
Identifying Food Deserts in Mississauga: A Comparative Analysis of Socioeconomic Indicators



Abstract
1. Introduction
2. Material and Methods
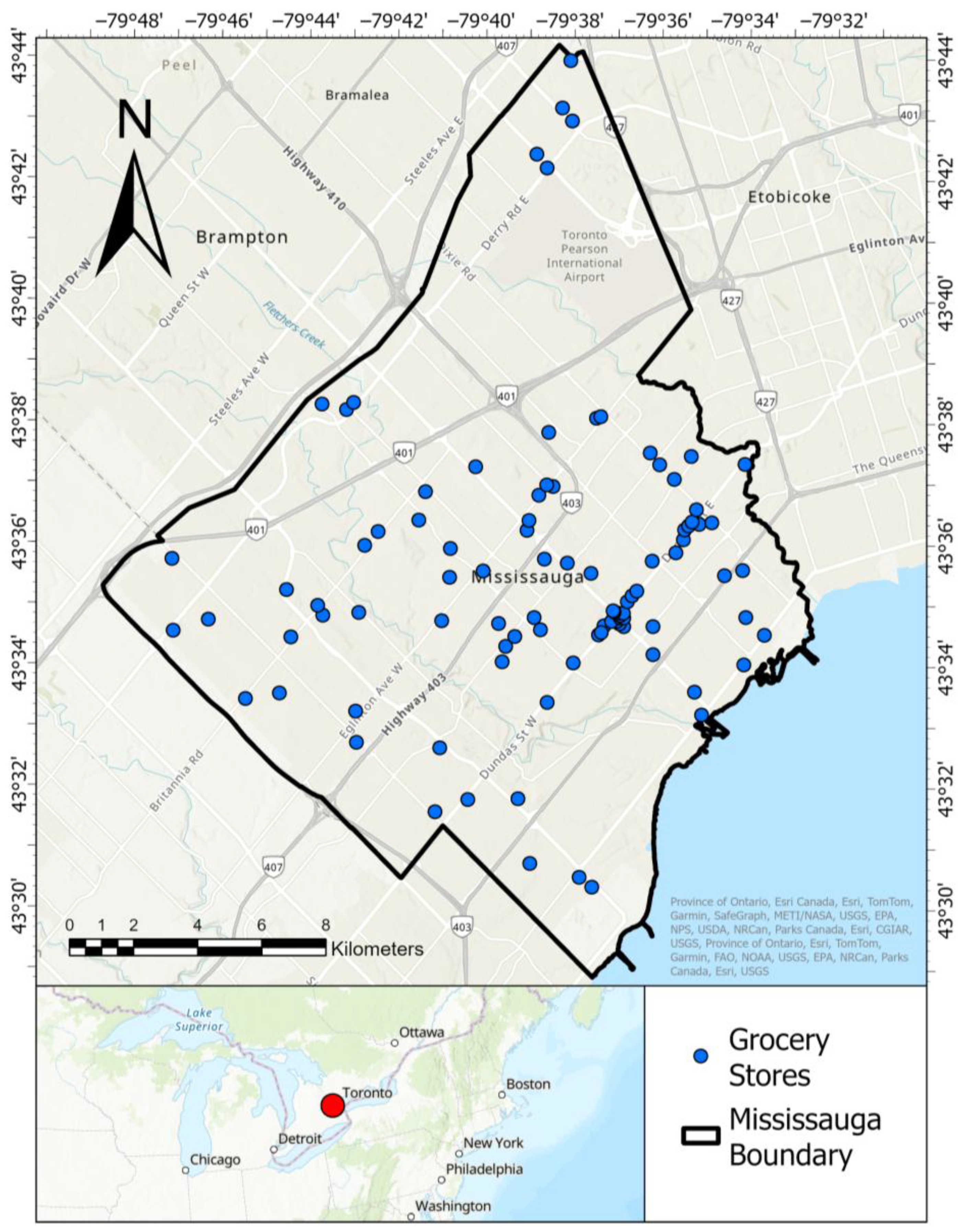
2.1. Study Area
2.2. Data Sources and Preprocessing
2.3. Identifying Food Desert Areas
3. Results
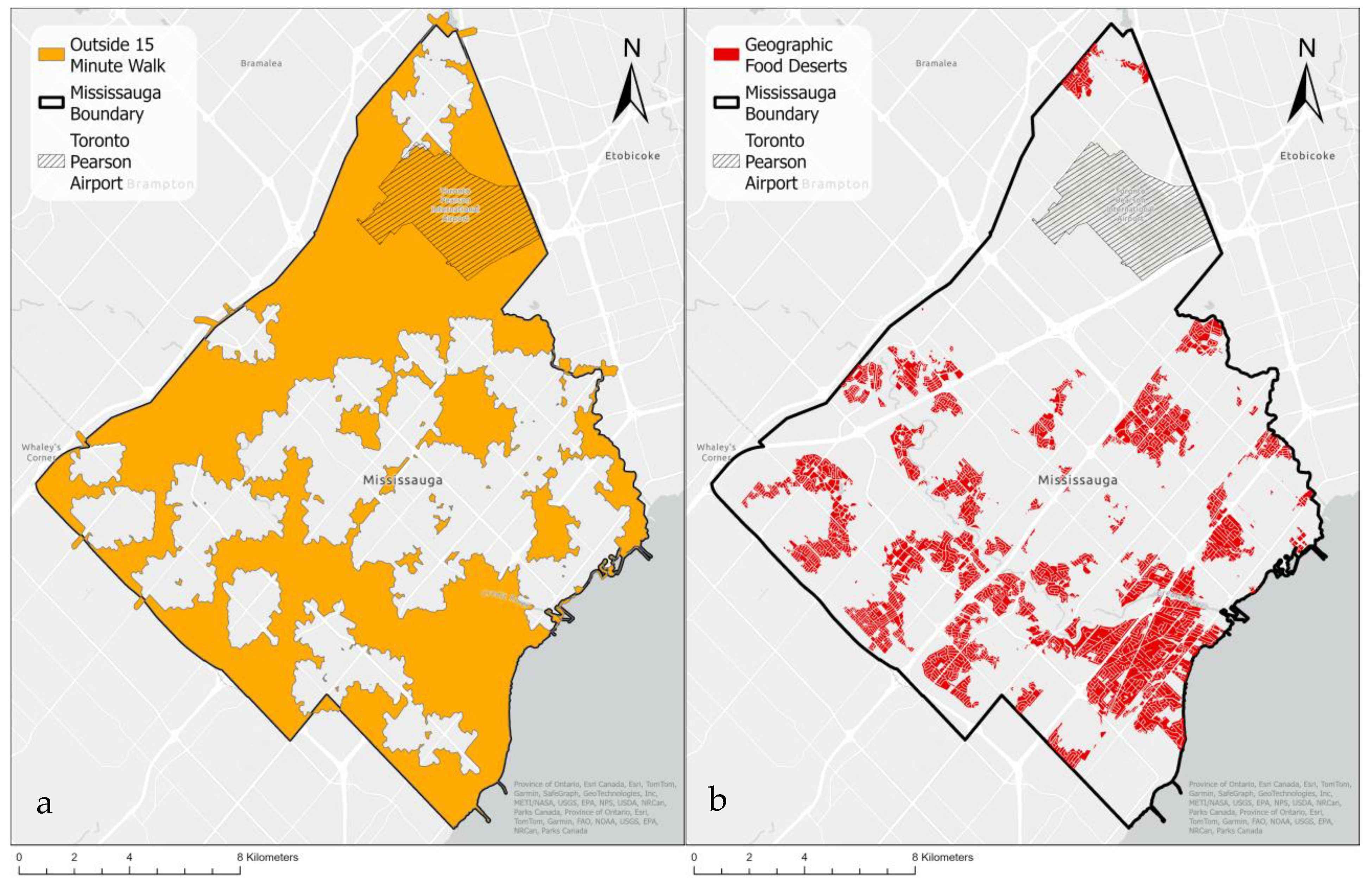
3.1. Food Deserts Based on Geographic Accessibility
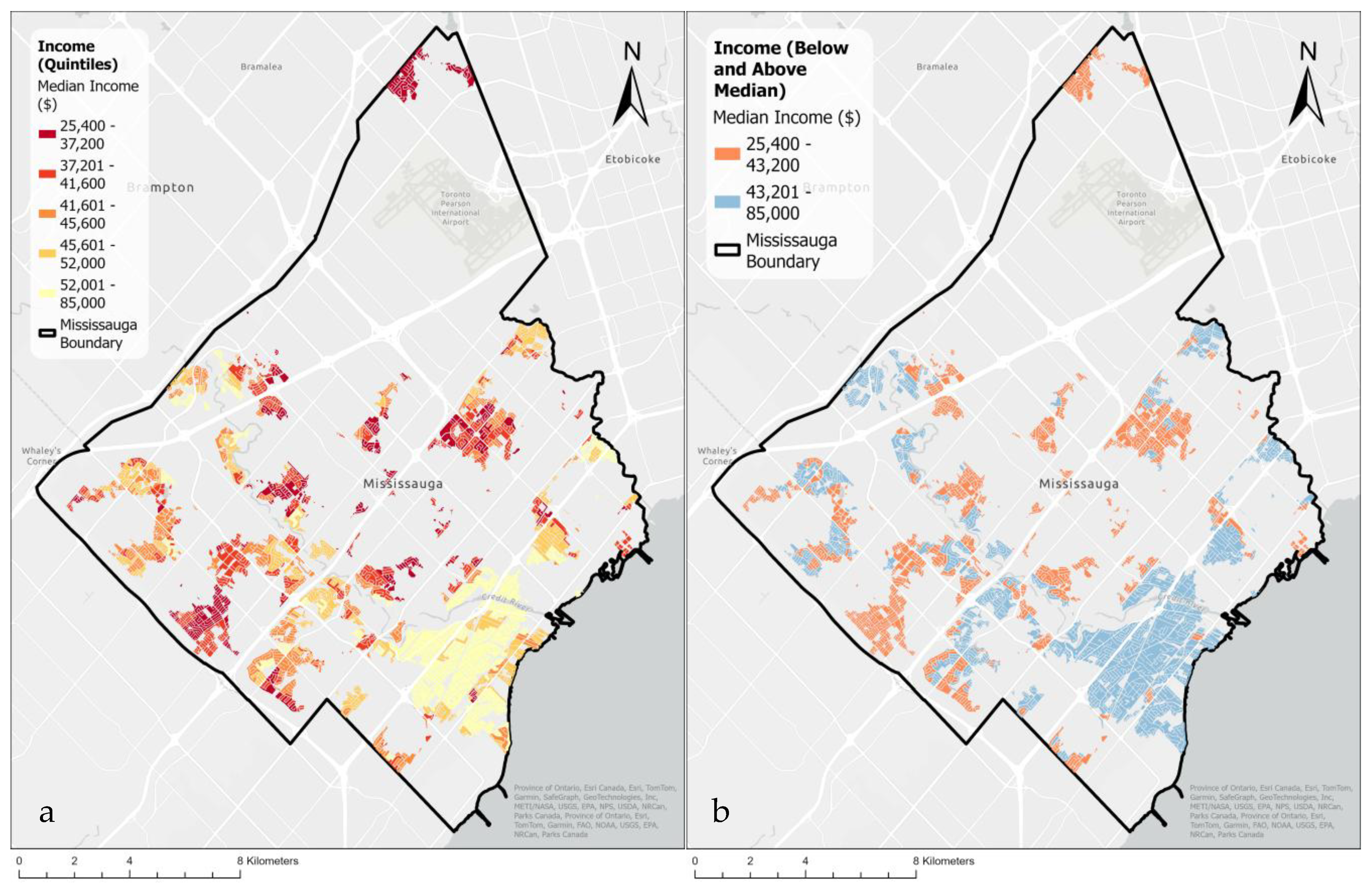
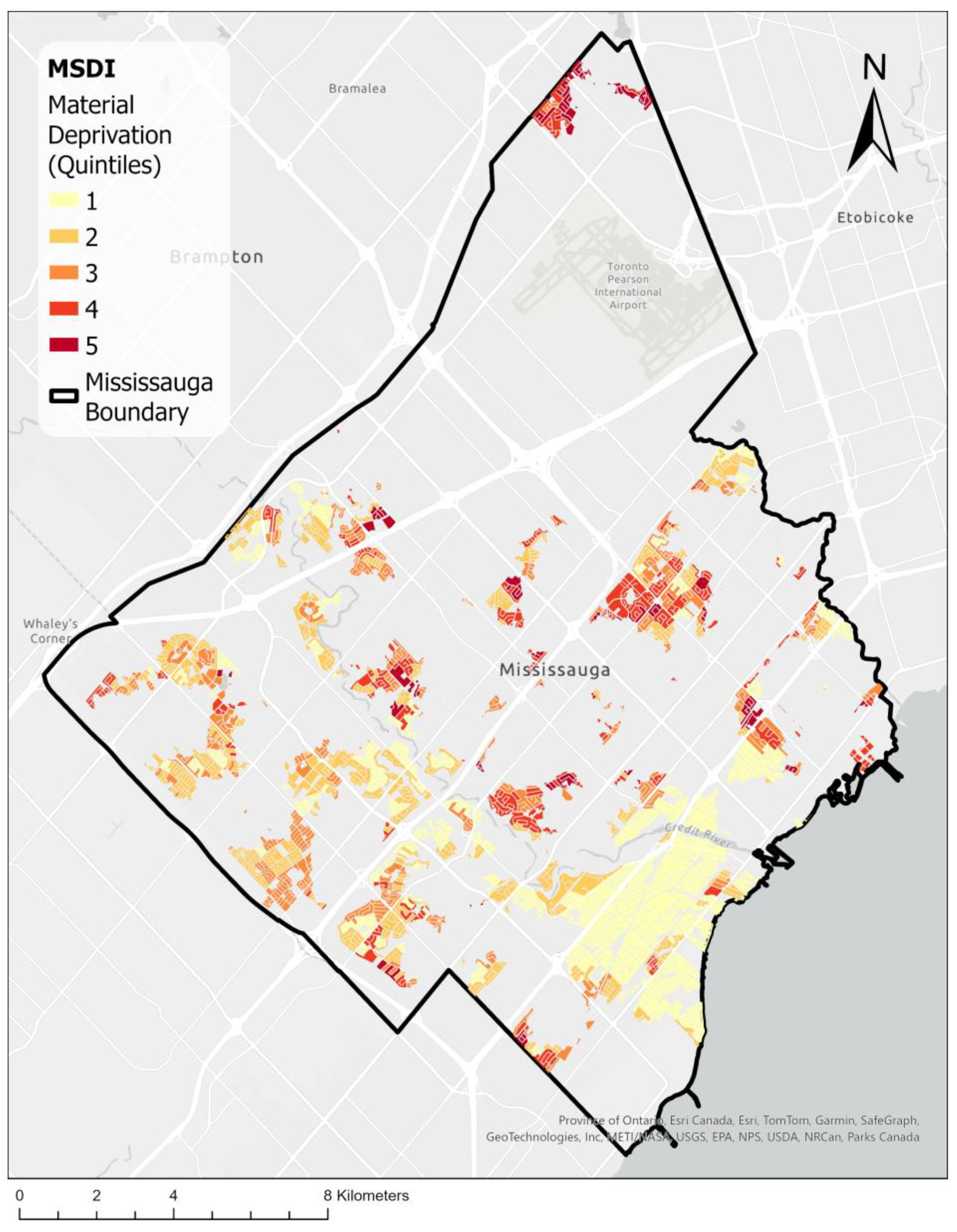
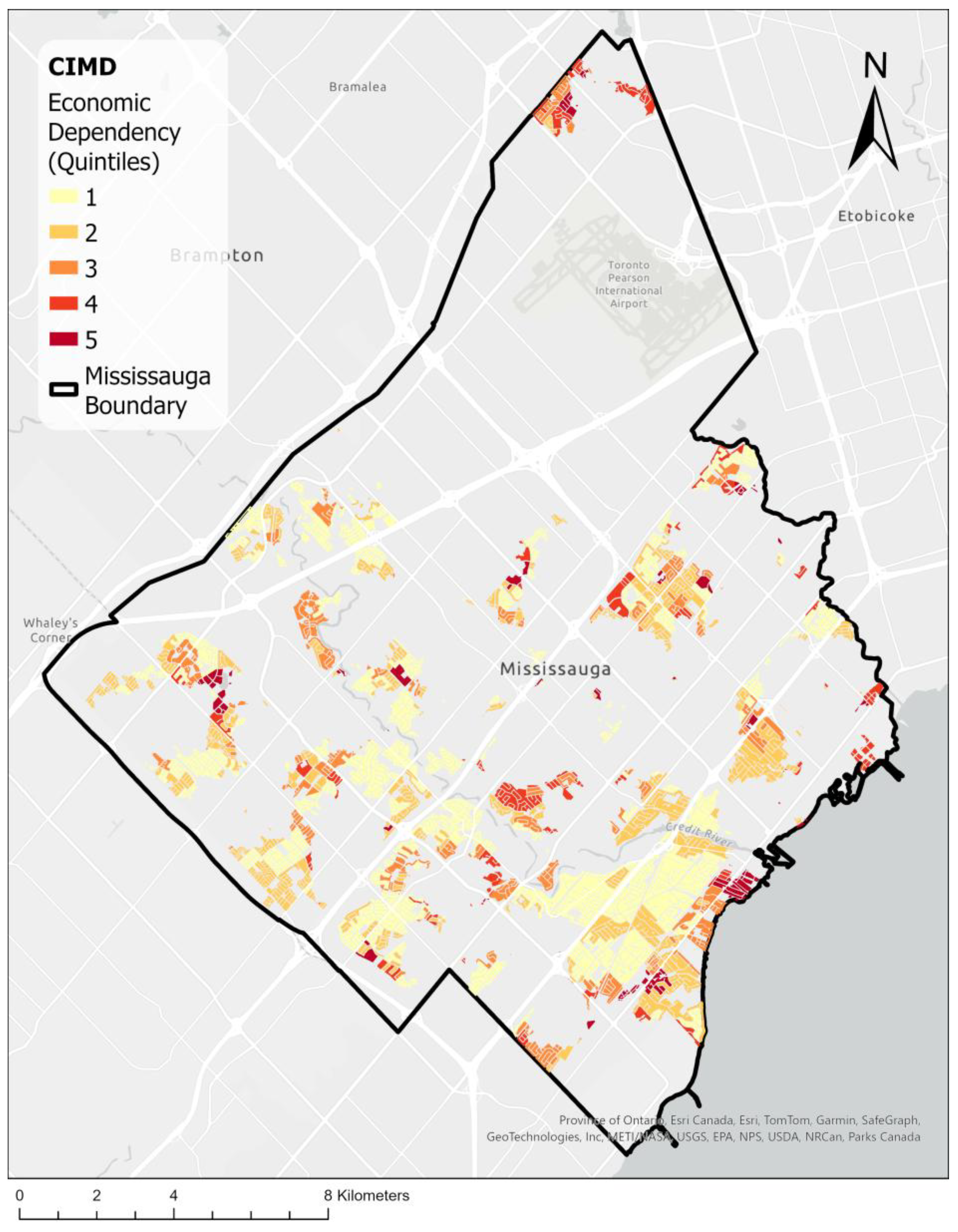
3.2. Socioeconomic Index Maps
3.3. Comparisons of Maps
4. Discussion
4.1. Comparison of Socioeconomic Indicators
4.2. Insights into Food Insecurity
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cummins, S.; Macintyre, S. A Systematic Study of an Urban Foodscape: The Price and Availability of Food in Greater Glasgow. Urban Stud. 2002, 39, 2115–2130. [Google Scholar] [CrossRef]
- McEntee, J. Highlighting Food Inadequacies: Does the Food Desert Metaphor Help This Cause? Br. Food J. 2009, 111, 349–363. [Google Scholar] [CrossRef]
- Breyer, B.; Voss-Andreae, A. Food Mirages: Geographic and Economic Barriers to Healthful Food Access in Portland, Oregon. Health Place 2013, 24, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Qiu, F.; Swallow, B. Can Community Gardens and Farmers’ Markets Relieve Food Desert Problems? A Study of Edmonton, Canada. Appl. Geogr. 2014, 55, 127–137. [Google Scholar] [CrossRef]
- Pollard, C.M.; Nyaradi, A.; Lester, M.; Sauer, K. Understanding Food Security Issues in Remote Western Australian Indigenous Communities. Health Promot. J. Aust. 2014, 25, 83–89. [Google Scholar] [CrossRef]
- de Castro Junior, P.C.; Suéte Matos, Y.A.; de Oliveira, R.T.; Salles-Costa, R.; Ferreira, A.A. Perception of the Food Environment and Food Security Levels of Residents of the City of Rio de Janeiro. Int. J. Environ. Res. Public Health 2025, 22, 642. [Google Scholar] [CrossRef]
- García Bulle Bueno, B.; Horn, A.L.; Bell, B.M.; Bahrami, M.; Bozkaya, B.; Pentland, A.; de la Haye, K.; Moro, E. Effect of Mobile Food Environments on Fast Food Visits. Nat. Commun. 2024, 15, 2291. [Google Scholar] [CrossRef]
- Olive, D. Our Cost-of-Living Crisis: In Just Three Years Rent and Groceries Are up Nearly 40 per Cent—There Are Solutions; Toronto Star: Toronto, ON, USA, 2024. [Google Scholar]
- Raine, K.D. Determinants of Healthy Eating in Canada: An Overview and Synthesis. Can. J. Public Health/Rev. Can. Sante’e Publique 2005, 96, S8–S14. [Google Scholar]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar]
- Chen, Y.; Rennie, D.C.; Dosman, J.A. Changing Prevalence of Obesity in a Rural Community between 1977 and 2003: A Multiple Cross-Sectional Study. Public Health 2009, 123, 15–19. [Google Scholar] [CrossRef]
- Luan, H.; Law, J.; Quick, M. Identifying Food Deserts and Swamps Based on Relative Healthy Food Access: A Spatio-Temporal Bayesian Approach. Int. J. Health Geogr. 2015, 14, 37. [Google Scholar] [PubMed]
- Brownell, K.D.; Kersh, R.; Ludwig, D.S.; Post, R.C.; Puhl, R.M.; Schwartz, M.B.; Willett, W.C. Personal Responsibility and Obesity: A Constructive Approach to A Controversial Issue. Health Aff. 2010, 29, 379–387. [Google Scholar] [CrossRef]
- Slater, J.; Epp-Koop, S.; Jakilazek, M.; Green, C. Food Deserts in Winnipeg, Canada: A Novel Method for Measuring a Complex and Contested Construct. Health Promot. Chronic Dis. Prev. Can. 2017, 37, 350–356. [Google Scholar] [PubMed]
- Smoyer-Tomic, K.E.; Spence, J.C.; Raine, K.D.; Amrhein, C.; Cameron, N.; Yasenovskiy, V.; Cutumisu, N.; Hemphill, E.; Healy, J. The Association between Neighborhood Socioeconomic Status and Exposure to Supermarkets and Fast Food Outlets. Health Place 2008, 14, 740–754. [Google Scholar] [CrossRef]
- Hemphill, E.; Raine, K.; Spence, J.C.; Smoyer-Tomic, K.E. Exploring Obesogenic Food Environments in Edmonton, Canada: The Association between Socioeconomic Factors and Fast-Food Outlet Access. Am. J. Health Promot. 2008, 22, 426–431. [Google Scholar] [CrossRef]
- Bao, K.Y.; Tong, D.; Plane, D.A.; Buechler, S. Urban Food Accessibility and Diversity: Exploring the Role of Small Non-Chain Grocers. Appl. Geogr. 2020, 125, 102275. [Google Scholar] [CrossRef]
- French, S.A.; Tangney, C.C.; Crane, M.M.; Wang, Y.; Appelhans, B.M. Nutrition Quality of Food Purchases Varies by Household Income: The SHoPPER Study. BMC Public Health 2019, 19, 231. [Google Scholar] [CrossRef]
- Seligman, H.K.; Berkowitz, S.A. Aligning Programs and Policies to Support Food Security and Public Health Goals in the United States. Annu. Rev. Public Health 2019, 40, 319–337. [Google Scholar]
- Cummins, S.; Macintyre, S. Food Environments and Obesity—Neighbourhood or Nation? Int. J. Epidemiol. 2005, 35, 100–104. [Google Scholar] [CrossRef]
- Wang, H.; Tao, L.; Qiu, F.; Lu, W. The Role of Socio-Economic Status and Spatial Effects on Fresh Food Access: Two Case Studies in Canada. Appl. Geogr. 2016, 67, 27–38. [Google Scholar] [CrossRef]
- Coplen, A.K. Julie Guthman: Weighing in: Obesity, Food Justice, and the Limits of Capitalism. Agric. Hum. Values 2013, 30, 485–486. [Google Scholar] [CrossRef]
- Shannon, J.; Reese, A.M.; Ghosh, D.; Widener, M.J.; Block, D.R. More Than Mapping: Improving Methods for Studying the Geographies of Food Access. Am. J. Public Health 2021, 111, 1418–1422. [Google Scholar] [CrossRef] [PubMed]
- Gregory, K. Black Food Geographies: Race, Self-Reliance, and Food Access in Washington, D.C. Ashante M. Reese. 2019. Chapel Hill: University of North Carolina Press. Notes, Index, 162 Pages. ISBN: 9781469651491 Paperback. Cult. Agric. Food Environ. 2022, 44, 93–95. [Google Scholar] [CrossRef]
- Robitaille, É.; Paquette, M.-C. Development of a Method to Locate Deserts and Food Swamps Following the Experience of a Region in Quebec, Canada. Int. J. Environ. Res. Public Health 2020, 17, 3359. [Google Scholar] [CrossRef]
- Vaz, E.; Damásio, B.; Bação, F.; Shaker, R.R.; Penfound, E. Urban Habitats and Food Insecurity: Lessons Learned throughout a Pandemic. Habitat Int. 2023, 135, 102779. [Google Scholar] [CrossRef]
- Statistic Canada. Census Profile, 2021 Census of Population; Statistic Canada: Ottawa, ON, Canada, 2021.
- Handy, S. A Cycle of Dependence: Automobiles, Accessibility, and the Evolution of the Transportation and Retail Hierarchies. Berkeley Plan. J. 1993, 8, 21–43. [Google Scholar] [CrossRef]
- Sorensen, A. Toronto Megacity: Growth, Planning Institutions, Sustainability. In Megacities: Urban Form, Governance, and Sustainability; Sorensen, A., Okata, J., Eds.; Springer: Tokyo, Japan, 2011; pp. 245–271. ISBN 978-4-431-99267-7. [Google Scholar]
- Filion, P. Enduring Features of the North American Suburb: Built Form, Automobile Orientation, Suburban Culture and Political Mobilization. Urban Plan. 2018, 3, 4–14. [Google Scholar] [CrossRef]
- Bushnik, T.; Tjepkema, M.; Martel, L. Socioeconomic Disparities in Life and Health Expectancy among the Household Population in Canada. Health Rep. 2020, 31, 3–14. [Google Scholar]
- Larsen, K.; Gilliland, J. Mapping the Evolution of “food Deserts” in a Canadian City: Supermarket Accessibility in London, Ontario, 1961–2005. Int. J. Health Geogr. 2008, 7, 16. [Google Scholar] [CrossRef]
- Pichora, E.; Polsky, J.Y.; Catley, C.; Perumal, N.; Jin, J.; Allin, S. Comparing Individual and Area-Based Income Measures: Impact on Analysis of Inequality in Smoking, Obesity, and Diabetes Rates in Canadians 2003–2013. Can. J. Public Health 2018, 109, 410–418. [Google Scholar] [CrossRef]
- Subramanian, S. 63The Quintile Income Statistic and Distributional Analysis. In Markets, Governance, and Institutions in the Process of Economic Development; Oxford University Press: Oxford, UK, 2017; ISBN 978-0-19-881255-5. [Google Scholar]
- Vanzella-Yang, A.; Veenstra, G. Family Income and Health in Canada: A Longitudinal Study of Stability and Change. BMC Public Health 2021, 21, 333. [Google Scholar] [CrossRef]
- Poirier, M.J.; Wilson, M.G. Rapid Synthesis: Identifying How Area-Based Socio-Economic Indicators Are Measured in Canada. Available online: https://librarysearch.georgebrown.ca/discovery/fulldisplay?vid=01OCLS_BROWN:BROWN&tab=Everything&docid=alma991005118406807310&lang=en&context=L&adaptor=Local%20Search%20Engine&query=sub,exact,Nicu,AND&mode=advanced&offset=10 (accessed on 7 May 2025).
- Pampalon, R.; Hamel, D.; Gamache, P.; Simpson, A.; Philibert, D. Validation of a Deprivation Index for Public Health: A Complex Exercise Illustrated by the Quebec Index; Chronic Diseases and Injuries in Canada; Institut National de Santé Publique du Québec: Québec, QC, Canada, 2014. [Google Scholar]
- Azevedo Da Silva, M.; Gravel, N.; Sylvain-Morneau, J. Material and Social Deprivation Index 2021. Available online: https://canadacommons.ca/artifacts/12251042/material-and-social-deprivation-index-2021/13144894/ (accessed on 1 July 2025).
- Tøge, A.G.; Bell, R. Material Deprivation and Health: A Longitudinal Study. BMC Public Health 2016, 16, 747. [Google Scholar] [CrossRef]
- Relova, S.; Joffres, Y.; Rasali, D.; Zhang, L.R.; McKee, G.; Janjua, N. British Columbia’s Index of Multiple Deprivation for Community Health Service Areas. Data 2022, 7, 24. [Google Scholar] [CrossRef]
- Statistics Canada. The Canadian Index of Multiple Deprivation, User Guide, 2021. Statistics Canada, 2023. Available online: https://www150.statcan.gc.ca/n1/pub/45-20-0001/452000012023002-eng.htm (accessed on 1 July 2025).
- Rent, P.D.; Kumar, S.; Dmello, M.K.; Purushotham, J. Psychosocial Status and Economic Dependence for Healthcare and Nonhealthcare among Elderly Population in Rural Coastal Karnataka. J. Mid-Life Health 2017, 8, 174–178. [Google Scholar]
- Zenk, S.N.; Lachance, L.L.; Schulz, A.J.; Mentz, G.; Kannan, S.; Ridella, W. Neighborhood Retail Food Environment and Fruit and Vegetable Intake in a Multiethnic Urban Population. Am. J. Health Promot. 2009, 23, 255–264. [Google Scholar] [CrossRef]
- Madlala, S.S.; Hill, J.; Kunneke, E.; Lopes, T.; Faber, M. Adult Food Choices in Association with the Local Retail Food Environment and Food Access in Resource-Poor Communities: A Scoping Review. BMC Public Health 2023, 23, 1083. [Google Scholar] [CrossRef]
- Lu, M.; Diab, E. Understanding the Determinants of X-Minute City Policies: A Review of the North American and Australian Cities’ Planning Documents. J. Urban Mobil. 2023, 3, 100040. [Google Scholar] [CrossRef]
- Hosford, K.; Beairsto, J.; Winters, M. Is the 15-Minute City within Reach? Evaluating Walking and Cycling Accessibility to Grocery Stores in Vancouver. Transp. Res. Interdiscip. Perspect. 2022, 14, 100602. [Google Scholar] [CrossRef]
- Lytle, L.A.; Sokol, R.L. Measures of the Food Environment: A Systematic Review of the Field, 2007–2015. Health Place 2017, 44, 18–34. [Google Scholar] [CrossRef]
- Yu, A.; Higgins, C.D. Travel Behaviour and the 15-Min City: Access Intensity, Sufficiency, and Non-Work Car Use in Toronto. Travel Behav. Soc. 2024, 36, 100786. [Google Scholar] [CrossRef]
- Behjat, A.; Koc, M.; Ostry, A. The Importance of Food Retail Stores in Identifying Food Deserts in Urban Settings. WIT Trans. Ecol. Environ. 2013, 170, 89–98. [Google Scholar]
- Páez, A.; Gertes Mercado, R.; Farber, S.; Morency, C.; Roorda, M. Relative Accessibility Deprivation Indicators for Urban Settings: Definitions and Application to Food Deserts in Montreal. Urban Stud. 2010, 47, 1415–1438. [Google Scholar] [CrossRef]
- Payette, H.; Shatenstein, B. Determinants of Healthy Eating in Community-Dwelling Elderly People. Can. J. Public Health 2005, 96, S30–S35. [Google Scholar] [CrossRef]
- Pampalon, R.; Hamel, D.; Alix, C.; Landry, M. A Strategy and Indicators for Monitoring Social Inequalities in Health in Quebec; Institut National de Santé Publique du Québec: Québec, QC, Canada, 2013. [Google Scholar]
- Leete, L.; Bania, N.; Sparks-Ibanga, A. Congruence and Coverage: Alternative Approaches to Identifying Urban Food Deserts and Food Hinterlands. J. Plan. Educ. Res. 2012, 32, 204–218. [Google Scholar] [CrossRef]
- Richardson, A.S.; Ghosh-Dastidar, M.; Beckman, R.; Flórez, K.R.; DeSantis, A.; Collins, R.L.; Dubowitz, T. Can the Introduction of a Full-Service Supermarket in a Food Desert Improve Residents’ Economic Status and Health? Ann. Epidemiol. 2017, 27, 771–776. [Google Scholar] [CrossRef]
- Widener, M.J. Spatial Access to Food: Retiring the Food Desert Metaphor. Physiol. Behav. 2018, 193, 257–260. [Google Scholar] [CrossRef]
- Jiao, J.; Moudon, A.V.; Ulmer, J.M.; Hurvitz, P.M.; Drewnowski, A. How to Identify Food Deserts: Measuring Physical and Economic Access to Supermarkets in King County, Washington. Am. J. Public Health 2012, 102, e32–e39. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description | Data Source |
|---|---|---|
| Median Total Income | Pre-tax employment income value per individual, based on 2021 census data for persons aged 15 years and over. | Statistics Canada |
| MSDI (Material and Social Deprivation Index) | The index measures two dimensions of deprivation, material and social, using Canadian Census variables. This is used in combination with principal component analysis (PCA) to produce a factor score between 1 and 5 to produce deprivation quintiles, with 1 representing the least and 5 representing the most deprived areas. | Statistics Canada |
| CIMD (Canadian Index of Multiple Deprivation) | An indicator capturing four distinct dimensions: residential instability, economic dependency, ethno-cultural composition, and situational vulnerability. The index is calculated with Canadian Census variables and is divided into quintiles from 1 to 5, with 1 representing the least and 5 representing the most deprived areas. | Statistics Canada |
| Healthy Food Providers | A point feature shapefile obtained from the 2021 Mississauga Business Directory and filtered according to the North American Industry Classification System (NAICS). | City of Mississauga Open Data Catalogue |
| Description | Area (km2) | Percentage (Relative to Total Residential Area) | Percentage (Relative to Residential Area Outside 15-Minute Walking Distance) |
|---|---|---|---|
| City of Mississauga | 292.40 | - | - |
| Total Residential Area | 93.75 | 100% | - |
| Residential Area Outside 15 Minutes’ Walking Distance | 39.62 | 42.26% | 100% |
| Below Median Income within GDFs | 16.40 | 17.49% | 41.39% |
| Lowest Income Quintile Area within GDFs | 6.00 | 6.40% | 15.14% |
| Lowest MSDI (Material and Social Deprivation Index) Quintile within GDFs | 2.05 | 2.19% | 5.17% |
| Lowest CIMD (Canadian Index of Multiple Deprivation) Quintile within GDFs | 1.63 | 1.74% | 4.11% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huda, T.; Wang, A.; Zhang, H.; Gao, L.; He, Y.; Zhu, T. Identifying Food Deserts in Mississauga: A Comparative Analysis of Socioeconomic Indicators. Urban Sci. 2025, 9, 265. https://doi.org/10.3390/urbansci9070265
Huda T, Wang A, Zhang H, Gao L, He Y, Zhu T. Identifying Food Deserts in Mississauga: A Comparative Analysis of Socioeconomic Indicators. Urban Science. 2025; 9(7):265. https://doi.org/10.3390/urbansci9070265
Chicago/Turabian StyleHuda, Taif, Amanda Wang, Hefan Zhang, Lewei Gao, Yuhong He, and Tingting Zhu. 2025. "Identifying Food Deserts in Mississauga: A Comparative Analysis of Socioeconomic Indicators" Urban Science 9, no. 7: 265. https://doi.org/10.3390/urbansci9070265
APA StyleHuda, T., Wang, A., Zhang, H., Gao, L., He, Y., & Zhu, T. (2025). Identifying Food Deserts in Mississauga: A Comparative Analysis of Socioeconomic Indicators. Urban Science, 9(7), 265. https://doi.org/10.3390/urbansci9070265