Current Overview of Environmental Disinfection and Decolonization of C. auris: A Systematic Review from 2020 to 2025

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
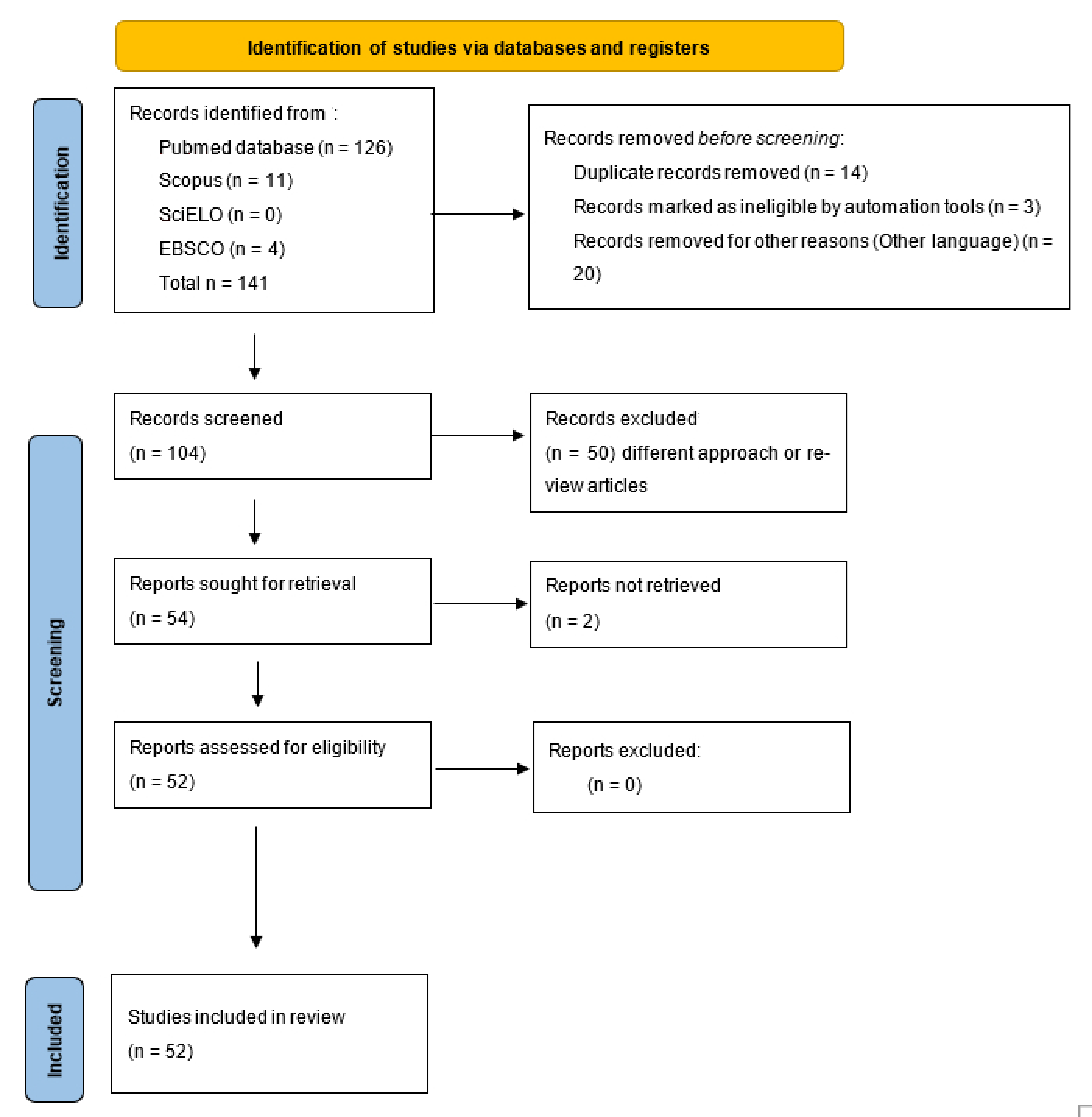
2. Materials and Methods
3. Results
3.1. Disinfection of Environments Contaminated by C. auris
3.2. Decolonization of C. auris
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Denning, D.W. Global incidence and mortality of severe fungal disease. Lancet Infect. Dis. 2024, 24, e428–e438. [Google Scholar] [CrossRef] [PubMed]
- Lass-Flörl, C.; Kanj, S.S.; Govender, N.P.; Thompson, G.R., 3rd; Ostrosky-Zeichner, L.; Govrins, M.A. Invasive candidiasis. Nat. Rev. Dis. Primers 2024, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- De Gaetano, S.; Midiri, A.; Mancuso, G.; Avola, M.G.; Biondo, C. Candida auris Outbreaks: Current status and future perspectives. Microorganisms 2024, 12, 927. [Google Scholar] [CrossRef]
- Fasciana, T.; Cortegiani, A.; Ippolito, M.; Giarratano, A.; Di Quattro, O.; Lipari, D.; Graceffa, D.; Giammanco, A. Candida auris: An overview of how to screen, detect, test and control this emerging pathogen. Antibiotics 2020, 9, 778. [Google Scholar] [CrossRef]
- Lockhart, S.R.; Etienne, K.A.; Vallabhaneni, S.; Farooqi, J.; Chowdhary, A.; Govender, N.P.; Colombo, A.L.; Calvo, B.; Cuomo, C.A.; Desjardins, C.A.; et al. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin. Infect. Dis. 2017, 67, 134–140. [Google Scholar] [CrossRef]
- Jackson, B.R.; Chow, N.; Forsberg, K.; Litvintseva, A.P.; Lockhart, S.R.; Welsh, R.; Vallabhaneni, S.; Chiller, T. On the origins of a species: What might explain the rise of Candida auris? J. Fungi 2019, 5, 58. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Fungal Priority Pathogens List to Guide Research, Development and Public Health Action; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/publications/i/item/9789240060241 (accessed on 26 January 2025).
- Tharp, B.; Zheng, R.; Bryak, G.; Litvintseva, A.P.; Hayden, M.K.; Chowdhary, A.; Thangamani, S. Role of microbiota in the skin colonization of Candida auris. mSphere 2023, 8, e0062322. [Google Scholar] [CrossRef]
- Southwick, K.; Ostrowsky, B.; Greenko, J.; Adams, E.; Lutterloh, E.; NYS C. auris Team; Denis, R.J.; Patel, R.; Erazo, R.; Fernandez, R.; et al. A description of the first Candida auris-colonized individuals in New York State, 2016–2017. Am. J. Infect. Control 2022, 50, 358–360. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, A.; Sood, P. On the emergence, spread and resistance of Candida auris: Host, pathogen and environmental tipping points. J. Med. Microbiol. 2021, 70, 001318. [Google Scholar] [CrossRef]
- Kean, R.; Sherry, L.; Townsend, E.; McKloud, E.; Short, B.; Akinbobola, A.; Mackay, W.G.; Williams, C.; Jones, B.L.; Ramage, G. Surface disinfection challenges for Candida auris: An in-vitro study. J. Hosp. Infect. 2018, 98, 433–436. [Google Scholar] [CrossRef]
- Welsh, R.M.; Bentz, M.L.; Shams, A.; Houston, H.; Lyons, A.; Rose, L.J.; Litvintseva, A.P. Survival, persistence, and isolation of the emerging multidrug-resistant pathogenic yeast Candida auris on a plastic health care surface. J. Clin. Microbiol. 2017, 55, 2996–3005. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, S.; Asadzadeh, M. Strategies to prevent transmission of Candida auris in healthcare settings. Curr. Fungal Infect. Rep. 2023, 17, 36–48. [Google Scholar] [CrossRef]
- Mulet Bayona, J.V.; Tormo Palop, N.; Salvador García, C.; Herrero Rodríguez, P.; Abril López de Medrano, V.; Ferrer Gómez, C.; Gimeno Cardona, C. Characteristics and management of candidaemia episodes in an established Candida auris outbreak. Antibiotics 2020, 9, 558. [Google Scholar] [CrossRef]
- Sabino, R.; Veríssimo, C.; Pereira, Á.A.; Antunes, F. Candida auris, an agent of hospital-associated outbreaks: Which challenging issues do we need to have in mind? Microorganisms 2020, 8, 181. [Google Scholar] [CrossRef]
- Bergeron, G.; Bloch, D.; Murray, K.; Kratz, M.; Parton, H.; Ackelsberg, J.; Antwi, M.; Del Rosso, P.; Dorsinville, M.; Kubinson, H.; et al. Candida auris Colonization after discharge to a community setting: New York City, 2017–2019. Open Forum Infect. Dis. 2020, 8, ofaa620. [Google Scholar] [CrossRef] [PubMed]
- Salvador-García, P.; Palop, N.T.; Bayona, J.V.M.; García, M.M.; Rodríguez, D.N.; Álvarez, M.B.; Serrano, M.D.R.G.; Cardona, C.G. Candida auris: Report of an outbreak. Enferm. Infecc. Microbiol. Clin. 2020, 38, 39–44. [Google Scholar] [CrossRef]
- Geremia, N.; Brugnaro, P.; Solinas, M.; Scarparo, C.; Panese, S. Candida auris as an emergent public health problem: A current update on European outbreaks and cases. Healthcare 2023, 11, 425. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.; Choi, H.; Ochoa, B.; Garmon, G.; Coppin, J.D.; Allton, Y.; Lukey, J.; Williams, M.D.; Navarathna, D.; Jinadatha, C. Clade-specific variation in susceptibility of Candida auris to broad-spectrum ultraviolet C light (UV-C). Infect. Control Hosp. Epidemiol. 2020, 41, 1384–1387. [Google Scholar] [CrossRef]
- Fu, L.; Le, T.; Liu, Z.; Wang, L.; Guo, H.; Yang, J.; Chen, Q.; Hu, J. Different efficacies of common disinfection methods against Candida auris and other Candida species. J. Infect. Public Health 2020, 13, 730–736. [Google Scholar] [CrossRef]
- Kumar, J.A.; Cadnum, J.L.; Jencson, A.L.; Donskey, C.J. Efficacy of a multi-purpose high level disinfection cabinet against Candida auris and other health care-associated pathogen. Am. J. Infect. Control 2020, 48, 849–850. [Google Scholar] [CrossRef]
- Kumar, J.A.; Cadnum, J.L.; Jencson, A.L.; Donskey, C.J. Are reduced concentrations of chlorine-based disinfectants effective against Candida auris? Am. J. Infect. Control 2020, 48, 448–450. [Google Scholar] [CrossRef] [PubMed]
- Lara, H.H.; Ixtepan-Turrent, L.; Jose Yacaman, M.; Lopez-Ribot, J. Inhibition of Candida auris biofilm formation on medical and environmental surfaces by silver nanoparticles. ACS Appl. Mater. Interfaces 2020, 12, 21183–21191. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Tan, C.K.; Ißleib, U.; Paßvogel, L.; Eilts, B.; Steinhauer, K. Investigation of the susceptibility of Candida auris and Candida albicans to chemical disinfectants using European Standards EN 13624 and EN 16615. J. Hosp. Infect. 2020, 105, 648–656. [Google Scholar] [CrossRef] [PubMed]
- Sexton, D.J.; Welsh, R.M.; Bentz, M.L.; Forsberg, K.; Jackson, B.; Berkow, E.L.; Litvintseva, A.P. Evaluation of nine surface disinfectants against Candida auris using a quantitative disk carrier method: EPA SOP-MB-35. Infect. Control Hosp. Epidemiol. 2020, 41, 1219–1221. [Google Scholar] [CrossRef]
- De Alteriis, E.; Maione, A.; Falanga, A.; Bellavita, R.; Galdiero, S.; Albarano, L.; Salvatore, M.M.; Galdiero, E.; Guida, M. Activity of free and liposome-encapsulated essential oil from Lavandula angustifolia against persister-derived biofilm of Candida auris. Antibiotics 2021, 11, 26. [Google Scholar] [CrossRef]
- Cadnum, J.L.; Pearlmutter, B.S.; Haq, M.F.; Jencson, A.L.; Donskey, C.J. Effectiveness and real-world materials compatibility of a novel hydrogen peroxide disinfectant cleaner. Am. J. Infect. Control 2021, 49, 1572–1574. [Google Scholar] [CrossRef]
- Eckbo, E.J.; Wong, T.; Bharat, A.; Cameron-Lane, M.; Hoang, L.; Dawar, M.; Charles, M. First reported outbreak of the emerging pathogen Candida auris in Canada. Am. J. Infect. Control 2021, 49, 804–807. [Google Scholar] [CrossRef]
- Füszl, A.; Zatorska, B.; Van den Nest, M.; Ebner, J.; Presterl, E.; Diab-Elschahawi, M. The use of a UV-C disinfection robot in the routine cleaning process: A field study in an Academic hospital. Antimicrob. Resist. Infect. Control 2021, 10, 84. [Google Scholar] [CrossRef]
- Truong, L.N.; Whitlock, B.D. Efficacy of compressed sodium chloride (CSC) against E. coli and Candida auris in minutes and methods improvement for testing. Sci. Rep. 2021, 11, 149. [Google Scholar] [CrossRef]
- Zatorska, B.; Moser, D.; Diab-Elschahawi, M.; Ebner, J.; Lusignani, L.S.; Presterl, E. The effectiveness of surface disinfectants and a micellic H2O2 based water disinfectant on Candida auris. J. Mycol. Med. 2021, 31, 101178. [Google Scholar] [CrossRef] [PubMed]
- Changaris, D.G.; Carenbauer, A.L. Potassium linoleate (isomerized) satisfies the united states environmental protection agency MB-05-16 for hospital disinfectant on hard, non-porous surfaces. Cureus 2022, 14, e22851. [Google Scholar] [CrossRef] [PubMed]
- Corcione, S.; Montrucchio, G.; Shbaklo, N.; De Benedetto, I.; Sales, G.; Cedrone, M.; Vita, D.; Costa, C.; Zozzoli, S.; Zaccaria, T.; et al. First Cases of Candida auris in a referral intensive care unit in Piedmont Region, Italy. Microorganisms 2022, 10, 1521. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.; Schnugh, D.; Thomas, T. Effectiveness of ultraviolet-C vs aerosolized hydrogen peroxide in ICU terminal disinfection. J. Hosp. Infect. 2022, 121, 114–119. [Google Scholar] [CrossRef]
- Mariita, R.M.; Davis, J.H.; Lottridge, M.M.; Randive, R.V. Shining light on multi-drug resistant Candida auris: Ultraviolet-C disinfection, wavelength sensitivity, and prevention of biofilm formation of an emerging yeast pathogen. Microbiologyopen 2022, 11, e1261. [Google Scholar] [CrossRef]
- Dire, O.; Ahmad, A.; Duze, S.; Patel, M. Survival of Candida auris on environmental surface materials and low-level resistance to disinfectant. J. Hosp. Infect. 2023, 137, 17–23. [Google Scholar] [CrossRef]
- Haq, M.F.; Cadnum, J.L.; Pearlmutter, B.S.; Jencson, A.L.; Donskey, C.J. Effectiveness of a novel 1-step cleaner and disinfectant against Candida auris. Infect. Control Hosp. Epidemiol. 2023, 44, 837–839. [Google Scholar] [CrossRef]
- Haq, M.F.; Pearlmutter, B.S.; Cadnum, J.L.; Donskey, C.J. Efficacy of 23 commonly used liquid disinfectants against Candida auris isolates from the 4 major clades. Infect. Control Hosp. Epidemiol. 2024, 45, 127–131. [Google Scholar] [CrossRef]
- McDougal, A.N.; DeMaet, M.A.; Garcia, B.; York, T.; Iverson, T.; Ojo, O.; Patel, J. A cluster investigation of Candida auris among hospitalized incarcerated patients. Antimicrob. Steward. Healthc. Epidemiol. 2023, 3, e244. [Google Scholar] [CrossRef]
- Różańska, A.; Walkowicz, M.; Bulanda, M.; Kasperski, T.; Synowiec, E.; Osuch, P.; Chmielarczyk, A. Evaluation of the efficacy of UV-C radiation in eliminating microorganisms of special epidemiological importance from touch surfaces under laboratory conditions and in the hospital environment. Healthcare 2023, 11, 3096. [Google Scholar] [CrossRef]
- Solomon, S.; Stachel, A.; Kelly, A.; Mraz, J.; Aguilar, P.; Gardner, J.; Medefindt, J.; Horrocks, A.; Sterling, S.; Aguero-Rosenfeld, M.; et al. The evaluation of electrolyzed water, sodium dichloroisocyanurate, and peracetic acid with hydrogen peroxide for the disinfection of patient room surfaces. Am. J. Infect. Control 2023, 51, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Voorn, M.G.; Kelley, A.M.; Chaggar, G.K.; Li, X.; Teska, P.J.; Oliver, H.F. Contact time and disinfectant formulation significantly impact the efficacies of disinfectant towelettes against Candida auris on hard, non-porous surfaces. Sci. Rep. 2023, 13, 5849. [Google Scholar] [CrossRef] [PubMed]
- Wells, K.M.; Ciftci, Y.; Peddinti, B.S.T.; Ghiladi, R.A.; Vediyappan, G.; Spontak, R.J.; Govind, R. Preventing the spread of life-threatening gastrointestinal microbes on the surface of a continuously self-disinfecting block polymer. J. Colloid Interface Sci. 2023, 652, 718–726. [Google Scholar] [CrossRef]
- Cox, C.A.; Manavathu, E.K.; Wakade, S.; Myntti, M.; Vazquez, J.A. Efficacy of biofilm disrupters against Candida auris and other Candida species in monomicrobial and polymicrobial biofilms. Mycoses 2024, 67, e13684. [Google Scholar] [CrossRef] [PubMed]
- Erganis, S.; Ozturk, A.; Uzuntas, S.T.; Kirca, F.; Dogan, A.; Dinc, B.; Kalkanci, A. Variable sensitivity of clinical Candida auris strains to biocides: Implications for infection control in healthcare settings. BMC Microbiol. 2024, 24, 447. [Google Scholar] [CrossRef]
- Gierke, A.M.; Hessling, M. Photoinactivation by UVA radiation and visible light of Candida auris compared to other fungi. Photochem. Photobiol. Sci. 2024, 23, 681–692. [Google Scholar] [CrossRef]
- Gupta, N.; Haughton, S.; Kemper, S.; Koehler, M.; Antoon, R.; Edwards, C.G.; Bardin, A. The antimicrobial effectiveness of chlorhexidine and chlorhexidine-silver sulfadiazine-impregnated central venous catheters against the emerging fungal pathogen Candida auris. Am. J. Infect. Control 2024, 52, 1283–1288. [Google Scholar] [CrossRef] [PubMed]
- Kaple, C.E.; Memic, S.; Cadnum, J.L.; Donskey, C.J. Evaluation of an automated far ultraviolet-C light technology for decontamination of surfaces and aerosolized viruses in bathrooms. Antimicrob. Resist. Infect. Control 2024, 13, 114. [Google Scholar] [CrossRef]
- Koutras, C.; Wade, R.L. Ultraviolet-C mediated inactivation of Candida auris, a rapid emerging health threat. Am. J. Infect. Control 2024, 52, 133–135. [Google Scholar] [CrossRef]
- Lee, E.H.; Choi, M.H.; Lee, K.H.; Kim, D.; Jeong, S.H.; Song, Y.G.; Han, S.H. Intrahospital transmission and infection control of Candida auris originating from a severely infected COVID-19 patient transferred abroad. J. Hosp. Infect. 2024, 143, 140–149. [Google Scholar] [CrossRef]
- Lemons, A.R.; McClelland, T.L.; Martin, S.B., Jr.; Lindsley, W.G.; Green, B.J. Inactivation of the multi-drug resistant pathogen Candida auris using ultraviolet germicidal irradiation (UVGI). J. Hosp. Infect. 2020, 105, 495–501. [Google Scholar] [CrossRef]
- Loftus, R.W.; Brindeiro, C.T.; Dexter, F.; Parra, M.C.; Hwang, S.M.; Wanta, B.; Szeluga, D.J.; Hadder, B.A.; Seering, M.S.; Charnin, J.E. Importance of Ultraviolet-C (UV-C) emitter configuration for the attenuation of Staphylococcus aureus and Candida auris pathogens. Cureus 2024, 16, e71612. [Google Scholar] [CrossRef] [PubMed]
- Memic, S.; Osborne, A.O.; Cadnum, J.L.; Donskey, C.J. Efficacy of a far-ultraviolet-C light technology for continuous decontamination of air and surfaces. Infect. Control Hosp. Epidemiol. 2024, 45, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Retore, Y.I.; Lucini, F.; Pimentel, L.R.; de Oliveira, H.C.; Simionatto, S.; Rossato, L. Screening of the global health priority BoxⓇ reveals potential new disinfectants against the emerging multidrug-resistant pathogen Candida auris. Microb. Pathog. 2024, 194, 106828. [Google Scholar] [CrossRef] [PubMed]
- Rutala, W.A.; Bolomey, A.C.; Cadnum, J.L.; Donskey, C.J. Inactivation and/or physical removal of Candida auris from floors by detergent cleaner, disinfectants, microfiber, and ultraviolet C light (UV-C). Infect. Control Hosp. Epidemiol. 2024, 45, 390–392. [Google Scholar] [CrossRef]
- Krishnan, S.; Venkatachalam, P.; Shanmugam, S.R.; Paramasivam, N. Fractional inhibitory concentration of bio-actives from agricultural waste disassembles biofilms and quenches virulence of nosocomial pathogens. J. Med. Microbiol. 2025, 74, 001980. [Google Scholar] [CrossRef]
- Memic, S.; Torres-Teran, M.M.; Cadnum, J.L.; Donskey, C.J. Evaluation of a far ultraviolet-C device for decontamination of portable equipment in clinical areas. Am. J. Infect. Control 2025, 53, 403–406. [Google Scholar] [CrossRef]
- Sathyapalan, D.T.; Antony, R.; Nampoothiri, V.; Kumar, A.; Shashindran, N.; James, J.; Thomas, J.; Prasanna, P.; Sudhir, A.S.; Philip, J.M.; et al. Evaluating the measures taken to contain a Candida auris outbreak in a tertiary care hospital in South India: An outbreak investigational study. BMC Infect. Dis. 2021, 21, 425. [Google Scholar] [CrossRef]
- Gierke, A.M.; Hessling, M. Sensitivity analysis of C. auris, S. cerevisiae, and C. cladosporioides by irradiation with Far-UVC, UVC, and UVB. Pathog. Immun. 2024, 9, 135–151. [Google Scholar] [CrossRef]
- Stoffel, J.J.; Kohler Riedi, P.L.; Hadj Romdhane, B. A multimodel regime for evaluating effectiveness of antimicrobial wound care products in microbial biofilms. Wound Repair Regen. 2020, 28, 438–447. [Google Scholar] [CrossRef]
- Huang, X.; Hurabielle, C.; Drummond, R.A.; Bouladoux, N.; Desai, J.V.; Sim, C.K.; Belkaid, Y.; Lionakis, M.S.; Segre, J.A. Murine model of colonization with fungal pathogen Candida auris to explore skin tropism, host risk factors and therapeutic strategies. Cell Host Microbe 2021, 29, 210–221.e6. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.J.; Eix, E.F.; Lam, B.C.; Wartman, K.M.; Meudt, J.J.; Shanmuganayagam, D.; Nett, J.E. Augmenting the activity of chlorhexidine for decolonization of Candida auris from porcine skin. J. Fungi 2021, 7, 804. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Fang, R.; Feng, R.; Li, Q.; Su, M.; Hou, C.; Zhuang, K.; Dai, Y.; Lei, N.; Jiang, Y.; et al. Cage-modified hypocrellin against multidrug-resistant Candida spp. with unprecedented activity in light-triggered combinational photodynamic therapy. Drug Resist. Updat. 2022, 65, 100887. [Google Scholar] [CrossRef]
- Elshaer, M.; Herrada, J.; Gamal, A.; McCormick, T.S.; Ghannoum, M. Efficacy of chlorhexidine in advanced performance technology formulation in decolonizing the skin using Candida auris skin colonization mouse model. Am. J. Infect. Control 2023, 51, 836–837. [Google Scholar] [CrossRef]
- Elbahr, U.; Khairy, A.; Dayyab, F.; Delos Reyes, C.S.; Pastrana, J.; Vineeth, C.; Hejres, S.; Sudha, S.P.; Keskin, O.; Rana, S.S.; et al. Can daily bathing with 4% chlorhexidine + daily chlorhexidine wipe for 1 week be effective in decolonizing Candida auris colonization? Eur. J. Clin. Microbiol. Infect. Dis. 2024, 43, 243–247. [Google Scholar] [CrossRef]
- Gugsch, F.; Tan, C.K.; Oh, D.Y.; Paßvogel, L.; Steinhauer, K. Efficacy of octenidine- and chlorhexidine-based wash-mitts against Candida albicans and Candida auris—A comparative study. J. Hosp. Infect. 2024, 143, 91–96. [Google Scholar] [CrossRef]
- Rosa, R.; Abbo, L.M.; Jimenez, A.; Carter, C.; Ruiz, M.; Gerald, W.; Jimenez Hamann, M. Effectiveness of a sodium hypochlorite isotonic solution in decolonization of patients with Candida auris: Learnings from a county health care system. Am. J. Infect. Control 2024, 52, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Gerges, B.Z.; Rosenblatt, J.; Truong, Y.L.; Jiang, Y.; Raad, I.I. The antifungal activity of a polygalacturonic and caprylic acid ointment in an in vitro, three-dimensional wound biofilm model. J. Fungi 2025, 11, 178. [Google Scholar] [CrossRef] [PubMed]
- Gavilanes-Martínez, M.A.; Coral-Garzón, A.; Cáceres, D.H.; García, A.M. Antifungal activity of boric acid, triclosan and zinc oxide against different clinically relevant Candida species. Mycoses 2021, 64, 1045–1052. [Google Scholar] [CrossRef]
- Wu, W.G.; Luk, K.S.; Hung, M.F.; Tsang, W.Y.; Lee, K.P.; Lam, B.H.; Cheng, K.L.; Cheung, W.S.; Tang, H.L.; To, W.K. Antifungal efficacy of natural antiseptic products against Candida auris. Med. Mycol. 2024, 62, myae060. [Google Scholar] [CrossRef]
- Ku, T.S.N.; Walraven, C.J.; Lee, S.A. Candida auris: Disinfectants and implications for infection control. Front. Microbiol. 2018, 9, 726. [Google Scholar] [CrossRef] [PubMed]
- Schelenz, S.; Hagen, F.; Rhodes, J.L.; Abdolrasouli, A.; Chowdhary, A.; Hall, A.; Ryan, L.; Shackleton, J.; Trimlett, R.; Meis, J.F.; et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob. Resist. Infect. Control 2016, 5, 35. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Agent | Concentration or Wavelength | Exposure Time | Logarithmic Reduction | Strain/Clade | Country | Reference |
|---|---|---|---|---|---|---|
| UV-C on steel surfaces | 200–280 nm | 30 min at 1.5 m distance | 0.52 log10 1.38 log10 0.04 log10 1.15 log10 | I II III IV | USA | [20] |
| UV-C and ozone on bed sheets | UV-C 253.7 nm Ozone 300 mg/m3 | 60 min, at 2.5 m distance 20 min, two cycles | 3.22 log10 3.260 log10 | III | China | [21] |
| C2H4O3 and H2O2 on portable medical equipment surfaces | 22% H2O2 and 4.5% C2H4O3 | A 21-min cycle | C. auris was eradicated | I | USA | [22] |
| Two chlorine-based disinfectants | 500, 1000, 2000, 4000 and 6500 ppm | 1 min of wet contact | >3 log10 to ≥4000 ppm | I | USA | [23] |
| AgNP (1 to 3 nm in diameter) in silicone elastomer and bandage fibers | 2.3 to 0.017 ppm | 24 h | 5.7 log10 | I | USA | [24] |
| Two surface disinfectants, an alcohol-based disinfectant and a QAC-based disinfectant | Alcohol 35% QAC 0.25% | 0.5 min contact 1 min contact | NR | DSM-21092 | Germany | [25] |
| Five H2O2 or alcohol-based disinfectants and four QAC-based disinfectants | H2O2 0.5 and 1.4% QAC 0.084, 0.5, 0.61, 2, 10.9 y 21.7% | H2O2 1, 3 and 10 min QAC 1, 2 and 10 min | ≥5.32 log10 0.25 to ≥5.29 log10 | IV | USA | [26] |
| Lavandula angustifolia essential oil, in free form or encapsulated in liposomes | 0.005–0.5% v/v | 24 and 48 h | C. auris was eradicated | DSM 21092 | Italy | [27] |
| H2O2-based disinfectant, and NaClO-based disinfectant | >0.1–4% H2O2 0.65% NaClO | 1 min 1 min | ≥5.1 log10 ≥6.1 log10 | II (AR-0381) and IV (AR-0385) | USA | [28] |
| Accelerated H2O2 for environmental disinfection twice a day | NR | Twice a day | NR | I | Canada | [29] |
| Robotic UV-C | 254 nm, 2.7 mJ/cm2 per second | 20–25 min at 1 m distance | >1.7 log10 | NCPF 8971, NCPF 8977, NCPF 8984 and DSM 21092 | Austria | [30] |
| CSC | 97.5–100% sodium chloride compressed into blocks | 1 min | 2.15 log10 | UAMH 12148 | Canada | [31] |
| ETH QAC ALD PP H2O2 mH2O2 | 100% 100% 0.5% 3% 3.4% 4.2% 5% 10% | 1 min 1 min 0.5% 30 min 5 min 5 min 15 min 15 min | >5 log10 >5 log10 >5 log10 >7 log10 >2 log10 >3 log10 No activity >2 log10 | NCPF8971, NCPF8977, NCPF8984, DSM21092 | Austria | [32] |
| C18H31KO2 (isomerized) | 86 mM | 48 h | NR | NR | USA | [33] |
| Chlorine solution. and a H2O2 nebulization | ≥1000 ppm on high-contact surfaces 5000 ppm at patient discharge | NR | NR | I | Italy | [34] |
| UV-C aHP | 254 nm, 900 mW/cm2 at 1 m and 450 mW/cm2 at 2 m 6% stabilized with silver | 20 min 1 h | C. auris was eradicated | III | South Africa | [35] |
| UV-C on stainless steel, plastic/polystyrene, and polycotton fabric surfaces | 252–280 nm, 5, 10, 20 and 40 mJ cm−2 | 5 s 10 s 20 s 40 s | 2.9 log10 | II | USA | [36] |
| Sodium dichloroisocyanurate (NADCC)Ethanol Benzalkonium chloride (BC) H2O2 on different surfaces | 1000 ppm 70% 95% NR | 24 h | C. auris was eradicated 4.36 log10 C. auris was eradicated 5.4 log10 | Cau 4888, Cau 3499 and Cau 6326 | South Africa | [37] |
| One-step anionic surfactant disinfectant (active ingredient C18H30O3S) | 0.29% | 1 min | 5.64 log10 (clade I) 5.2 log10 (clade II) 4.97 log10 (clade III) 4.78 log10 (clade IV) | I (AR-0389) II (AR-0381) III (AR-0383) IV (AR-0385) | USA | [38] |
| 23 liquid disinfectants | QAC-Alcohol 0.25% H2O2 0.5% | NR | NR | I, II, III and IV | USA | [39] |
| Quaternary ammonium and isopropyl alcohol-based germicidal wipe (Sani-Cloth®, PDI Healthcare, Woodcliff Lake, NJ, USA) on medical equipment surfaces, and 0.65% sodium hypochlorite on high-contact surfaces | sodium hypochlorite 0.65% | NR | NR | III | USA | [40] |
| UV-C on contact surfaces (steel, plastic, and glass supports/holders) in laboratory and hospital environments | 254 nm | 10 min | 2.93 log10 | I | Poland | [41] |
| EW, NaDCC, and PAA/H2O2 applied by electrostatic sprayers | NR >4000 ppm 2000 ppm/0.5% | 1 min | 1.57 log10 1.15 log10 1.26 log10 | I | USA | [42] |
| H2O2 QAC-isopropyl alcohol based disinfectant wipes (EPA approved) | 0.5% 0.25–55% | 1, 2, 3 and 10 min | >6 log10 | MYA-5001 | USA | [43] |
| Solid surface of a self-disinfecting anionic block polymer that inherently generates a surface layer of acidic water when hydrated (pH < 1) | 52 mol% midblock sulfonation | At contact, after hydration | NR | I | USA | [44] |
| CHD and BD (BlastX, Torrent, NSSD) on surfaces | NR | NR | NR | I | USA | [45] |
| Chlorine chlorhexidine benzalkonium chloride | 200 ppm 500 ppm 2 and 4% NR | 1, 5 and 30 min | >3 log10 (clade I) with 500 ppm >3 log10 with 4%Resistance | I and IV | Turkey | [46] |
| Photoinactivation with UV-A | 365, 400, and 450 nm | NR | 1 log10 | I | Germany | [45] |
| Far UV-C UV-C short-wave UV-B on yeast solutions | 222 nm 254 nm 302 nm | 4.3 mJ/cm2 6.1 mJ/cm2 51.3 mJ/cm2 | 1 log10 | II | Germany | [47] |
| CHD and CHD-S impregnated in segments of central venous catheters | 0.03 to 512 μg/mL | 24 h | NR | II, IV | USA | [48] |
| Far UV-C on bathroom surfaces | 222 nm | 2 h, 11.7 µW/cm2 in direct line and 0.4 µW/cm2 in non-direct line | ≥1.2 log10 | AR0385 (Clade IV) | USA | [49] |
| UV-C on hard surfaces | 254 nm | 250 mJ/cm2 for 7 min at 2.4 m distance | ≥3.86 log10 | AR0385 (IV) | USA | [50] |
| Ten-fold diluted NaClO in medical devices | 10% | NR (intensive) | C. auris was eradicated | II | Korea | [51] |
| UVGI to inactivate C. auris strains in aqueous solution | 254 nm | 10, 20, 30, 40, 50, 60, 70, 80, 90, 100 and 150 mJ/cm2 at a 27.9 cm distance | 5 log10 at a dose of 66 to 110 mJ/cm2 | I, II, III and IV | USA | [52] |
| UV-C | 254 nm | 596.62 ± 27.98 mJ/cm2, 2.74 m | >6 log10 | ATCC MYA-5001 | USA | [53] |
| Far UV-C installed on the wall. | 254 nm | 45 min at a 2 and 3 m distance | <3 log10 | I | USA | [54] |
| 240 compounds from the Global Health Priority Box® | Hydramethylnon (MMV1577471) 16 μg/mL Flufenerim (MMV1794206) 4 μg/mL | NR | NR | IV | Brazil | [55] |
| Detergent, microfiber mop UV-C Disinfectant with non-sporicidal activity based on QAC Disinfectant with sporicidal activity based on NaClO | UV-C 252 nm QAC NaClO 0.25% | NR | NR | I | USA | [56] |
| C5H6O2, C6H8O and C7H8O2 on stainless steel | 8% v/v 9% v/v 2% v/v | 24 h 24 h 24 h | 6.3 log10 | I | India | [57] |
| Far UV-C on the surface of portable equipment in clinical areas | 222 nm | 4 and 12 h | >2 log10 after 4 h >3 log10 after 12 h | I | USA | [58] |
| Sodium hypochlorite | 0.5 at 1% | Three times a day and after patient’s discharge | NR | I | India | [59] |
| Decolonization Agent | Concentration | Exposure Time | Logarithmic Reduction | Strain/Clade | Country | Reference |
|---|---|---|---|---|---|---|
| Disinfectant 84 comprises chlorine iodine tincture QAC 75% ethanol benzalkonium bromide | 1000 mg/L 2% (w/v) 2000 ppm 75% (v/v) 1000 mg/L | 1 min 1 min 10 min 15 s 10 min | 3 log10 NR Resistance 3 log10 NR | CBS12766, INCa-1, INCa-2 | China | [21] |
| Iodine, silver, polyhexamethylene biguanide, octenidine, hypochlorous acid, benzalkonium chloride, surfactant-based topical containing poloxamer 188 | NR | 24 h | >6 log10 >6 log10 >6 log10 Resistance <1 log10 >6 log10 1 log10 | B11903 | USA | [61] |
| CHX | 2% | 1 s | Complete eradication of skin colonization | I, II, III, IV, NIH, MYA-2876 | USA | [62] |
| CHX Isopropanol tea tree oil (Melaleuca alternifolia) lemongrass oil (Cymbopogon flexuosus) | 2% 70% 10% 5% | 1 h daily for 3 days | 0.5 log10 1 log10 1.5 log10 NR | I | USA | [63] |
| HA (isolated from Shiraia bambusicola and Hypocrella bambusae) bound to a novel organic compound (COP1T) with PEG chains | 0.78 µg/mL 1.56 µg/mL 3.125 µg/mL | 30 °C under a 470 nm laser (MDL-III-470 nm, 100 mW/cm2) for 30 min | 4.2 log10 4.1 log10 2.7 log10 | BJCA001 | China | [64] |
| CHG in Advanced Penetration Technology (APT™) formulation | CHG 3.39% with APT | twice daily for 7 days | NR | I | USA | [65] |
| CHX | 4% | daily bath for 1 week | NR | I | Bahrain | [66] |
| Wash mitts impregnated with CHG or OCT-based antiseptic | 97% ≥10% | 30 s | 3 log10 ≥4 log10 | DSM 21092, DSM 105986 | Germany | [67] |
| Sodium hypochlorite isotonic solution | 0.1% | daily bath | NR | I | USA | [65] |
| Synthetic (CHX, povidone iodine, and nystatin) natural (tea tree and manuka oil) antiseptics | NR <1.25% (v/v) | daily bath, contact with wounds | NR | III | China | [68] |
| PG and CAP Ointment | 1 and 0.8% | 3 h | 5 log10 | 0391 | USA | [69] |
| Triclosan Boric acid Zinc oxide | 0.2 and 0.3% 1.9 and 5.0% 8.6 and 25% | 48 h | NR | IV | Colombia | [70] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frías-De-León, M.G.; Betancourt-Cisneros, P.; Martínez-Herrera, E.; Zarate-Segura, P.B.; Castro-Fuentes, C.A.; García-Salazar, E. Current Overview of Environmental Disinfection and Decolonization of C. auris: A Systematic Review from 2020 to 2025. Trop. Med. Infect. Dis. 2025, 10, 155. https://doi.org/10.3390/tropicalmed10060155
Frías-De-León MG, Betancourt-Cisneros P, Martínez-Herrera E, Zarate-Segura PB, Castro-Fuentes CA, García-Salazar E. Current Overview of Environmental Disinfection and Decolonization of C. auris: A Systematic Review from 2020 to 2025. Tropical Medicine and Infectious Disease. 2025; 10(6):155. https://doi.org/10.3390/tropicalmed10060155
Chicago/Turabian StyleFrías-De-León, María Guadalupe, Paola Betancourt-Cisneros, Erick Martínez-Herrera, Paola Berenice Zarate-Segura, Carlos Alberto Castro-Fuentes, and Eduardo García-Salazar. 2025. "Current Overview of Environmental Disinfection and Decolonization of C. auris: A Systematic Review from 2020 to 2025" Tropical Medicine and Infectious Disease 10, no. 6: 155. https://doi.org/10.3390/tropicalmed10060155
APA StyleFrías-De-León, M. G., Betancourt-Cisneros, P., Martínez-Herrera, E., Zarate-Segura, P. B., Castro-Fuentes, C. A., & García-Salazar, E. (2025). Current Overview of Environmental Disinfection and Decolonization of C. auris: A Systematic Review from 2020 to 2025. Tropical Medicine and Infectious Disease, 10(6), 155. https://doi.org/10.3390/tropicalmed10060155