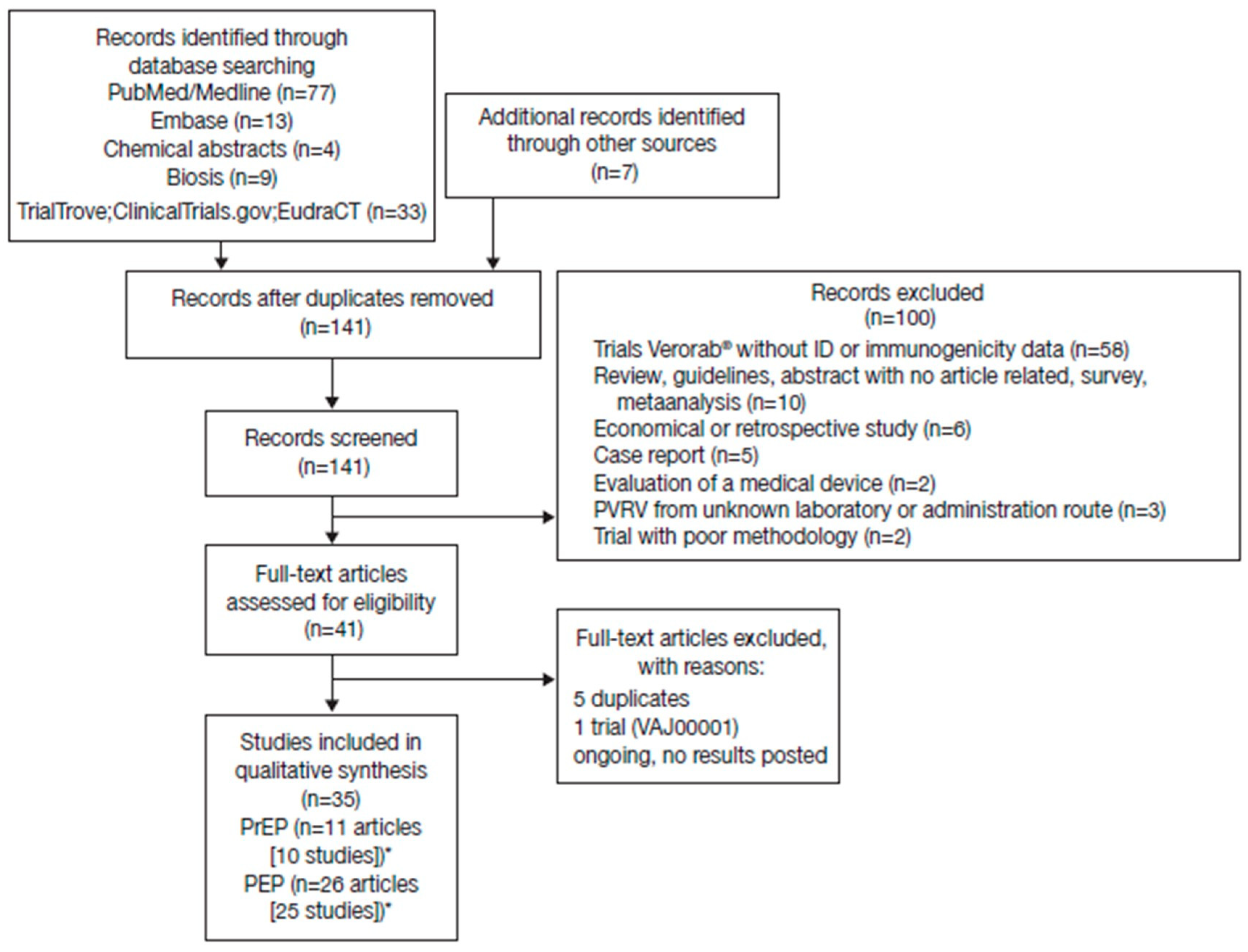
2. Materials and Methods
3. Results
3.1. Immunogenicity of PrEP Regimens
3.1.1. Immunogenicity Up to 1 Year
3.1.2. Booster Responses
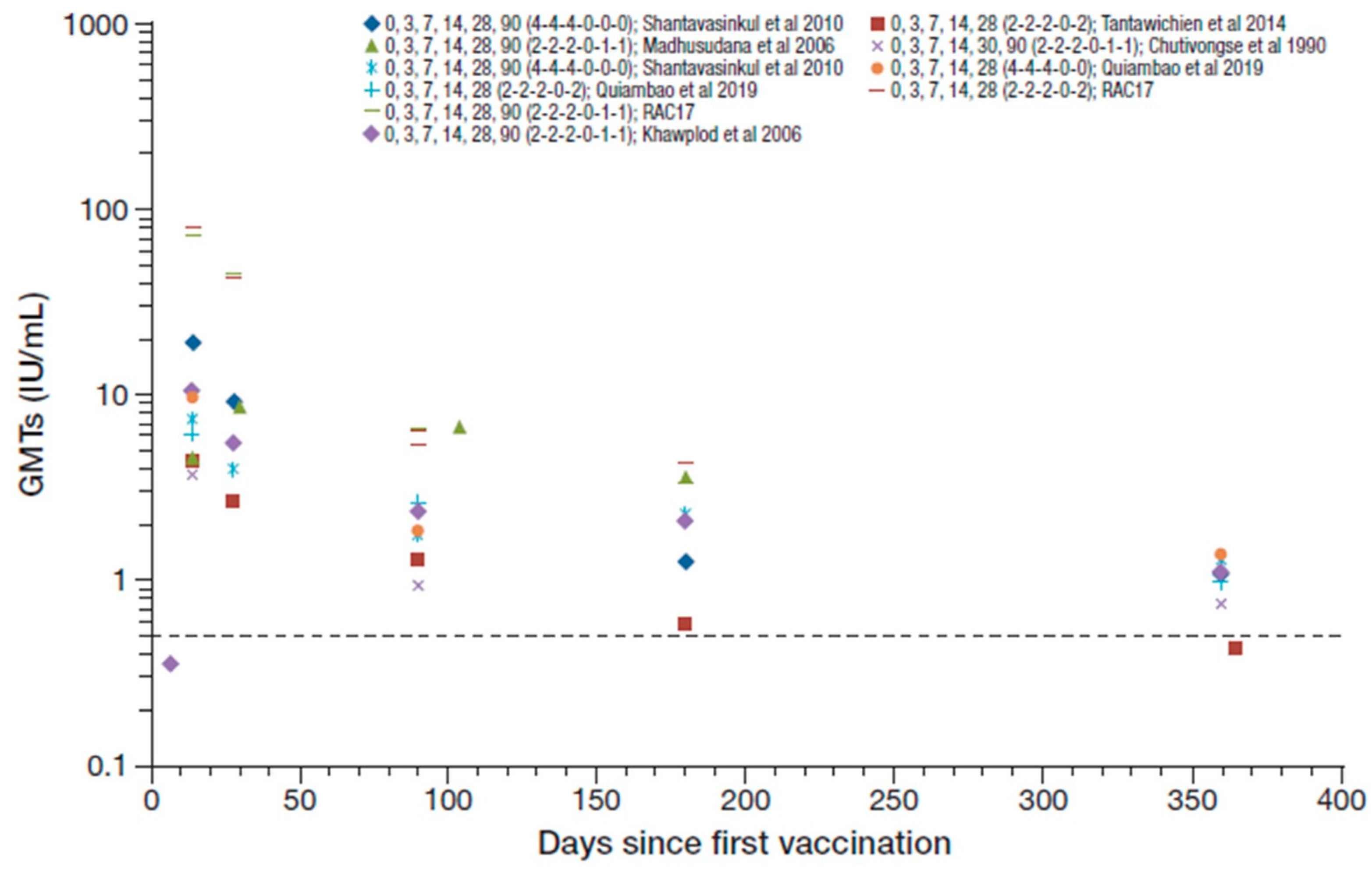
3.2. Immunogenicity of PEP Regimens
3.2.1. Immunogenicity Up to 1 Year
3.2.2. Persistence of PEP Immunogenicity
3.2.3. Booster Response
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fooks, A.R.; Cliquet, F.; Finke, S.; Freuling, C.; Hemachudha, T.; Mani, R.S.; Muller, T.; Nadin-Davis, S.; Picard-Meyer, E.; Wilde, H.; et al. Rabies. Nat. Rev. Dis. Prim. 2017, 3, 17091. [Google Scholar] [CrossRef]
- Wunner, W.H.; Briggs, D.J. Rabies in the 21 century. PLoS Negl. Trop. Dis. 2010, 4, e591. [Google Scholar] [CrossRef]
- Hampson, K.; Cleaveland, S.; Briggs, D. Evaluation of cost-effective strategies for rabies post-exposure vaccination in low-income countries. PLoS Negl. Trop. Dis. 2011, 5, e982. [Google Scholar] [CrossRef]
- World Health Organization. Rabies vaccines: WHO position paper—April 2018. Wkly. Epidemiol. Rec. 2018, 16, 201–220. [Google Scholar]
- World Health Organization. Rabies. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/rabies (accessed on 16 September 2019).
- World Health Organization. Frequently Asked Questions about Rabies for the General Public. 2018. Available online: https://www.who.int/rabies/Rabies_General_Public_FAQs_21Sep2018.pdf?ua=1 (accessed on 16 September 2019).
- Yamamoto, S.; Iwasaki, C.; Oono, H.; Ninomiya, K.; Matsumura, T. The first imported case of rabies into Japan in 36 years: A forgotten life-threatening disease. J. Travel Med. 2008, 15, 372–374. [Google Scholar] [CrossRef]
- Smith, J.; McElhinney, L.; Parsons, G.; Brink, N.; Doherty, T.; Agranoff, D.; Miranda, M.E.; Fooks, A.R. Case report: Rapid ante-mortem diagnosis of a human case of rabies imported into the UK from the Philippines. J. Med. Virol. 2003, 69, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Hicks, D.J.; Fooks, A.R.; Johnson, N. Developments in rabies vaccines. Clin. Exp. Immunol. 2012, 169, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Smith, T.G.; Rupprecht, C.E. From brain passage to cell adaptation: The road of human rabies vaccine development. Expert Rev. Vaccines 2011, 10, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.M. Louis Pasteur and rabies: A brief note. J. Neurol. Neurosurg. Psychiatry 2002, 73, 82. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Rabies. 2015. Available online: https://www.who.int/biologicals/vaccines/rabies/en/ (accessed on 25 November 2019).
- World Health Organization. WHO Expert Consultation on Rabies. Second report. WHO Technical Report Series No. 982. 2013. Available online: https://apps.who.int/iris/handle/10665/85346 (accessed on 16 September 2019).
- Gongal, G.; Sampath, G. Introduction of intradermal rabies vaccination—A paradigm shift in improving post-exposure prophylaxis in Asia. Vaccine 2018. [Google Scholar] [CrossRef]
- Tarantola, A.; Tejiokem, M.C.; Briggs, D.J. Evaluating new rabies post-exposure prophylaxis (PEP) regimens or vaccines. Vaccine 2019, 37 (Suppl. 1), A88–A93. [Google Scholar] [CrossRef]
- Jonker, E.F.F.; Visser, L.G. Single visit rabies pre-exposure priming induces a robust anamnestic antibody response after simulated post-exposure vaccination: Results of a dose-finding study. J. Travel Med. 2017, 24. [Google Scholar] [CrossRef] [PubMed]
- Pichon, S.; Guinet-Morlot, F.; Minutello, M.; Donazzolo, Y.; Rouzier, R.; Chassard, D.; Fitoussi, S.; Hou, V. A serum-free, purified vero cell rabies vaccine is safe and as immunogenic as the reference vaccine Verorab for pre-exposure use in healthy adults: Results from a randomized controlled phase-II trial. Vaccine 2013, 31, 2295–2301. [Google Scholar] [CrossRef] [PubMed]
- Toovey, S. Preventing rabies with the Verorab vaccine: 1985-2005 Twenty years of clinical experience. Travel Med. Infect. Dis. 2007, 5, 327–348. [Google Scholar] [CrossRef] [PubMed]
- Centre for Reviews and Dissemination. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care. University of York: York, UK, 2006. Available online: https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf (accessed on 25 October 2019).
- Wongsaroj, P.; Udomchaisakul, P.; Tepsumethanon, S.; Khawplod, P.; Tantawichien, T. Rabies neutralizing antibody after 2 intradermal doses on days 0 and 21 for pre-exposure prophylaxis. Vaccine 2013, 31, 1748–1751. [Google Scholar] [CrossRef]
- De Pijper, C.A.; Boersma, J.; Terryn, S.; Van Gucht, S.; Goorhuis, A.; Grobusch, M.P.; Stijnis, C. Rabies antibody response after two intradermal pre-exposure prophylaxis immunizations: An observational cohort study. Travel Med. Infect. Dis. 2018, 22, 36–39. [Google Scholar] [CrossRef]
- Cunha, R.S.; Silva Ade, C.; Batista, A.M.; Chaves, L.B.; Barata, R.B. Equivalence between pre-exposure schemes for human rabies and evaluation of the need for serological monitoring. Rev. Saude Publica 2010, 44, 548–554. [Google Scholar] [CrossRef]
- Sabchareon, A.; Chantavanich, P.; Pasuralertsakul, S.; Pojjaroen-Anant, C.; Prarinyanupharb, V.; Attanath, P.; Singhasivanon, V.; Buppodom, W.; Lang, J. Persistence of antibodies in children after intradermal or intramuscular administration of preexposure primary and booster immunizations with purified Vero cell rabies vaccine. Pediatr. Infect. Dis. J. 1998, 17, 1001–1007. [Google Scholar] [CrossRef]
- Lang, J.; Hoa, D.Q.; Gioi, N.V.; Vien, N.C.; Nguyen, C.V.; Rouyrre, N.; Forrat, R. Immunogenicity and safety of low-dose intradermal rabies vaccination given during an Expanded Programme on immunization session in Viet Nam: Results of a comparative randomized trial. Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 208–213. [Google Scholar] [CrossRef]
- Khawplod, P.; Wilde, H.; Benjavongkulchai, M.; Sriaroon, C.; Chomchey, P. Immunogenicity study of abbreviated rabies preexposure vaccination schedules. J. Travel Med. 2007, 14, 173–176. [Google Scholar] [CrossRef]
- Khawplod, P.; Benjavongkulchai, M.; Limusanno, S.; Chareonwai, S.; Kaewchompoo, W.; Tantawichien, T.; Wilde, H. Four-site intradermal postexposure boosters in previously rabies vaccinated subjects. J. Travel Med. 2002, 9, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Vien, N.C.; Feroldi, E.; Lang, J. Long-term anti-rabies antibody persistence following intramuscular or low- dose intradermal vaccination of young Vietnamese children. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Tantawichien, T.; Benjavongkulchai, M.; Limsuwan, K.; Khawplod, P.; Kaewchompoo, W.; Chomchey, P.; Sitprija, V. Antibody response after a four-site intradermal booster vaccination with cell-culture rabies vaccine. Clin. Infect. Dis. 1999, 28, 1100–1103. [Google Scholar] [CrossRef] [PubMed]
- Angsuwatcharakon, P.; Ratananpinit, N.; Yoksan, S.; Saengseesom, W.; Sriaksorn, R.; Raksahket, N.; Tantawichien, T. Immunogenicity and safety of a double-dose, two-visit, pre-exposure rabies prophylaxis regimen versus a conventional regimen with Vero cell rabies and concomitant chimeric live-attenuated Japanese encephalitis vaccine administration. Vaccine 2019, submitted. [Google Scholar]
- Khawplod, P.; Wilde, H.; Tepsumethanon, S.; Limusanno, S.; Tantawichien, T.; Chomchey, P.; Ayuthaya, A.B.; Wangroonsarb, Y. Prospective immunogenicity study of multiple intradermal injections of rabies vaccine in an effort to obtain an early immune response without the use of immunoglobulin. Clin. Infect. Dis. 2002, 35, 1562–1565. [Google Scholar] [CrossRef]
- Quiambao, B.P.; Ambas, C.; Diego, S.; Bosch Castells, V.; Korejwo, J.; Petit, C.; Rasuli, A.; Houillon, G. A single-visit, 4-site intradermal (ID) rabies vaccination during simulated post-exposure induces a robust immune response 5 years after primary 1-week, 4-site ID post-exposure prophylaxis regimen in the Philippines. Vaccine 2019, submitted. [Google Scholar]
- Kositprapa, C.; Limsuwun, K.; Wilde, H.; Jaijaroensup, W.; Saikasem, A.; Khawplod, P.; Kri-aksorn, U.; Supich, C. Immune response to simulated postexposure rabies booster vaccinations in volunteers who received preexposure vaccinations. Clin. Infect. Dis. 1997, 25, 614–616. [Google Scholar] [CrossRef]
- Tantawichien, T.; Tantawichien, T.; Supit, C.; Khawplod, P.; Sitprija, V. Three-year experience with 4-site intradermal booster vaccination with rabies vaccine for postexposure prophylaxis. Clin. Infect. Dis. 2001, 33, 2085–2087. [Google Scholar] [CrossRef]
- Phanuphak, P.; Khaoplod, P.; Benjavongkulchai, M.; Chutivongse, S.; Wilde, H. What happens if intradermal injections of rabies vaccine are partially or entirely injected subcutaneously? Bull. World Health Organ. 1990, 68, 83–85. [Google Scholar]
- Narayana, A.; Manoharan, A.; Narayan, M.S.; Kalappa, S.M.; Biligumba, G.; Haradanahalli, R.; Anand, A.M. Comparison of safety and immunogenicity of 2 WHO prequalified rabies vaccines administered by one week, 4 site intra dermal regimen (4-4-4-0-0) in animal bite cases. Hum. Vaccines Immunother. 2015, 11, 1748–1753. [Google Scholar] [CrossRef]
- Sudarshan, M.K.; Narayana, D.H.; Madhusudana, S.N.; Holla, R.; Ashwin, B.Y.; Gangaboraiah, B.; Ravish, H.S. Evaluation of a one week intradermal regimen for rabies post-exposure prophylaxis: Results of a randomized, open label, active-controlled trial in healthy adult volunteers in India. Hum. Vaccines Immunother. 2012, 8, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- Tantawichien, T.; Sibunruang, S.; Tantawichien, T.; Angsanakul, J.; Benjavongkulchai, M.; Limsuwan, K.; Udomchaisakul, P.; Khomvilai, S.; Sitprija, V. Safety and immunogenicity of chromatographically purified Vero cell rabies vaccine for intradermal pre- and post-exposure rabies prophylaxis. Expert Rev. Vaccines 2014, 13, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Sampath, G.; Madhusudana, S.N.; Sudarshan, M.K.; Ashwathnarayana, D.H.; Mahendra, B.J.; Ullas, T.P.; Mohan, K.; Madhusudhan, S.K.; Ravish, H.S. Immunogenicity and safety study of Indirab: A Vero cell based chromatographically purified human rabies vaccine. Vaccine 2010, 28, 4086–4090. [Google Scholar] [CrossRef] [PubMed]
- Phanuphak, P.; Khawplod, P.; Sirivichayakul, S.; Siriprasomsub, W.; Ubol, S.; Thaweepathomwat, M. Humoral and cell-mediated immune responses to various economical regimens of purified Vero cell rabies vaccine. Asian Pac. J. Allergy Immunol. 1987, 5, 33–37. [Google Scholar] [PubMed]
- Quiambao, B.P.; Gepanayao, C.; Bermal, N.; Ambas, M.C.; Dy-Tioco, H.; Crisostomo, M.; Dizon, R. Rabies vaccination regimens using purified Vero cell rabies vaccine. APCRI J. 2008, 10, 15–19. [Google Scholar]
- Ambrozaitis, A.; Laiskonis, A.; Balciuniene, L.; Banzhoff, A.; Malerczyk, C. Rabies post-exposure prophylaxis vaccination with purified chick embryo cell vaccine (PCECV) and purified Vero cell rabies vaccine (PVRV) in a four-site intradermal schedule (4-0-2-0-1-1): An immunogenic, cost-effective and practical regimen. Vaccine 2006, 24, 4116–4121. [Google Scholar] [CrossRef] [PubMed]
- Khawplod, P.; Wilde, H.; Sirikwin, S.; Benjawongkulchai, M.; Limusanno, S.; Jaijaroensab, W.; Chiraguna, N.; Supich, C.; Wangroongsarb, Y.; Sitprija, V. Revision of the Thai Red Cross intradermal rabies post-exposure regimen by eliminating the 90-day booster injection. Vaccine 2006, 24, 3084–3086. [Google Scholar] [CrossRef]
- Madhusudana, S.N.; Sanjay, T.V.; Mahendra, B.J.; Suja, M.S. Simulated post-exposure rabies vaccination with purified chick embryo cell vaccine using a modified Thai Red Cross regimen. Int. J. Infect. Dis. 2004, 8, 175–179. [Google Scholar] [CrossRef]
- Tanisaro, T.; Tantawichien, T.; Tiranathanagul, K.; Susantitaphong, P.; Chirananthavat, T.; Praditpornsilpa, K.; Sitprija, V.; Eiam-Ong, S. Neutralizing antibody response after intradermal rabies vaccination in hemodialysis patients. Vaccine 2010, 28, 2385–2387. [Google Scholar] [CrossRef]
- Madhusudana, S.N.; Sanjay, T.V.; Mahendra, B.J.; Sudarshan, M.K.; Narayana, D.H.; Giri, A.; Muhamuda, K.; Ravi, V.; Vakil, H.B.; Malerczyk, C. Comparison of saftey and immunogenicity of purified chick embryo cell rabies vaccine (PCECV) and purified vero cell rabies vaccine (PVRV) using the Thai Red Cross intradermal regimen at a dose of 0.1 ML. Hum. Vaccines 2006, 2, 200–204. [Google Scholar] [CrossRef]
- Chutivongse, S.; Wilde, H.; Supich, C.; Baer, G.M.; Fishbein, D.B. Postexposure prophylaxis for rabies with antiserum and intradermal vaccination. Lancet 1990, 335, 896–898. [Google Scholar] [CrossRef]
- Briggs, D.J.; Banzhoff, A.; Nicolay, U.; Sirikwin, S.; Dumavibhat, B.; Tongswas, S.; Wasi, C. Antibody response of patients after postexposure rabies vaccination with small intradermal doses of purified chick embryo cell vaccine or purified Vero cell rabies vaccine. Bull. World Health Organ. 2000, 78, 693–698. [Google Scholar] [PubMed]
- Shantavasinkul, P.; Tantawichien, T.; Wilde, H.; Sawangvaree, A.; Kumchat, A.; Ruksaket, N.; Lohsoonthorn, V.; Khawplod, P.; Tantawichien, T. Postexposure rabies prophylaxis completed in 1 week: Preliminary study. Clin. Infect. Dis. 2010, 50, 56–60. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Warrell, M.J.; Riddell, A.; Yu, L.M.; Phipps, J.; Diggle, L.; Bourhy, H.; Deeks, J.J.; Fooks, A.R.; Audry, L.; Brookes, S.M.; et al. A simplified 4-site economical intradermal post-exposure rabies vaccine regimen: A randomised controlled comparison with standard methods. PLoS Negl. Trop. Dis. 2008, 2, e224. [Google Scholar] [CrossRef]
- Quiambao, B.P.; Ambas, C.; Diego, S.; Bosch Castells, V.; Korejwo, J.; Petit, C.; Houillon, G. Intradermal post-exposure rabies vaccination with purified Vero cell rabies vaccine: Comparison of a one-week, 4-site regimen versus updated Thai Red Cross regimen in a randomized non-inferiority trial in the Philippines. Vaccine 2019, 37, 2268–2277. [Google Scholar] [CrossRef]
- Tantawichien, T.; Jaijaroensup, W.; Khawplod, P.; Sitprija, V. Failure of multiple-site intradermal postexposure rabies vaccination in patients with human immunodeficiency virus with low CD4+ T lymphocyte counts. Clin. Infect. Dis. 2001, 33, E122–E124. [Google Scholar] [CrossRef]
- RAC17. Clinical Study Report. Combined immunogenicity of Chromatographically Purified Rabies Vaccine (CPRV, with and without Merthiolate) and equine rabies immune globulin (ERIG), in comparison with Purified Vero Rabies Vaccine (PVRV) and ERIG, administered by intradermal route, in subjects with a WHO Category I, II, or III Rabies exposure. Unpublished work. 13 March 2002. [Google Scholar]
- Cantaert, T.; Borand, L.; Kergoat, L.; Leng, C.; Ung, S.; In, S.; Peng, Y.; Phoeun, C.; Hing, C.; Taing, C.N.; et al. A 1-week intradermal dose-sparing regimen for rabies post-exposure prophylaxis (RESIST-2): An observational cohort study. Lancet Infect. Dis. 2019. [Google Scholar] [CrossRef]
- Buchy, P.; Preiss, S.; Singh, V.; Mukherjee, P. Heterogeneity of Rabies Vaccination Recommendations across Asia. Trop. Med. Infect. Dis. 2017, 2, 23. [Google Scholar] [CrossRef]
- World Health Organization. WHO Expert Consultation on Rabies, Third Report: WHO Technical Report Series, No. 1012. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/272364/9789241210218-eng.pdf (accessed on 16 September 2019).
- Kessels, J.; Tarantola, A.; Salahuddin, N.; Blumberg, L.; Knopf, L. Rabies post-exposure prophylaxis: A systematic review on abridged vaccination schedules and the effect of changing administration routes during a single course. Vaccine 2019, 37 (Suppl. 1), A107–A117. [Google Scholar] [CrossRef]
- Angsuwatcharakon, P. Neutralizing Immunogenicity Antibody After 2 Intradermal Doses Pre-Exposure Prophylaxis of Purified Vero Cell Rabies Vaccine (PVRV) to 12–24 month-old Children, concomitantly with Chimeric Live-Attenuated JE Vaccine (IMOJEV). Unpublished data. 2018. [Google Scholar]
- Langedijk, A.C.; De Pijper, C.A.; Spijker, R.; Holman, R.; Grobusch, M.P.; Stijnis, C. Rabies Antibody Response After Booster Immunization: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2018, 67, 1932–1947. [Google Scholar] [CrossRef]
- Kessels, J.A.; Recuenco, S.; Navarro-Vela, A.M.; Deray, R.; Vigilato, M.; Ertl, H.; Durrheim, D.; Rees, H.; Nel, L.H.; Abela-Ridder, B.; et al. Pre-exposure rabies prophylaxis: A systematic review. Bull. World Health Organ. 2017, 95, 210C–219C. [Google Scholar] [CrossRef] [PubMed]
- Hampson, K.; Abela-Ridder, B.; Bharti, O.; Knopf, L.; Lechenne, M.; Mindekem, R.; Tarantola, A.; Zinsstag, J.; Trotter, C. Modelling to inform prophylaxis regimens to prevent human rabies. Vaccine 2019, 37 (Suppl. 1), A166–A173. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.M.; Hanlon, C.A. Rabies-specific antibodies: Measuring surrogates of protection against a fatal disease. PLoS Negl. Trop. Dis. 2010, 4, e595. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Regimen; Days (Number of Sites) [n] | Patients/Participants | Source |
|---|---|---|
| 0, 3, 7 (2-2-2) [n = 21] | Simulated PEP (healthy participants) | [26] |
| 0, 3, 7 (4-4-4) [n = 21] | Simulated PEP (healthy participants) | [26] |
| 0, 3, 7 (4-4-4) [n = 40] | Simulated PEP (healthy participants) | [36] |
| 0, 3, 7 (8-0-4) [n = 22] | Simulated PEP (healthy participants) | [26] |
| 0, 3, 7, 14, 28 (2-2-2-0-2) [n = 63] | Simulated PEP (healthy participants) | [38] |
| 0, 3, 7, 14, 28 (2-2-2-0-2) [n = 20] | Simulated PEP (healthy participants) | [53] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 38] | Simulated PEP (healthy participants) | [43] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 58] | Simulated PEP (healthy participants) | [49] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 14] | Simulated PEP (hemodialysis patients) | [44] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-2-2) [n = 10] | Simulated PEP (healthy participants) | [25] |
| 0, 3, 7, 14, 28, 90 (4-0-2-0-1-1) [n = 55] | Simulated PEP (healthy participants) | [49] |
| 0, 3, 7, 14, 30, 90 (4-0-2-0-1-1) [n = 87] | Simulated PEP (healthy participants) | [41] |
| 0, 3, 7, 14, 28, 90 (8-0-4-0-1-1) [n = 58] | Simulated PEP (healthy participants) | [49] |
| 0, 3, 7, 14, 28, 90 (4-4-4-0-0-0) [n = 45] | Simulated PEP (healthy participants) | [48] |
| 0, 3, 7 (2-2-2) [n = 15] | Category I/II | [34] |
| 0, 3, 7 (4-4-4) [n = 182] | Category I | [50] |
| 0, 3, 7, 28 (1-1-1-1) [n = 14] | Category I/II | [39] |
| 0, 3, 7, 28 (2-2-2-2) [n = 15] | Category I/II | [39] |
| 0, 3, 7, 28 (4-4-4-4) [n = 14] | Category I/II | [39] |
| 0, 3, 7, 14, 28, 90 (4-0-2-0-1-1) [n = 96] | Category I/II | [40] |
| 0, 3, 7, 14, 28, 90 (8-0-4-0-1-1) [n = 96] | Category I/II | [40] |
| 0, 3, 7 (4-4-4) [n = 44] | Category II/III/ with or without ERIG groups combined | [35] |
| 0, 3, 7, 14, 28 (4-4-4-0-0) [n = 170] | Category III/concomitant ERIG | [50] |
| 0, 3, 7, 14, 28, 90 (4-4-4-0-0-0) [n = 45] | Simulated PEP (healthy participants)/concomitant ERIG | [48] |
| 0, 3, 7, 14, 28, 90 (4-4-4-0-0-0) [n = 41] | Category III/concomitant ERIG | [48] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 99] | Category I/II/concomitant ERIG | [40] |
| 0, 3, 7, 14, 28 (2-2-2-0-2) [n = 31] | Simulated PEP (healthy participants)/concomitant ERIG | [37] |
| 0, 3, 7, 14, 28 (2-2-2-0-2) [n = 177] | Category III/concomitant ERIG | [50] |
| 0, 3, 7, 14, 28 (2-2-2-0-2) [n = 116] | Category III/concomitant ERIG | [53] |
| 0, 3, 7, 14, 28 (2-2-2-0-2) [n = 82] | Category I–III/concomitant ERIG | [52] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 50] | Category III/concomitant ERIG | [45] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 10] | High risk exposure/concomitant ERIG | [46] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 48] | Category I–III/concomitant ERIG | [52] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 105] | Category III/concomitant HRIG | [42] |
| 0, 3, 7, 14, 28, 90 (2-2-2-0-1-1) [n = 59] | Category II/III/ concomitant HRIG (groups combined) | [47] |
| 0, 3, 7, 14, 30, 90 (4-4-4-0-2-2) [n = 10] | Category III/ HIV patients/concomitant ERIG | [51] |
| 0, 3 (4-0) [n = 20] | Prior PreP 1 year earlier/simulated PEP (booster) | [28] |
| 0, 3 (4-0) [n = 10] | Prior PrEP or PEP 1–10 years earlier/simulatedPEP (booster) | [33] |
| 0, 3 (1-1) [n = 35] | Prior PreP 12–16 month earlier/simulated PEP (booster) | [32] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moulenat, T.; Petit, C.; Bosch Castells, V.; Houillon, G. Purified Vero Cell Rabies Vaccine (PVRV, Verorab®): A Systematic Review of Intradermal Use Between 1985 and 2019. Trop. Med. Infect. Dis. 2020, 5, 40. https://doi.org/10.3390/tropicalmed5010040
Moulenat T, Petit C, Bosch Castells V, Houillon G. Purified Vero Cell Rabies Vaccine (PVRV, Verorab®): A Systematic Review of Intradermal Use Between 1985 and 2019. Tropical Medicine and Infectious Disease. 2020; 5(1):40. https://doi.org/10.3390/tropicalmed5010040
Chicago/Turabian StyleMoulenat, Thomas, Céline Petit, Valérie Bosch Castells, and Guy Houillon. 2020. "Purified Vero Cell Rabies Vaccine (PVRV, Verorab®): A Systematic Review of Intradermal Use Between 1985 and 2019" Tropical Medicine and Infectious Disease 5, no. 1: 40. https://doi.org/10.3390/tropicalmed5010040
APA StyleMoulenat, T., Petit, C., Bosch Castells, V., & Houillon, G. (2020). Purified Vero Cell Rabies Vaccine (PVRV, Verorab®): A Systematic Review of Intradermal Use Between 1985 and 2019. Tropical Medicine and Infectious Disease, 5(1), 40. https://doi.org/10.3390/tropicalmed5010040