Young Adults in Endemic Areas: An Untreated Group in Need of School-Based Preventive Chemotherapy for Schistosomiasis Control and Elimination

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Health Assembly Resolution WHA 54.19 Elimination of Schistosomiasis. 2001. Available online: http://www.who.int/entity/neglected_diseases/mediacentre/WHA_54.19_Eng.pdf?ua=1 (accessed on 10 February 2017).
- World Health Organization. World Health Assembly Resolution WHA 65.21 Elimination of Schistosomiasis. 2012. Available online: http://www.who.int/neglected_diseases/mediacentre/WHA_65.21_Eng.pdf (accessed on 15 February 2017).
- Abudho, B.O.; Ndombi, E.M.; Guya, B.; Carter, J.M.; Riner, D.K.; Kittur, N.; Karanja, D.M.S.; Secor, W.E.; Colley, D.G. Impact of four years of annual mass drug administration on prevalence and intensity of schistosomiasis among primary and high school children in Western Kenya: A repeated cross-sectional study. Am. J. Trop. Med. Hyg. 2018, 98, 1397–1402. [Google Scholar] [CrossRef] [PubMed]
- Masaku, M.F.; Gichuki, P.M.; Okoyo, C.; Njenga, S.M. High prevalence of helminths infection and associated risk factors among adults living in a rural setting, central Kenya: A cross-sectional study. Trop. Med. Health 2017, 45, 15. [Google Scholar] [CrossRef] [PubMed]
- Riner, D.K.; Ndombi, E M.; Carter, J.M.; Omondi, A.; Kittur, N.; Kavere, E.; Korir, H.K.; Flaherty, B.; Karanja, D.; Colley, D.G. Schistosoma mansoni infection can jeopardize the duration of protective levels of antibody responses to immunizations against hepatitis B and tetanus toxoid. PLoS Negl. Trop. Dis. 2016, 10, e0005180. [Google Scholar]
- Katz, N.; Chaves, A.; Pellegrino, J. A simple device for quantitative stool thick-smear technique in Schistosomiasis mansoni. Rev. Inst. Med. Trop. Sao Paulo 1972, 14, 397–400. [Google Scholar] [PubMed]
- World Health Organization. Helminth Control in School Age Children. A Guide for Control Managers. 2011. Available online: http://apps.who.int/iris/bitstream/handle/10665/44671/9789241548267_eng.pdf;jsessionid=1906846F5DDE37F11A805DE0E5BD5F44?sequence=1 (accessed on 23 May 2013).
- Clements, M.N.; Donnelly, C.A.; Fenwick, A.; Kabatereine, N.B.; Knowles, S.C L.; Meité, A.; N’Goran, E.K.; Nalule, Y.; Nogaro, S.; Phillips, A.E.; et al. Interpreting ambiguous ‘trace’ results in Schistosoma mansoni CCA Tests: Estimating sensitivity and specificity of ambiguous results with no gold standard. PLoS Negl. Trop. Dis. 2017, 11, e0006102. [Google Scholar] [CrossRef] [PubMed]
- Colley, D.G.; Andros, T.S.; Campbell, C.H. Schistosomiasis is more prevalent than previously thought: What does it mean for public health goals, policies, strategies, guidelines and intervention programs? Infect. Dis. Poverty 2017, 6, 63. [Google Scholar] [CrossRef] [PubMed]
- Ogongo, P.; Kariuki, T.M.; Wilson, R.A. Diagnosis of schistosomiasis mansoni: An evaluation of existing methods and research towards single worm pair detection. Parasitology 2018. [Google Scholar] [CrossRef] [PubMed]
- Danso-Appiah, A.; Minton, J.; Boamah, D.; Otchere, J.; Asmah, R.H.; Rodgers, M.; Bosompem, K.M.; Eusebi, P.; De Vlas, S.J. Accuracy of point-of-care testing for circulatory cathodic antigen in the detection of schistosome infection: Systematic review and meta-analysis. Bull. World Health Organ. 2016, 94, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Kittur, N.; Castleman, J.D.; Campbell, C.H.; King, C.H.; Colley, D.G. Comparison of Schistosoma mansoni prevalence and intensity of infection, as determined by the circulating cathodic antigen urine assay or by the Kato-Katz fecal assay: A systematic review. Am. J. Trop. Med. Hyg. 2016, 94, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Utzinger, J.; Raso, G.; Brooker, S.; De Savigny, D.; Tanner, M.; Ornbjerg, N.; Singer, B.H.; N’goran, E.K. Schistosomiasis and neglected tropical diseases: Towards integrated and sustainable control and a word of caution. Parasitology 2009, 136, 1859–1874. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prevention and Control of Schistosomiasis and Soil-Transmitted Helminthiasis. 2002. Available online: http://apps.who.int/iris/bitstream/handle/10665/42588/WHO_TRS_912.pdf?sequence=1&isAllowed=y (accessed on 31 July 2018).
- Vennervald, B.J.; Dunne, D.W. Morbidity in schistosomiasis: an update. Curr. Opin. Infect. Dis. 2004, 17, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Ezeamama, A.E.; He, C.L.; Shen, Y.; Yin, X.P.; Binder, S.C.; Campbell, C.H.; Rathbun, S.; Whalen, C.C.; N’Goran, E.K.; Utzinger, J.; et al. Gaining and sustaining schistosomiasis control: Study protocol and baseline data prior to different treatment strategies in five African countries. BMC Infect. Dis. 2016, 16, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, C.H.; Sturrock, R.F.; Kariuki, H.C.; Hamburger, J. Transmission control for schistosomiasis—Why it matters now. Trends Parasitol. 2006, 22, 575–582. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | Number of Participants (%) | ||
|---|---|---|---|
| Age, median (range) years | 22 (17–41) | ||
| Male sex | 132 (45.4%) | ||
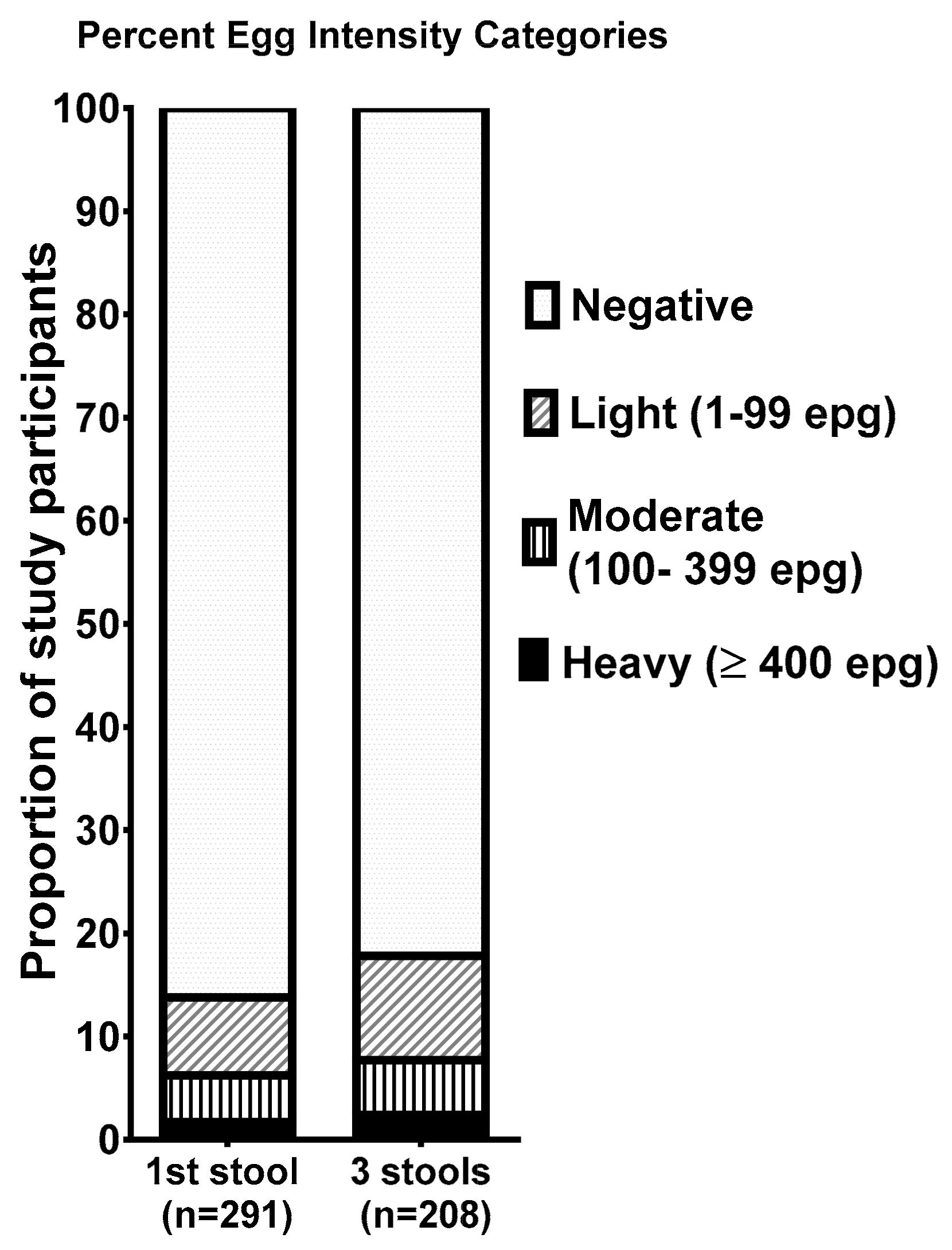
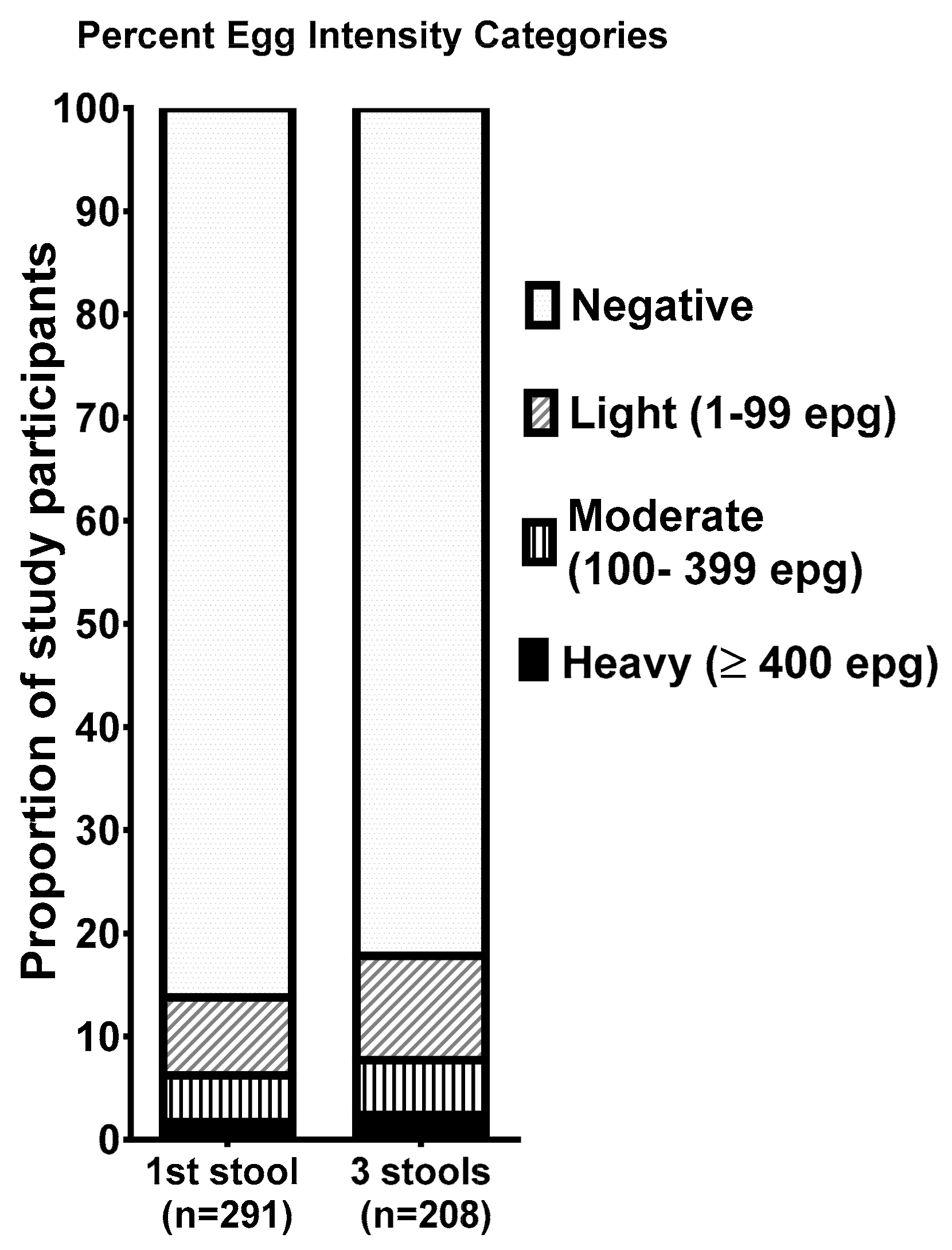
| Prevalence of helminth infections | 1 urine sample (CCA) (n = 276) | 1 stool sample (n = 291) | 3 stool samples (n = 208) |
| Schistosoma mansoni prevalence (%) | 64 (23.2%) | 40 (13.7%) | 37 (17.8%) |
| Ascaris lumbricoides prevalence (%) | N/A | 4 (1.4%) | 4 (1.4%) |
| Trichuris trichiura prevalence (%) | N/A | 7 (2.4%) | 9 (3.1%) |
| Hookworm prevalence (%) | N/A | 4 (1.4%) | 12 (4.1%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korir, H.K.; Riner, D.K.; Kavere, E.; Omondi, A.; Landry, J.; Kittur, N.; Ndombi, E.M.; Ondigo, B.N.; Secor, W.E.; Karanja, D.M.S.; et al. Young Adults in Endemic Areas: An Untreated Group in Need of School-Based Preventive Chemotherapy for Schistosomiasis Control and Elimination. Trop. Med. Infect. Dis. 2018, 3, 100. https://doi.org/10.3390/tropicalmed3030100
Korir HK, Riner DK, Kavere E, Omondi A, Landry J, Kittur N, Ndombi EM, Ondigo BN, Secor WE, Karanja DMS, et al. Young Adults in Endemic Areas: An Untreated Group in Need of School-Based Preventive Chemotherapy for Schistosomiasis Control and Elimination. Tropical Medicine and Infectious Disease. 2018; 3(3):100. https://doi.org/10.3390/tropicalmed3030100
Chicago/Turabian StyleKorir, Harrison K., Diana K. Riner, Emmy Kavere, Amos Omondi, Jasmine Landry, Nupur Kittur, Eric M. Ndombi, Bartholomew N. Ondigo, W. Evan Secor, Diana M. S. Karanja, and et al. 2018. "Young Adults in Endemic Areas: An Untreated Group in Need of School-Based Preventive Chemotherapy for Schistosomiasis Control and Elimination" Tropical Medicine and Infectious Disease 3, no. 3: 100. https://doi.org/10.3390/tropicalmed3030100
APA StyleKorir, H. K., Riner, D. K., Kavere, E., Omondi, A., Landry, J., Kittur, N., Ndombi, E. M., Ondigo, B. N., Secor, W. E., Karanja, D. M. S., & Colley, D. G. (2018). Young Adults in Endemic Areas: An Untreated Group in Need of School-Based Preventive Chemotherapy for Schistosomiasis Control and Elimination. Tropical Medicine and Infectious Disease, 3(3), 100. https://doi.org/10.3390/tropicalmed3030100