Geographical Distribution of β-Lactam Resistance among Klebsiella spp. from Selected Health Facilities in Ghana

 , ,
, ,
Abstract
1. Introduction
2. Materials and Method
2.1. Collection and Identification of Isolates
2.2. Phenotypic Techniques
Antimicrobial Susceptibility Testing (AST)
2.3. Genotypic Techniques
2.4. Data Analysis
3. Results
3.1. Study Population
3.2. Antimicrobial Susceptibility Profile of Isolates
3.3. Phenotypic Distribution of ESBL-, AmpC-, MBL-, and Carbapenemase-Producing Klebsiella Isolate by Specimen Type
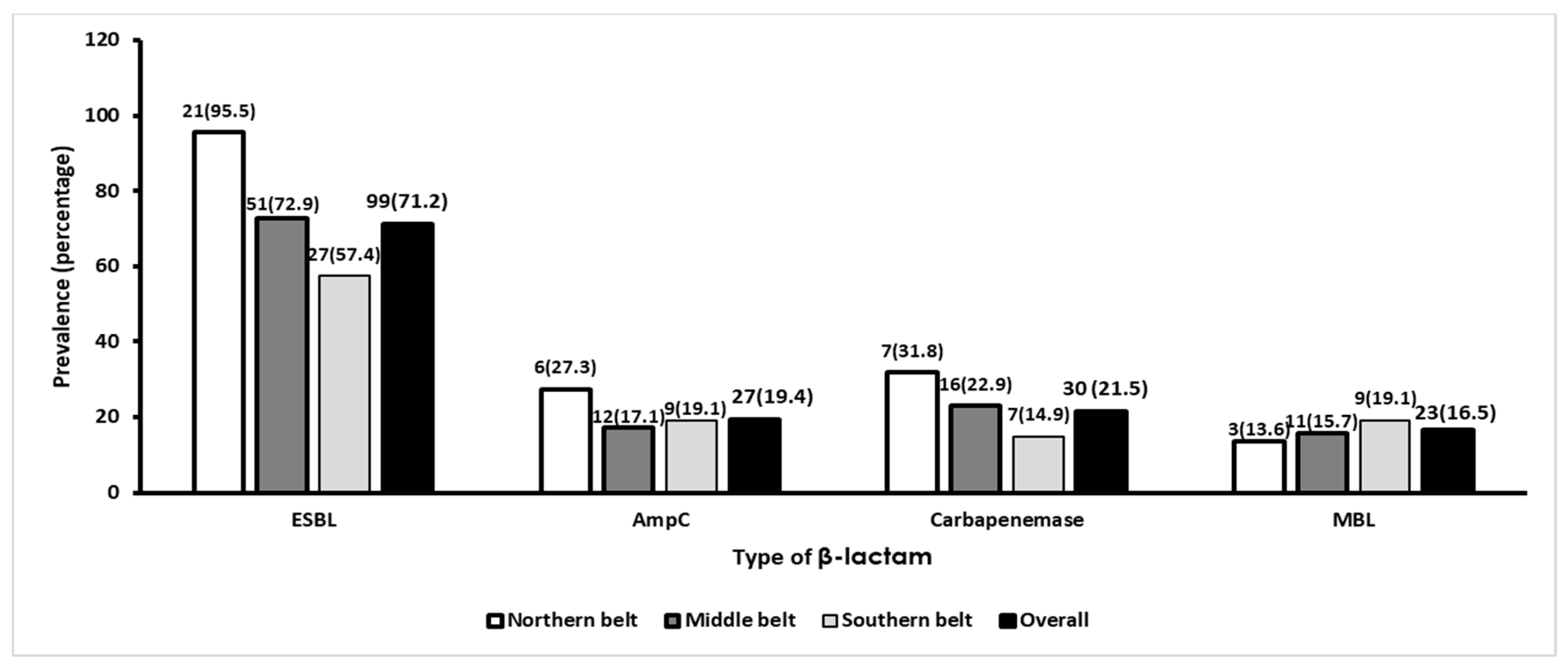
3.4. Phenotypic Distribution of ESBL-, AmpC-, and Carbapenemase-Producing Klebsiella Species by Geographical Location
3.5. Genotypic Distribution of bla ESBL-Encoding Genes in Klebsiella Species
3.6. Distribution of Blacarbapenemase-Positive Isolates
3.7. Agreement between Phenotypic Tests and Genotypic Test
4. Discussion
5. Conclusions
6. Future Perspective
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pitout, J.D.D.; Nordmann, P.; Poirel, L. Carbapenemase-Producing Klebsiella pneumoniae, a Key Pathogen Set for Global Nosocomial Dominance. Antimicrob. Agents Chemother. 2015, 59, 5873–5884. [Google Scholar] [CrossRef] [PubMed]
- Singh, L.; Cariappa, M.; Kaur, M. Klebsiella oxytoca: An emerging pathogen? Med. J. Armed Forces India 2016, 72, S59–S61. [Google Scholar] [CrossRef] [PubMed]
- Agyepong, N.; Govinden, U.; Owusu-Ofori, A.; Essack, S.Y. Multidrug-resistant gram-negative bacterial infections in a teaching hospital in Ghana. Antimicrob. Resist. Infect. Control. 2018, 7, 37. [Google Scholar] [CrossRef] [PubMed]
- Boye, A.; Siakwa, P.M.; Boampong, J.N.; Koffuor, G.A.; Ephraim, R.K.D.; Amoateng, P.; Penu, D. Asymptomatic urinary tract infections in pregnant women attending antenatal clinic in Cape Coast, Ghana. E3 J. Med. Res. 2012, 1, 74–83. [Google Scholar]
- Acquah, S.E.; Quaye, L.; Sagoe, K.; Ziem, J.B.; Bromberger, P.; Amponsem, A. Susceptibility of bacterial etiological agents to commonly-used antimicrobial agents in children with sepsis at the Tamale Teaching Hospital. BMC Infect. Dis. 2013, 13, 89. [Google Scholar] [CrossRef] [PubMed]
- Codjoe, F.S.; Donkor, E.S. Carbapenem Resistance: A Review. Med. Sci. 2018, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Thomson, K.S. Controversies about extended-spectrum and AmpC beta-lactamases. Emerg. Infect. Dis. 2001, 7, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Tzouvelekis, L.S.; Markogiannakis, A.; Psichogiou, M.; Tassios, P.T.; Daikos, G.L. Carbapenemases in Klebsiella pneumoniae and Other Enterobacteriaceae: An Evolving Crisis of Global Dimensions. Clin. Microbiol. Rev. 2012, 25, 682–707. [Google Scholar] [CrossRef] [PubMed]
- Livermore, D.M. Bacterial Resistance: Origins, Epidemiology, and Impact. Clin. Infect. Dis. 2003, 36, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, U.; Aggarwal, R. Extended spectrum B-lactamases (ESBL)–An emerging threat to clinical therapeutics. Indian J. Med. Microbiol. 2004, 22, 75–80. [Google Scholar]
- Notake, S.; Matsuda, M.; Tamai, K.; Yanagisawa, H.; Hiramatsu, K.; Kikuchi, K. Detection of IMP Metallo-β-Lactamase in Carbapenem-Nonsusceptible Enterobacteriaceae and Non-Glucose-Fermenting Gram-Negative Rods by Immunochromatography Assay. J. Clin. Microbiol. 2013, 51, 1762–1768. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sangare, S.A.; Rondinaud, E.; Maataoui, N.; Maiga, A.I.; Guindo, I.; Camara, N.; Dicko, O.A.; Dao, S.; Diallo, S.; Bougoudogo, F.; et al. Very high prevalence of extended-spectrum beta-lactamase-producing Enterobacteriaceae in bacteriemic patients hospitalized in teaching hospitals in Bamako, Mali. PLoS ONE 2017, 12, e0172652. [Google Scholar] [CrossRef] [PubMed]
- Ouedraogo, A.-S.; Sanou, M.; Kissou, A.; Sanou, S.; Solaré, H.; Kaboré, F.; Poda, A.; Aberkane, S.; Bouzinbi, N.; Sano, I.; et al. High prevalence of extended-spectrum ß-lactamase producing enterobacteriaceae among clinical isolates in Burkina Faso. BMC Infect. Dis. 2016, 16, 2. [Google Scholar] [CrossRef] [PubMed]
- Okoche, D.; Asiimwe, B.B.; Katabazi, F.A.; Kato, L.; Najjuka, C.F. Prevalence and Characterization of Carbapenem-Resistant Enterobacteriaceae Isolated from Mulago National Referral Hospital, Uganda. PLoS ONE 2015, 10, e0135745. [Google Scholar] [CrossRef] [PubMed]
- Poirel, L.; Revathi, G.; Bernabeu, S.; Nordmann, P. Detection of NDM-1-producing Klebsiella pneumoniae in Kenya. Antimicrob. Agents Chemother. 2011, 55, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Brink, A.J.; Coetzee, J.; Clay, C.G.; Sithole, S.; Richards, G.A.; Poirel, L.; Nordmann, P. Emergence of New Delhi Metallo-Beta-Lactamase (NDM-1) and Klebsiella pneumoniae Carbapenemase (KPC-2) in South Africa. J. Clin. Microbiol. 2012, 50, 525. [Google Scholar] [CrossRef] [PubMed]
- Feglo, P.; Adu-Sarkodie, Y. Antimicrobial Resistance Patterns of Extended Spectrum Β-Lactamase Producing Klebsiellae and E. coli Isolates from a Tertiary Hospital in Ghana. Eur. Sci. J. ESJ 2016, 12, 12. [Google Scholar]
- Feglo, P.; Adu-Sarkodie, Y.; Ayisi, L.; Jain, R.; Spurbeck, R.R.; Springman, A.C.; Walk, S.T. Emergence of a Novel Extended-Spectrum-β-Lactamase (ESBL)-Producing, Fluoroquinolone-Resistant Clone of Extraintestinal Pathogenic Escherichia Coli in Kumasi, Ghana. J. Clin. Microbiol. 2013, 51, 728–730. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Opoku, S.; Feglo, P. AmpC beta-lactamase production among Pseudomonas aeruginosa and Proteus mirabilis isolates at the Komfo Anokye Teaching Hospital, Kumasi, Ghana. J. Microbiol. Antimicrob. 2014, 6, 13–20. [Google Scholar]
- Eibach, D.; Campos, C.B.; Krumkamp, R.; Al-Emran, H.M.; Dekker, D.; Boahen, K.G.; Kreuels, B.; Adu-Sarkodie, Y.; Aepfelbacher, M.; Park, S.E.; et al. Extended spectrum beta-lactamase producing Enterobacteriaceae causing bloodstream infections in rural Ghana, 2007–2012. Int. J. Med Microbiol. 2016, 306, 249–254. [Google Scholar] [CrossRef]
- United Nations. Ghana Country Analysis. 2010. Available online: https://www.undp.org/content/dam/ghana/docs/UNDAF/UNDP_GH_IG_GhanaCountryAnalysis2010_10102013.pdf.pdf (accessed on 2 March 2019).
- Environmental Protection Agency. Ghana’s Second National Communication (GSNC) to the UNFCCC; United Nations Development Programme: New York, NY, USA, 2011. [Google Scholar]
- Blair, J.M.A. A climate for antibiotic resistance. Nat. Clim. Chang. 2018, 8, 460–461. [Google Scholar] [CrossRef]
- MacFadden, D.R.; McGough, S.F.; Fisman, D.; Santillana, M.; Brownstein, J.S. Antibiotic Resistance Increases with Local Temperature. Nat. Clim. Chang. 2018, 8, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.S.; Dias, R.C.D.S.; De Castro, A.C.D.; Riley, L.W.; Moreira, B.M. Identification of Clinical Isolates of Indole-Positive and Indole-Negative Klebsiella spp. J. Clin. Microbiol. 2006, 44, 3640–3646. [Google Scholar] [CrossRef] [PubMed]
- CSLI. Performance Standards for Antimicrobial Susceptibility Testing; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2017. [Google Scholar]
- Sageerabanoo, S.; Malini, A.; Mangaiyarkarasi, T.; Hemalatha, G. Phenotypic detection of extended spectrum β-lactamase and Amp-C β-lactamase producing clinical isolates in a Tertiary Care Hospital: A preliminary study. J. Nat. Sci. Boil. Med. 2015, 6, 383–387. [Google Scholar]
- Maraskolhe, D.; Deotale, V.; Mendiratta, D.; Narang, P. Comparision of Three Laboratory Tests for Detection of AmpC β Lactamases in Klebsiella Species and E. Coli. J. Clin. Diagn. Res. 2014, 8, DC05–DC08. [Google Scholar] [PubMed]
- Anwar, M.; Ejaz, H.; Zafar, A.; Hamid, H. Phenotypic Detection of Metallo-Beta-Lactamases in Carbapenem Resistant Acinetobacter baumannii Isolated from Pediatric Patients in Pakistan. J. Pathog. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, J.K.; Anderson, G.J.; Yigit, H.; Queenan, A.M.; Doménech-Sánchez, A.; Swenson, J.M.; Tenover, F.C. Characterization of the Extended-Spectrum β-Lactamase Reference Strain, Klebsiella pneumoniae/K6 (ATCC 700603), Which Produces the Novel Enzyme SHV-18. Antimicrob. Agents Chemother. 2000, 44, 2382–2388. [Google Scholar] [CrossRef]
- ElHariri, M.; Hamza, D.; Elhelw, R.; Dorgham, S.M. Extended-spectrum beta-lactamase-producing Pseudomonas aeruginosa in camel in Egypt: Potential human hazard. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 710. [Google Scholar] [CrossRef]
- Zhang, J.; Zheng, B.; Zhao, L.; Wei, Z.; Ji, J.; Li, L.; Xiao, Y. Nationwide high prevalence of CTX-M and an increase of CTX-M-55 in Escherichia coli isolated from patients with community-onset infections in Chinese county hospitals. BMC Infect. Dis. 2014, 14, 659. [Google Scholar] [CrossRef]
- Fallah, F.; Noori, M.; Hashemi, A.; Goudarzi, H.; Karimi, A.; Erfanimanesh, S.; Alimehr, S. Prevalence of bla NDM, bla PER, bla VEB, bla IMP, and bla VIM Genes among Acinetobacter baumannii Isolated from Two Hospitals of Tehran, Iran. Sci. 2014, 2014, 1–6. [Google Scholar]
- Mushi, M.F.; Mshana, S.E.; Imirzalioglu, C.; Bwanga, F. Carbapenemase Genes among Multidrug Resistant Gram Negative Clinical Isolates from a Tertiary Hospital in Mwanza, Tanzania. BioMed Res. Int. 2014, 2014, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jia, W.; Li, C.; Zhang, H.; Li, G.; Liu, X.; Wei, J. Prevalence of Genes of OXA-23 Carbapenemase and AdeABC Efflux Pump Associated with Multidrug Resistance of Acinetobacter baumannii Isolates in the ICU of a Comprehensive Hospital of Northwestern China. Int. J. Environ. Res. Public Heal. 2015, 12, 10079–10092. [Google Scholar] [CrossRef] [PubMed]
- Soudeiha, M.A.H.; Dahdouh, E.A.; Azar, E.; Sarkis, D.K.; Daoud, Z. In vitro Evaluation of the Colistin-Carbapenem Combination in Clinical Isolates of A. baumannii Using the Checkerboard, Etest, and Time-Kill Curve Techniques. Front. Microbiol. 2017, 7, 209. [Google Scholar]
- Opintan, J.; Newman, M.J.; Arhin, R.E.; Donkor, E.S.; Gyansa-Lutterodt, M.; Mills-Pappoe, W. Laboratory-based nationwide surveillance of antimicrobial resistance in Ghana. Infect. Drug Resist. 2015, 8, 379–389. [Google Scholar] [CrossRef] [PubMed]
- USAID. Ghana Climate Change Vulnerability and Adaptation Assessment. 2011. Available online: https://www.climatelinks.org/sites/default/files/asset/document/Climate%20Change%20Assessment_Ghana_%20FINAL.pdf (accessed on 2 March 2019).
- Alividza, V.; Mariano, V.; Ahmad, R.; Charani, E.; Rawson, T.M.; Holmes, A.H.; Castro-Sánchez, E. Investigating the impact of poverty on colonization and infection with drug-resistant organisms in humans: A systematic review. Infect. Dis. Poverty 2018, 7, 76. [Google Scholar] [CrossRef] [PubMed]
- Miller-Petrie, M.; Gelband, H. Socioeconomics, Antimicrobial Use and Antimicrobial Resistance. 2017. Available online: http://resistancecontrol.info/2017/socioeconomics-antimicrobial-use-and-antimicrobial-resistance/ (accessed on 2 March 2019).
- Codjoe, F.S. Detection and Characterisation of Carbapenem-Resistant Gram-Negative Bacilli Infections in Ghana; Sheffield Hallam University: Sheffield, UK, 2016. [Google Scholar]
- Ben Nasr, A.; Decré, D.; Compain, F.; Genel, N.; Barguellil, F.; Arlet, G. Emergence of NDM-1 in Association with OXA-48 in Klebsiella pneumoniae from Tunisia. Antimicrob. Agents Chemother. 2013, 57, 4089–4090. [Google Scholar] [CrossRef] [PubMed]
- Robberts, F.J.L.; Kohner, P.C.; Patel, R. Unreliable Extended-Spectrum β-Lactamase Detection in the Presence of Plasmid-Mediated AmpC in Escherichia Coli Clinical Isolates. J. Clin. Microbiol. 2009, 47, 358–361. [Google Scholar] [CrossRef]


{kind=link}
| Name | Primer Sequence (5’→3’) | Amplicon Size (bp) | Reference |
|---|---|---|---|
| TEM | Forward-ATGAGTATTCAACATTTCCG Reverse-TTACCAATGCTTAATCAGTGAG | 861 | [31] |
| SHV | Forward-TCAGCGAAAAACACCTTG Reverse-TCCCGCAGATAAATCACCA | 472 | [31] |
| CTX-M | Forward-GCGATGGGCAGTACCAGTAA Reverse-TTACCCAGCGTCAGATTCCG | 392 | [31] |
| KPC | Forward-CATTCAAGGGCTTTCTTGCTGC Reverse-ACGACGGCATAGTCATTTGC | 538 | [32] |
| NDM | Forward-GGTTTGGCGATCTGGTTTTC Reverse-CGGAATGGCTCATCACGATC | 521 | [33] |
| IMP | Forward-TTGACACTCCATTTACAG Reverse-GATTGAGAATTAAGCCACTCT | 232 | [34] |
| VIM | Forward-TTATGGAGCAACCGATGT Reverse-CAAAAGTCCCGCTCCAACGA | 920 | [35] |
| OXA-48 | Forward-GCTTGATCGCCCTCGATT Reverse-GATTTGCTCCGTTGGCCAAA | 281 | [36] |
| Facility | Specimen n (%) | Total | |||||
|---|---|---|---|---|---|---|---|
| Blood | HVS | Sputum | Urine | Wound Swab | Others * | ||
| Northern belt | |||||||
| TTH | |||||||
| Klebsiella oxytoca | 0 | 0 | 2 (66.7) | 2 (50.0) | 0 | 0 | 4 (40.0) |
| Klebsiella pneumoniae | 1 (100) | 1 (100) | 1 (33.3) | 2 (50.0) | 0 | 1 (100) | 6 (60.0) |
| BRH | |||||||
| Klebsiella oxytoca | 0 | 0 | 0 | 3 (30.0) | 0 | 1 (50.0) | 4 (33.3) |
| Klebsiella pneumoniae | 0 | 0 | 0 | 7 (70.0) | 0 | 1 (50.0) | 8 (66.7) |
| Middle belt | |||||||
| KATH | |||||||
| Klebsiella oxytoca | 3 (21.4) | 0 | 2 (20.0) | 13 (39.4) | 2 (20.0) | 0 | 20 (28.6) |
| Klebsiella pneumoniae | 11 (78.6) | 0 | 8 (80.0) | 20 (60.6) | 8 (80.0) | 3 (100) | 50 (71.4) |
| Southern belt | |||||||
| CCTH | |||||||
| Klebsiella oxytoca | 1 (33.3) | 3 (100) | 0 | 3 (37.5) | 3 (50.0) | 0 | 10 (47.6) |
| Klebsiella pneumoniae | 2 (66.7) | 0 | 0 | 5 (62.5) | 3 (50.0) | 1 (100) | 11 (52.4) |
| EFNTH | |||||||
| Klebsiella oxytoca | 0 | 2 (25.0) | 3 (42.9) | 3 (37.5) | 2 (100) | 0 | 10 (38.5) |
| Klebsiella pneumoniae | 0 | 6 (75.0) | 4 (57.1) | 5 (62.5) | 0 | 1 (100) | 16 (61.5) |
| Total | 18 (100) | 12 (100) | 20 (100) | 63 (100) | 18 (100) | 8 (100) | 139 (100) |
| Variable | K. oxytoca (n = 48) | p-Value | K. pneumoniae (n = 91) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| R n (%) | I n (%) | S n (%) | R n (%) | I n (%) | S n (%) | |||
| β-lactams | ||||||||
| Penicillin | ||||||||
| Ampicillin | 47 (97.9) | 1 (2.1) | 0 (0.0) | <0.001 | 91 (100) | 0 (0.0) | 0 (0.0) | <0.001 |
| 3rd-gen cephalosporin | ||||||||
| Ceftriaxone | 40 (83.3) | 3 (6.3) | 5 (10.4) | <0.001 | 83 (91.2) | 7 (7.7) | 1 (1.1) | <0.001 |
| Cefotaxime | 44 (91.7) | 2 (4.2) | 2 (4.2) | <0.001 | 70 (76.9) | 8 (8.8) | 13 (14.3) | <0.001 |
| Ceftazidime | 38 (79.2) | 4 (8.3) | 6 (12.5) | <0.001 | 65 (71.4) | 15 (16.5) | 11 (12.1) | <0.001 |
| 2nd-gen cephalosporin | ||||||||
| Cefuroxime | 42 (87.5) | 3 (6.3) | 3 (6.3) | <0.001 | 90 (98.9) | 1 (2.1) | 0 (0.0) | <0.001 |
| Cefoxitin | 18 (37.5) | 11 (22.9) | 19 (39.5) | 0.168 | 31 (36.5) | 24 (28.2) | 30 (35.3) | 0.480 |
| Cefotetan | 14 (29.2) | 1 (2.1) | 33 (68.8) | <0.001 | 18 (19.8) | 4 (4.4) | 69 (75.8) | <0.001 |
| Carbapenem | ||||||||
| Meropenem | 18 (37.5) | 9 (18.8) | 21 (43.8) | 0.026 | 27 (29.7) | 25 (27.5) | 39 (42.9) | 0.059 |
| Imipenem | 5 (10.4) | 0(0.0) | 43 (89.6) | <0.001 | 13 (14.3) | 1 (1.1) | 77 (84.6) | <0.001 |
| Ertapenem | 7 (14.6) | 9 (18.8) | 32 (66.7) | <0.001 | 15 (16.5) | 14 (15.4) | 62 (68.1) | <0.001 |
| Non-β-lactams | ||||||||
| Tetracycline | 41 (85.4) | 3 (6.3) | 4 (8.3) | <0.001 | 77 (84.6) | 1 (1.1) | 13 (14.3) | <0.001 |
| Cotrimoxazole | 43 (89.6) | - | 5 (10.4) | <0.001 | 83 (91.2) | 0 (0.0) | 8 (8.8) | <0.001 |
| Ciprofloxacin | 33 (68.8) | 15 (31.3) | 0 (0.0) | <0.001 | 69 (75.8) | 22 (24.2) | 0 (0.0) | <0.001 |
| Chloramphenicol | 26 (54.2) | 4 (8.3) | 18 (37.5) | <0.001 | 67 (73.6) | 4 (4.4) | 20 (22) | <0.001 |
| Gentamicin | 31 (64.6) | 4 (8.3) | 13 (27.1) | <0.001 | 67 (73.6) | 3 (3.3) | 21 (23.1) | <0.001 |
| Amikacin | 1 (2.1) | 0 (0.0) | 47 (97.9) | <0.001 | 4 (4.4) | 0 (0.0) | 87 (95.6) | <0.001 |
| Resistance Mechanism | Species | Within Species | Total | Blood n = 18 | HVS n = 12 | Sputum n = 20 | Urine n = 63 | Wound Swab n = 18 | Others n = 8 |
|---|---|---|---|---|---|---|---|---|---|
| ESBL producers n = 99 | K.O | 35/48 (72.9) # | 35/99 (35.4) | 4/4 (100) | 2/5 (40.0) | 5/7 (71.4) | 17/24 (70.8) | 6/7 (85.7) | 1/1 (100) |
| K.P | 64/91 (70.3) | 64/99 (64.6) | 9/14 (64.2) | 5/7 (71.4) | 9/13 (69.2) | 29/39 (74.3) | 7/11 (63.6) | 5/7 (71.4) | |
| Overall prevalence (%) | 99/139 (71.2) | (100) | 13/18 (72.2) | 7/12 (58.3) | 14/20 (70.0) | 46/63 (73.0) | 13/18 (72.2) | 6/8 (75.0) | |
| AmpC producers n = 27 | K.O | 8/48 (16.6) # | 8/27 (29.6) | 3/4 (75.0) | 2/5 (40.0) | 0/7 (0) | 3/24 (12.5) | 0/7 (0) | 0/1 (0) |
| K.P | 19/91 (20.8) | 19/27 (70.4) | 1/14 (7.1) | 3/7 (42.9) | 5/13 (38.5) | 7/39 (17.9) | 2/11 (18.1) | 1/7 (14.3) | |
| Overall prevalence (%) | 27/139 (19.4) | (100) | 4/18 (22.2) | 5/12 (41.7) | 5/20 (25.0) | 10/63 (15.9) | 2/18 (11.1) | 1/8 (12.5) | |
| MBL producers n = 23 | K.O | 5/48 (10.4) # | 5/23 (21.7) | 0/4 | 1/5 (20.0) | 2/7 (28.6) | 1/24 (4.1) | 1/7 (14.3) | 0/1 |
| K.P | 18/91 (19.8) | 18/23 (78.3) | 3/14 (21.1) | 3/7 (42.9) | 3/13 (23.1) | 3/39 (7.7) | 4/11 (36.4) | 2/7 (28.6) | |
| Overall prevalence (%) | 23/139 (16.5) | (100) | 3/18 (16.7) | 4/12 (33.3) | 5/20 (25.0) | 4/63 (6.3) | 5/18 (27.8) | 2/8 (25.0) | |
| Carbapenemase producers n = 30 | K.O | 6/48 (12.5) * | 6/30 (20.0) | 0/4 (0) | 1/5 (20.0) | 1/7 (14.3) | 4/24 (16.7) | 0/7 (0) | 0/1 (0) |
| K.P | 24/91 (26.4) | 24/30 (80.0) | 4/14 (28.6) | 3/7(42.9) | 4/13 (30.8) | 12/39 (30.8) | 5/11 (45.5) | 2/7 (28.6) | |
| Overall prevalence (%) | 30/139 (21.6) | (100) | 4/18 (22.2) | 4/12 (33.3) | 5/20 (25.0) | 16 (25.4) | 5/18 (27.8) | 2/8 (25.0) | |
| Variable | BlaESBL | ||
|---|---|---|---|
| TEM (n = 36) | SHV (n = 40) | CTX-M (n = 37) | |
| Species | |||
| Klebsiella oxytoca (n = 48) | 11/48 (22.9%) | 13/48 (27.1%) | 10/48 (20.8%) |
| Klebsiella pneumoniae (n = 91) | 25/91 (27.5%) | 27/91 (29.7%) | 27/91 (29.7%) |
| p-Valuea | 0.560 | 0.749 | 0.262 |
| Region | |||
| Northern belt (n = 22) | 9/22 (40.9%) | 6/22 (27.3%) | 7/22 (31.8%) |
| Middle belt (n = 70) | 19/70 (27.1%) | 25/70 (35.7%) | 22/70 (31.4%) |
| Southern belt (n = 47) | 8/47 (17.0%) | 9/47 (19.1%) | 8/47 (17.0%) |
| p-Valueb | 0.221 | 0.465 | 0.973 |
| p-Valuec | 0.032 | 0.446 | 0.165 |
| p-Valued | 0.203 | 0.053 | 0.080 |
| Specimen | |||
| Blood (n = 18) | 3/18 (16.7%) | 5/18 (27.8%) | 6/18 (33.3%) |
| HVS (n = 12) | 2/12 (16.7%) | 4/12 (33.3%) | 3/12 (25.0%) |
| Others (n = 8) | 1/8 (12.5%) | 2/8 (25.0%) | 2/8 (25.0%) |
| Sputum (n = 20) | 7/20 (35.0%) | 6/20 (30.0%) | 3/20 (15.0%) |
| Urine (n = 63) | 18/63 (28.5%) | 18/63 (28.5%) | 19/63 (30.1%) |
| Wound swab (n = 18) | 5/18 (27.7%) | 5/18 (27.7%) | 4/18 (22.2%) |
| Total | 36/139 (25.9%) | 40/139 (28.8%) | 37 (26.6%) |
| Variable | Resistance Profile | ||
|---|---|---|---|
| Carbapenemase | OXA-48, NDM | OXA-48 | OXA-48 |
| ID | EF 41 | EF 141 | KATH 05 |
| Presence of ESBL | TEM, CTX-M | SHV | - |
| Species | K. pneumoniae | K. pneumoniae | K. pneumoniae |
| Age(years) | 73 | 40 | 57 |
| Specimen | Urine | Sputum | Sputum |
| Hospital | Effia Nkwanta Regional Hospital | Effia Nkwanta Regional Hospital | Komfo Anokye Teaching Hospital |
| Geographical location | Southern belt | Southern belt | Middle belt |
| β-Lactams | |||
| 3rd-gen cephalosporin | |||
| Ceftriaxone | R | R | S |
| Cefotaxime | R | R | S |
| Ceftazidime | R | R | R |
| 2nd-gen cephalosporin | |||
| Cefuroxime | R | R | R |
| Cefoxitin | S | I | S |
| Cefotetan | S | S | R |
| Carbapenems | |||
| Meropenem | I | R | R |
| Imipenem | R | R | R |
| Ertapenem | S | S | R |
| Non-β-lactams | |||
| Ampicillin | R | R | R |
| Tetracycline | S | R | R |
| Cotrimoxazole | R | R | S |
| Ciprofloxacin | R | R | R |
| Chloramphenicol | R | R | S |
| Gentamicin | R | R | R |
| Amikacin | S | S | S |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quansah, E.; Amoah Barnie, P.; Omane Acheampong, D.; Obiri-Yeboah, D.; Odarkor Mills, R.; Asmah, E.; Cudjoe, O.; Dadzie, I. Geographical Distribution of β-Lactam Resistance among Klebsiella spp. from Selected Health Facilities in Ghana. Trop. Med. Infect. Dis. 2019, 4, 117. https://doi.org/10.3390/tropicalmed4030117
Quansah E, Amoah Barnie P, Omane Acheampong D, Obiri-Yeboah D, Odarkor Mills R, Asmah E, Cudjoe O, Dadzie I. Geographical Distribution of β-Lactam Resistance among Klebsiella spp. from Selected Health Facilities in Ghana. Tropical Medicine and Infectious Disease. 2019; 4(3):117. https://doi.org/10.3390/tropicalmed4030117
Chicago/Turabian StyleQuansah, Elvis, Prince Amoah Barnie, Desmond Omane Acheampong, Dorcas Obiri-Yeboah, Richael Odarkor Mills, Ebenezer Asmah, Obed Cudjoe, and Isaac Dadzie. 2019. "Geographical Distribution of β-Lactam Resistance among Klebsiella spp. from Selected Health Facilities in Ghana" Tropical Medicine and Infectious Disease 4, no. 3: 117. https://doi.org/10.3390/tropicalmed4030117
APA StyleQuansah, E., Amoah Barnie, P., Omane Acheampong, D., Obiri-Yeboah, D., Odarkor Mills, R., Asmah, E., Cudjoe, O., & Dadzie, I. (2019). Geographical Distribution of β-Lactam Resistance among Klebsiella spp. from Selected Health Facilities in Ghana. Tropical Medicine and Infectious Disease, 4(3), 117. https://doi.org/10.3390/tropicalmed4030117