A Teledermatology Pilot Programme for the Management of Skin Diseases in Primary Health Care Centres: Experiences from a Resource-Limited Country (Mali, West Africa)

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Ethical Statements
2.2. Health Care System in Mali
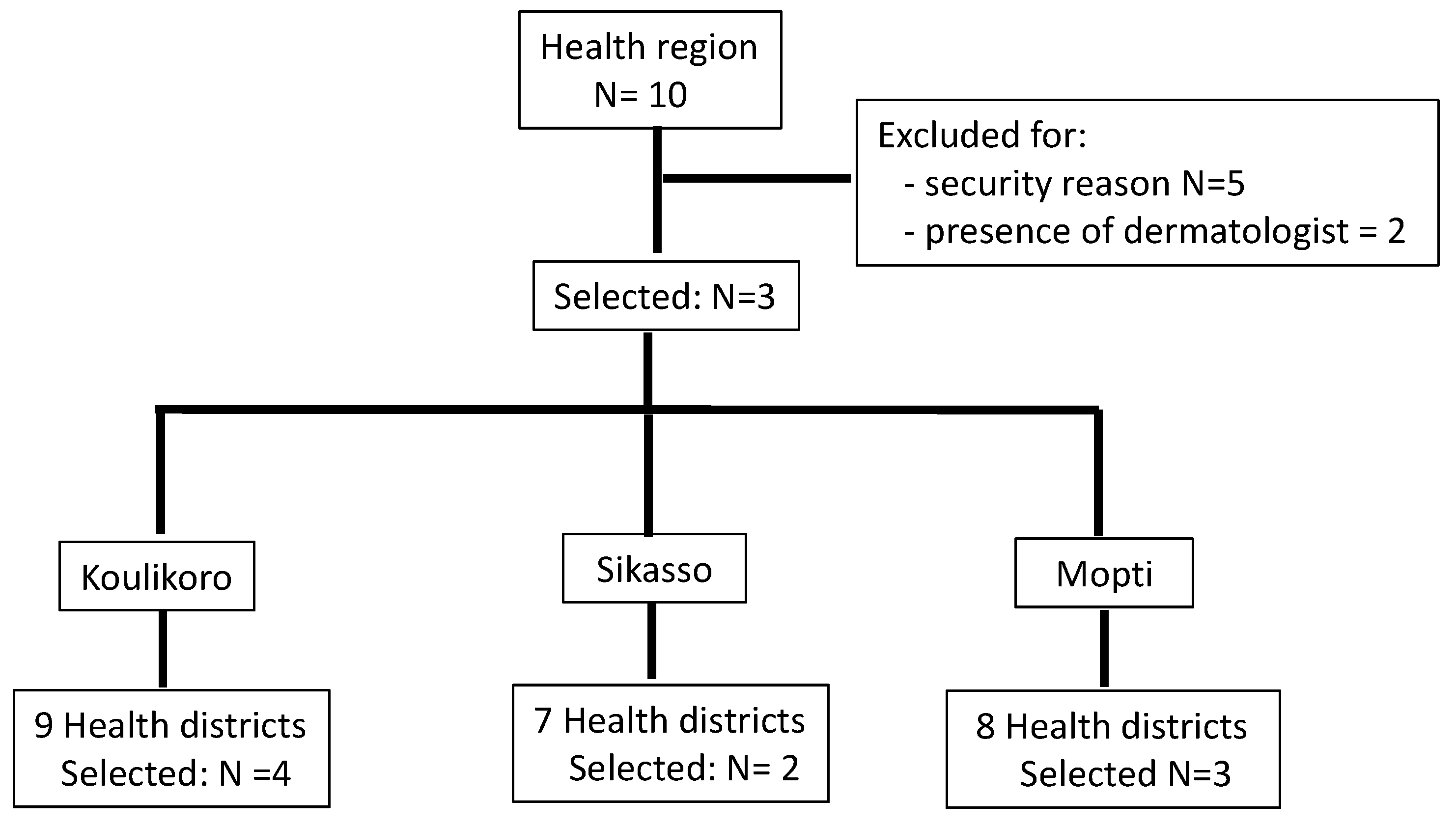
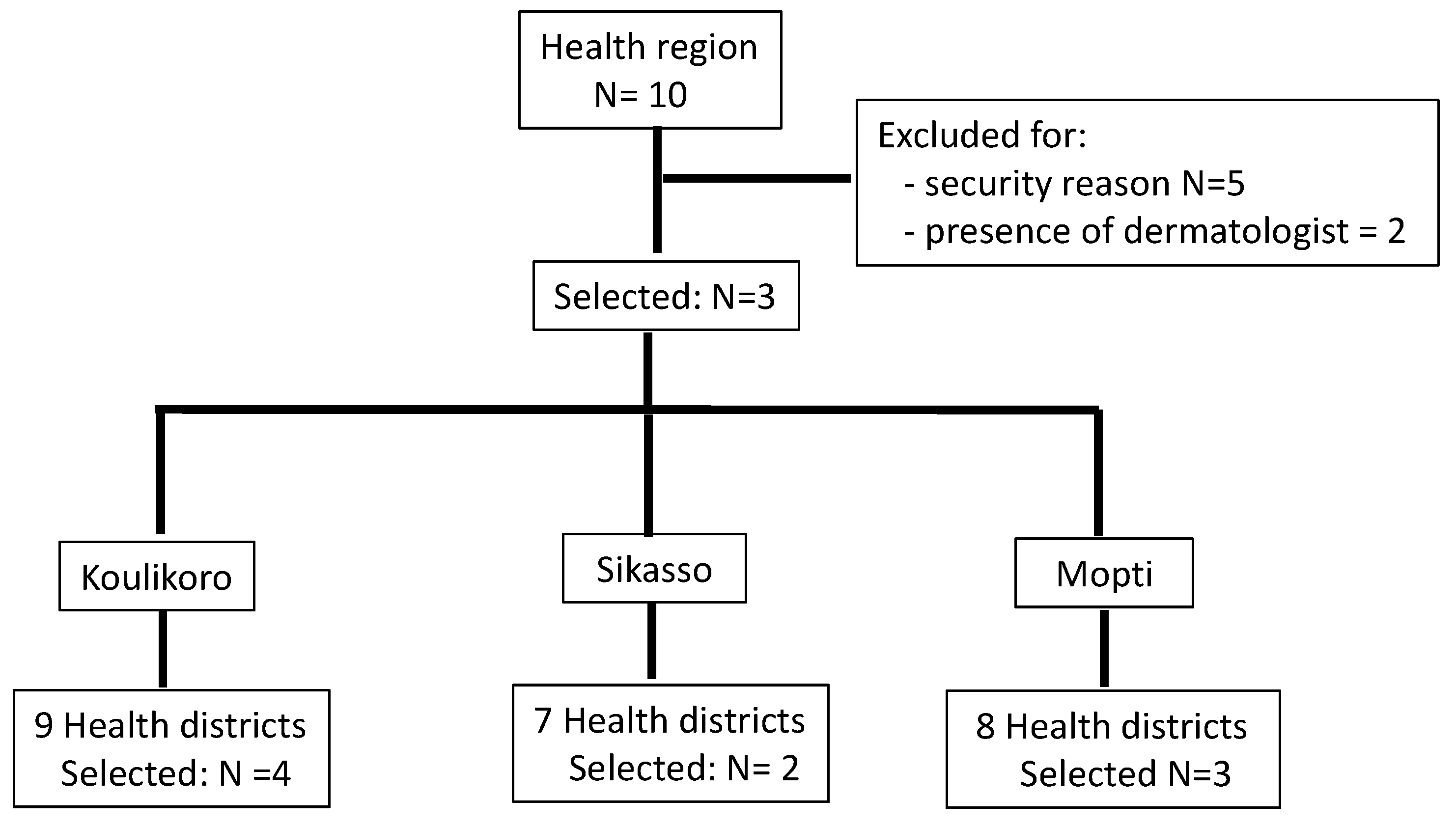
2.3. Study Design, Sites, and Duration
2.4. Intervention—Equipment and Participants
2.5. Teledermatology Operating Procedures
2.6. Evaluation
2.7. Data Collection and Statistical Analysis
3. Results
3.1. Characteristics of the Study Sites and Trainees:
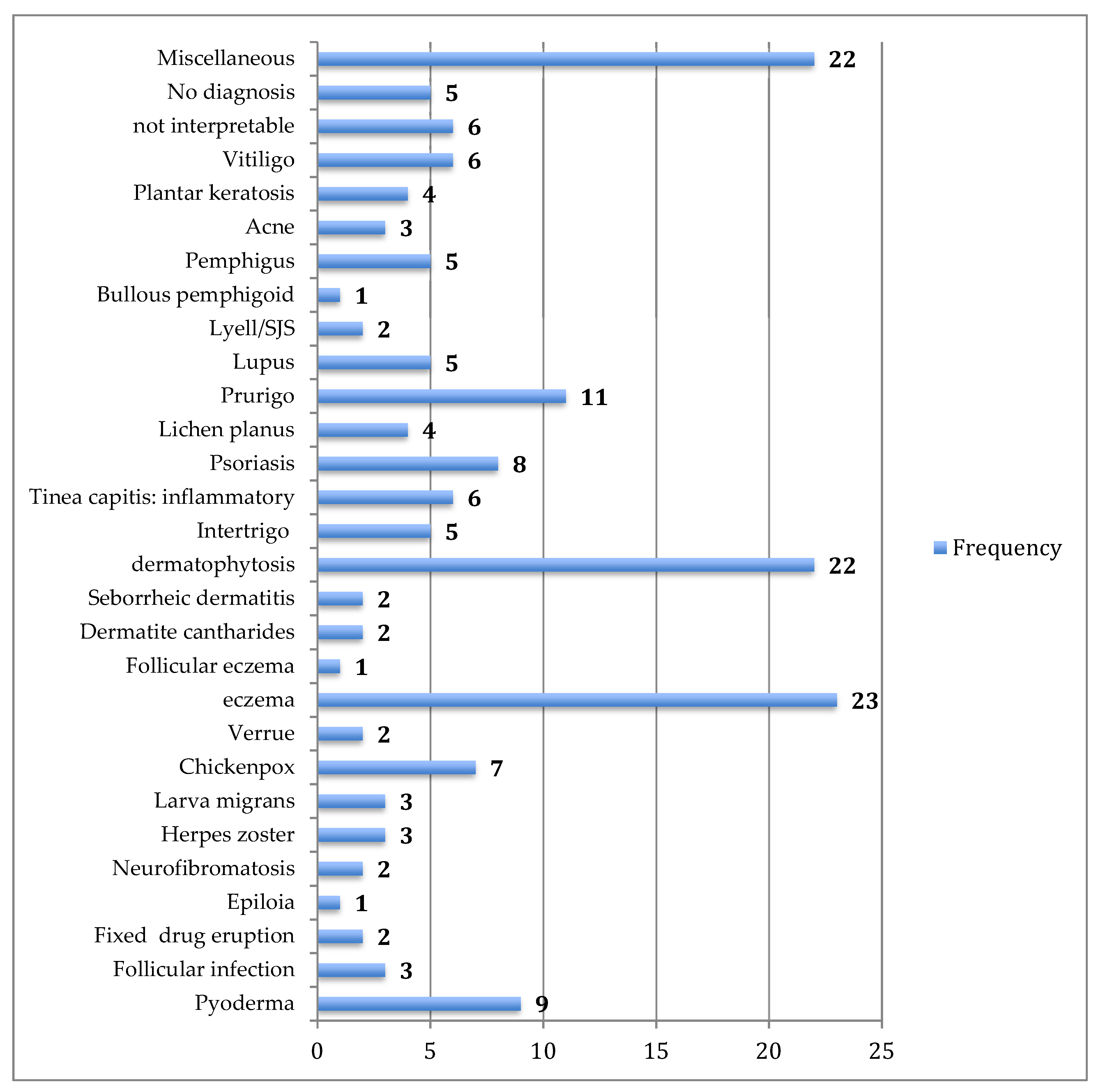
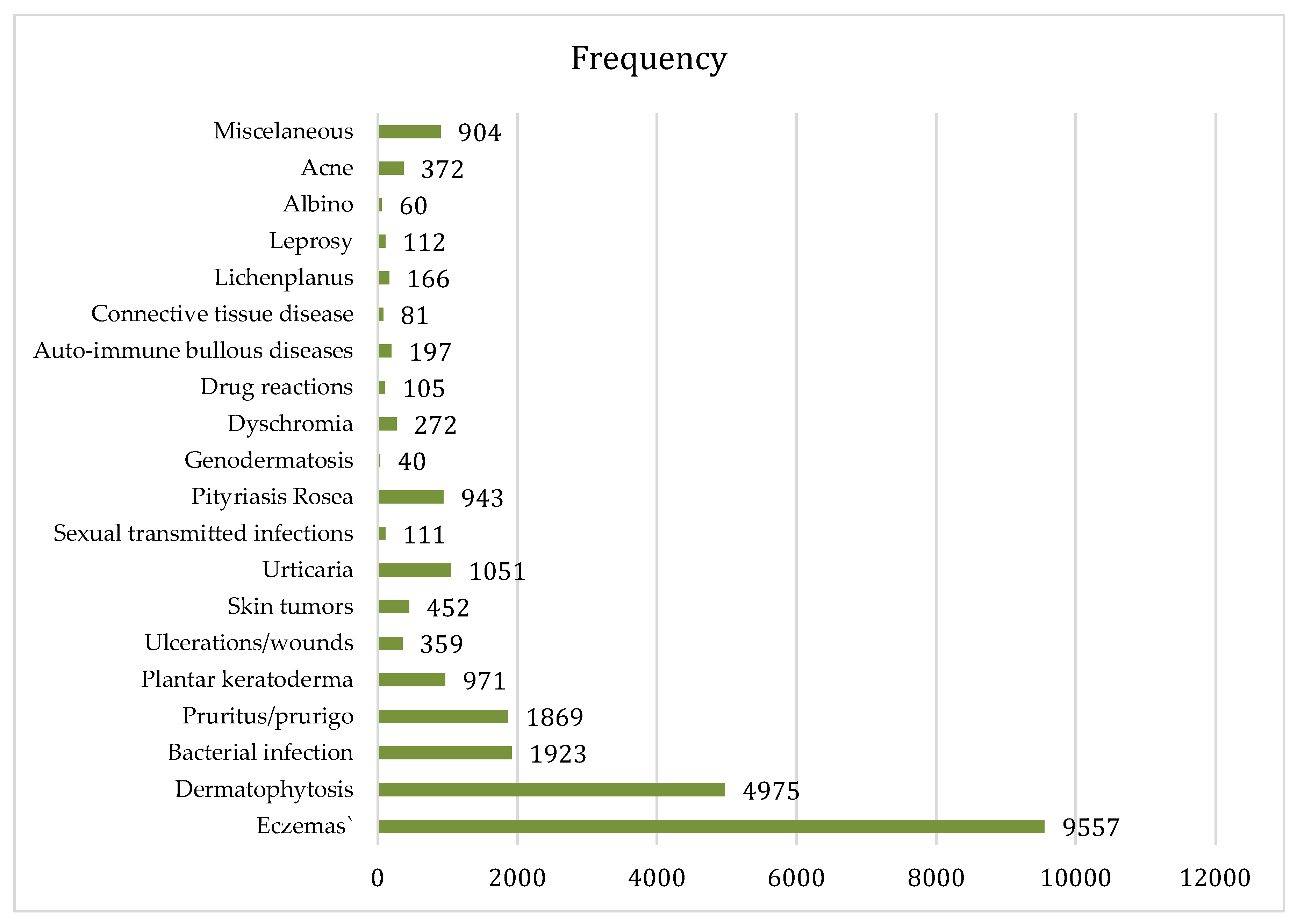
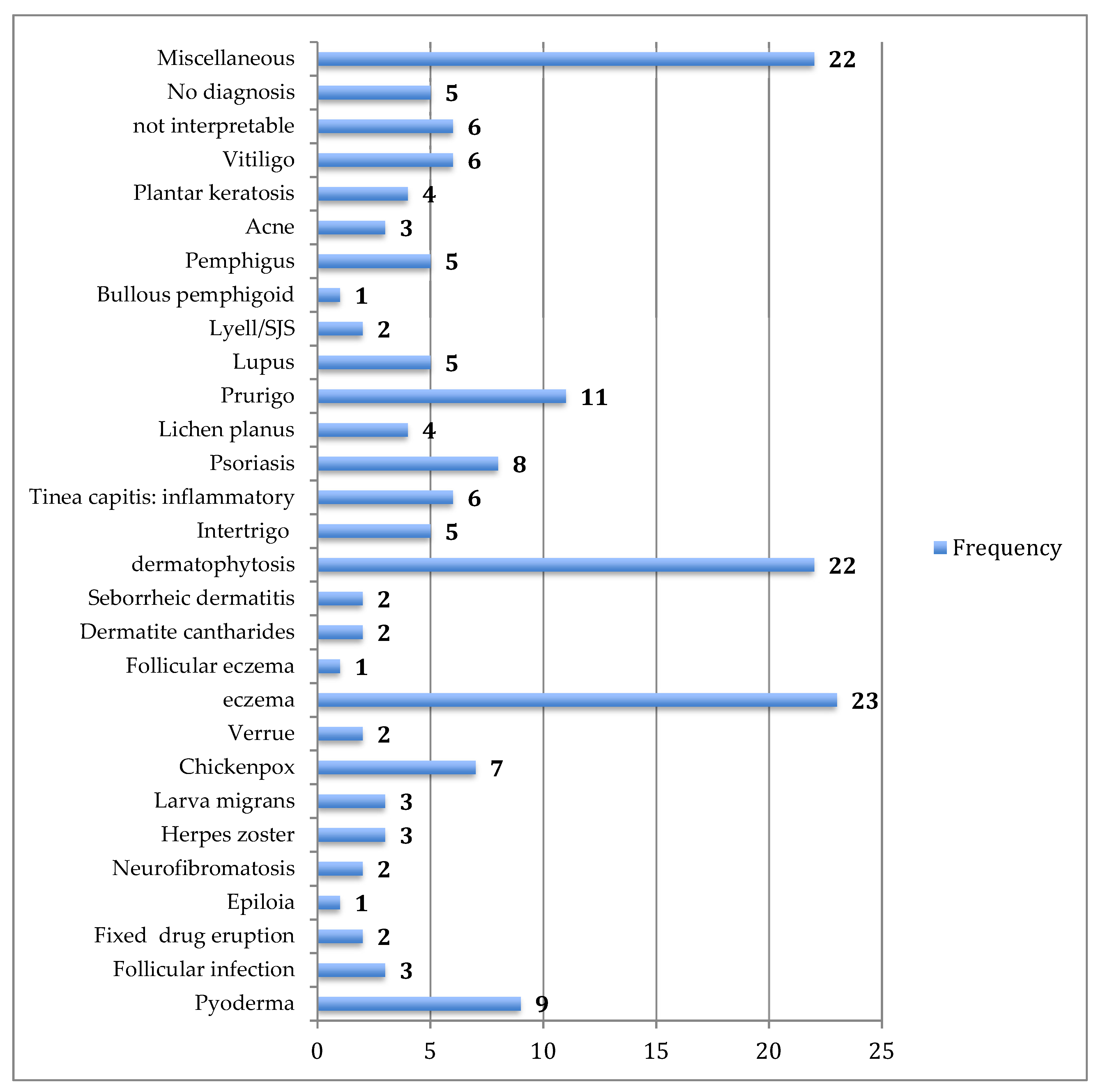
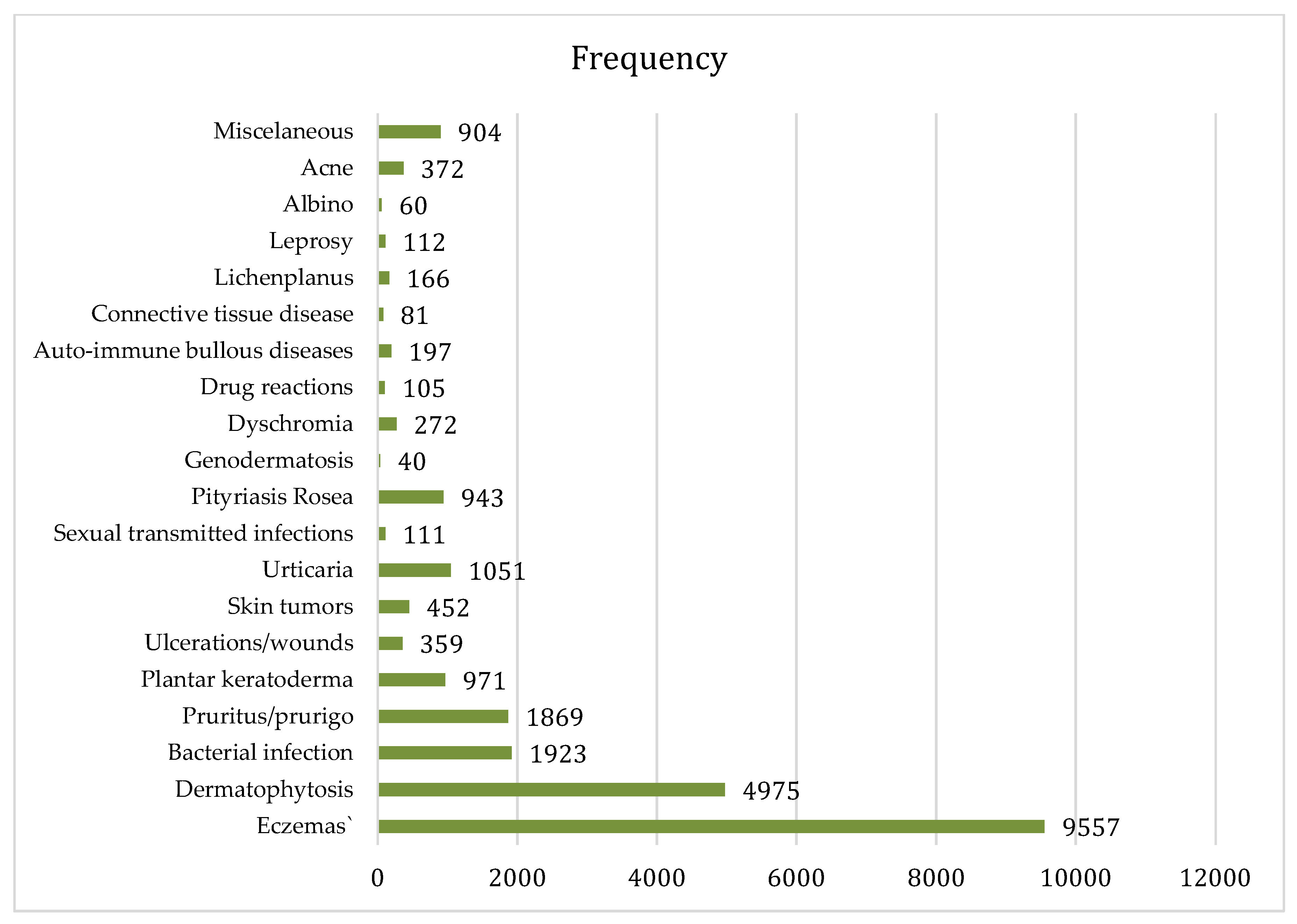
3.2. Skin Diseases Diagnosed by HCWs
3.3. Management of Skin Diseases via Teledermatology
3.4. Satisfaction of HWCs and Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Anonymous. Skin disease and public health medicine. Lancet 1991, 337, 1008–1009. [Google Scholar] [CrossRef]
- Figueroa, J.I.; Fuller, L.C.; Abraha, A.; Hay, R.J. Dermatology in southwestern Ethiopia: Rationale for a community approach. Int. J. Dermatol. 1998, 37, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Mahé, A.; Prual, A.; Konaté, M.; Bobin, P. Skin diseases of children in Mali: A public health problem. Trans. R. Soc. Trop. Med. Hyg. 1995, 89, 467–470. [Google Scholar] [CrossRef]
- Walker, S.L.; Shah, M.; Hubbard, V.G.; Pradhan, H.M.; Ghimire, M. Skin disease is common in rural Nepal: Results of a point prevalence study. Br. J. Dermatol. 2008, 158, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Saw, S.M.; Koh, D.; Adjani, M.R.; Wong, M.L.; Hong, C.Y.; Lee, J.; Chia, S.E.; Munoz, C.P.; Ong, C.N. A population-based prevalence survey of skin diseases in adolescents and adults in rural Sumatra, Indonesia, 1999. Trans. R. Soc. Trop. Med. Hyg. 2001, 95, 384–388. [Google Scholar] [CrossRef]
- Abdel-Hafez, K.; Abdel-Aty, M.A.; Hofny, E.R. Prevalence of skin diseases in rural areas of Assiut Governorate, Upper Egypt. Int. J. Dermatol. 2003, 42, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Leekassa, R.; Bizuneh, E.; Alem, A.; Fekadu, A.; Shibre, T. Community diagnosis of common skin diseases in the Zay community of the Zeway Islands, Ethiopia. Ethiop. Med. J. 2005, 43, 189–195. [Google Scholar] [PubMed]
- Dogra, S.; Kumar, B. Epidemiology of skin diseases in school children: A study from northern India. Pediatr. Dermatol. 2003, 20, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Bechelli, L.M.; Haddad, N.; Pimenta, W.P.; Pagnano, P.M.; Melchior, J.E.; Fregnan, R.C.; Zanin, L.C.; Arenas, A. Epidemiological survey of skin diseases in schoolchildren living in the Purus Valley (Acre State, Amazonia, Brazil). Dermatologica 1981, 163, 78–93. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, S.A.M. Skin disease and socioeconomic conditions in rural Africa: Tanzania. Int. J. Dermatol. 1996, 35, 633–639. [Google Scholar] [CrossRef] [PubMed]
- National Health Administration of the Minister of Health. Direction Nationale de la Santé. Données du Système d’Information Sanitaire National: Annuaire Statistique 2007; Ministère de la Santé: Bamako, Mali, 2007; p. 145. (In French).
- Karimkhani, C.; Dellavalle, R.P.; Coffeng, L.E.; Flohr, C.; Hay, R.J.; Langan, S.M.; Nsoesie, E.O.; Ferrari, A.J.; Erskine, H.E.; Silverberg, J.I.; et al. Global skin disease morbidity and mortality: an update from the global burden of disease study 2013. JAMA Dermatol. 2017, 153, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Faye, O.; Keita, S.; N’diaye, H.; Konare, H.; Coulibaly, I. Evaluation du niveau de connaissance des agents de santé sur le diagnostic de la lèpre à Bamako (MALI): Proposition pour l’avenir de la lutte anti-lépreuse. Mali. Méd. 2003, 18, 32–34. (In French) [Google Scholar]
- Mahé, A.; Cissé, I.A.; Faye, O.; N′ Diaye, H.T.; Niamba, P. Skin diseases in Bamako (Mali). Int. J. Dermatol. 1998, 37, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Mahé, A.; Faye, O.; N’Diaye, H.T.; Konaré, H.D.; Coulibaly, I.; Kéita, S.; Traoré, A.K.; Hay, R.J. Integration of basic dermatological care into primary health care services in Mali. Bull World Health Organ. 2005, 83, 935–943. [Google Scholar] [PubMed]
- Warshaw, E.M.; Hillman, Y.J.; Greer, N.L.; Hagel, E.M.; MacDonald, R.; Rutks, I.R.; Wilt, T.J. Teledermatology for diagnosis and management of skin conditions: A systematic review. J. Am. Acad. Dermatol. 2011, 64, 759–772. [Google Scholar] [CrossRef] [PubMed]
- Heffner, V.A.; Lyon, V.B.; Brousseau, D.C.; Holland, K.E.; Yen, K. Store-and-forward teledermatology versus in-person visits: A comparison in pediatric teledermatology clinic. J. Am. Acad. Dermatol. 2009, 60, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Edison, K.E.; Ward, D.S.; Dyer, J.A.; Lane, W.; Chance, L.; Hicks, L.L. Diagnosis, diagnostic confidence, and management concordance in live-interactive and store-and-forward teledermatology compared to in-person examination. Telemed. E-Health, 2008, 14, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Ramirez, D.; Ferrandiz, L.; Nieto-Garcia, A.; Carrasco, R.; Moreno-Alvarez, P.; Galdeano, R.; Bidegain, E.; Rios-Martin, J.J.; Camacho, F.M. Store-and-forward teledermatology in skin cancer triage: Experience and evaluation of 2009 teleconsultations. Arch. Dermatol. 2007, 143, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Ramirez, D.; Ferrandiz, L.; Bernal, A.P.; Duran, R.C.; Martin, J.J.; Camacho, F. Teledermatology as a filtering system in pigmented lesion clinics. J. Telemed. Telecare 2005, 11, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, M.R.; Wen, C.L.; Neto, C.F.; Silveira, P.S.; Rivitti, E.A.; Böhm, G.M. Web site for training nonmedical health-care workers to identify potentially malignant skin lesions and for teledermatology. Telemed. J. E-Health 2002, 8, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Bogou. Available online: http://raft.unige.ch/bogou/ (accessed on 18 July 2018).
- Bediang, G.; Perrin, C.; Ruiz de Castañeda, R.; Kamga, Y.; Sawadogo, A.; Bagayoko, C.O.; Geissbuhler, A. The RAFT telemedicine network: Lessons learnt and perspectives from a decade of educational and clinical services in low-and middle-incomes countries. Front. Public Health 2014, 2, 180. [Google Scholar] [CrossRef] [PubMed]
- Tran, K.; Ayad, M.; Weinberg, J.; Cherng, A.; Chowdhury, M.; Monir, S.; Hariri, M.; Kovarik, C. Mobile teledermatology in the developing world: Implications of a feasibility study on 30 Egyptian patients with common skin diseases. J. Am. Acad. Dermatol. 2011, 64, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Trettel, A.; Eissing, L.; Augustin, M. Telemedicine in dermatology: Findings and experiences worldwide–A systematic literature review. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Delaigue, S.; Bonnardot, L.; Olson, D.; Morand, J.J. Overview of teledermatology in low-resource settings. Med. Sante Trop. 2015, 25, 365–372. [Google Scholar] [PubMed]
- Khatibi, B.; Bambe, A.; Chantalat, C.; Resche-Rigon, M.; Sanna, A.; Fac, C.; Bagot, M.; Guibal, F. Teledermatology in a prison setting: A retrospective study of 500 expert opinions. Ann. Dermatol. Venereol. 2016, 143, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Yim, K.M.; Florek, A.G.; Oh, D.H.; McKoy, K.; Armstrong, A.W. Teledermatology in the United States: An Update in a Dynamic Era. Telemed. J. E-Health 2018, in press. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Centre | Number of Trainees | Number of Cases Posted via the Platform | Before Training | After Training | ||
|---|---|---|---|---|---|---|
| Number of Skin Diseases (%) | Number of Consults | Number of Skin Diseases (%) | Number of Consults | |||
| Koulikoro a | 2 | 9 | 82 | 900 | 76 | 756 |
| Banamba a | 3 | 32 | 185 | 1512 | 185 | 1426 |
| Nara | 2 | 3 | 95 | 542 | 85 | 501 |
| Sikasso a | 2 | 16 | 692 (65) | 1067 | 706 (63) | 1121 |
| Ngolobougou | 1 | 36 | 51 (8) | 612 | 65 (9) | 723 |
| Kadiolo | 2 | 6 | 60 | 415 | 79 | 608 |
| Mopti a | 4 | 35 b | 108 | 902 | 166 | 1091 |
| Douentza | 2 | 17 b | 45 | 480 | 60 | 461 |
| Bankass | 2 | 26 | 78 | 678 | 106 | 816 |
| TOTAL | 20 | 180 | 1396 | 7108 | 1528 | 7503 |
| Skin Diseases | Before Intervention | After Intervention |
|---|---|---|
| Dermatosis | 322 | 84 |
| Eczema | 6 | 92 |
| Dermatophytosis | - | 47 |
| Mycoses | 30 | 7 |
| Tinea capitis | 3 | 36 |
| Pyoderma | 16 | 193 |
| Wounds | 65 | - |
| Urticaria | - | 11 |
| Allergy | 53 | 14 |
| Follicular infection | 8 | - |
| Pruritus | 28 | - |
| Scabies | 3 | 15 |
| Onychodystrophy | - | 13 |
| Candidiasis | - | 20 |
| Measles | - | 12 |
| Herpes zoster | - | 3 |
| Herpes labialis | - | 5 |
| Genital infection | 44 | 8 |
| Prurigo | 30 | |
| Erysipelas | 7 | 11 |
| Rash | 4 | 8 |
| Molluscum contagiosum | - | 3 |
| Aphthous ulcers | - | 3 |
| Patches | 6 | - |
| Intertrigo | - | 6 |
| Chickenpox | - | 20 |
| Vitiligo | - | 4 |
| Lipoma | - | 1 |
| Miliaria | - | 22 |
| Burn | 4 | - |
| Keloid | - | 4 |
| Ulceration | - | 7 |
| Total | 599 | 679 |
| Skin Disorders | Frequency |
|---|---|
| Sun burn | 2 |
| Eczematised miliaria | 2 |
| Hemangioma | 1 |
| Alopecia areata | 2 |
| Epidermal cyst | 1 |
| Vulvovaginitis | 1 |
| Leprosy | 1 |
| Viral exanthema | 1 |
| Multiple keloid | 2 |
| Transient pustular melanosis | 1 |
| Onychodystrophy | 1 |
| Eruptive hidradenoma | 1 |
| Lichen simplex | 1 |
| Plantar ulcer | 1 |
| Congenital keratoderma | 2 |
| Varicose veins | 2 |
| Total | 22 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faye, O.; Bagayoko, C.O.; Dicko, A.; Cissé, L.; Berthé, S.; Traoré, B.; Fofana, Y.; Niang, M.; Traoré, S.T.; Karabinta, Y.; et al. A Teledermatology Pilot Programme for the Management of Skin Diseases in Primary Health Care Centres: Experiences from a Resource-Limited Country (Mali, West Africa). Trop. Med. Infect. Dis. 2018, 3, 88. https://doi.org/10.3390/tropicalmed3030088
Faye O, Bagayoko CO, Dicko A, Cissé L, Berthé S, Traoré B, Fofana Y, Niang M, Traoré ST, Karabinta Y, et al. A Teledermatology Pilot Programme for the Management of Skin Diseases in Primary Health Care Centres: Experiences from a Resource-Limited Country (Mali, West Africa). Tropical Medicine and Infectious Disease. 2018; 3(3):88. https://doi.org/10.3390/tropicalmed3030088
Chicago/Turabian StyleFaye, Ousmane, Cheick Oumar Bagayoko, Adama Dicko, Lamissa Cissé, Siritio Berthé, Bekaye Traoré, Youssouf Fofana, Mahamoudan Niang, Seydou Tidiane Traoré, Yamoussa Karabinta, and et al. 2018. "A Teledermatology Pilot Programme for the Management of Skin Diseases in Primary Health Care Centres: Experiences from a Resource-Limited Country (Mali, West Africa)" Tropical Medicine and Infectious Disease 3, no. 3: 88. https://doi.org/10.3390/tropicalmed3030088
APA StyleFaye, O., Bagayoko, C. O., Dicko, A., Cissé, L., Berthé, S., Traoré, B., Fofana, Y., Niang, M., Traoré, S. T., Karabinta, Y., Gassama, M., Guindo, B., Keita, A., Tall, K., Keita, S., Geissbuhler, A., Mahé, A., & Teledermali Team. (2018). A Teledermatology Pilot Programme for the Management of Skin Diseases in Primary Health Care Centres: Experiences from a Resource-Limited Country (Mali, West Africa). Tropical Medicine and Infectious Disease, 3(3), 88. https://doi.org/10.3390/tropicalmed3030088