
Impact of Nutritional Counselling and Support on Body Mass Index Recovery and Treatment Outcomes Among Tuberculosis Patients in the Lao People’s Democratic Republic

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Study Design
2.3. Data Collection
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Changes in BMI During TB Treatment
3.3. TB Treatment Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Portnoy, A.; Yamanaka, T.; Nguhiu, P.; Nishikiori, N.; Baena, I.G.; Floyd, K.; A Menzies, N. Costs incurred by people receiving tuberculosis treatment in low-income and middle-income countries: A meta-regression analysis. Lancet Glob. Health 2023, 11, e1640–e1647. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2024; World Health Organization: Geneva, Switzerland, 2024. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2023; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- WHO Report Shows Global Tuberculosis Cases Are Rising [Internet]. 2024. Available online: https://www.cidrap.umn.edu/tuberculosis/who-report-shows-global-tuberculosis-cases-are-rising (accessed on 30 April 2025).
- Global Fund. Tuberculosis; Global Fund: Geneva, Switzerland, 2024. [Google Scholar]
- Sinha, P.; Ponnuraja, C.; Gupte, N.; Babu, S.P.; Cox, S.R.; Sarkar, S.; Mave, V.; Paradkar, M.; Cintron, C.; Govindarajan, S.; et al. Impact of Undernutrition on Tuberculosis Treatment Outcomes in India: A Multicenter, Prospective, Cohort Analysis. Clin. Infect. Dis. 2023, 76, 1483–1491. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dauphinais, M.R.; Koura, K.G.; Narasimhan, P.B.; Mehta, S.; Finkelstein, J.L.; Heysell, S.K.; Sinha, P. Nutritionally acquired immunodeficiency must be addressed with the same urgency as HIV to end tuberculosis. BMC Glob. Public. Health 2024, 2, 4. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Scrimshaw, N.S.; SanGiovanni, J.P. Synergism of nutrition, infection, and immunity: An overview. Am. J. Clin. Nutr. 1997, 66, 464S–477S. [Google Scholar] [CrossRef] [PubMed]
- Lonnroth, K.; Williams, B.G.; Cegielski, P.; Dye, C. A consistent log-linear relationship between tuberculosis incidence and body mass index. Int. J. Epidemiol. 2010, 39, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, A.; Bhargava, M.; Meher, A.; Teja, G.S.; Velayutham, B.; Watson, B.; Benedetti, A.; Barik, G.; Singh, V.P.; Singh, D.; et al. Nutritional support for adult patients with microbiologically confirmed pulmonary tuberculosis: Outcomes in a programmatic cohort nested within the RATIONS trial in Jharkhand, India. Lancet Glob. Health 2023, 11, e1402–e1411. [Google Scholar] [CrossRef] [PubMed]
- Darnton-Hill, I.; Mandal, P.P.; de Silva, A.; Bhatia, V.; Sharma, M. Opportunities to prevent and manage undernutrition to amplify efforts to end TB. Int. J. Tuberc. Lung Dis. 2022, 26, 6–11. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Franke, M.A.; Emmrich, J.V.; Ranjaharinony, F.; Ravololohanitra, O.G.; Andriamasy, H.E.; Knauss, S.; Muller, N. A cross-sectional analysis of the effectiveness of a nutritional support programme for people with tuberculosis in Southern Madagascar using secondary data from a non-governmental organisation. Infect. Dis. Poverty 2024, 13, 13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Padmapriyadarsini, C.; Shobana, M.; Lakshmi, M.; Beena, T.; Swaminathan, S. Undernutrition & tuberculosis in India: Situation analysis & the way forward. Indian. J. Med. Res. 2016, 144, 11–20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Franco, J.V.; Bongaerts, B.; Metzendorf, M.-I.; Risso, A.; Guo, Y.; Silva, L.P.; Boeckmann, M.; Schlesinger, S.; Damen, J.A.; Richter, B.; et al. Undernutrition as a risk factor for tuberculosis disease. Cochrane Database Syst Rev. 2024, 6, CD015890. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Health Organization. The End TB Strategy; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization. Guideline: Nutritional Care and Support for Patients with Tuberculosis; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Yen, Y.-F.; Chuang, P.-H.; Yen, M.-Y.; Lin, S.-Y.; Chuang, P.; Yuan, M.-J.; Ho, B.-L.; Chou, P.; Deng, C.-Y. Association of Body Mass Index with Tuberculosis Mortality: A Population-Based Follow-Up Study. Medicine 2016, 95, e2300. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bhargava, A.; Bhargava, M. Tuberculosis deaths are predictable and preventable: Comprehensive assessment and clinical care is the key. J. Clin. Tuberc. Other Mycobact. Dis. 2020, 19, 100155. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wondmieneh, A.; Gedefaw, G.; Getie, A.; Demis, A. Prevalence of undernutrition among adult tuberculosis patients in Ethiopia: A systematic review and meta-analysis. J. Clin. Tuberc. Other Mycobact. Dis. 2021, 22, 100211. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ockenga, J.; Fuhse, K.; Chatterjee, S.; Malykh, R.; Rippin, H.; Pirlich, M.; Yedilbayev, A.; Wickramasinghe, K.; Barazzoni, R. Tuberculosis and malnutrition: The European perspective. Clin. Nutr. 2023, 42, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, A.; Chatterjee, M.; Jain, Y.; Chatterjee, B.; Kataria, A.; Bhargava, M.; Kataria, R.; D’sOuza, R.; Jain, R.; Benedetti, A.; et al. Nutritional status of adult patients with pulmonary tuberculosis in rural central India and its association with mortality. PLoS ONE 2013, 8, e77979. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zachariah, R.; Spielmann, M.P.; Harries, A.D.; Salaniponi, F.M. Moderate to severe malnutrition in patients with tuberculosis is a risk factor associated with early death. Trans. R. Soc. Trop. Med. Hyg. 2002, 96, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.P.; Nancy, A.P.; Moideen, K.; Menon, P.A.; Banurekha, V.V.; Nair, D.; Nott, S.; Babu, S. Low body mass index is associated with diminished plasma cytokines and chemokines in both active and latent tuberculosis. Front. Nutr. 2023, 10, 1194682. [Google Scholar] [CrossRef] [PubMed]
- Carwile, M.E.; Hochberg, N.S.; Sinha, P. Undernutrition is feeding the tuberculosis pandemic: A perspective. J. Clin. Tuberc. Other Mycobact. Dis. 2022, 27, 100311. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ministry of Health, Lao People’s Democratic Republic. National Nutrition Strategy to 2025 and Plan of Action 2016–2020; Ministry of Health, Lao People’s Democratic Republic: Vientiane, Laos, 2016.
- United Nations. Department of Economic and Social Affairs. SDG Indicator Database; SDG Country Profile, Lao People’s Democratic Republic. Available online: https://unstats.un.org/sdgs/dataportal/countryprofiles/lao#goal-3 (accessed on 30 April 2025).
- World Bank Open Data [Internet]. Available online: https://data.worldbank.org/indicator/SH.STA.MALN.ZS?locations=LA (accessed on 30 April 2025).
- World Bank Open Data [Internet]. Available online: https://data.worldbank.org/indicator/SH.STA.STNT.ZS?locations=LA (accessed on 30 April 2025).
- Ministry of Planning and Investment, Lao People’s Democratic Republic. 9th Five-Year National Socio-Economic Development Plan (2021–2025); Ministry of Planning and Investment, Lao People’s Democratic Republic: Vientiane, Laos, 2021.
- Ministry of Health, Lao People’s Democratic Republic. Health Sector Reform Strategy and Framework till 2025; Ministry of Planning and Investment, Lao People’s Democratic Republic: Vientiane, Laos, 2016.
- Chittamany, P.; Yamanaka, T.; Suthepmany, S.; Sorsavanh, T.; Siphanthong, P.; Sebert, J.; Viney, K.; Vixaysouk, T.; Nagai, M.; Seevisay, V.; et al. First national tuberculosis patient cost survey in Lao People’s Democratic Republic: Assessment of the financial burden faced by TB-affected households and the comparisons by drug-resistance and HIV status. PLoS ONE 2020, 15, e0241862. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tuberculosis Patient Cost Surveys: A Hand Book; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Inthavong, D.; Elsayed, H.; Keonakhone, P.; Seevisay, V.; Souksanh, S.; Suthepmany, S.; Chanthavong, M.; Keodavong, X.; Kommanivanh, P.; Siphanthong, P.; et al. The prevalence of undernutrition and associated risk factors in people with tuberculosis in Lao People’s Democratic Republic. PLoS ONE 2025, 20, e0324838. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Inthavong, D.; Elsayed, H.; Keonakhone, P.; Seevisay, V.; Souksanh, S.; Suthepmany, S.; Siphanthong, P.; Sengmany, P.; Sisounon, B.; Sebert, J.; et al. Does nutritional support contribute to mitigating the financial burden faced by TB-affected households? IJTLD Open 2025, 2, 260–268. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. National Surveys of Costs Faced by Tuberculosis Patients and Their Households 2015–2021; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Ter Beek, L.; Bolhuis, M.S.; Jager-Wittenaar, H.; Brijan, R.X.D.; Sturkenboom, M.G.G.; Kerstjens, H.A.M.; de Lange, W.C.M.; Tiberi, S.; van der Werf, T.S.; Alffenaar, J.-W.C.; et al. Malnutrition assessment methods in adult patients with tuberculosis: A systematic review. BMJ Open 2021, 11, e049777. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gupta, K.B.; Gupta, R.; Atreja, A.; Verma, M.; Vishvkarma, S. Tuberculosis and nutrition. Lung India 2009, 26, 9–16. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Campbell, J.R.; Chan, E.D.; Falzon, D.; Trajman, A.; Keshavjee, S.; Leung, C.C.; Miller, A.C.; Monedero-Recuero, I.; Rodrigues, D.S.; Seo, H.; et al. Low Body Mass Index at Treatment Initiation and Rifampicin-Resistant Tuberculosis Treatment Outcomes: An Individual Participant Data Meta-Analysis. Clin. Infect. Dis. 2022, 75, 2201–2210. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.H.; Lai, Y.J.; Yen, Y.F. Association of Body Mass Index with Timing of Death during Tuberculosis Treatment. PLoS ONE 2017, 12, e0170104. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sahile, Z.; Tezera, R.; Haile Mariam, D.; Collins, J.; Ali, J.H. Nutritional status and TB treatment outcomes in Addis Ababa, Ethiopia: An ambi-directional cohort study. PLoS ONE 2021, 16, e0247945. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shah, V.; Murugan, Y.; Patel, S.S.; Trivedi, N.S.; Pithadiya, D.; Makwana, N.; Parmar, D. Nutritional Supplementation in Tuberculosis Treatment: A Mixed Methods Study of Clinical Outcomes and Patient Perceptions in Jamnagar, India. Cureus 2024, 16, e70300. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tola, A.; Minshore, K.M.; Ayele, Y.; Mekuria, A.N. Tuberculosis Treatment Outcomes and Associated Factors among TB Patients Attending Public Hospitals in Harar Town, Eastern Ethiopia: A Five-Year Retrospective Study. Tuberc. Res. Treat. 2019, 2019, 1503219. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chilyabanyama, R.; Kamanga, N.; Mwandia, J.N. Factors associated with tuberculosis treatment outcomes among TB patients aged 15 years and older at chawama level one hospital in Lusaka, Zambia. Glob. Public Health 2024, 19, 2307979. [Google Scholar] [CrossRef] [PubMed]
- Chaves Torres, N.M.; Quijano Rodriguez, J.J.; Porras Andrade, P.S.; Arriaga, M.B.; Netto, E.M. Factors predictive of the success of tuberculosis treatment: A systematic review with meta-analysis. PLoS ONE 2019, 14, e0226507. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kabuya, M.; Musekiwa, A.; Takuva, S.; Thabane, L.; Mbuagbaw, L. Predictors of tuberculosis treatment outcome at Senkatana clinic in Lesotho. Pan Afr. Med. J. 2024, 49, 91. [Google Scholar] [CrossRef] [PubMed]
- Sariem, C.N.; Odumosu, P.; Dapar, M.P.; Musa, J.; Ibrahim, L.; Aguiyi, J. Tuberculosis treatment outcomes: A fifteen-year retrospective study in Jos-North and Mangu, Plateau State, North—Central Nigeria. BMC Public Health 2020, 20, 1224. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zenatti, G.; Raviglione, M.; Tesfaye, F.; Bobosha, K.; Björkman, P.; Walles, J. High variability in tuberculosis treatment outcomes across 15 health facilities in a semi-urban area in central Ethiopia. J. Clin. Tuberc. Other Mycobact. Dis. 2023, 30, 100344. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gatechompol, S.; Kawkitinarong, K.; Suwanpimolkul, G.; Kateruttanakul, P.; Manosuthi, W.; Sophonphan, J.; Ubolyam, S.; Kerr, S.J.; Avihingsanon, A.; Ruxrungtham, K. Treatment outcomes and factors associated with mortality among individuals with both TB and HIV in the antiretroviral era in Thailand. J. Virus Erad. 2019, 5, 225–230. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- van de Water, B.J.; Fulcher, I.; Cilliers, S.; Meyer, N.; Wilson, M.; Young, C.; Gaunt, B.; le Roux, K.; Isaakidis, P. Association of HIV infection and antiretroviral therapy with the occurrence of an unfavorable TB treatment outcome in a rural district hospital in Eastern Cape, South Africa: A retrospective cohort study. PLoS ONE 2022, 17, e0266082. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Choi, H.; Lee, M.; Chen, R.Y.; Kim, Y.; Yoon, S.; Joh, J.S.; Park, S.K.; E Dodd, L.; Lee, J.; Song, T.; et al. Predictors of pulmonary tuberculosis treatment outcomes in South Korea: A prospective cohort study, 2005-2012. BMC Infect. Dis. 2014, 14, 360. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wagnew, F.; Gray, D.; Tsheten, T.; Kelly, M.; Clements, A.C.A.; Alene, K.A. Effectiveness of nutritional support to improve treatment adherence in patients with tuberculosis: A systematic review. Nutr. Rev. 2024, 82, 1216–1225. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Thomas, B.E.; Thiruvengadam, K.; Rani, S.; Kadam, D.; Ovung, S.; Sivakumar, S.; Shivakumar, S.V.B.Y.; Paradkar, M.; Gupte, N.; Suryavanshi, N.; et al. Smoking, alcohol use disorder and tuberculosis treatment outcomes: A dual co-morbidity burden that cannot be ignored. PLoS ONE 2019, 14, e0220507, Erratum in PLoS ONE 2019, 14, e0224914. 10.1371/journal.pone.0224914. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ragan, E.J.; Kleinman, M.B.; Sweigart, B.; Gnatienko, N.; Parry, C.D.; Horsburgh, C.R.; LaValley, M.P.; Myers, B.; Jacobson, K.R. The impact of alcohol use on tuberculosis treatment outcomes: A systematic review and meta-analysis. Int. J. Tuberc. Lung Dis. 2020, 24, 73–82. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Miyoshi, M.; Phommasack, B.; Nakamura, S.; Kuroiwa, C. Nutritional status of children in rural Lao PDR: Who are the most vulnerable? Eur. J. Clin. Nutr. 2005, 59, 887–890. [Google Scholar] [CrossRef] [PubMed]
- Multi-Sector Convergence Approach to Reducing Malnutrition in Lao PDR [Internet]. 2022. Available online: https://www.worldbank.org/en/country/lao/brief/multi-sector-convergence-approach-to-reducing-malnutrition-in-lao-pdr (accessed on 30 April 2025).
- Li, A.; Yuan, S.Y.; Li, Q.G.; Li, J.X.; Yin, X.Y.; Liu, N.N. Prevalence and risk factors of malnutrition in patients with pulmonary tuberculosis: A systematic review and meta-analysis. Front. Med. 2023, 10, 1173619. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]


{kind=link}
{kind=link}
{kind=link}
| Variable | Category | Observation Group N (%) | Intervention Group N (%) | Total N (%) | p-Value |
|---|---|---|---|---|---|
| Total | 154 (51.9) | 143 (48.1) | 297 (100) | - | |
| Demographic characteristics | |||||
| Age group (years) | Mean (SD) | 48.9 (18.3) | 47.7 (16.1) | 48.3 (17.3) | 0.567 |
| 0–14 | 1 (0.6) | 0 (0.0) | 1 (0.3) | 0.347 | |
| 15–24 | 16 (10.4) | 11 (7.7) | 27 (9.1) | ||
| 25–34 | 28 (18.2) | 25 (17.5) | 53 (17.8) | ||
| 35–44 | 17 (11.0) | 23 (16.1) | 40 (13.5) | ||
| 45–54 | 26 (16.9) | 30 (21.0) | 56 (18.9) | ||
| 55–64 | 28 (18.2) | 31 (21.7) | 59 (19.9) | ||
| 65+ | 38 (24.7) | 23 (16.1) | 61 (20.5) | ||
| Sex | Female | 66 (42.9) | 46 (32.2) | 112 (37.7) | 0.075 |
| Male | 88 (57.1) | 97 (67.8) | 185 (62.3) | ||
| Marital status | Single | 40 (26.0) | 32 (22.4) | 72 (24.2) | 0.289 |
| Married | 87 (56.5) | 93 (65.0) | 180 (60.6) | ||
| Divorced/separated/widowed | 27 (17.5) | 18 (12.6) | 45 (15.2) | ||
| Insurance type | None | 52 (33.8) | 56 (39.2) | 108 (36.4) | 0.557 |
| National Health Insurance | 86 (55.8) | 76 (53.1) | 162 (54.5) | ||
| Community-Based Health Insurance | 2 (1.3) | 1 (0.7) | 3 (1.0) | ||
| Social Security Organization | 5 (3.2) | 4 (2.8) | 9 (3.0) | ||
| State Authority for Social Security | 6 (3.9) | 5 (3.5) | 11 (3.7) | ||
| Private health insurance | 3 (1.9) | 0 (0.0) | 3 (1.0) | ||
| Other | 0 (0.0) | 1 (0.7) | 1 (0.3) | ||
| Smoker | No smoking experience | 83 (53.9) | 66 (46.2) | 149 (50.2) | 0.383 |
| Current smoker | 13 (8.4) | 16 (11.2) | 29 (9.8) | ||
| Ex-smoker | 58 (37.7) | 61 (42.7) | 119 (40.1) | ||
| Alcohol use | Daily | 10 (6.5) | 15 (10.5) | 25 (8.4) | 0.324 |
| Weekly | 13 (8.4) | 18 (12.6) | 31 (10.4) | ||
| Monthly | 17 (11.0) | 12 (8.4) | 29 (9.8) | ||
| Rarely/Never | 114 (74.0) | 98 (68.5) | 212 (71.4) | ||
| Educational level | No education | 20 (13.0) | 10 (7.0) | 30 (10.1) | 0.249 |
| Primary | 40 (26.0) | 36 (25.2) | 76 (25.6) | ||
| Lower/higher secondary | 69 (44.8) | 65 (45.5) | 134 (45.1) | ||
| Diploma or higher, vocational, other | 25 (16.2) | 32 (22.4) | 57 (19.2) | ||
| Employment status before TB | Unemployed | 44 (28.6) | 31 (21.7) | 75 (25.3) | 0.038 |
| Formal paid work | 19 (12.3) | 27 (18.9) | 46 (15.5) | ||
| Informal paid work | 67 (43.5) | 74 (51.7) | 141 (47.5) | ||
| Retired/student/housework/other | 24 (15.6) | 11 (7.7) | 35 (11.8) | ||
| Clinical characteristics | |||||
| TB type | Pulmonary, bacteriologically confirmed | 111 (72.1) | 101 (70.6) | 212 (71.4) | 0.800 |
| Pulmonary, bacteriologically unconfirmed (clinically diagnosed) | 36 (23.4) | 33 (23.1) | 69 (23.2) | ||
| Extrapulmonary | 7 (4.5) | 9 (6.3) | 16 (5.4) | ||
| HIV status | HIV negative | 135 (87.7) | 120 (83.9) | 255 (85.9) | 0.428 |
| HIV positive | 19 (12.3) | 22 (15.4) | 41 (13.8) | ||
| HIV test not done | 0 (0.0) | 1 (0.7) | 1 (0.3) | ||
| Treatment history | New | 145 (94.2) | 136 (95.1) | 281 (94.6) | 0.227 |
| Relapse | 6 (3.9) | 7 (4.9) | 13 (4.4) | ||
| Retreatment | 3 (1.9) | 0 (0.0) | 3 (1.0) | ||
| Diagnostic delay | No | 72 (46.8) | 79 (55.2) | 151 (50.8) | 0.178 |
| Yes (>4 weeks from onset of TB symptoms) | 82 (53.2) | 64 (44.8) | 146 (49.2) | ||
| Variables | Phase | Observation Group | Intervention Group | p-Value |
|---|---|---|---|---|
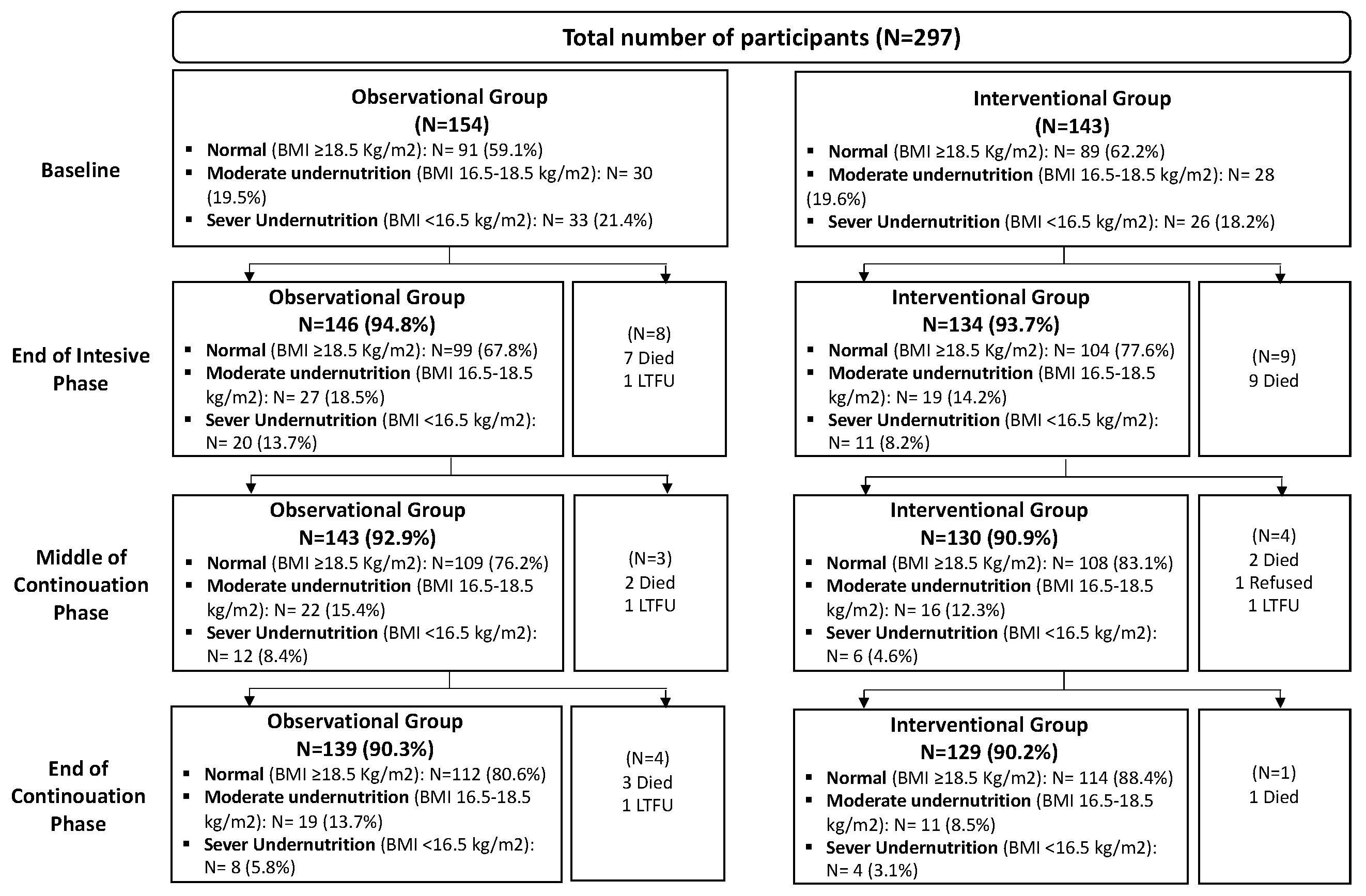
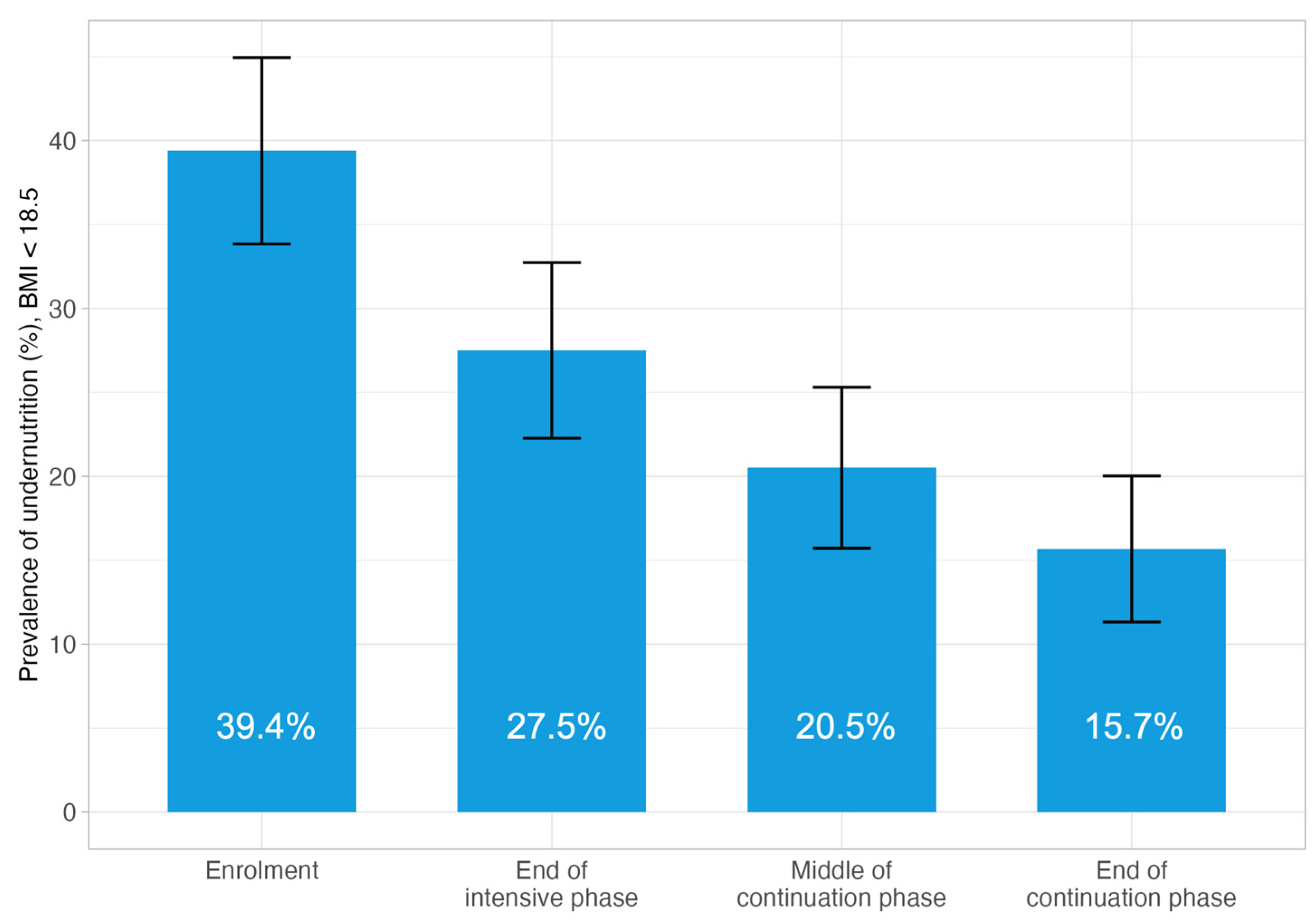
| Prevalence of BMI * < 18.5 | At TB diagnosis | 40.9% | 37.8% | 0.663 |
| End of intensive phase | 32.2% | 22.4% | 0.089 | |
| Middle of continuation phase | 23.8% | 16.9% | 0.211 | |
| End of continuation phase | 19.4% | 11.6% | 0.113 | |
| Prevalence of BMI * < 16.5 | At TB diagnosis | 21.4% | 18.2% | 0.773 |
| End of intensive phase | 13.7% | 8.2% | 0.164 | |
| Middle of continuation phase | 8.4% | 4.6% | 0.311 | |
| End of continuation phase | 5.8% | 3.1% | 0.211 |
| Variable | Category | Observation Group; N (%) | Intervention Group; N (%) | Total; N (%) | p-Value |
|---|---|---|---|---|---|
| Treatment outcomes | Treatment success | 139 (90.3) | 130 (90.9) | 269 (90.6) | 0.639 |
| Treatment failure | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Died | 12 (7.8) | 12 (8.4) | 24 (8.1) | ||
| Lost to follow-up | 3 (1.9) | 1 (0.6) | 4 (1.3) | ||
| Occurrence of deaths during TB treatment | End of intensive phase | 7 (4.6) | 9 (6.3) | 16 (5.4) | 0.929 |
| Middle of continuation phase | 2 (1.3) | 2 (1.4) | 4 (1.4) | ||
| End of continuation phase | 3 (1.9) | 1 (0.7) | 4 (1.4) |
| Variable | Category | N | n (%) | p-Value | Crude OR (95% CI, p-Value) | Adjusted OR (95% CI, p-Value) |
|---|---|---|---|---|---|---|
| Age group | 65+ | 61 | 54 (88.5%) | 0.781 | Ref | Ref |
| 0–44 | 121 | 111 (91.7%) | 1.44 (0.50–3.95, p = 0.484) | 4.26 (1.17–17.01, p = 0.031) | ||
| 45–64 | 115 | 104 (90.4%) | 1.23 (0.43–3.29, p = 0.691) | 1.44 (0.48–4.11, p = 0.504) | ||
| Sex | Male | 185 | 163 (88.1%) | 0.096 | Ref | Ref |
| Female | 112 | 106 (94.6%) | 2.38 (0.99–6.65, p = 0.069) | 2.30 (0.92–6.62, p = 0.094) | ||
| Marital status | Single | 72 | 65 (90.3%) | 0.897 | Ref | - |
| Married | 180 | 164 (91.1%) | 1.10 (0.41–2.72, p = 0.836) | - | ||
| Divorced/separated/widowed | 45 | 40 (88.9%) | 0.86 (0.26–3.08, p = 0.810) | - | ||
| Insurance type | No insurance | 108 | 95 (88.0%) | 0.339 | Ref | - |
| With insurance | 189 | 174 (92.1%) | 1.59 (0.72–3.48, p = 0.248) | - | ||
| Smoking status | Current smoker | 29 | 23 (79.3%) | 0.059 | Ref | - |
| No smoking experience | 149 | 139 (93.3%) | 3.63 (1.14–10.77, p = 0.022) | - | ||
| Ex-smoker | 119 | 107 (89.9%) | 2.33 (0.75–6.67, p = 0.125) | - | ||
| Alcohol use | Daily | 25 | 23 (92.0%) | 0.580 | Ref | - |
| Weekly | 31 | 26 (83.9%) | 0.45 (0.06–2.32, p = 0.369) | - | ||
| Monthly | 29 | 27 (93.1%) | 1.17 (0.13–10.42, p = 0.877) | - | ||
| Rarely/Never | 212 | 193 (91.0%) | 0.88 (0.14–3.32, p = 0.873) | - | ||
| HIV status | HIV positive | 41 | 32 (78.0%) | 0.012 | Ref | Ref |
| HIV negative | 255 | 236 (92.5%) | 3.49 (1.40–8.22, p = 0.005) | 9.49 (2.83–34.67, p < 0.001) | ||
| Status unknown | 1 | 1 (100.0%) | - | - | ||
| Educational level | No education | 30 | 26 (86.7%) | 0.717 | Ref | - |
| Primary | 76 | 71 (93.4%) | 2.18 (0.51–8.88, p = 0.270) | - | ||
| Lower/higher secondary | 134 | 121 (90.3%) | 1.43 (0.38–4.43, p = 0.557) | - | ||
| Diploma or higher, vocational, other | 57 | 51 (89.5%) | 1.31 (0.31–4.99, p = 0.697) | - | ||
| Employment status before TB | Unemployed | 75 | 69 (92.0%) | 0.820 | Ref | - |
| Formal paid work | 46 | 40 (87.0%) | 0.58 (0.17–1.97, p = 0.372) | - | ||
| Informal paid work | 141 | 128 (90.8%) | 0.86 (0.29–2.27, p = 0.763) | - | ||
| Retired/student/housework/other | 35 | 32 (91.4%) | 0.93 (0.23–4.61, p = 0.919) | - | ||
| Nutritional intervention | Without any intervention | 154 | 139 (90.3%) | 1.000 | Ref | - |
| With nutritional intervention | 143 | 130 (90.9%) | 1.08 (0.49–2.39, p = 0.848) | - | ||
| TB type | Pulmonary, bacteriologically confirmed | 212 | 190 (89.6%) | 0.480 | Ref | Ref |
| Pulmonary, clinically diagnosed | 69 | 65 (94.2%) | 1.88 (0.69–6.61, p = 0.261) | 3.26 (1.05–12.87, p = 0.060) | ||
| Extrapulmonary | 16 | 14 (87.5%) | 0.81 (0.21–5.38, p = 0.790) | 1.17 (0.24–9.11, p = 0.859) | ||
| Treatment history | Relapse/retreatment | 16 | 14 (87.5%) | 1.000 | Ref | - |
| New | 281 | 255 (90.7%) | 1.40 (0.21–5.39, p = 0.667) | - | ||
| Household size | ≥5 | 149 | 131 (87.9%) | 0.170 | Ref | Ref |
| <5 | 148 | 138 (93.2%) | 1.90 (0.86–4.41, p = 0.121) | 2.21 (0.95–5.49, p = 0.073) | ||
| Diagnostic delay | No | 151 | 136 (90.1%) | 0.916 | Ref | - |
| Yes | 146 | 133 (91.1%) | 1.13 (0.52–2.50, p = 0.762) | - | ||
| BMI at TB diagnosis | <18.5 | 117 | 102 (87.2%) | 0.159 | Ref | Ref |
| ≥18.5 | 180 | 167 (92.8%) | 1.89 (0.86–4.19, p = 0.111) | 1.85 (0.79–4.37, p = 0.153) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inthavong, D.; Elsayed, H.; Keonakhone, P.; Seevisay, V.; Souksanh, S.; Suthepmany, S.; Chanthavong, M.; Keodavong, X.; Kommanivanh, P.; Siphanthong, P.; et al. Impact of Nutritional Counselling and Support on Body Mass Index Recovery and Treatment Outcomes Among Tuberculosis Patients in the Lao People’s Democratic Republic. Trop. Med. Infect. Dis. 2025, 10, 198. https://doi.org/10.3390/tropicalmed10070198
Inthavong D, Elsayed H, Keonakhone P, Seevisay V, Souksanh S, Suthepmany S, Chanthavong M, Keodavong X, Kommanivanh P, Siphanthong P, et al. Impact of Nutritional Counselling and Support on Body Mass Index Recovery and Treatment Outcomes Among Tuberculosis Patients in the Lao People’s Democratic Republic. Tropical Medicine and Infectious Disease. 2025; 10(7):198. https://doi.org/10.3390/tropicalmed10070198
Chicago/Turabian StyleInthavong, Donekham, Hend Elsayed, Phonesavanh Keonakhone, Vilath Seevisay, Somdeth Souksanh, Sakhone Suthepmany, Misouk Chanthavong, Xaysomvang Keodavong, Phonesavanh Kommanivanh, Phitsada Siphanthong, and et al. 2025. "Impact of Nutritional Counselling and Support on Body Mass Index Recovery and Treatment Outcomes Among Tuberculosis Patients in the Lao People’s Democratic Republic" Tropical Medicine and Infectious Disease 10, no. 7: 198. https://doi.org/10.3390/tropicalmed10070198
APA StyleInthavong, D., Elsayed, H., Keonakhone, P., Seevisay, V., Souksanh, S., Suthepmany, S., Chanthavong, M., Keodavong, X., Kommanivanh, P., Siphanthong, P., Sengmany, P., Sisounon, B., Sebert, J., Yanagawa, M., Morishita, F., Nishikiori, N., & Yamanaka, T. (2025). Impact of Nutritional Counselling and Support on Body Mass Index Recovery and Treatment Outcomes Among Tuberculosis Patients in the Lao People’s Democratic Republic. Tropical Medicine and Infectious Disease, 10(7), 198. https://doi.org/10.3390/tropicalmed10070198