Epidemiology, Risk Factors and Seasonal Variation of Scrub Typhus Fever in Central Nepal

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic Profile
3.2. Clinical Characteristics
3.3. Experimental Findings
3.4. Antibiotics
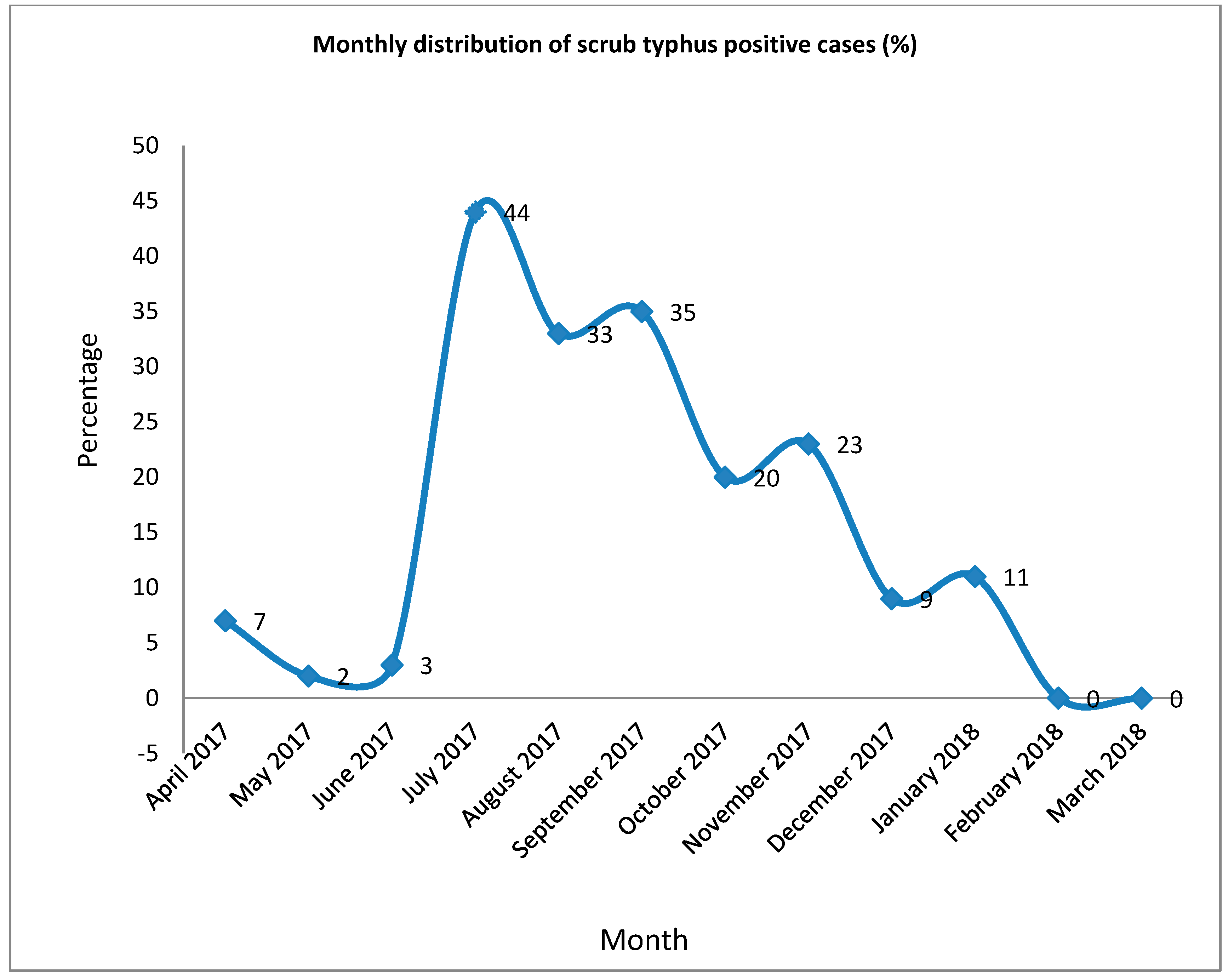
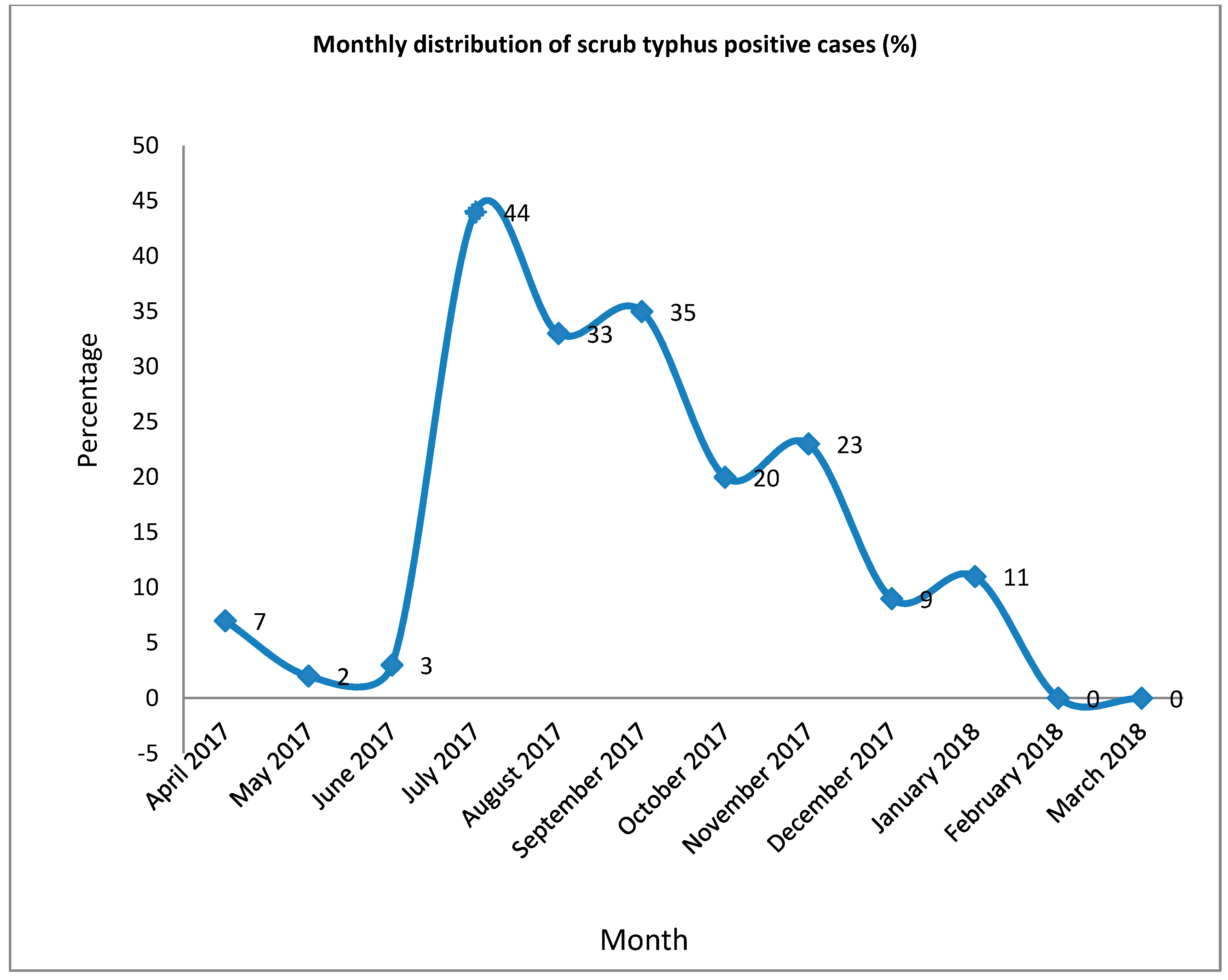
3.5. Seasonal Variation and Monthly Data
3.6. Risk Factor Analysis
4. Discussion
- Females
- Rural residential locations
- Houses near grassland
- The presence of mice inside the house and
- Working in the field.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kelly, D.J.; Fuerst, P.A.; Ching, W.M.; Richards, A.L. Scrub typhus: The geographic distribution of phenotypic and genotypic variants of Orientia tsutsugamushi. Clin. Infect. Dis. 2009, 48 (Suppl. 3), S203–S230. [Google Scholar] [CrossRef] [PubMed]
- Luce-Fedrow, A.; Lehman, M.; Kelly, D.; Mullins, K.; Maina, A.; Stewart, R.; Ge, H.; John, H.; Jiang, J.; Richards, A. A Review of Scrub Typhus (Orientia tsutsugamushi and Related Organisms): Then, Now, and Tomorrow. Trop. Med. Infect. Dis. 2018, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Lerdthusnee, K.; Khlaimanee, N.; Monkanna, T.; Sangjun, N.; Mungviriya, S.; Linthicum, K.J.; Frances, S.P.; Kollars, T.M., Jr.; Coleman, R.E. Efficiency of Leptotrombidium chiggers (Acari: Trombiculidae) at transmitting Orientia tsutsugamushi to laboratory mice. J. Med. Entomol. 2002, 39, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Tay, S.; Ho, T.M.; Rohani, M.Y.; Devi, S. Antibodies to Orientia tsutsugamushi, Rickettsia typhi and spotted fever group rickettsiae among febrile patients in rural areas of Malaysia. Trans. R. Soc. Trop. Med. Hyg. 2000, 94, 280–284. [Google Scholar] [CrossRef]
- Kim, D.-M.; Kim, S.W.; Choi, S.H.; Yun, N.R. Clinical and laboratory findings associated with severe scrub typhus. BMC Infect. Dis. 2010, 10, 108. [Google Scholar] [CrossRef] [PubMed]
- Peter, J.V.; Sudarsan, T.I.; Prakash, J.A.; Varghese, G.M. Severe scrub typhus infection: Clinical features, diagnostic challenges and management. World J. Crit. Care Med. 2015, 4, 244. [Google Scholar] [CrossRef] [PubMed]
- Bonell, A.; Bonell, A.; Lubell, Y.; Newton, P.N.; Crump, J.A.; Paris, D.H. Estimating the burden of scrub typhus: A systematic review. PLoS Negl. Trop. Dis. 2017, 11, e0005838. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.M.; Sekkizhar, G.; Kanagasabai, S.; Gopal, P.; Gopal, T.; Elumalai, S. Seroprevalence and clinical manifestations of scrub typhus infection in Chennai city: A cross-sectional study. Int. J. Health Allied Sci. 2018, 7, 201. [Google Scholar]
- Dasch, G.A.; Halle, S.; Bourgeois, A.L. Sensitive microplate enzyme-linked immunosorbent assay for detection of antibodies against the scrub typhus rickettsia, Rickettsia tsutsugamushi. J. Clin. Microbiol. 1979, 9, 38–48. [Google Scholar]
- Koraluru, M.; Bairy, I.; Varma, M.; Vidyasagar, S. Diagnostic validation of selected serological tests for detecting scrub typhus. Microbiol. Immunol. 2015, 59, 371–374. [Google Scholar] [CrossRef]
- Coleman, R.E.; Sangkasuwan, V.; Suwanabun, N.; Eamsila, C.; Mungviriya, S.; Devine, P.; Richards, A.L.; Rowland, D.; Ching, W.M.; Sattabongkot, J.; et al. Comparative evaluation of selected diagnostic assays for the detection of IgG and IgM antibody to Orientia tsutsugamushi in Thailand. Am. J. Trop. Med. Hyg. 2002, 67, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Prakash, J.; Abraham, O.; Mathai, E. Evaluation of tests for serological diagnosis of scrub typhus. Trop. Dr. 2006, 36, 212–213. [Google Scholar] [CrossRef]
- Mørch, K.; Manoharan, A.; Chandy, S.; Chacko, N.; Alvarez-Uria, G.; Patil, S.; Henry, A.; Nesaraj, J.; Kuriakose, C.; Singh, A.; et al. Acute undifferentiated fever in India: A multicentre study of aetiology and diagnostic accuracy. BMC Infect. Dis. 2017, 17, 665. [Google Scholar] [CrossRef]
- Blacksell, S.D.; Tanganuchitcharnchai, A.; Nawtaisong, P.; Kantipong, P.; Laongnualpanich, A.; Day, N.P.; Paris, D.H. Diagnostic accuracy of the InBios scrub typhus detect enzyme-linked immunoassay for the detection of IgM antibodies in Northern Thailand. Clin. Vaccine Immunol. 2016, 23, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Blacksell, S.; Kingston, H.; Tanganuchitcharnchai, A.; Phanichkrivalkosil, M.; Hossain, M.; Hossain, A.; Ghose, A.; Leopold, S.; Dondorp, A.; Day, N.; et al. Diagnostic Accuracy of the InBios Scrub Typhus Detect™ ELISA for the Detection of IgM Antibodies in Chittagong, Bangladesh. Trop. Med. Infect. Dis. 2018, 3, 95. [Google Scholar] [CrossRef] [PubMed]
- Isaac, R.; Isaac, R.; Varghese, G.M.; Mathai, E.; Manjula, J.; Joseph, I. Scrub typhus: Prevalence and diagnostic issues in rural Southern India. Clin. Infect. Dis. 2004, 39, 1395–1396. [Google Scholar] [CrossRef] [PubMed]
- Upadhyaya, B.; Shakya, G.; Adhikari, S.; Rijal, N.; Acharya, J.; Maharjan, L.; Marasini, B.R. Scrub typhus: An emerging neglected tropical disease in Nepal. J. Nepal Health Res. Counc. 2016, 14, 122–127. [Google Scholar]
- Thapa, S.; Sapkota, L.; Hamal, P. Threat of scrub typhus in post-earthquake Nepal. J. Chitwan Med. Coll. 2016, 6, 1–6. [Google Scholar] [CrossRef]
- Bithu, R.; Kanodia, V.; Maheshwari, R. Possibility of scrub typhus in fever of unknown origin (FUO) cases: An experience from Rajasthan. Indian J. Med. Microbiol. 2014, 32, 387. [Google Scholar] [CrossRef]
- Bang, H.; Lee, M.; Lee, W. Comparative research on epidemiological aspects of tsutsugamushi disease (scrub typhus) between Korea and Japan. Jpn. J. Infect. Dis. 2008, 61, 148. [Google Scholar]
- Jyothi, R.; Sahira, H.; Sathyabhama, M.C.; Bai, J.R. Seroprevalence of Scrub typhus among Febrile Patients in a Tertiary Care Hospital in Thiruvananthapuram, Kerala. J. Acad. Ind. Res. (Jair) 2015, 3, 542. [Google Scholar]
- Kuo, C.-C.; Huang, J.L.; Ko, C.Y.; Lee, P.F.; Wang, H.C. Spatial analysis of scrub typhus infection and its association with environmental and socioeconomic factors in Taiwan. Acta Trop. 2011, 120, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Vallée, J.; Thaojaikong, T.; Moore, C.E.; Phetsouvanh, R.; Richards, A.L.; Souris, M.; Fournet, F.; Salem, G.; Gonzalez, J.P.; Newton, P.N. Contrasting spatial distribution and risk factors for past infection with scrub typhus and murine typhus in Vientiane City, Lao PDR. PLoS Negl. Trop. Dis. 2010, 4, e909. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Tan, Z.; Ren, D.; Zhang, X.; He, Y.; Bao, C.; Liu, D.; Yi, Q.; Qian, W.; Yin, J.; et al. Clinical characteristics and risk factors of an outbreak with scrub typhus in previously unrecognized areas, Jiangsu province, China 2013. PLoS ONE 2015, 10, e0125999. [Google Scholar] [CrossRef] [PubMed]
- Maude, R.R.; Maude, R.J.; Ghose, A.; Amin, M.R.; Islam, M.B.; Ali, M.; Bari, M.S.; Majumder, M.I.; Tanganuchitcharnchai, A.; Dondorp, A.M.; et al. Serosurveillance of Orientia tsutsugamushi and Rickettsia typhi in Bangladesh. Am. J. Trop. Med. Hyg. 2014, 91, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.I.; Devi, K.P.; Tilotama, R.; Ningombam, S.; Gopalkrishna, Y.; Singh, T.B.; Murhekar, M.V. An outbreak of scrub typhus in Bishnupur district of Manipur, India, 2007. Trop. Dr. 2010, 40, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Lerdthusnee, K.; Nigro, J.; Monkanna, T.; Leepitakrat, W.; Leepitakrat, S.; Insuan, S.; Charoensongsermkit, W.; Khlaimanee, N.; Akkagraisee, W.; Chayapum, K.; et al. Surveys of rodent-borne disease in Thailand with a focus on scrub typhus assessment. Integr. Zool. 2008, 3, 267–273. [Google Scholar] [CrossRef]
- Frances, S.; Watcharapichat, P.; Phulsuksombati, D.; Tanskul, P. Transmission of Orientia tsutsugamushi, the aetiological agent for scrub typhus, to co-feeding mites. Parasitology 2000, 120, 601–607. [Google Scholar] [CrossRef]
- Frances, S.P.; Watcharapichat, P.; Phulsuksombati, D.; Tanskul, P.; Linthicum, K.J. Seasonal occurrence of Leptotrombidium deliense (Acari: Trombiculidae) attached to sentinel rodents in an orchard near Bangkok, Thailand. J. Med. Entomol. 1999, 36, 869–874. [Google Scholar] [CrossRef]
- Gurung, S.; Pradhan, J.; Bhutia, P. Outbreak of scrub typhus in the North East Himalayan region-Sikkim: An emerging threat. Indian J. Med. Microbiol. 2013, 31, 72. [Google Scholar] [CrossRef]
- Kingston, H.W.; Hossain, M.; Leopold, S.; Anantatat, T.; Tanganuchitcharnchai, A.; Sinha, I.; Plewes, K.; Maude, R.J.; Chowdhury, M.H.; Paul, S.; et al. Rickettsial illnesses as important causes of febrile illness in Chittagong, Bangladesh. Emerg. Infect. Dis. 2018, 24, 638. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.-J.; Yeh, H.-C. Scrub typhus islands in the Taiwan area and the association between scrub typhus disease and forest land use and farmer population density: Geographically weighted regression. BMC Infect. Dis. 2013, 13, 191. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.J.; Paris, D.H.; Newton, P.N. A systematic review of mortality from untreated scrub typhus (Orientia tsutsugamushi). PLoS Negl. Trop. Dis. 2015, 9, e0003971. [Google Scholar] [CrossRef] [PubMed]
- Wangrangsimakul, T.; Althaus, T.; Mukaka, M.; Kantipong, P.; Wuthiekanun, V.; Chierakul, W.; Blacksell, S.D.; Day, N.P.; Laongnualpanich, A.; Paris, D.H. Causes of acute undifferentiated fever and the utility of biomarkers in Chiangrai, northern Thailand. PLoS Negl. Trop. Dis. 2018, 12, e0006477. [Google Scholar] [CrossRef] [PubMed]
- Varghese, G.M.; Janardhanan, J.; Trowbridge, P.; Peter, J.V.; Prakash, J.A.; Sathyendra, S.; Thomas, K.; David, T.S.; Kavitha, M.L.; Abraham, O.C.; et al. Scrub typhus in South India: Clinical and laboratory manifestations, genetic variability, and outcome. Int. J. Infect. Dis. 2013, 17, e981–e987. [Google Scholar] [CrossRef] [PubMed]
- Bibhuti Saha, S.; Mitra, K.; Ghosh, S.; Naskar, A.; Ghosh, M.K.; Parui, S.; Thakur, A.; Bhattacharya, B.; Majumdar, D.; Chakraborty, S. Socio-demographic and Clinico-Epidemiological Study of Scrub Typhus in Two Tertiary Care Hospitals of Kolkata. J. Assoc. Phys. India 2018, 66, 22. [Google Scholar]
- Sirisanthana, V.; Puthanakit, T.; Sirisanthana, T. Epidemiologic, clinical and laboratory features of scrub typhus in thirty Thai children. Pediatr. Infect. Dis. J. 2003, 22, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Varghese, G.M.; Trowbridge, P.; Janardhanan, J.; Thomas, K.; Peter, J.V.; Mathews, P.; Abraham, O.C.; Kavitha, M.L. Clinical profile and improving mortality trend of scrub typhus in South India. Int. J. Infect. Dis. 2014, 23, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Silpapojakul, K.; Varachit, B.; Silpapojakul, K. Paediatric scrub typhus in Thailand: A study of 73 confirmed cases. Trans. R. Soc. Trop. Med. Hyg. 2004, 98, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.J.; Kim, S.; Wook, Y.D.; Lee, J.W.; Kim, K.I.; Lee, S.H. Scrub typhus: Clinical, pathologic, and imaging findings. Radiographics 2007, 27, 161–172. [Google Scholar] [CrossRef]
- Mahajan, S.K.; Rolain, J.M.; Kashyap, R.; Bakshi, D.; Sharma, V.; Prasher, B.S.; Pal, L.S.; Raoult, D. Scrub typhus in Himalayas. Emerg. Infect. Dis. 2006, 12, 1590. [Google Scholar] [CrossRef] [PubMed]
- Vivekanandan, M.; Mani, A.; Priya, Y.S.; Singh, A.P.; Jayakumar, S.; Purty, S. Outbreak of scrub typhus in Pondicherry. J. Assoc. Phys. India 2010, 58, 24–28. [Google Scholar]
- Singh, S.; Singh, R.; Ahmad, N. A study of complications of scrub typhus in a tertiary health care institute of Uttarakhand, India. Int. J. Res. Med. Sci. 2017, 2, 246–249. [Google Scholar] [CrossRef]
- Prakash, A.; Acharya, A.S.; Jain, N.; Bhattacharya, D.; Chhabra, M. Scrub typhus–An emerging public health problem in Delhi! Indian J. Med. Spec. 2014, 5, 68–72. [Google Scholar] [CrossRef]
- Seong, S.-Y.; Choi, M.-S.; Kim, I.-S. Orientia tsutsugamushi infection: Overview and immune responses. Microbes Infect. 2001, 3, 11–21. [Google Scholar] [CrossRef]

{kind=link}
| Variables | ELISA Report | p-Value | Odds Ratio | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Positive | Negative | ||||
| Sex | |||||
| Male | 138 (16.7%) | 690 (83.3%) | 1 | ||
| Female | 220 (29.1%) | 537 (70.9%) | <0.001 | 0.488 | 0.384–0.621 |
| Occupation | |||||
| Housewives | 78(28.3%) | 198(71.7%) | <0.001 | 3.008 | 1.889–5.051 |
| Daily wages | 17(26.2%) | 48 (73.8%) | 0.004 | 2.777 | 1.390–5.549 |
| Students | 171(24.9%) | 517(75.1%) | <0.001 | 2.593 | 1.652–4.070 |
| Farmers | 67(20.0%) | 268(80.0%) | 0.008 | 1.960 | 1.195–3.215 |
| Other [business, job] | 25 (11.3%) | 196(88.7%) | 1 | ||
| Education | |||||
| Secondary level | 74(24.3%) | 231(75.7%) | 0.125 | 2.323 | 0.791–6.823 |
| Primary level | 99(22.9%) | 334(77.1%) | 0.161 | 2.149 | 0.738–6.260 |
| Higher secondary | 85(22.4%) | 295(77.6%) | 0.178 | 2.089 | 0.714–6.108 |
| No education | 96(22.1%) | 338(77.9%) | 0.186 | 2.059 | 0.707–6.001 |
| Graduate | 4(12.1%) | 29(87.9%) | 1 | ||
| Age Group | |||||
| 1–10 Years | 61(22.7%) | 208(77.3%) | 0.046 | 2.236 | 1.015–4.929 |
| 11–20 | 80(26.3%) | 224(73.7%) | 0.012 | 2.723 | 1.248–5.940 |
| 21–30 | 62(21.5%) | 226(78.5%) | 0.067 | 2.092 | 0.951–4.603 |
| 31–40 | 53 (22.6%) | 181(77.4%) | 0.049 | 2.233 | 1.005–4.959 |
| 41–50 | 39(22.0%) | 138(78.0%) | 0.066 | 2.155 | 0.951–4.884 |
| 51–60 | 45 (28.5%) | 113(71.5%) | 0.007 | 3.037 | 1.345–6.853 |
| 61–70 | 10(11.6%) | 76(88.4%) | 0.995 | 1.003 | 0.373–2.697 |
| 71 and above | 8 (11.6%) | 61(88.4%) | 1 | ||
| Seasonal variation | |||||
| Spring | 3 (2.3%) | 130(97.7%) | 1 | ||
| Winter | 10(7.5%) | 124(92.5%) | 0.062 | 3.495 | 0.940–12.996 |
| Fall/Autumn | 236(24.9%) | 713(75.1%) | <0.001 | 14.343 | 4.523–45.480 |
| Summer | 109(29.5%) | 260(70.5%) | <0.001 | 18.167 | 5.660–58.312 |
| Residential location | |||||
| Rural | 279 (23.8%) | 892 (76.2%) | 0.048 | 1.326 | 1.003–1.754 |
| Urban | 79 (19.1%) | 335 (80.9%) | 1 | ||
| Type of house | |||||
| Cemented floor | 84 (20.0%) | 336 (80.0%) | 1 | ||
| No cemented floor | 274 (23.5%) | 891 (76.5%) | 0.140 | 0.813 | 0.618–1.070 |
| House near grassland | |||||
| Yes | 303 (25.4%) | 891 (74.6%) | <0.001 | 2.078 | 1.518–2.842 |
| No | 55 (14.1%) | 336 (85.9%) | 1 | ||
| Piling weeds in house | |||||
| Yes | 63 (23.8%) | 202 (76.2%) | 0.613 | 1.084 | 0.794–1.479 |
| No | 295 (22.3%) | 1025(77.7%) | 1 | ||
| Piling weeds on the yard | |||||
| Yes | 239(41.8%) | 333(58.2%) | <0.001 | 5.392 | 4.185–6.947 |
| No | 119(11.7%) | 894(88.3%) | 1 | ||
| Presence of mice | |||||
| Yes | 268(42.3%) | 365(57.7%) | <0.001 | 7.032 | 5.377–9.197 |
| No | 90(9.5%) | 862(90.5%) | 1 | ||
| Working in the field | |||||
| Yes | 237(43.8%) | 304(56.2%) | <0.001 | 5.947 | 4.611–7.670 |
| No | 121 (11.6%) | 923(88.4%) | 1 | ||
| Clinical Characteristics | Number (%) |
|---|---|
| Fever | 358 (100) |
| Nausea | 181 (50.6) |
| Headache | 180 (50.3) |
| Shortness of breath | 105 (29.3) |
| Abdominal pain | 67 (18.7) |
| Tachypnea | 60 (16.8) |
| Ventilation support | 52 (14.5) |
| Jaundice | 42 (11.7) |
| Hypertension | 21 (5.9) |
| Seizure | 17 (4.7) |
| COPD | 15 (4.2) |
| Diabetes | 13 (3.6) |
| Hypotension | 13 (3.6) |
| Eschar | 11 (3.1) |
| Pregnancy | 5 (1.4) |
| Laboratory Parameters | Value | Number (%) |
|---|---|---|
| Hemoglobin | <11.0 gm/dL | 163 (45.3) |
| >11.0 gm/dL | 196 (54.7) | |
| Total leucocyte count | <4000 cumm | 35 (9.8) |
| 4000–11,000 cumm | 238 (66.5) | |
| >11,000 cumm | 85 (23.7) | |
| Platelet count | <150,000/µL | 265 (74.09) |
| 150,000–450,000/µL | 93 (26.0) | |
| Urea | >45 mg/dL | 48 (13.4) |
| <45 mg/dL | 310 (86.6) | |
| Creatinine | >1.4 mg/dl | 67 (18.7) |
| <1.4 mg/dl | 291 (81.3) | |
| Bilirubin(total) | >1.2 mg/dL | 87 (24.3) |
| Up to 1.2 mg/dL | 271 (75.7) | |
| Bilirubin(direct) | >0.4 mg/dL | 115 (32.1) |
| Up to 0.4 mg/dL | 243 (67.9) | |
| AST | >45 mg/dL | 255 (71.2) |
| Up to 45 mg/dL | 103 (28.8) | |
| ALT | >40 mg/dL | 277 (77.4) |
| Up to 40 mg/dL | 81 (22.6) | |
| ALP | >192.0 U/L | 115 (32.1) |
| <192.0 U/L | 243 (67.9) | |
| Protein | >6.0 mg/dL | 276 (77.1) |
| Up to 6.0 mg/dL | 82 (22.9) | |
| Albumin | >3.5 mg/dL | 119 (33.2) |
| Up to 3.5 mg/dL | 239 (66.8) |
| Number (%) | |
|---|---|
| Doxycycline | 154 (43.0) |
| Doxycycline/Ciprofloxacin/Azithromycin | 64 (17.9) |
| Doxycycline/Azithromycin | 57 (15.9) |
| Ceftriaxone/Azithromycin | 20 (5.6) |
| Azithromycin | 18 (5.0) |
| Piperacillin/Tazobactum | 16 (4.5) |
| Amikacin IV | 13 (3.6) |
| Levofloxacin/Ceftazidime | 9 (2.5) |
| Ceftriaxone IV | 7 (2.0) |
| Variables | ELISA Report | p-Value | Adjusted Odds Ratio | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Positive | Negative | ||||
| Sex | |||||
| Male | 138 (16.7%) | 690 (83.3%) | 1 | ||
| Female | 220 (29.1%) | 537 (70.9%) | <0.001 | 1.976 | 1.417–2.756 |
| Occupation | |||||
| Housewives | 83(28.3%) | 210(71.7%) | 0.033 | 2.054 | 1.060–3.982 |
| Daily wages | 16(25.8%) | 46(74.2%) | 0.092 | 2.115 | 0.886–5.049 |
| Students | 173(24.6%) | 531(75.4%) | 0.014 | 2.231 | 1.174–4.238 |
| Farmers | 66(19.2%) | 277(80.8%) | 0.105 | 1.704 | 0.895–3.245 |
| Other [business, job] | 20(10.9%) | 163(89.1%) | 1 | ||
| Age groups | |||||
| 1–10 Years | 61(22.7%) | 208(77.3%) | 0.171 | 2.042 | 0.736–5.667 |
| 11–20 | 80(26.3%) | 224(73.7%) | 0.329 | 1.690 | 0.589–4.848 |
| 21–30 | 62(21.5%) | 226(78.5%) | 0.381 | 1.557 | 0.578–4.191 |
| 31–40 | 53 (22.6%) | 181(77.4%) | 0.406 | 1.504 | 0.575–3.934 |
| 41–50 | 39(22.0%) | 138(78.0%) | 0.387 | 1.537 | 0.580–4.075 |
| 51–60 | 45 (28.5%) | 113(71.5%) | 0.077 | 2.403 | 0.908–6.357 |
| 61–70 | 10(11.6%) | 76(88.4%) | 0.665 | 0.773 | 0.240–2.485 |
| 71 and Above | 8(11.6%) | 61(88.4%) | 1 | ||
| Season | |||||
| Spring | 3 (2.3%) | 130(97.7%) | 1 | ||
| Winter | 10(7.5%) | 124(92.5%) | 0.004 | 7.877 | 1.967–31.538 |
| Fall autumn | 236(24.9%) | 713(75.1%) | <0.001 | 25.141 | 7.528–83.970 |
| Summer | 109(29.5%) | 260(70.5%) | <0.001 | 17.879 | 5.303–60.276 |
| Residential location | |||||
| Rural | 279 (23.8%) | 892 (76.2%) | 0.001 | 1.32 | 1.245–1.675 |
| Urban | 79 (19.1%) | 335 (80.9%) | 1 | ||
| House near grassland | |||||
| Yes | 303 (25.4%) | 891 (74.6%) | <0.001 | 3.288 | 1.935–5.587 |
| No | 55 (14.1%) | 336 (85.9%) | 1 | ||
| Piling weeds in yard | |||||
| Yes | 239(41.8%) | 333(58.2%) | 0.409 | 0.517 | 0.108–2.480 |
| No | 119(11.7%) | 894(88.3%) | 1 | ||
| Presence of mice | |||||
| Yes | 268(42.3%) | 365(57.7%) | <0.001 | 5.504 | 4.074–7.435 |
| No | 90(9.5%) | 862(90.5%) | 1 | ||
| Working in the field | |||||
| Yes | 237(43.8%) | 304(56.2%) | 0.004 | 9.764 | 2.059–46.315 |
| No | 121 (11.6%) | 923(88.4%) | 1 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gautam, R.; Parajuli, K.; Sherchand, J.B. Epidemiology, Risk Factors and Seasonal Variation of Scrub Typhus Fever in Central Nepal. Trop. Med. Infect. Dis. 2019, 4, 27. https://doi.org/10.3390/tropicalmed4010027
Gautam R, Parajuli K, Sherchand JB. Epidemiology, Risk Factors and Seasonal Variation of Scrub Typhus Fever in Central Nepal. Tropical Medicine and Infectious Disease. 2019; 4(1):27. https://doi.org/10.3390/tropicalmed4010027
Chicago/Turabian StyleGautam, Rajendra, Keshab Parajuli, and Jeevan Bahadur Sherchand. 2019. "Epidemiology, Risk Factors and Seasonal Variation of Scrub Typhus Fever in Central Nepal" Tropical Medicine and Infectious Disease 4, no. 1: 27. https://doi.org/10.3390/tropicalmed4010027
APA StyleGautam, R., Parajuli, K., & Sherchand, J. B. (2019). Epidemiology, Risk Factors and Seasonal Variation of Scrub Typhus Fever in Central Nepal. Tropical Medicine and Infectious Disease, 4(1), 27. https://doi.org/10.3390/tropicalmed4010027