
Prognostic Value of the Brixia Radiological Score in COVID-19 Patients: A Retrospective Study from Romania

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic and Behavioral Data
3.2. Clinical and Biological Characteristics of Hospitalized COVID-19 Patients
3.3. Radiological Characteristics of Hospitalized COVID-19 Patients
3.4. Disease Progression and Complications
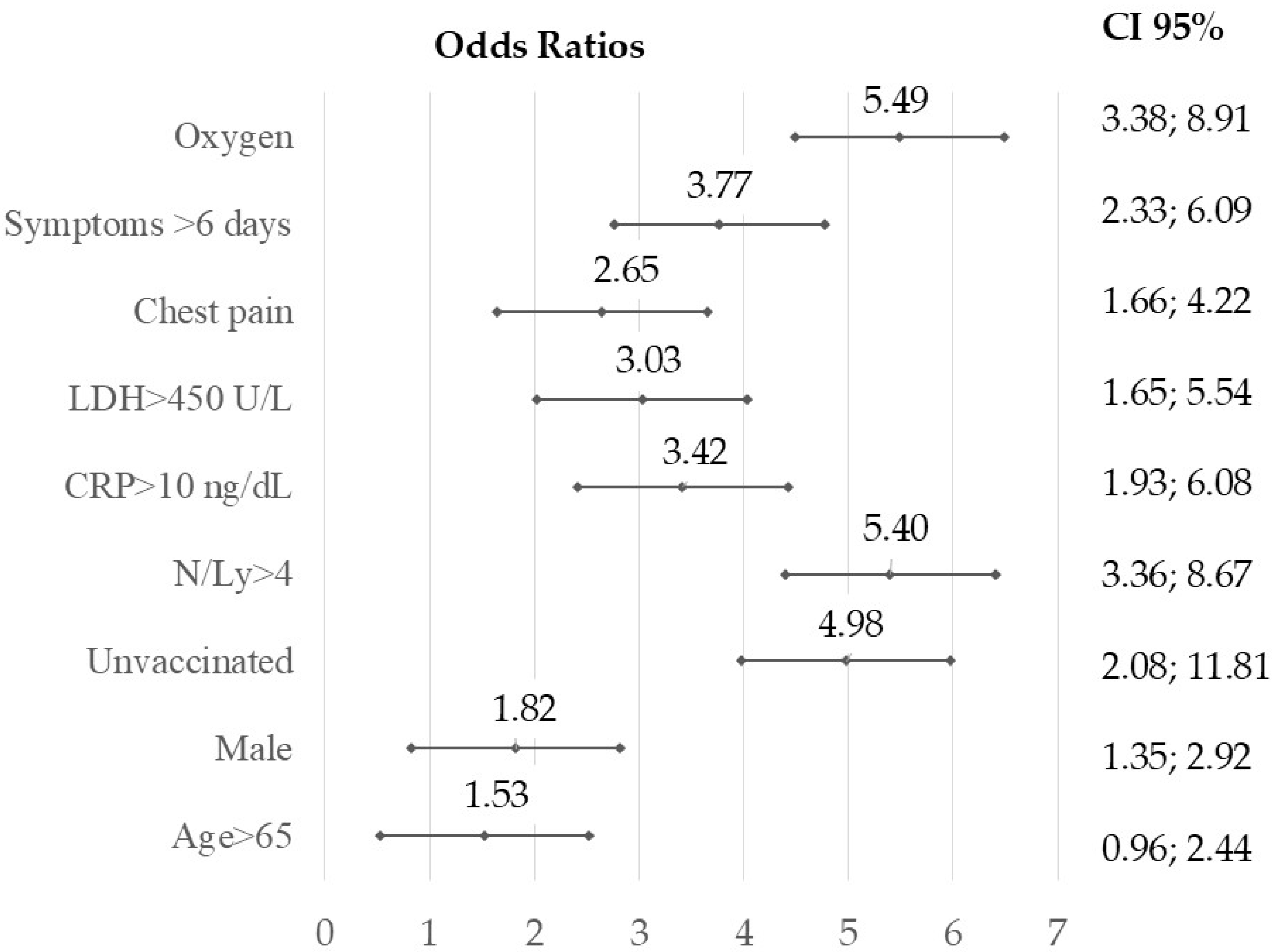
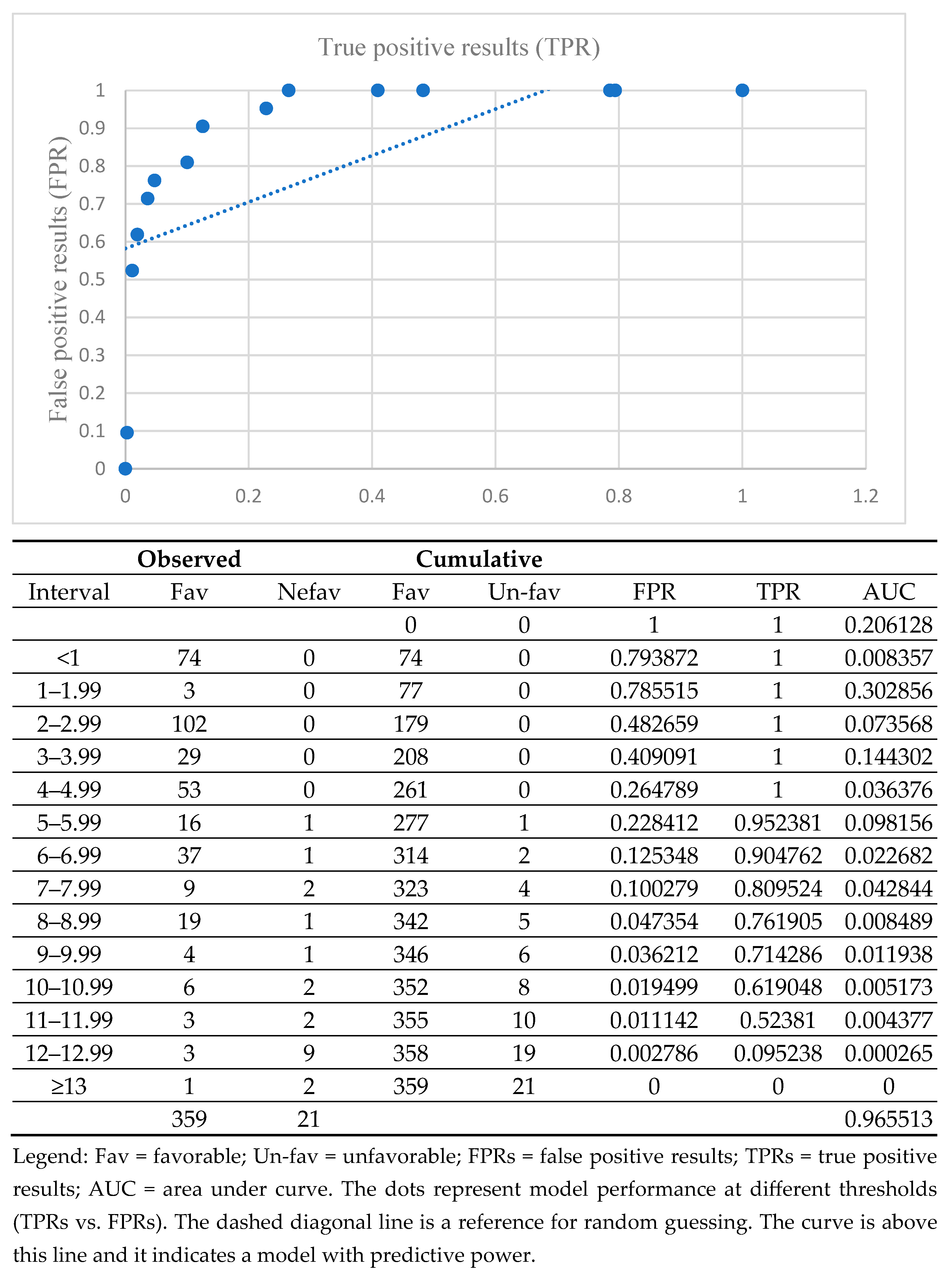
3.5. Correlations Between Favorable and Unfavorable Outcomes
4. Discussion
4.1. Behavioral and Clinical Characteristics of COVID-19 Within the Study Population
4.2. The Role of the Brixia Score in Predicting COVID-19 Severity
4.3. Artificial Intelligence and Brixia Score: Current Insights and Future Directions
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALT | Alanine transaminase |
| AST | Aspartate aminotransferase |
| AUC | Area under the curve |
| CI | Confidence interval |
| COVID-19 | Coronavirus disease 2019 |
| CT | Computed tomography |
| CCD | Chronic cardiac disease |
| COPD | Chronic obstructive pulmonary disease |
| CRP | C-reactive protein |
| ERS | Erythrocyte sedimentation rate |
| FPRs | False positive results |
| LDH | Serum lactate dehydrogenase |
| qSOFA | Quick Sequential Organ Failure Assessment |
| MREMS | Modified Rapid Emergency Medicine Score |
| NLR | Neutrophil-to-lymphocyte ratio |
| OR | Odds ratio |
| RPAS | Rapid Acute Physiology Score |
| RT-PCR | Real-Time Polymerase Chain Reaction |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SD | Standard deviation |
| TPRS | True positive results |
Appendix A

{kind=link}
{kind=link}
{kind=link}
| N = 380 | n | % | p | |
|---|---|---|---|---|
| Gender | Female | 160 | 42.11% | 0.002 |
| Male | 220 | 57.89% | ||
| Living area | Urban | 282 | 74.21% | <0.001 |
| Rural | 98 | 25.79% | ||
| Formal education | Uneducated | 9 | 2.36% | <0.001 |
| 4 years | 19 | 5% | ||
| 8 years | 87 | 22.89% | ||
| High school | 118 | 31.05% | ||
| Vocational school | 92 | 24.21% | ||
| University degree | 55 | 14.47% | ||
| Smoking | Yes | 133 | 35% | p < 0.001 |
| No | 247 | 65% | ||
| Alchool | Yes | 95 | 25% | p < 0.001 |
| No | 285 | 75% | ||
| SARS-CoV-2 vaccine ≥ 1 doze | Yes | 61 | 16% | p < 0.001 |
| No | 319 | 84% | ||
| N = 380 | Normal Values | Average ± SD | Median | Minim | Maxim | % Abnormal Values |
|---|---|---|---|---|---|---|
| Leucocyte | 4000–10,000 μL | 10764 ± 5242.83 | 9800 | 3500 | 53,200 | 30.5% |
| NLR | 1–2 | 4.70 ± 4.52 | 0.73 | 0.73 | 44.91 | 56.57% |
| CRP | 0–1 ng/dL | 8.44 ± 18.14 | 4.6 | 0.5 | 307 | 94.21% |
| ESR | 2–22 mm/30 min | 52.20 ± 29.69 | 45 | 5 | 140 | 90.78% |
| Fibrinogen | 200–400 mg/dL | 665.07± | 643 | 260 | 1224 | 96.70% |
| LDH | 135–225 U/L | 291 ± 147.68 | 255 | 98 | 1000 | 65.26% |
| CK | 30–170 U/L | 118.04 ± 148.27 | 134.25 | 20 | 1164 | 17.10% |
| Creatinine | 0.5–1.25 mg/dL | 0.93 ± 0.71 | 0.84 | 0.35 | 11.53 | 10.52% |
| AST | 14–59 U/L | 60.96 ± 46.22 | 46 | 12 | 458 | 61.31% |
| ALT | 30–110 U/L | 89.82 ± 84.68 | 67 | 10 | 853 | 73.15% |
| Na+ | 137–145 mmol/L | 136.58 ± 5.09 | 137 | 114 | 149 | 30% |
| K+ | 3.5/5.1 mmol/L | 4.002 ± 0.57 | 4.1 | 2.5 | 5.6 | 20.14% |
| Cl- | 98/107 mmol/L | 99.12 ± 4.42 | 99 | 78 | 109 | 34.43% |
References
- Sočan, M.; Mrzel, M.; Prosenc, K.; Korva, M.; Avšič-Županc, T.; Poljak, M.; Lunar, M.M.; Zupanič, T. Comparing COVID-19 severity in patients hospitalized for community-associated Delta, BA.1 and BA.4/5 variant infection. Front. Public Health 2024, 12, 1294261. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pleșea-Condratovici, C.; Gatej, E.R.; Rizeanu, S.; Pleșea-Condratovici, A. Anxiety in home-quarantined patients with COVID-19. Brain 2022, 13, 347–360. [Google Scholar] [CrossRef]
- Tan, C.; Huang, Y.; Shi, F.; Tan, K.; Ma, Q.; Chen, Y.; Jiang, X.; Li, X. C-reactive protein correlates with computed tomographic findings and predicts severe COVID-19 early. J. Med. Virol. 2020, 92, 856–862. [Google Scholar] [CrossRef]
- Shammus, R.; Mahbub, S.; Rauf, M.A.; Harky, A. The role of imaging and other diagnostic approaches in COVID-19. Acta Biomed. 2020, 91, e2020019. [Google Scholar] [CrossRef]
- Wong, H.Y.F.; Lam, H.Y.S.; Fong, A.H.; Leung, S.T.; Chin, T.W.; Lo, C.S.Y.; Lui, M.M.; Lee, J.C.Y.; Chiu, K.W.; Chung, T.W.; et al. Frequency and Distribution of Chest Radiographic Findings in Patients Positive for COVID-19. Radiology 2020, 296, E72–E78. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Nair, A.; Procter, A.; Halligan, S.; Parry, T.; Ahmed, A.; Duncan, M.; Taylor, M.; Chouhan, M.; Gaunt, T.; Roberts, J.; et al. Chest radiograph classification and severity of suspected COVID-19 by different radiologist groups and attending clinicians: Multi-reader, multi-case study. Eur. Radiol. 2023, 33, 2096–2104. [Google Scholar] [CrossRef]
- Maia, R.; Carvalho, V.; Faria, B.; Miranda, I.; Catarino, S.; Teixeira, S.; Lima, R.; Minas, G.; Ribeiro, J. Diagnosis Methods for COVID-19: A Systematic Review. Micromachines 2022, 13, 1349. [Google Scholar] [CrossRef] [PubMed]
- Ministerul Sănătăţii. Ordinul nr. 487 din 23 Martie 2020 Pentru Aprobarea Protocolului de Tratament al Infecției cu Virusul SARS-CoV-2. Monitorul Oficial, nr. 242, 24 martie 2020; nr. 1167, 3 Decembrie 2020. Available online: https://legislatie.just.ro/public/DetaliiDocument/224341 (accessed on 5 March 2024).
- Ministerul Sănătăţii. OMS 533/2021 din 22 Aprilie 2021 Privind Modificarea anexei la Ordinul Ministrului Sănătăţii nr. 487/2020 Pentru Aprobarea Protocolului de Tratament al Infecţiei cu Virusul SARS-CoV-2. Emitent: Ministerul Sănătăţii Publicat În: Monitorul Oficial NR. 434 din 23 Aprilie 2021. Available online: https://legislatie.just.ro/Public/DetaliiDocument/241318 (accessed on 5 March 2024).
- Ministerul Sănătății. Ordinul nr. 2.103 din 12 Octombrie 2021 Privind Modificarea Anexei la Ordinul Ministrului Sănătății nr. 487/2020 Pentru Aprobarea Protocolului de Tratament al Infecției cu Virusul SARS-CoV-2; Monitorul Oficial, nr. 978, 13 octombrie 2021. Available online: https://legislatie.just.ro/Public/DetaliiDocument/247389 (accessed on 5 March 2024).
- Ministerul Sănătății. Ordinul nr. 74 din 13 Ianuarie 2022 Privind Modificarea Anexei la Ordinul Ministrului Sănătății nr. 487/2020 Pentru Aprobarea Protocolului de Tratament al Infecției cu Virusul SARS-CoV-2; Monitorul Oficial, nr. 40, 13 Ianuarie 2022. Available online: https://legislatie.just.ro/public/DetaliiDocument/250463 (accessed on 5 March 2024).
- Nabulsi, Z.; Sellergren, A.; Jamshy, S.; Lau, C.; Santos, E.; Kiraly, A.P.; Ye, W.; Yang, J.; Pilgrim, R.; Kazemzadeh, S.; et al. Deep learning for distinguishing normal versus abnormal chest radiographs and generalization to two unseen diseases tuberculosis and COVID-19. Sci. Rep. 2021, 11, 15523. [Google Scholar] [CrossRef]
- Au-Yong, I.; Higashi, Y.; Giannotti, E.; Fogarty, A.; Morling, J.R.; Grainge, M.; Race, A.; Juurlink, I.; Simmonds, M.; Briggs, S.; et al. Chest Radiograph Scoring Alone or Combined with Other Risk Scores for Predicting Outcomes in COVID-19. Radiology 2022, 302, E11. [Google Scholar] [CrossRef]
- Borghesi, A.; Zigliani, A.; Golemi, S.; Carapella, N.; Maculotti, P.; Farina, D.; Maroldi, R. Chest X-ray severity index as a predictor of in-hospital mortality in coronavirus disease 2019: A study of 302 patients from Italy. Int. J. Infect. Dis. 2020, 96, 291–293. [Google Scholar] [CrossRef]
- Maroldi, R.; Rondi, P.; Agazzi, G.M.; Ravanelli, M.; Borghesi, A.; Farina, D. Which role for chest x-ray score in predicting the outcome in COVID-19 pneumonia? Eur. Radiol. 2021, 31, 4016–4022. [Google Scholar] [CrossRef] [PubMed]
- WHO. Clinical Management of COVID-19: Living Guideline, 18 August 2023; WHO/2019-nCoV/clinical/2023.2; World Health Organization: Geneva, Switzerland, 2023; Available online: https://iris.who.int/handle/10665/372288 (accessed on 16 February 2024).
- Smith, G.B.; Redfern, O.C.; Pimentel, M.A.; Gerry, S.; Collins, G.S.; Malycha, J.; Prytherch, D.; Schmidt, P.E.; Watkinson, P.J. The National Early Warning Score 2 (NEWS2). Clin. Med. 2019, 19, 260. [Google Scholar] [CrossRef] [PubMed]
- Myrstad, M.; Ihle-Hansen, H.; Tveita, A.A.; Andersen, E.L.; Nygård, S.; Tveit, A.; Berge, T. National Early Warning Score 2 (NEWS2) on admission predicts severe disease and in-hospital mortality from Covid-19—A prospective cohort study. Scand. J. Trauma Resusc. Emerg. Med. 2020, 28, 66. [Google Scholar] [CrossRef] [PubMed]
- Smeltzer, M.P.; Ray, M.A. Statistical considerations for outcomes in clinical research: A review of common data types and methodology. Exp. Biol. Med. 2022, 247, 734–742. [Google Scholar] [CrossRef]
- Vasile, M.C.; Vasile, C.I.; Arbune, A.A.; Nechifor, A.; Arbune, M. Cognitive Dysfunction in Hospitalized Patient with Moderate-to-Severe COVID-19: A 1-Year Prospective Observational Study. J. Multidiscip. Healthc. 2023, 16, 3367–3378. [Google Scholar] [CrossRef]
- Testino, G. Are Patients with Alcohol Use Disorders at Increased Risk for COVID-19 Infection? Alcohol Alcohol. 2020, 55, 344–346. [Google Scholar] [CrossRef]
- Calina, D.; Hartung, T.; Mardare, I.; Mitroi, M.; Poulas, K.; Tsatsakis, A.; Rogoveanu, I.; Docea, A.O. COVID-19 pandemic and alcohol consumption: Impacts and interconnections. Toxicol. Rep. 2021, 8, 529–535. [Google Scholar] [CrossRef]
- Reddy, R.K.; Charles, W.N.; Sklavounos, A.; Dutt, A.; Seed, P.T.; Khajuria, A. The effect of smoking on COVID-19 severity: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 1045–1056. [Google Scholar] [CrossRef]
- Salehi, Z.; Motlagh Ghoochani, B.F.N.; Hasani Nourian, Y.; Jamalkandi, S.A.; Ghanei, M. The controversial effect of smoking and nicotine in SARS-CoV-2 infection. Allergy Asthma Clin. Immunol. 2023, 19, 49. [Google Scholar] [CrossRef]
- Vargas-Gandica, J.; Winter, D.; Schnippe, R.; Rodriguez-Morales, A.G.; Mondragon, J.; Escalera-Antezana, J.P.; Trelles-Thorne, M.D.P.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J.; Paniz-Mondolfi, A. Ageusia and anosmia, a common sign of COVID-19? A case series from four countries. J. Neurovirol. 2020, 26, 785–789. [Google Scholar] [CrossRef]
- Carbone, F.; Casaleggio, A.; Fiannacca, M.; Borda, F.; Ministrini, S.; Vischi, G.; Carpaneto, V.; Sobrero, M.; Monti, C.; De Stefano, D.; et al. Chest X-ray severity score Brixia: From marker of early COVID-19 infection to predictor of worse outcome in internal medicine wards. Eur. J. Clin. Investig. 2023, 53, e13908. [Google Scholar] [CrossRef]
- Gatti, M.; Calandri, M.; Barba, M.; Biondo, A.; Geninatti, C.; Gentile, S.; Greco, M.; Morrone, V.; Piatti, C.; Santonocito, A.; et al. Baseline chest X-ray in coronavirus disease 19 (COVID-19) patients: Association with clinical and laboratory data. Radiol. Med. 2020, 125, 1271–1279. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, D.; Albanesi, M.; Cavigli, E.; Moroni, C.; Bindi, A.; Luvarà, S.; Lucarini, S.; Busoni, S.; Mazzoni, L.N.; Miele, V. Chest X-ray in new Coronavirus Disease 2019 (COVID-19) infection: Findings and correlation with clinical outcome. Radiol. Med. 2020, 125, 730–737. [Google Scholar] [CrossRef]
- Hanley, M.; Brosnan, C.; O’Neill, D.; Ni Mhuircheartaigh, N.; Logan, M.; Morrin, M.M.; Hurley, K.; Sulaiman, I.; O’Brien, E.; Morgan, R.; et al. Modified Brixia chest X-ray severity scoring system and correlation with intubation, non-invasive ventilation and death in a hospitalised COVID-19 cohort. J. Med. Imaging Radiat. Oncol. 2022, 66, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Sofic, A.; Cizmic, M.; Beslagic, E.; Becirevic, M.; Mujakovic, A.; Husic-Selimovic, A.; Granov, L.A. Brixia Chest X-ray Severity Scoring System is in Relation with C-reactive Protein and D-dimer Values in Patients with COVID-19. Mater. Sociomed. 2022, 34, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Nukovic, J.A.; Opancina, V.; Zdravkovic, N.; Prodanovic, N.; Pejcic, A.; Opancina, M.; Nukovic, J.J.; Vojinovic, R.; Dulovic, D.; Jukovic, F.; et al. Brixia Chest X-ray Score, Laboratory Parameters and Vaccination Status for Prediction of Mortality in COVID-19 Hospitalized Patients. Diagnostics 2023, 13, 2122. [Google Scholar] [CrossRef]
- Lian, J.; Jin, C.; Hao, S.; Zhang, X.; Yang, M.; Jin, X.; Lu, Y.; Hu, J.; Zhang, S.; Zheng, L.; et al. High neutrophil-to-lymphocyte ratio associated with progression to critical illness in older patients with COVID-19: A multicenter retrospective study. Aging 2020, 12, 13849–13859. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Y.; Xiang, P.; Pu, L.; Xiong, H.; Li, C.; Zhang, M.; Tan, J.; Xu, Y.; Song, R.; et al. Neutrophil-to-lymphocyte ratio predicts critical illness patients with 2019 coronavirus disease in the early stage. J. Transl. Med. 2020, 18, 206. [Google Scholar] [CrossRef]
- Higaki, A.; Okayama, H.; Homma, Y.; Sano, T.; Kitai, T.; Yonetsu, T.; Torii, S.; Kohsaka, S.; Kuroda, S.; Node, K.; et al. Predictive value of neutrophil-to-lymphocyte ratio for the fatality of COVID-19 patients complicated with cardiovascular diseases and/or risk factors. Sci. Rep. 2022, 12, 13606. [Google Scholar] [CrossRef]
- Fialek, B.; Pruc, M.; Smereka, J.; Jas, R.; Rahnama-Hezavah, M.; Denegri, A.; Szarpak, A.; Jaguszewski, M.J.; Peacock, F.W.; Szarpak, L. Diagnostic value of lactate dehydrogenase in COVID-19: A systematic review and meta-analysis. Cardiol. J. 2022, 29, 751–758. [Google Scholar] [CrossRef]
- Celik Tellioglu, E.; Oncul, A.; Diktas, H.; Atasoy Tahtasakal, C.; Aktas, E.; Genc Yaman, I.; Yildiz Sevgi, D.; Dokmetas, I. The Role of Dynamic Changes in Hematologic and Biochemical Parameters in Predicting Mortality in Covid-19 Patients. Sisli Etfal Hastan. Tip. Bul. 2024, 58, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Martín-Rodríguez, F.; Martín-Conty, J.L.; Sanz-García, A.; Rodríguez, V.C.; Rabbione, G.O.; Cebrían Ruíz, I.; Oliva Ramos, J.R.; Castro Portillo, E.; Polonio-López, B.; Enríquez de Salamanca Gambarra, R.; et al. Early Warning Scores in Patients with Suspected COVID-19 Infection in Emergency Departments. J. Pers. Med. 2021, 11, 170. [Google Scholar] [CrossRef] [PubMed]
- Baig, F.A.; Hamid, A. Predictive Performance of the National Early Warning Score 2 for Stratification of Critically Ill COVID-19 Patients. Eurasian J. Emerg. Med. 2023, 22, 49–54. [Google Scholar] [CrossRef]
- Hoang, S.V.; Nguyen, K.M.; Huynh, T.M.; Huynh, K.L.A.; Nguyen, P.H.; Tran, H.P.N. Chest X-ray Severity Score as a Putative Predictor of Clinical Outcome in Hospitalized Patients: An Experience from a Vietnamese COVID-19 Field Hospital. Cureus 2022, 14, e23323. [Google Scholar] [CrossRef]
- Singh, T.; Mishra, S.; Kalra, R.; Satakshi; Kumar, M.; Kim, T. COVID-19 severity detection using chest X-ray segmentation and deep learning. Sci. Rep. 2024, 14, 19846. [Google Scholar] [CrossRef]
- Aboutalebi, H.; Pavlova, M.; Shafiee, M.J.; Sabri, A.; Alaref, A.; Wong, A. COVID-Net CXR-S: Deep Convolutional Neural Network for Severity Assessment of COVID-19 Cases from Chest X-ray Images. Diagnostics 2021, 12, 25. [Google Scholar] [CrossRef]
- Tenda, E.D.; Yunus, R.E.; Zulkarnaen, B.; Yugo, M.R.; Pitoyo, C.W.; Asaf, M.M.; Islamiyati, T.N.; Pujitresnani, A.; Setiadharma, A.; Henrina, J.; et al. Comparison of the Discrimination Performance of AI Scoring and the Brixia Score in Predicting COVID-19 Severity on Chest X-Ray Imaging: Diagnostic Accuracy Study. JMIR Form Res. 2024, 8, e46817. [Google Scholar] [CrossRef]
- Pérez Laencina, M.; Plasencia Martínez, J.M.; Sánchez Canales, M.; Pulido, C.J.; Mondéjar, R.R.; Encarnación, L.M.; Hidalgo, C.G.; Galián, D.G.; Madrid, P.H.; Caballero, L.C.; et al. A commercial AI tool untrained for COVID-19 demonstrates slight improvement in the interpretation of COVID-19 pneumonia x-rays, especially among inexperienced readers. Radiología, 2025; in press. [Google Scholar] [CrossRef]
- Olar, A.; Biricz, A.; Bedőházi, Z.; Sulyok, B.; Pollner, P.; Csabai, I. Automated prediction of COVID-19 severity upon admission by chest X-ray images and clinical metadata aiming at accuracy and explainability. Sci. Rep. 2023, 13, 4226. [Google Scholar] [CrossRef]
- Rajpoot, R.; Gour, M.; Jain, S.; Semwal, V.B. Integrated ensemble CNN and explainable AI for COVID-19 diagnosis from CT scan and X-ray images. Sci. Rep. 2024, 14, 24985. [Google Scholar] [CrossRef] [PubMed]
- Aboshosha, A. AI based medical imagery diagnosis for COVID-19 disease examination and remedy. Sci. Rep. 2025, 15, 1607. [Google Scholar] [CrossRef] [PubMed]

| Anatomy Region | Score | Score 3 | Score 2 | Score 1 | Score 0 | ||||
|---|---|---|---|---|---|---|---|---|---|
| Average ± SD | n | % | n | % | n | % | n | % | |
| A | 0.45 ± 0.84 | 22 | 5.79% | 22 | 5.79% | 63 | 16.58% | 273 | 71.84% |
| B | 0.88 ± 0.80 | 16 | 4.21% | 55 | 14.47% | 180 | 47.63% | 129 | 33.95% |
| C | 1.26 ± 0.85 | 33 | 8.68% | 105 | 37.63% | 173 | 45.53% | 69 | 18.68% |
| D | 0.37 ± 0.75 | 14 | 3.68% | 21 | 5.52% | 58 | 15.26% | 278 | 75.53% |
| E | 0.86 ± 0.76 | 12 | 3.15% | 52 | 13.68% | 188 | 49.47 | 128 | 33.68% |
| F | 1.30 ± 0.86 | 31 | 8.15% | 124 | 32.63% | 156 | 41.05% | 69 | 18.16% |
| Favorable | Unfavorable | OR | CI 95% | p | ||
|---|---|---|---|---|---|---|
| Age [years] | >65 | 119 | 12 | 2.68 | 1.13; 6.36 | 0.024 |
| <65 | 240 | 9 | ||||
| Gender | Male | 203 | 17 | 3.26 | 1.13; 9.36 | 0.027 |
| Female | 156 | 4 | ||||
| Formal education [years] | >8 | 225 | 9 | 3.26 | 1.39; 7.66 | 0.006 |
| ≤8 | 104 | 12 | ||||
| Smoking | Yes | 235 | 12 | 1.42 | 0.58; 3.45 | 0.437 |
| No | 124 | 9 | ||||
| Alcohol | Yes | 85 | 10 | 2.93 | 1.24; 6.89 | 0.013 |
| No | 274 | 11 | ||||
| Obesity | Yes | 147 | 6 | 1.73 | 0.66; 4.52 | 0.261 |
| No | 212 | 15 | ||||
| Time from onset to admission [days] | ≥6 | 175 | 15 | 2.62 | 1.02; 6.71 | 0.043 |
| <6 | 184 | 6 | ||||
| Chest pains | Yes | 168 | 17 | 4.83 | 1.75; 13.32 | 0.002 |
| No | 191 | 4 | ||||
| Respiratory distress | Yes | 152 | 17 | 5.78 | 2.14; 15.64 | <0.001 |
| No | 207 | 4 | ||||
| NLR | >4 | 139 | 20 | 31.65 | 8.39; 119.31 | <0.001 |
| ≤4 | 220 | 1 | ||||
| CRP [ng/dL] | <10 | 317 | 10 | 8.30 | 3.75; 18.35 | <0.001 |
| ≥10 | 42 | 11 | ||||
| LDH [U/L] | <450 | 320 | 13 | 5.04 | 2.13; 11.94 | <0.001 |
| ≥450 | 39 | 8 | ||||
| Brixia Score > 5 | Yes | 83 | 20 | 66.50 | 21.30; 207.60 | <0.001 |
| No | 276 | 1 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popovici, G.-C.; Georgescu, C.-V.; Plesea, A.C.; Arbune, A.-A.; Cristian, G.; Arbune, M. Prognostic Value of the Brixia Radiological Score in COVID-19 Patients: A Retrospective Study from Romania. Trop. Med. Infect. Dis. 2025, 10, 130. https://doi.org/10.3390/tropicalmed10050130
Popovici G-C, Georgescu C-V, Plesea AC, Arbune A-A, Cristian G, Arbune M. Prognostic Value of the Brixia Radiological Score in COVID-19 Patients: A Retrospective Study from Romania. Tropical Medicine and Infectious Disease. 2025; 10(5):130. https://doi.org/10.3390/tropicalmed10050130
Chicago/Turabian StylePopovici, George-Cosmin, Costinela-Valerica Georgescu, Alina Condratovici Plesea, Anca-Adriana Arbune, Gutu Cristian, and Manuela Arbune. 2025. "Prognostic Value of the Brixia Radiological Score in COVID-19 Patients: A Retrospective Study from Romania" Tropical Medicine and Infectious Disease 10, no. 5: 130. https://doi.org/10.3390/tropicalmed10050130
APA StylePopovici, G.-C., Georgescu, C.-V., Plesea, A. C., Arbune, A.-A., Cristian, G., & Arbune, M. (2025). Prognostic Value of the Brixia Radiological Score in COVID-19 Patients: A Retrospective Study from Romania. Tropical Medicine and Infectious Disease, 10(5), 130. https://doi.org/10.3390/tropicalmed10050130