



Social Participation of Frail Older People with Functional Limitations Ageing Alone in Place in Italy, and Its Impact on Loneliness: An Urban–Rural Comparison





Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Sites, and Participants
2.1.1. Study Design
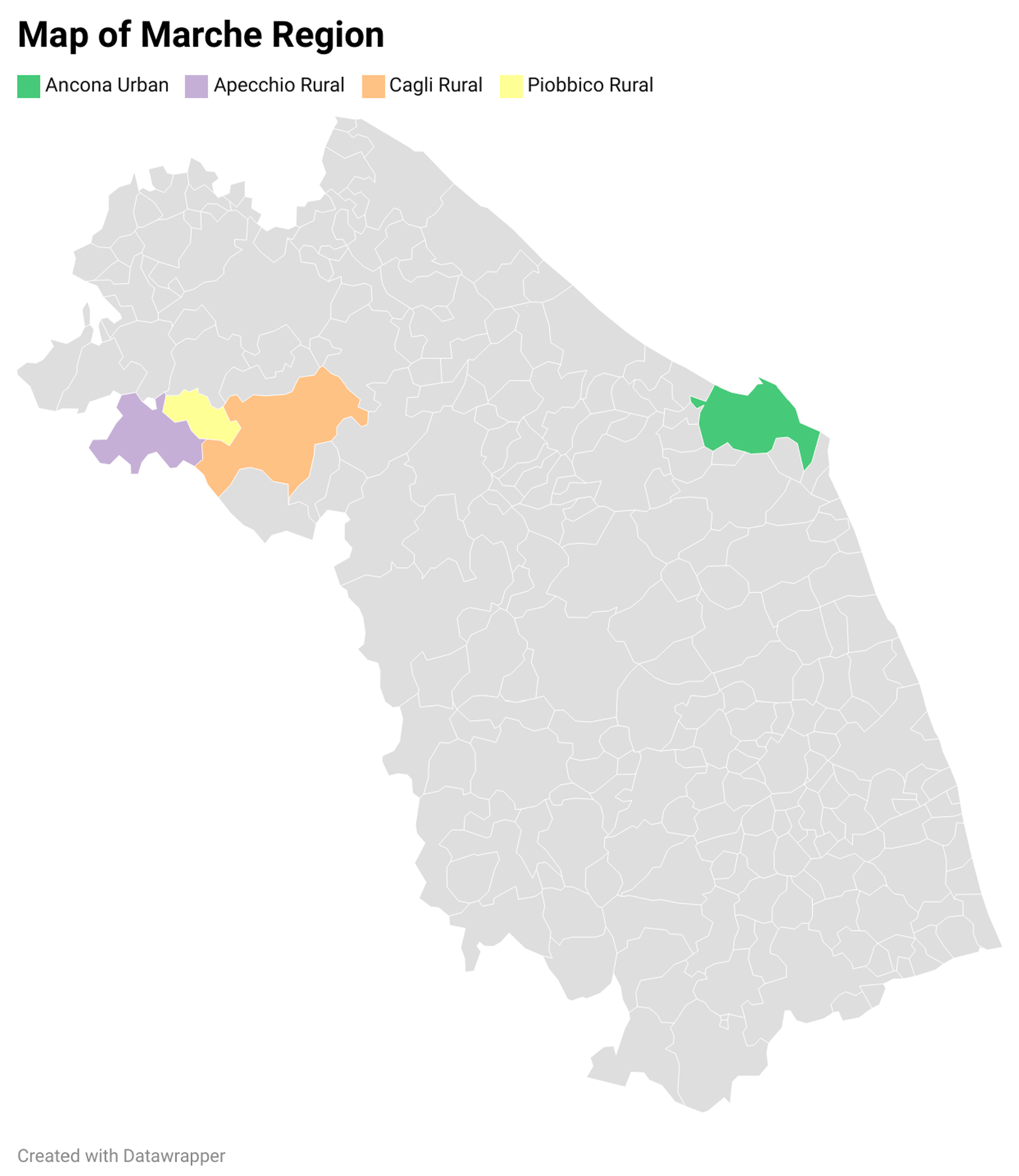
2.1.2. Sites
2.1.3. Participants
2.2. Instruments, Measures, and Ethical Approval
2.2.1. Topic Guide and Ethical Approval
2.2.2. Daily Life Activities
2.2.3. Perceived Loneliness
2.2.4. Social–Leisure Activities
2.3. Data Analysis
2.3.1. Approach and Dimensions
2.3.2. Quantification of Statements and Quotations
2.3.3. The Trustworthiness of the Qualitative Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Social–Leisure Activities of Older People in Urban and Rural Sites of Marche Region: The Count of Statements
3.2.1. Types of Social–Leisure Activities Still Practised
3.2.2. Types of Social–Leisure Activities No Longer Practised
3.2.3. Macro-Categories of Social–Leisure Activities Still Practised
3.2.4. Macro-Categories of Social–Leisure Activities Still Practised and Level of Functional Limitations
3.2.5. Macro-Categories of Social–Leisure Activities Still Practised and Level of Perceived Loneliness
3.3. Social–Leisure Activities of Older People in Urban and Rural Sites of Marche Region: A Storytelling by Oder People
3.3.1. Activities Still Practised
I visit friends I am most familiar with. (Rur-11)
I exchange a few visits with some old friends, those a little freer from grandchildren. (Urb-3)
I watch a lot of TV. I always have the TV on. (Rur-11)
By watching TV too much I have also lost the habit of reading. I have become addicted to TV! The fact of having the immediate image, the immediate word, without effort, evidently takes away my desire to read. (Urb-14)
I often go for walks with friends when they come to visit me. (Rur-16)
I am happy to walk with other seniors that attend with me a day care centre. (Urb-23)
Sometimes on Sundays I go out to eat with two friends. But not often, it is also a question of money! (Rur-10)
I use to go for a pizza with my friends. (Rur-3)
When I go out, we mostly go out to eat pizza together. (Rur-5)
Three or four times a year, for instance at Christmas, Easter or for my birthday, I have lunch at a restaurant with my family. I pay, and I want to do it to bring the family together, children and grandchildren and sometimes my sister too. It is really important to me! (Urb-19)
I practice some gymnastic activities, for instance rehabilitation, at the day care centre, where an operator trains me to walk twice a week with a walker. The centre organises also animation activities. (Urb-20)
If there is a festival, even a parish celebration, I am always the first one to go. (Rur-11)
I like reading, I dedicate most of my time to that. (Rur-15)
I read books and magazines. I really like it, since I was a little girl. (Urb-15)
I have a small vegetable garden that I cultivate. I like to keep it clean. I spend time there. (Rur-12)
Whenever possible I go to the theatre with my daughter. (Rur-14)
I have offered my availability to help cleaning the church in preparation of some charity evening. I can do this but nothing more. (Rur-11)
I take care of plants on my terrace. I like doing it. I also like to play the piano sometimes. (Urb-21)
The library organises a nice initiative in the winter. Somebody chooses a book and the following month everyone comments it in a group, and I participate because I like reading, I dedicate most of my time to that. (Rur-15)
I attend a neighbourhood club quite regularly, with other seniors like me. We play cards. (Urb-8)
I play burraco with friends, sometimes at my house and sometimes at their house. (Rur-10)
I like burraco and every afternoon my sister and some friends come to my house to play together. (Urb-6)
In the summer I take part in some holiday trips organised for older people. We go to the seaside on our region’s coast. (Rur-3)
Every morning, I go to the bar for a coffee. There I meet several people, we talk. (Urb-13)
When I go to the hairdresser, I like it also because I talk to other ladies. (Urb-24)
I visit older people living in nursing homes. I go with some friends. We spend some time together. (Rur-12)
3.3.2. Activities No Longer Practised but That Seniors Would Still Like to Practise
I used to go to the theatre with my husband. Since I am a widow, I do not go there anymore. (Rur-13)
In the past years we used to meet to play cards. Currently we do not do this not anymore, because the other players are all older than me, and the younger ones do not play cards. (Rur-11)
Now between one thing and another we do not see each other anymore, also because someone has died. (Rur-12)
I would like to attend a social club, as I did in the past, but the fact that I do not know other persons who could share this activity with me represents a strong obstacle. (Rur-15)
I used to travel with my husband, but now that I am a widow I do not want to travel with other couples, because I feel uncomfortable among them. They pay too much attention to me, and it seems to me that I am almost a burden, so I avoid it. (Urb-18)
Rural seniors in particular complain about the lack of dedicated spaces allowing seniors to meet and spend time together.
Here we have no spaces to meet with other older people. There is only the nursing home! (Rur-1)
Where I live, we lack a club for seniors. A cinema is lacking too. There is only a tobacconist, we meet there. (Rur-7)
I would really like to have places to meet with other seniors, a recreational place dedicated to us! (Rur-5)
I do not want to do anything anymore. I do not have great relationships with anything. (Urb-1)
I do not practise any activity with other people. When I go out, I feel “out of the world”, I am not comfortable! (Urb-22)
My current bad physical situation prevents me from moving freely, from taking long walks, and so on. However, I am calm, I do not feel the need of such activities. My needs have changed with ageing, and thus I have adapted to do what is still possible for me. (Urb-18)
The streets are made of cobblestones and when I walk, I fear falling! (Rur-1)
The bus has a short timeline, only few trips a day! (Rur-9)
3.3.3. Activities Still Practised and Physical Limitations
Since my health has worsened, I move little. My friends come to visit me. (Urb-7)
My children often invite me out to eat at a restaurant, but this is a problem! I cannot eat what I want, I have to be careful. (Urb-24)
I spent almost two years volunteering for older people. I entertained them with games and I also accompanied them home. I cannot do the latter anymore. Because I use a stick to walk and thus, I fear I cannot appropriately support others. I am afraid of making them falling. (Urb-16)
I only hear Mass on the radio, the church is far away and I cannot go there. My knee is in bad shape! (Rur-5)
I am not so well. I watch Holy Mass on Sundays on TV. Then the priest comes to bring me Communion at home once a month. (Rur-16)
I used to always go to church, but now I cannot and thus I listen to Mass on TV every morning. (Urb-13)
I walk a lot. I like going out with friends or with my niece. However, I do not walk for long distances because I get tired. I take a lot of short walks. (Rur-13)
I go for walks but I have to be careful, now I walk badly and I am afraid of falling. (Rur-14)
I do not go to the gym. I have trouble moving. My daughter does yoga and taught me how to do some exercises that I can do alone at home. (Rur-11)
I do rehabilitation and walks organised by the day care centre. (Urb-23)
I go on mountain walking which are organised by the parish. (Urb-4)
I take short walks every day with a stick, but I walk badly, slowly and I stop often. (Urb-16)
For Easter and Christmas I go to my sister’s house or she comes to mine and we play cards. (Rur-8)
I read the newspaper, it helps me pass the time and feel less alone. (Rur-10)
Sometimes I go to visit a daughter out of my region. However, I am old and I feel less and less safe traveling alone. I am afraid to be alone for three hours on the train, without some relative. What if I feel sick during the travel? (Urb-15)
I cannot go out alone anymore, because otherwise I fall. Also, I cannot take the bus alone. In fact, I used to take the bus, I did volunteer work, I played burraco, I went on trips. Now I spend almost all my time at home watching TV, and many times I get bored, it is not a nice life. Sometimes my grandchildren come to visit me, but they also have their own commitments! (Urb-9)
Now I cannot do many activities anymore. Some years ago, I had a more active life, I went out, I went to the market, I met people, I talked with other seniors. Now I only watch TV. I watch a lot of TV, maybe too much! (Urb-10)
I watch TV but I do not see it, I just listen to it. (Rur-3)
I do not go to parties because I cannot move alone. Nobody takes me there! (Rur-16)
I would like to be active in politics again. In the past I was more active, now I have some physical problems and I should be accompanied. I would like to have such a commitment, not only to spend time, but also to do something good for the society. (Urb-3)
I cannot go anywhere! To be able to move I need someone who would accompany me! (Urb-7)
When I had a better health, I did volunteering activity, went to cinemas and museums, and played cards. I took a lot of walks. Now I would like to do all these things as in the past, but I cannot walk well on my own anymore, I cannot even go shopping alone. (Rur-3)
I was active in politics, I did volunteer work, I used to travel and take long walks. I cannot do anything anymore! (Rur-10)
3.3.4. Activities Still Practised and Perceived Loneliness
To overcome some moments of loneliness I turn on the TV and make zapping. I go back and forth among channels until I find something that gives me a bit of joy, or that engages me in thinking a little. (Urb-14)
I am calm, I do not get down, even if I spend a lot of time alone, the TV is always on, it keeps me company. I also have a lot of people close to me. I am fine like this. (Rur-2)
I do not feel alone. I always see my children. They come to visit me very often. (Urb-5)
If there is some cultural event, I am invited and accompanied. I am happy to go. (Urb-13)
Spending time with my burraco friends, talking to them, helps me a lot. (Urb-6)
I have a small vegetable garden near the river, and take care of it keeps me company. (Rur-7)
I am fine, I do not feel alone because my children call me and come to visit me all the time. I am fine alone, I watch TV, then I do crosswords. I also go out and I meet many people and we talk together. I also talk a little with the parish priest who gives me strength. (Urb-24)
I spend little time with the family, at least lunches or dinners only at Easter and Christmas, twice a year. I feel alone (Urb-12)
I would like to see my daughters more often. I also miss my village dinners, which I cannot longer have. I feel isolated, and these moments weigh on me, especially when my friends have dinners together and do not invite me! (Rur-9)
It is hard for me to be alone, I would like to see friends, to spend time with them, to go out and chat with them. (Rur-4)
What weighs on me most is the lack of company. The company of friends is what I need most. I would like to meet other people, go out more often. (Rur-1)
I feel a deep sense of loneliness, because being always at home, seeing only these four walls, makes me feel extremely melancholic. It is like a prison and I cannot stand it anymore. I was so dynamic, I practised many activities, and now I do not do anything anymore. This is not a nice life! (Urb-9)
I do not make any activity anymore. Everything has “decayed” since I got old. I feel like I have nothing left. I am alone. (Urb-11)
I receive visits from my friends. Once a week with my friends we go to eat at the restaurant. I go to the UNI-3. Two or three times a year I go to the theatre to listen to music. Every day I go for walks with a stick. Yet I often feel alone, my moments of solitude weigh on me, I miss a male companion. (Rur-8)
Sometimes I go with friends to eat at the restaurant. I go to Mass every day. I also play burraco, I always watch TV. When the theatre is open, I go about once a month. However, I feel loneliness! (Rur-10)
I spend every Sunday with my daughters, but despite this I feel alone. (Urb-15)
I feel alone even when I spend time with my family. The problem is that I am widow! (Urb-18)
The older you get, the more fragile and alone you become. Sometimes the hours are long and so heavy! (Urb-1)
I do not feel loneliness, because I chat a lot with old friends also by smartphone. (Urb-2)
I do not feel lonely. I meet friends, and we chat. (Rur-11)
4. Discussion
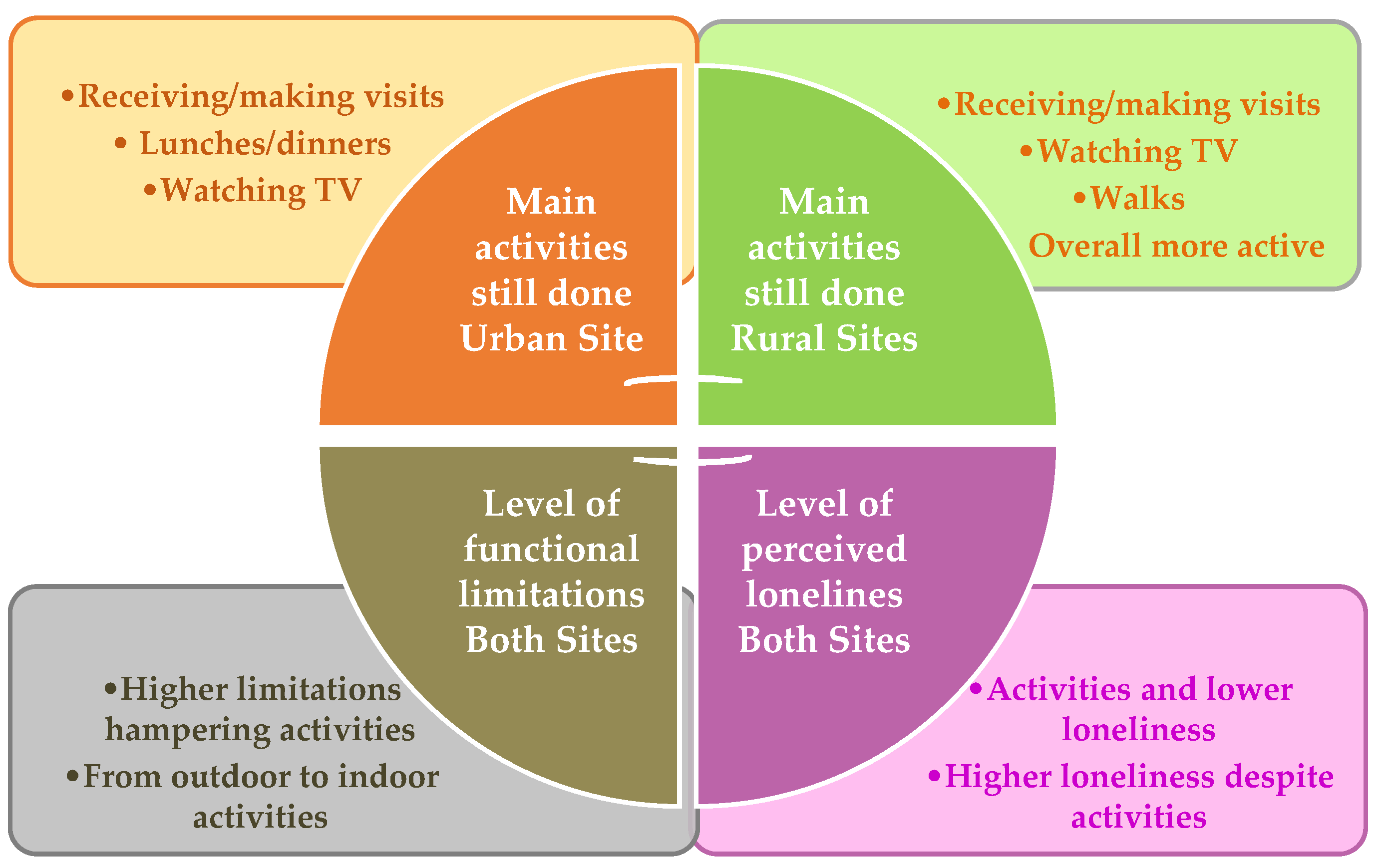
4.1. Social–Leisure Activities Still Practised by Older People in Urban–Rural Sites
4.2. Social–Leisure Activities No Longer Practised by Older People in Urban–Rural Sites
4.3. Social–Leisure Activities Still Practised and Level of Functional Limitations in Urban–Rural Sites
4.4. Social–Leisure Activities Still Practised and Level of Perceived Loneliness in Urban–Rural Sites
4.5. Limitations
4.6. Possible Practical Interventions
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, E. Inventory and analysis of definitions of social participation found in the aging literature: Proposed taxonomy of social activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef] [PubMed]
- Levasseur, M.; Naud, D.; Bruneau, J.F.; Généreux, M. Environmental Characteristics Associated with Older Adults’ Social Participation: The Contribution of Sociodemography and Transportation in Metropolitan, Urban, and Rural Areas. Int. J. Environ. Res. Public Health 2020, 17, 8399. [Google Scholar] [CrossRef] [PubMed]
- Hashidate, H.; Shimada, H.; Fujisawa, Y.; Yatsunami, M. An Overview of Social Participation in Older Adults: Concepts and Assessments. Phys. Ther. Res. 2021, 24, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Feng, Q.; Zhu, H.; Dupre, M.E.; Gu, D. Social Participation. In Encyclopedia of Gerontology and Population Aging; Gu, D., Dupre, M.E., Eds.; Springer: Cham, Switzerland, 2022; pp. 1–10. [Google Scholar]
- Piškur, B.; Daniëls, R.; Jongmans, M.J.; Ketelaar, M.; Smeets, R.J.; Norton, M.; Beurskens, A.J. Participation and social participation: Are they distinct concepts? Clin. Rehabil. 2014, 28, 211–220. [Google Scholar] [CrossRef]
- Toepoel, V. Ageing, Leisure, and Social Connectedness: How could Leisure Help Reduce Social Isolation of Older People? Soc. Indic. Res. 2013, 113, 355–372. [Google Scholar] [CrossRef]
- Walsh, K.; Scharf, T.; Keating, N. Social exclusion of older persons: A scoping review and conceptual framework. Eur. J. Ageing 2017, 14, 81–98. [Google Scholar] [CrossRef]
- Moffatt, S.; Glasgow, N. How Useful is the Concept of Social Exclusion when Applied to Rural Older People in the United Kingdom and the United States? Reg. Stud. 2009, 43, 1291–1303. [Google Scholar] [CrossRef]
- Levasseur, M.; Lussier-Therrien, M.; Biron, M.L.; Raymond, E.; Castonguay, J.; Naud, D.; Fortier, M.; Sévigny, A.; Houde, S.; Tremblay, L. Scoping study of definitions of social participation: Update and co-construction of an interdisciplinary consensual definition. Age Ageing 2022, 51, afab215. [Google Scholar] [CrossRef]
- Duppen, D.; Lambotte, D.; Dury, S.; Smetcoren, A.S.; Pan, H.; De Donder, L.; D-SCOPE Consortium. Social Participation in the Daily Lives of Frail Older Adults: Types of Participation and Influencing Factors. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 2062–2071. [Google Scholar] [CrossRef]
- Pospíšil, J.; Pospíšilová, H.; Trochtová, L. The Catalogue of Leisure Activities: A New Structured Values and Content Based Instrument for Leisure Research Usable for Social Development and Community Planning. Sustainability 2022, 14, 2657. [Google Scholar] [CrossRef]
- Adams, K.B.; Leibbrandt, S.; Moon, H. A critical review of the literature on social and leisure activity and wellbeing in later life. Ageing Soc. 2011, 31, 683–712. [Google Scholar] [CrossRef]
- Suanet, B. Social Participation. Longitudinal Aging Study Amsterdam; LASA: Amsterdam, The Netherland, 2020; Available online: https://lasa-vu.nl/topics/social-participation/ (accessed on 10 January 2025).
- Serrat, R.; Scharf, T.; Villar, F.; Gómez, C. Fifty-five years of research into older people’s civic participation: Recent trends, future directions. Gerontologist 2020, 60, e38–e51. [Google Scholar] [CrossRef] [PubMed]
- Kahlert, D.; Ehrhardt, N. Out-of-Home Mobility and Social Participation of Older People: A Photo-Based Ambulatory Assessment Study. J. Popul. Ageing 2020, 13, 547–560. [Google Scholar] [CrossRef]
- Körlof, L.; Nyman, A.; Isaksson, G.; Larsson, E. Older Adults’ Experiences of Using Strategies to Maintain and Foster Social Participation: A Systematic Review with Metasynthesis of Qualitative Studies. Health Soc. Care Community 2024, 61, 1–16. [Google Scholar] [CrossRef]
- Dehi Aroogh, M.; Mohammadi Shahboulaghi, F. Social Participation of Older Adults: A Concept Analysis. Int. J. Community Based Nurs. Midwifery 2020, 8, 55–72. [Google Scholar] [CrossRef]
- Costa, G.; Melchiorre, M.G.; Arlotti, M. Ageing in place in different care regimes. The role of care arrangements and the implications for the quality of life and social isolation of frail older people. DAStU Work. Pap. Ser. 2020, 3, LPS.10. Available online: http://www.lps.polimi.it/wp-content/uploads/2020/09/WP-Dastu-32020_new-2.pdf (accessed on 15 January 2025).
- Svensson, G.L.; Stjernborg, V. Ageing, social participation, and everyday mobility—Facilitating age-friendly environments. J. Urban Mobil. 2024, 6, 100096. [Google Scholar] [CrossRef]
- Lodi Rizzini, C.; Maino, F.; De Tommaso, C.V. Ageing in Place, Healthy Ageing: Local Community Involvement in the Prevention Approach to Eldercare. Soc. Incl. 2024, 12, 7438. [Google Scholar] [CrossRef]
- WHO. How to Use ICF. A Practical Manual for Using the International Classification of Functioning, Disability and Health; WHO: Geneva, Switzerland, 2013; Available online: https://www.who.int/publications/m/item/how-to-use-the-icf---a-practical-manual-for-using-the-international-classification-of-functioning-disability-and-health (accessed on 15 January 2025).
- Dykstra, P.A. Older adult loneliness: Myths and realities. Eur. J. Ageing 2009, 6, 91–100. [Google Scholar] [CrossRef]
- Latikka, R.; Rubio-Hernández, R.; Lohan, E.S.; Rantala, J.; Nieto Fernández, F.; Laitinen, A.; Oksanen, A. Older Adults’ Loneliness, Social Isolation, and Physical Information and Communication Technology in the Era of Ambient Assisted Living: A Systematic Literature Review. J. Med. Internet Res. 2021, 23, e28022. [Google Scholar] [CrossRef]
- Teh, J.K.L.; Tey, N.P. Effects of selected leisure activities on preventing loneliness among older Chinese. SSM Popul. Health 2019, 9, 100479. [Google Scholar] [CrossRef] [PubMed]
- Aman, H.K. The impact of sense of loneliness on geriatric depression: The mediating role of sense of mattering and psychological adjustment. Middle East Curr Psychiatry 2024, 31, 70. [Google Scholar] [CrossRef]
- Banerjee, A.; Duflo, E.; Grela, E.; McKelway, M.; Schilbach, F.; Sharma, G.; Vaidyanathan, G. Depression and Loneliness among the Elderly in Low- and Middle-Income Countries. J. Econ. Perspect. 2023, 37, 179–202. [Google Scholar] [CrossRef]
- Holwerda, T.J.; Rhebergen, D.; Comijs, H.C.; Dekker, J.J.M.; Stek, M.L. Loneliness and mortality in older adults and the role of depression. Int. Psychogeriatr. 2020, 32, 64. [Google Scholar] [CrossRef]
- Singh, A.; Misra, N. Loneliness, depression and sociability in old age. Ind. Psychiatry J. 2009, 18, 51–55. [Google Scholar] [CrossRef]
- Martinelli, F.; Cilio, A.; Vecchio Ruggeri, S. Ageing in place e contesto abitativo I condizionamenti dell’ambiente costruito sulla qualitaà della vita e sui rischi di isolamento degli anziani fragili che invecchiano soli a casa propria: Barriere, mobilitaà, socialitaà. DAStU Work. Pap. Ser. 2021, 6, LPS.20. Available online: https://www.lps.polimi.it/wp-content/uploads/2021/05/DAStU_WP_no-62021.pdf (accessed on 15 January 2025).
- Martinelli, F.; Sarlo, A.; Bagnato, F. Ageing in place: L’importanza dell’ambiente costruito. In La Solitudine Dei Numeri Ultimi. Invecchiare Da Soli Nell’epoca Della Pandemia; Ranci, C., Arlotti, M., Lamura, G., Martinelli, F., Eds.; Il Mulino: Bologna, Italy, 2023; pp. 139–176. [Google Scholar]
- Figueiredo, M.; Eloy, S.; Marques, S.; Dias, L. Older people perceptions on the built environment: A scoping review. Appl. Ergon. 2023, 108, 103951. [Google Scholar] [CrossRef]
- Katz, S. Assessing Self-Maintenance: Activities of Daily Living, Mobility, and Instrumental Activities of Daily Living. J. Am. Geriatr. Soc. 1983, 31, 721–727. [Google Scholar] [CrossRef]
- Qin, Y.; Hao, X.; Lv, M.; Zhao, X.; Wu, S.; Li, K. A global perspective on risk factors for frailty in community-dwelling older adults: A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2023, 105, 104844. [Google Scholar] [CrossRef]
- Yang, X.; Wang, W.; Zhou, W.; Zhang, H. Effect of leisure activity on frailty trajectories among Chinese older adults: A 16-year longitudinal study. BMC Geriatr. 2024, 24, 771. [Google Scholar] [CrossRef]
- Shimada, H.; Doi, T.; Tsutsumimoto, K.; Lee, S.; Bae, S.; Arai, H. Behavioral factors related to the incidence of frailty in older adults. J. Clin. Med. 2020, 9, 3074. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Li, X.; Gao, X.; Wei, Y.; Ye, L.; Liu, S.; Ye, J.; Qiu, Y.; Zheng, X.; Chen, C.; et al. Leisure activities, genetic risk, and Frailty: Evidence from the Chinese adults aged 80 years or older. Gerontology 2023, 69, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.J.; Wray, L.; Lin, Y. Social relationships, leisure activity, and health in older adults. Health Psychol. 2014, 33, 516–523. [Google Scholar] [CrossRef]
- Bengtson, V.L.; Putney, N. Handbook of Theories of Ageing; Springer: Cham, Switzerland, 2009. [Google Scholar]
- Principi, A.; Di Rosa, M.; Domínguez-Rodríguez, A.; Varlamova, M.; Barbabella, F.; Lamura, G.; Socci, M. The Active Ageing Index and policy making in Italy. Ageing Soc. 2023, 43, 2554–2579. [Google Scholar] [CrossRef]
- Xu, Z.; Zhang, W.; Zhang, X.; Wang, Y.; Chen, Q.; Gao, B.; Li, N. Multi-Level Social Capital and Subjective Wellbeing Among the Elderly: Understanding the Effect of Family, Workplace, Community, and Society Social Capital. Front. Public Health 2022, 10, 772601. [Google Scholar] [CrossRef]
- Diener, E. Subjective well-being: The science of happiness and a proposal for a national index. Am. Psychol. 2000, 55, 34–43. [Google Scholar] [CrossRef]
- Tough, H.; Siegrist, J.; Fekete, C. Social relationships, mental health and well-being in physical disability: A systematic review. BMC Pub. Health 2017, 17, 414. [Google Scholar] [CrossRef]
- Routasalo, P.E.; Tilvis, R.S.; Kautiainen, H.; Pitkala, K.H. Effects of psychosocial group rehabilitation on social functioning, loneliness and well-being of lonely, older people: Randomized controlled trial. J. Adv. Nurs. 2010, 65, 297–305. [Google Scholar] [CrossRef]
- Cramm, J.M.; Nieboer, A.P. Social cohesion and belonging predict the well-being of community-dwelling older people. BMC Geriatr. 2015, 15, 30. [Google Scholar] [CrossRef]
- Jiao, D.; Miura, K.W.; Sawada, Y.; Matsumoto, M.; Ajmal, A.; Tanaka, E.; Watanabe, T.; Sujisawa, Y.; Ito, S.; Okumura, R.; et al. Social Relationships and Onset of Functional Limitation among Older Adults with Chronic Conditions: Does gender matter? Sultan Qaboos Univ. Med. J. 2023, 23, 13–21. [Google Scholar] [CrossRef]
- Provencher, V.; Carbonneau, H. Social participation, leisure and active aging. Soc. Leis. 2019, 42, 1–3. [Google Scholar] [CrossRef]
- Du, C.; Li, X.; Li, J.; Wang, W.; Dang, M.; Cheng, J.; Xu, K.; Wang, J.; Chen, C.; Chen, Y.; et al. Leisure activities as reserve mediators of the relationship between loneliness and cognition in aging. Transl. Psychiatry 2024, 14, 217. [Google Scholar] [CrossRef] [PubMed]
- Conde-Sala, J.L.; Garre-Olmo, J.; Calvó-Perxas, L.; Turró-Garriga, O.; Vilalta-Franch, J. Course of depressive symptoms and associated factors in people aged 65+ in Europe: A two-year follow-up. J Affect. Disord. 2019, 245, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Jiao, D.; Watanabe, K.; Sawada, Y.; Tanaka, E.; Watanabe, T.; Tomisaki, E.; Ito, S.; Okumura, R.; Kawasaki, Y.; Anme, T. Multimorbidity and functional limitation: The role of social relationships. Arch. Gerontol. Geriatr. 2021, 92, 104249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Hao, X.; Qin, Y.; Yang, Y.; Zhao, X.; Wu, S.; Li, K. Social participation classification and activities in association with health outcomes among older adults: Results from a scoping review. J. Adv. Nurs. 2025, 81, 661–678. [Google Scholar] [CrossRef]
- Hanlon, P.; Wightman, H.; Politis, M.; Kirkpatrick, S.; Jones, C.; Andrew, M.K.; Vetrano, D.L.; Dent, E.; Hoogendijk, E.O. The relationship between frailty and social vulnerability: A systematic review. Lancet Healthy Longev. 2024, 5, e214–e226. [Google Scholar] [CrossRef]
- Farinella, R.; Dorato, E. Ricerca-Intervento “Per Una Città Attiva E Amica Degli Anziani”; Laboratorio di Ricerca CITER—Dipartimento di Architettura dell’Università degli Studi di Ferrara, CFR Consorzio Futuro in Ricerca, ACER: Ferrara, Italy, 2022; Available online: https://www.acerferrara.it/media/uploads/allegati/125/estratto-ricerca-intervento-anziani.pdf (accessed on 15 February 2025).
- Elmose-Østerlund, K.; Dalgas, B.W.; Bredahl, T.V.G.; Lenze, L.; Høyer-Kruse, J.; Ibsen, B. Motives for leisure-time physical activity participation: An analysis of their prevalence, consistency and associations with activity type and social background. BMC Public Health 2023, 23, 2399. [Google Scholar] [CrossRef]
- Stojanovic, J.; Collamati, A.; Mariusz, D.; Onder, G.; La Milia, D.I.; Ricciardi, W. Decreasing loneliness and social isolation among the older people: Systematic search and narrative review. Epidemiol. Biostat. Public Health 2017, 14, e12408/1–e12408/8. [Google Scholar] [CrossRef]
- Feng, Z.; Cramm, J.M.; Jin, C.; Twisk, J.; Nieboer, A.P. The longitudinal relationship between income and social participation among Chinese older people. SSM Popul. Health 2020, 11, 100636. [Google Scholar] [CrossRef]
- Commins, P. Poverty and social exclusion in rural areas: Characteristics, processes and research issues. Sociol. Rural. 2004, 44, 60–75. [Google Scholar] [CrossRef]
- Walsh, K.; O’Shea, E.; Scharf, T. Social Exclusion and Ageing in Diverse Rural Communities; Irish Centre for Social Gerontology, National University of Ireland: Galway, Ireland, 2012; Available online: https://researchrepository.universityofgalway.ie/server/api/core/bitstreams/66cd8e02-9a5a-40c2-8c50-95e6a72ce31a/content (accessed on 2 March 2025).
- De Rossi, A. (Ed.) Riabitare l’Italia. In Aree Interne Tra Abbandoni e Riconquiste; Donzelli Editore: Roma, Italy, 2020. [Google Scholar]
- Richard, L.; Gauvin, L.; Gosselin, C.; Laforest, S. Staying connected: Neighbourhood correlates of social participation among older adults living in an urban environment in Montreal, Quebec. Health Promot. Int. 2009, 24, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Vogelsang, E.M. Older adult social participation and its relationship with health: Rural-urban differences. Health Place 2016, 42, 111–119. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Popolazione Italiana Residente al 1 Gennaio, 2025; ISTAT, Geodemo: Roma, Italy, 2024; Available online: https://demo.istat.it/app/?i=POS&l=it (accessed on 14 April 2025).
- EUROSTAT. Population Structure and Ageing; European Commission, Statistics Explained: Luxembourg, 2024; Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing (accessed on 2 February 2025).
- Midão, L.; Brochado, P.; Almada, M.; Duarte, M.; Paúl, C.; Costa, E. Frailty Status and Polypharmacy Predict All-Cause Mortality in Community Dwelling Older Adults in Europe. Int. J. Environ. Res. Public Health 2021, 18, 3580. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Rapporto Annuale 2022. La Situazione Del Paese; ISTAT: Roma, Italy, 2022; Available online: https://www.istat.it/storage/rapporto-annuale/2022/Rapporto_Annuale_2022.pdf (accessed on 8 January 2025).
- ISTAT. La Popolazione Anziana in Italia Tra Invecchiamento Demografico e Qualità Della Vita; ISTAT: Roma, Italy, 2022; Available online: https://www.istat.it/it/files/2022/09/53_ISTAT_MILeS2022_Sicuro_Tucci.pdf (accessed on 8 January 2025).
- EUROSTAT. Ageing Europe. Looking at the Lives of Older People in the EU.; European Commission: Luxembourg, 2020; Available online: https://ec.europa.eu/eurostat/web/products-statistical-books/-/KS-02-20-655 (accessed on 12 February 2025).
- ISTAT. Rapporto Annuale 2024. La Situazione Del Paese; ISTAT: Roma, Italy, 2024; Available online: https://www.istat.it/wp-content/uploads/2024/05/Rapporto-Annuale-2024.pdf (accessed on 12 February 2025).
- Molina, M.Á.; Cañadas-Reche, J.L.; Serrano-del-Rosal, R. Social Participation of the Elders in Europe: The Influence of Individual and Contextual Variables. Ageing Int. 2018, 43, 190–206. [Google Scholar] [CrossRef]
- ISTAT. Le Condizioni Di Salute Della Popolazione Anziana in Italia, Anno 2019; ISTAT, Statistiche Report: Roma, Italy, 2021; Available online: https://www.istat.it/it/files/2021/07/Report-anziani-2019.pdf (accessed on 8 March 2025).
- Melchiorre, M.G.; Quattrini, S.; Lamura, G.; Socci, M. A Mixed-Methods Analysis of Care Arrangements of Older People with Limited Physical Abilities Living Alone in Italy. Int. J. Environ. Res. Public Health 2021, 18, 12996. [Google Scholar] [CrossRef]
- Abramowska-Kmon, A.; Łatkowski, W.; Rynko, M. Informal Care and Subjective Well-Being among Older Adults in Selected European Countries. Ageing Int. 2023, 48, 1163–1189. [Google Scholar] [CrossRef]
- Marroni, C.; Corazza, L. L’Italia spopolata dei Comuni interni: Gli abitanti fuggono, restano gli over 80. Il Sole 24 Ore 2024, 76, 4–5. Available online: https://drive.google.com/drive/folders/1_xzOE2ROU-ZHixScgU0EIch3ZWBaB87n (accessed on 10 March 2025).
- OECD. OECD Regions and Cities at a Glance 2022; OECD Publishing: Paris, France, 2022; Available online: https://www.oecd.org/publications/oecd-regions-and-cities-at-a-glance-26173212.htm (accessed on 20 December 2024).
- Fina, S.; Heider, B.; Prota, F. Unequal Italy Regional Socio-Economic Disparities in Italy; Friedrich-Ebert-Stiftung, ILS: Roma, Italy, 2021; Available online: https://feps-europe.eu/wp-content/uploads/2021/07/Unequal-Italy-Regional-socio-economic-disparities-in-Italy.pdf (accessed on 18 May 2025).
- Bertin, G.; Pantalone, M. Comparing hybrid welfare systems: The differentiation of health and social care policies at the regional level in Italy. Ital. Sociol. Rev. 2018, 8, 1–23. [Google Scholar] [CrossRef]
- Bertin, G.; Carradore, M. Differentiation of welfare regimes: The case of Italy. Int. J. Soc. Welf. 2016, 25, 149–160. [Google Scholar] [CrossRef]
- NNA—Network non Autosufficienza. L’Assistenza Agli Anziani non Autosufficienti in Italia. 7° Rapporto 2020/2021. Punto di non Ritorno; Maggioli Editore: Santarcangelo di Romagna, Italy, 2020; Available online: http://www.irisonline.it/web/images/7dicembre2020/nna_2020_7%B0_rapporto.pdf (accessed on 18 May 2025).
- ISTAT. La Spesa dei Comuni per i Servizi Sociali. Anno 2021; ISTAT, Statistiche Report: Roma, Italy, 2024; Available online: https://www.istat.it/wp-content/uploads/2024/06/REPORT_SPESA-SOCIALE-COMUNI.pdf (accessed on 18 May 2025).
- De Vincenti, C. Relazione Annuale Sulla Strategia Nazionale Per Le Aree Interne; Ministro per la Coesione Territoriale e il Mezzogiorno: Roma, Italy, 2018. Available online: https://www.agenziacoesione.gov.it/wp-content/uploads/2020/07/Relazione_CIPE_2018.pdf (accessed on 20 December 2024).
- Ritchie, J.; Lewis, J. (Eds.) Qualitative Research Practice. A Guide for Social Science Students and Researchers; Sage Publications: London, UK, 2003. [Google Scholar]
- Bunt, S.; Steverink, N.; Olthof, J.; van der Schans, C.P.; Hobbelen, J.S.M. Social frailty in older adults: A scoping review. Eur. J. Ageing 2017, 14, 323–334. [Google Scholar] [CrossRef]
- Cardoso, A.F.; Bobrowicz-Campos, E.; Teixeira-Santos, L.; Cardoso, D.; Couto, F.; Apóstolo, J. Validation and Screening Capacity of the European Portuguese Version of the SUNFRAIL Tool for Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 1394. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K. Frailty and its definition: A worthy challenge. J. Am. Geriatr. Soc. 2005, 53, 1069–1070. [Google Scholar] [CrossRef] [PubMed]
- Lamura, G.; Dohner, H.; Kofhal, C. (Eds.) Supporting Family Carers of Older People in Europe—Empirical Evidence, Policy Trends and Future Perspectives; Lit Verlag: Hamburg, Germany, 2008. [Google Scholar]
- ISTAT. Indagine Statistica Multiscopo Sulle Famiglie; ISTAT, Scheda di rilevazione: Roma, Italy, 2011; Available online: https://www.istat.it/it/files//2011/01/Arancio_Mod_IMF_8A.pdf (accessed on 10 January 2025).
- ISTAT. Conoscere il Mondo Della Disabilità: Persone, Relazioni e Istituzioni; ISTAT, Letture Statistiche, Temi: Roma, Italy, 2019; Available online: https://www.istat.it/wp-content/uploads/2019/12/Disabilita.pdf (accessed on 10 January 2025).
- Chistell, F.; Stängle, S.; Fringer, A. “Loneliness is a monotonous thing”: Descriptive qualitative research on the loneliness of caring relatives. BMC Nurs. 2023, 22, 161. [Google Scholar] [CrossRef]
- Galenkamp, H.; Gagliardi, C.; Principi, A.; Golinowska, S.; Moreira, A.; Schmidt, A.E.; Winkelmann, J.; Sowa, A.; van der Pas, S.; Deeg, D.J.H. Predictors of social leisure activities in older Europeans with and without multimorbidity. Eur. J. Ageing 2016, 13, 129–143. [Google Scholar] [CrossRef]
- Hulteen, R.M.; Smith, J.J.; Morgan, P.J.; Barnett, L.M.; Hallal, P.C.; Colyvas, K.; Lubans, D.R. Global participation in sport and leisure-time physical activities: A systematic review and meta-analysis. Prev. Med. 2017, 95, 14–25. [Google Scholar] [CrossRef]
- Van Groenou, M.B.; Deeg, D.J. Formal and informal social participation of the’young-old’in the Netherlands in 1992 and 2002. Ageing Soc. 2010, 30, 445–465. [Google Scholar] [CrossRef]
- Ekman, J.; Amnå, E. Political participation and civic engagement: Towards a new typology. Hum. Aff. 2012, 22, 283–300. [Google Scholar] [CrossRef]
- ISTAT. Indagine “Inclusione Sociale Delle Persone Con Limitazioni Funzionali”. Anno 2011; ISTAT, Nota metodologica: Roma, Italy, 2011; Available online: https://www.istat.it/it/files//2012/12/Nota-metodologica.pdf (accessed on 7 January 2025).
- William, F.K.A. Interpretivism or Constructivism: Navigating Research Paradigms in Social Science Research. Int. J. Res. Publ. 2024, 143, 134–138. [Google Scholar] [CrossRef]
- Srivastava, A.; Thomson, S.B. Framework Analysis: A Qualitative Methodology for Applied Policy Research. JOAAG 2009, 4, 72–79. Available online: http://research.apc.org/images/a/ad/Framework_analysis.pdf (accessed on 20 January 2025).
- Ritchie, J.; Spencer, L. Qualitative data analysis for applied policy research. In Analyzing Qualitative Data; Bryman, A., Burgess, R.G., Eds.; Routledge: London, UK, 1994; pp. 173–194. [Google Scholar]
- Vaismoradi, M.; Turunen, H.; Bondas, T. Content Analysis and Thematic Analysis: Implications for Conducting a Qualitative Descriptive Study. Nurs. Health Sci. 2013, 15, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Saldana, J. The Coding Manual for Qualitative Researchers; Sage Publications: London, UK, 2009. [Google Scholar]
- Weitzman, E.A. Software and qualitative research. In Handbook of Qualitative Research, 2nd ed.; Denzin, N.K., Lincoln, Y.S., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2000; pp. 803–820. [Google Scholar]
- Smith, J.; Firth, J. Qualitative Data Analysis: The Framework Approach. Nurs. Res. 2011, 18, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Arlotti, M.; Cerea, S. Invecchiare a Domicilio Nei Contesti Urbani e Nelle Aree Interne. Fragilità, Isolamento Sociale e Senso di Solitudine. DAStU Work. Pap. Ser. 2021, 4, LPS.18. Available online: http://www.lps.polimi.it/wp-content/uploads/2021/05/DAStU_WP_no.418.pdf (accessed on 20 March 2025).
- Smith, K.; Victor, C. Typologies of loneliness, living alone and social isolation, and their associations with physical and mental health. Ageing Soc. 2019, 39, 1709–1730. [Google Scholar] [CrossRef]
- ISTAT. Cambiamenti Nei Tempi di Vita e Attività del Tempo Libero; Statistiche Report; ISTAT: Roma, Italy, 2011; Available online: https://www.istat.it/wp-content/uploads/2011/12/testo-uso-del-tempo2008-2009.pdf (accessed on 16 January 2025).
- ISTAT. I Tempi Della Vita Quotidiana. Lavoro, Conciliazione, Parità di Genere e Benessere Soggettivo; ISTAT: Roma, Italy, 2019; Available online: https://www.istat.it/it/files/2019/05/ebook-I-tempi-della-vita-quotidiana.pdf (accessed on 16 January 2025).
- Goodarzi, S.; Jiang, J.; Head, M.; Lu, X. Exploring the impact of online social participation on loneliness in older adults: Evidence from The Canadian Longitudinal Study on Aging. Int. J. Inf. Manag. 2023, 73, 102685. [Google Scholar] [CrossRef]
- van Hees, S.G.M.; van den Borne, B.H.P.; Menting, J.; Sattoe, J.N.T. Patterns of social participation among older adults with disabilities and the relationship with well-being: A latent class analysis. Arch. Gerontol. Geriatr. 2020, 86, 103933. [Google Scholar] [CrossRef]
- Seifert, A.; Rössel, J. Digital Participation. In Encyclopedia of Gerontology and Population Aging; Gu, D., Dupre, M., Eds.; Springer: Cham, Switzerland, 2019; pp. 1–5. [Google Scholar]
- Morse, J.M. Principles of mixed methods and multimethod research design. In Handbook of Mixed Methods in Social and Behavioral Research; Tashakkori, A., Teddlie, C., Eds.; Sage Publications: Thousand Oaks, CA, USA, 2003; pp. 189–208. [Google Scholar]
- Corden, A.; Sainsbury, R. Using Verbatim Quotations in Reporting Qualitative Social Research: Researchers’ Views; The Social Policy Research Unit, University of York: York, UK, 2006; Available online: https://www.york.ac.uk/inst/spru/pubs/pdf/verbquotresearch.pdf (accessed on 14 December 2024).
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage Publications: Beverly Hills, CA, USA, 1985. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. La sorveglianza Passi d’Argento. I Dati per l’Italia. La Partecipazione Sociale Negli Ultra 65enni; EpiCentro: Roma, Italy, 2023; Available online: https://www.epicentro.iss.it/passi-argento/dati/partecipazione (accessed on 4 January 2025).
- Baeriswyl, M.; Oris, M. Social participation and life satisfaction among older adults: Diversity of practices and social inequality in Switzerland. Ageing Soc. 2021, 43, 1259–1283. [Google Scholar] [CrossRef]
- Björnwall, A.; Mattsson Sydner, Y.; Koochek, A.; Neuman, N. Eating Alone or Together among Community-Living Older People—A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 3495. [Google Scholar] [CrossRef]
- Liu, Y. The relationship and heterogeneity of family participation and social participation among older adults: From an intersectionality perspective. BMC Geriatr. 2024, 24, 949. [Google Scholar] [CrossRef]
- Anzai, S.; Ohsugi, H.; Shiba, Y. Factors associated with social participation among community-dwelling frail older adults in Japan: A cross-sectional study. BMC Geriatr. 2024, 24, 235. [Google Scholar] [CrossRef] [PubMed]
- Letak, A.M. The Promise of Sociology of Television: Investigating the Potential of Phenomenological Approaches. Sociol. Forum 2022, 37, 581–602. [Google Scholar] [CrossRef]
- Löfgren, M.; Larsson, E.; Isaksson, G.; Nyman, A. Older adults’ experiences of maintaining social participation: Creating opportunities and striving to adapt to changing situations. Scand. J. Occup. Ther. 2022, 29, 587–597. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Tempo Libero e Partecipazione Culturale: Tra Vecchie e Nuove Pratiche; ISTAT, Statistiche Report: Roma, Italy, 2022; Available online: https://www.istat.it/wp-content/uploads/2022/09/Tempo-libero-e-partecipazione-culturale_Ebook.pdf (accessed on 10 March 2025).
- Malone, J.; Dadswell, A. The Role of Religion, Spirituality and/or Belief in Positive Ageing for Older Adults. Geriatrics 2018, 3, 28. [Google Scholar] [CrossRef]
- McManus, D. The Intersection of Spirituality, Religiosity, and Lifestyle Practices in Religious Communities to Successful Aging: A Review Article. Religions 2024, 15, 478. [Google Scholar] [CrossRef]
- Carrick, R.M.; Wadsworth, D. The older adult: Physical activity considerations and learning to age in place. Work. Older People 2024, 28, 336–344. [Google Scholar] [CrossRef]
- Bertolini, P.; Pagliacci, F. Quality of Life and Territorial Imbalances. A Focus on Italian Inner and Rural Areas. Bio-Based Appl. Econ. 2017, 6, 183–208. [Google Scholar] [CrossRef]
- Basile, G.; Cavallo, A. Rural Identity, Authenticity, and Sustainability in Italian Inner Areas. Sustainability 2020, 12, 1272. [Google Scholar] [CrossRef]
- Viganó, F.; Grossi, E.; Tavano Blessi, G. Urban-Rural dwellers’ well-being determinants: When the city size matters. The case of Italy. City Cult. Soc. 2019, 19, 100293. [Google Scholar] [CrossRef]
- Larsson Ranada, Å.; Österholm, J. Promoting Active and Healthy Ageing at Day Centers for Older People. Act. Adapt. Aging 2022, 46, 236–250. [Google Scholar] [CrossRef]
- Nyqvist, F.; Serrat, R.; Nygård, M.; Näsman, M. Does social capital enhance political participation in older adults? Multi-level evidence from the European Quality of Life Survey. Eur. J. Ageing 2024, 21, 30. [Google Scholar] [CrossRef] [PubMed]
- Utz, R.L.; Carr, D.; Nesse, R.; Wortman, C.B. The effect of widowhood on older adults’ social participation: An evaluation of activity, disengagement, and continuity theories. Gerontologist 2002, 42, 522–533. [Google Scholar] [CrossRef] [PubMed]
- Arlotti, M. Older people and care networks in rural areas: An exploratory study in Italy. Sociol. Rural. 2024, 64, 376–396. [Google Scholar] [CrossRef]
- Sarlo, A.; Martinelli, F. Time and space in the care of older people: Ageing in place and the built environment. Arch. Studi Urbani Reg. 2023, 136, 147–171. [Google Scholar] [CrossRef]
- Melchiorre, M.G.; D’Amen, B.; Quattrini, S.; Lamura, G.; Socci, M. Health Emergencies, Falls, and Use of Communication Technologies by Older People with Functional and Social Frailty: Ageing in Place in Deprived Areas of Italy. Int. J. Environ. Res. Public Health 2022, 19, 14775. [Google Scholar] [CrossRef]
- Amodio, T. Territories at risk of abandonment in Italy and hypothesis of repopulation. Belgeo 2022, 4, 1–23. [Google Scholar] [CrossRef]
- Levasseur, M.; Cohen, A.A.; Dubois, M.F.; Généreux, M.; Richard, L.; Therrien, F.H.; Payette, H. Environmental Factors Associated with Social Participation of Older Adults Living in Metropolitan, Urban, and Rural Areas: The NuAge Study. Am. J. Public Health 2015, 105, 1718–1725. [Google Scholar] [CrossRef]
- Shrestha, B.P.; Millonig, A.; Hounsell, N.B.; McDonald, M. Review of Public Transport Needs of Older People in European Context. J. Popul. Ageing 2017, 10, 343–361. [Google Scholar] [CrossRef]
- Levasseur, M.; Routhier, S.; Clapperton, I.; Doré, C.; Gallagher, F. Social participation needs of older adults living in a rural regional county municipality: Toward reducing situations of isolation and vulnerability. BMC Geriatr. 2020, 20, 456. [Google Scholar] [CrossRef]
- Corcoran, R.; Marshall, G. From lonely cities to prosocial places: How evidence-informed urban design can reduce the experience of loneliness. In Narratives of Loneliness; Sagan, O., Miller, E., Eds.; Routledge: London, UK, 2017; pp. 127–139. [Google Scholar]
- Herbers, D.J.; Mulder, C.H. Housing and subjective well-being of older adults in Europe. J. Hous. Built Environ. 2017, 32, 533–558. [Google Scholar] [CrossRef]
- ISTAT. I Tempi Della Vita Quotidiana. Anno 2014; Statistiche Report; ISTAT: Roma, Italy, 2016; Available online: https://www.istat.it/wp-content/uploads/2016/11/Report_Tempidivita_2014.pdf (accessed on 5 March 2025).
- Ghenta, M.; Bobarnat, E.S. Engagement of older persons in cultural activities: Importance and barriers. J. Econ. Dev. Environ. People 2019, 8, 6–12. [Google Scholar] [CrossRef]
- Pöllänen, S. The meaning of craft: Craft makers’ descriptions of craft as an occupation. Scand. J. Occup. Ther. 2013, 20, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Chacur, K.; Serrat, R.; Villar, F. Older adults’ participation in artistic activities: A scoping review. Eur. J. Ageing 2022, 19, 931–944. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, A.; Fraser, S.; Wittich, W. Barriers and Facilitators That Influence Social Participation in Older Adults with Dual Sensory Impairment. Front. Educ. 2020, 5, 127. [Google Scholar] [CrossRef]
- EUROSTAT. Tourism Trends and Ageing; European Commission, Statistics Explained: Luxembourg, 2024; Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Tourism_trends_and_ageing (accessed on 2 February 2025).
- Singh, B.; Kirans, U.V. Recreational Activities for Senior Citizens. J. Humanit. Soc. Sci. 2014, 19, 24–30. [Google Scholar] [CrossRef]
- Lattman, K.; Olsson, L.E.; Waygood, E.O.D.; Friman, M. Nowhere to go—Effects on elderly’s travel during Covid-19. Travel Behav. Soc. 2023, 32, 100574. [Google Scholar] [CrossRef]
- Kim, J.; Park, G.R.; Namkung, E.H. The link between disability and social participation revisited: Heterogeneity by type of social participation and by socioeconomic status. Disabil. Health J. 2024, 17, 101543. [Google Scholar] [CrossRef]
- Zhao, L.; Wu, L. The Association between Social Participation and Loneliness of the Chinese Older Adults over Time-The Mediating Effect of Social Support. Int. J. Environ. Res. Public Health 2022, 19, 815. [Google Scholar] [CrossRef]
- Pettigrew, S. Reducing the experience of loneliness among older consumers. J. Res. Consum. 2007, 12, 1–4. Available online: https://www.jrconsumers.com/Consumer_Articles/issue_12/loneliness_consumer.pdf (accessed on 2 March 2025).
- Stenner, B.J.; Buckley, J.D.; Mosewich, A.D. Reasons why older adults play sport: A systematic review. J. Sport Health Sci. 2020, 9, 530–541. [Google Scholar] [CrossRef]
- Sarlo, A.; Bagnato, F.; Martinelli, F. Ageing in place and the built environment. Implications for the quality of life and the risks of isolation of frail older people. DAStU Work. Pap. Ser. 2019, 4, LPS.06. Available online: https://www.lps.polimi.it/wp-content/uploads/2019/12/DAStU_LPS_WP06-2019.pdf (accessed on 18 March 2025).
- Victor, C.; Scambler, S.; Bond, J.; Bowling, A. Being alone in later life: Loneliness, social isolation and living alone. Rev. Clin. Gerontol. 2000, 10, 407–417. [Google Scholar] [CrossRef]
- Malli, M.A.; Ryan, S.; Maddison, J.; Kharicha, K. Experiences and meaning of loneliness beyond age and group identity. Sociol. Health Illn. 2023, 45, 70–89. [Google Scholar] [CrossRef] [PubMed]
- Grenade, L.; Boldy, D. Social isolation and loneliness among older people: Issues and future challenges in community and residential settings. Aust. Health Rev. 2008, 32, 468–478. [Google Scholar] [CrossRef]
- De Jong Gierveld, J.; Van Tilburg, T. A 6-Item scale for overall, emotional, and social loneliness: Confirmatory tests on survey data. Res. Aging 2006, 28, 582–598. [Google Scholar] [CrossRef]
- Shutter, N.; Koorevaar, L.; Holwerda, T.J.; Stek, M.L.; Dekker, J.; Comijs, H.C. ‘Big Five’ personality characteristics are associated with loneliness but not with social network size in older adults, irrespective of depression. Int. Psychogeriatr. 2019, 32, 53–63. [Google Scholar] [CrossRef]
- ISTAT. Rapporto Annuale 2018. La Situazione del Paese; Statistiche Report; ISTAT: Roma, Italy, 2018; Available online: https://www.istat.it/storage/rapporto-annuale/2018/Rapportoannuale2018.pdf (accessed on 10 March 2025).
- Ang, S. The Social Circles Framework—A New Theoretical Framework for Mapping the Domains of Loneliness and Social Connectedness. Acad. Lett. 2021, 2496, 1–7. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Reinwarth, A.C.; Ernst, M.; Krakau, L.; Brähler, E.; Beutel, M.E. Screening for loneliness in representative population samples: Validation of a single-item measure. PLoS ONE 2023, 18, e0279701. [Google Scholar] [CrossRef]
- Gardiner, C.; Geldenhuys, G.; Gott, M. Interventions to reduce social isolation and loneliness among older people: An integrative review. Health Soc. Care Community 2018, 26, 147–157. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Richardson, E.A.; Tunstall, H.; Shortt, N.K.; Mitchell, R.J.; Pearce, J.R. The relationship between wealth and loneliness among older people across Europe: Is social participation protective? Prev. Med. 2016, 91, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Orellana, K.; Manthorpe, J.; Tinker, A. Day centres for older people: A systematically conducted scoping review of the literature about their benefits, purpose and how they are perceived. Ageing Soc. 2020, 40, 73–104. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Indagine Sugli Interventi e i Servizi Sociali dei Comuni. Dataset 2022; ISTAT, I.Stat: Roma, Italy, 2025; Available online: http://dati.istat.it/Index.aspx?QueryId=23474# (accessed on 2 March 2025).
- Barbabella, F.; Cela, E.; Socci, M.; Lucantoni, D.; Zannella, M.; Principi, A. Active Ageing in Italy: A Systematic Review of National and Regional Policies. Int. J. Environ. Res. Public Health 2022, 19, 600. [Google Scholar] [CrossRef] [PubMed]
- UNECE. Older Persons in Vulnerable Situations. Policy Brief on Ageing; United Nations, Standing Working Group on Ageing: Geneva, Switzerland, 2023; Available online: https://unece.org/sites/default/files/2023-06/ECE-WG.1-42-PB28.pdf (accessed on 2 March 2025).
- WHO. The Global Network for Age-Friendly Cities and Communities; WHO: Geneva, Switzerland, 2018; Available online: https://www.jcafc.hk/uploads/docs/The-Global-Network-for-Age-friendly-Cities-and-Communities-Looking-back-over-the-last-decade-looking-forward-to-the-next-1.pdf (accessed on 22 November 2024).
- Bergefurt, L.; Kemperman, A.; van den Berg, P.; Borgers, A.; van derWaerden, P.; Oosterhuis, G.; Hommel, M. Loneliness and Life Satisfaction Explained by Public-Space Use and Mobility Patterns. Int. J. Environ. Res. Public Health 2019, 16, 4282. [Google Scholar] [CrossRef]
- Ricciardi, E.; Spano, G.; Tinella, L.; Lopez, A.; Clemente, C.; Bosco, A.; Caffò, A.O. Perceived Social Support Mediates the Relationship between Use of Greenspace and Geriatric Depression: A Cross-Sectional Study in a Sample of South-Italian Older Adults. Int. J. Environ. Res. Public Health 2023, 20, 5540. [Google Scholar] [CrossRef]
- Barbabella, F.; Poli, A.; Chiatti, C.; Pelliccia, L.; Pesaresi, F. La bussola di NNA: Lo stato dell’arte basato sui dati. In L’Assistenza Agli Anziani non Autosufficienti in Italia, 6° Rapporto 2017/2018, Il Tempo Delle Risposte; Network Non Autosufficienza (NNA), Ed.; Maggioli Editore: Santarcangelo di Romagna, Italy, 2017; pp. 33–54. Available online: https://www.luoghicura.it/wp-content/uploads/2017/12/NNA_2017_6%C2%B0_Rapporto.pdf (accessed on 15 February 2025).
- Martinelli, F. I divari Nord-Sud nei servizi sociali in Italia. Un regime di cittadinanza differenziato e un freno allo sviluppo del Paese. Riv. Econ. Mezzog. 2019, 33, 41–79. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Macro-Categories | Sub-Categories |
|---|---|
| Social/religious 1 |
|
| |
| |
| |
| |
| |
| Cultural |
|
| |
| |
| |
| |
| Political |
|
| |
| Sports/physical exercises |
|
| |
| |
| Recreational |
|
| |
| Productive–artistic 2 |
|
| |
| |
| Travelling |
|
| |
| Watching television (TV) 3 | - |
| Characteristics | Urban Site | Rural Sites | Marche Region | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Age groups (years) | ||||||
| 65–79 | 7 | 29 | 3 | 19 | 10 | 25 |
| 80 and over | 17 | 71 | 13 | 81 | 30 | 75 |
| Gender | ||||||
| Male | 5 | 21 | 3 | 19 | 8 | 20 |
| Female | 19 | 79 | 13 | 81 | 32 | 80 |
| Education | ||||||
| No title | 2 | 8 | 7 | 44 | 9 | 23 |
| Primary/middle school (5 and 3 years) | 17 | 71 | 7 | 44 | 24 | 60 |
| High School/university (3–5 years both) | 5 | 21 | 2 | 12 | 7 | 17 |
| Marital status | ||||||
| Single | 2 | 8 | 3 | 19 | 5 | 12 |
| Divorced/separated | 3 | 13 | - | - | 3 | 8 |
| Widowed | 19 | 79 | 13 | 81 | 32 | 80 |
| Living situation | ||||||
| Alone | 21 | 88 | 11 | 69 | 32 | 80 |
| With personal/private care assistant (PCA) 1 | 3 | 12 | 5 | 31 | 8 | 20 |
| Level of functional limitations 2 | ||||||
| Mild/Moderate | 12 | 50 | 12 | 75 | 24 | 60 |
| High/Very high | 12 | 50 | 4 | 25 | 16 | 40 |
| Main source of support 3 | ||||||
| Family | 19 | 79 | 14 | 88 | 33 | 83 |
| Public services 4 | 15 | 63 | 8 | 50 | 23 | 58 |
| Private services 5 | 14 | 58 | 4 | 25 | 18 | 45 |
| Total cases/respondents | 24 | 100 | 16 | 100 | 40 | 100 |
| Social–Leisure Activities 1 | Urban Site | Rural Sites | Marche Region | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Receiving/making visits | 14 | 58 | 15 | 94 | 29 | 73 |
| Lunches/dinners | 12 | 50 | 9 | 56 | 21 | 53 |
| Social clubs | 6 | 25 | 4 | 25 | 10 | 25 |
| Parties, festivals | - | - | 3 | 19 | 3 | 8 |
| Unpaid volunteering | 2 | 8 | 3 | 19 | 5 | 13 |
| Religious functions | 9 | 38 | 11 | 69 | 20 | 50 |
| Shows, music concerts, cinema, theatres, museums, conferences | 1 | 4 | 4 | 25 | 5 | 13 |
| Reading books/magazines/newspapers, UNI-3 2 | 3 | 13 | 3 | 19 | 6 | 15 |
| Political parties, Trade unions | - | - | - | - | - | - |
| Gymnastics, running, dancing | 2 | 8 | - | - | 2 | 5 |
| Walking | 6 | 25 | 12 | 75 | 18 | 45 |
| Playing cards, chess, crosswords, sudoku | 5 | 21 | 3 | 19 | 8 | 20 |
| Hobbies, crafts, vegetable garden/garden, raising poultry 3 | 2 | 8 | 4 | 25 | 6 | 15 |
| Voyages, cruises | 1 | 4 | 1 | 6 | 2 | 5 |
| Watching TV | 10 | 42 | 15 | 94 | 25 | 63 |
| Other 4 | 2 | 8 | 1 | 6 | 3 | 8 |
| Total cases/respondents | 24 | 100 | 16 | 100 | 40 | 100 |
| Frequency of Social–Leisure Activities 1 | Urban Site | Rural Sites | Marche Region | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Weekly 2 | 15 | 63 | 16 | 100 | 31 | 78 |
| Monthly 3 | 5 | 21 | 8 | 50 | 13 | 33 |
| Less often 4 | 13 | 54 | 11 | 69 | 24 | 60 |
| Total cases/respondents | 24 | 100 | 16 | 100 | 40 | 100 |
| Social–Leisure Activities 2 | Urban Site | Rural Sites | Marche Region | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Receiving/making visits | 1 | 4 | 1 | 6 | 2 | 5 |
| Lunches/dinners | 2 | 8 | - | - | 2 | 5 |
| Social clubs | - | - | 1 | 6 | 1 | 3 |
| Parties, festivals | - | - | 2 | 13 | 2 | 5 |
| Unpaid volunteering | 2 | 8 | 3 | 19 | 5 | 13 |
| Religious functions | 4 | 17 | 3 | 19 | 7 | 18 |
| Shows, music concerts, cinema, theatres, museums, conferences | - | - | 4 | 25 | 4 | 10 |
| Reading books/magazines/newspapers, UNI-3 3 | - | - | - | - | - | - |
| Political parties, Trade unions | 1 | 4 | 2 | 13 | 3 | 8 |
| Gymnastics, running, dancing | - | - | 3 | 19 | 3 | 8 |
| Walking | 3 | 13 | 4 | 25 | 7 | 18 |
| Playing cards, chess, crosswords, sudoku | 1 | 4 | 4 | 25 | 5 | 13 |
| Hobbies, crafts, vegetable garden/garden, raising poultry | - | - | 1 | 6 | 1 | 3 |
| Voyages, cruises | 1 | 4 | 1 | 6 | 2 | 5 |
| Watching TV | - | - | - | - | - | - |
| Total cases/respondents | 24 | 100 | 16 | 100 | 40 | 100 |
| Macro-Categories of Social–Leisure Activities 1 | Urban Site | Rural Sites | Marche Region | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Social/religious 2 | 19 | 79 | 16 | 100 | 35 | 88 |
| Cultural | 4 | 17 | 5 | 31 | 9 | 23 |
| Political | - | - | - | - | - | - |
| Sports/physical exercises | 7 | 29 | 12 | 75 | 19 | 48 |
| Recreational | 5 | 21 | 3 | 19 | 8 | 20 |
| Productive–artistic 3 | 1 | 4 | 4 | 25 | 5 | 13 |
| Travelling | 1 | 4 | 1 | 6 | 2 | 5 |
| Watching TV | 10 | 42 | 15 | 94 | 25 | 63 |
| Total cases/respondents | 24 | 100 | 16 | 100 | 40 | 100 |
| Macro-Categories of Social–Leisure Activities 1 | Level of Functional Limitations | |||
|---|---|---|---|---|
| Mild/Moderate | High/Very High | |||
| n | % | n | % | |
| Social/religious 2 | 22 | 92 | 13 | 81 |
| Cultural | 6 | 25 | 3 | 19 |
| Political | - | - | - | - |
| Sports/physical exercises | 11 | 46 | 8 | 50 |
| Recreational | 4 | 17 | 4 | 25 |
| Productive–artistic 3 | 5 | 21 | - | - |
| Travelling | 2 | 8 | - | - |
| Watching TV | 16 | 67 | 9 | 56 |
| Total cases/respondents | 24 | 100 | 16 | 100 |
| Macro-Categories of Social–Leisure Activities 1 | Level of Functional Limitations | |||
|---|---|---|---|---|
| Mild/Moderate | High/Very High | |||
| n | % | n | % | |
| Social/religious 2 | 10 | 83 | 9 | 75 |
| Cultural | 3 | 25 | 1 | 8 |
| Political | - | - | - | - |
| Sports/physical exercises | 1 | 8 | 6 | 50 |
| Recreational | 3 | 25 | 2 | 17 |
| Productive–artistic 3 | 1 | 8 | - | - |
| Travelling | 1 | 8 | - | - |
| Watching TV | 5 | 42 | 5 | 42 |
| Total cases/respondents | 12 | 100 | 12 | 100 |
| Macro-Categories of Social–Leisure Activities 1 | Level of Functional Limitations | |||
|---|---|---|---|---|
| Mild/Moderate | High/Very High | |||
| n | % | n | % | |
| Social/religious 2 | 12 | 100 | 4 | 100 |
| Cultural | 3 | 25 | 2 | 50 |
| Political | - | - | - | - |
| Sports/physical exercises | 10 | 83 | 2 | 50 |
| Recreational | 1 | 8 | 2 | 50 |
| Productive–artistic | 4 | 33 | - | - |
| Travelling | 1 | 8 | - | - |
| Watching TV | 11 | 92 | 4 | 100 |
| Total cases/respondents | 12 | 100 | 4 | 100 |
| Macro-Categories of Social–Leisure Activities 1 | Loneliness | |||
|---|---|---|---|---|
| Absent/Mild-Moderate | High/Very High | |||
| n | % | n | % | |
| Social/religious 2 | 19 | 86 | 16 | 89 |
| Cultural | 5 | 23 | 4 | 22 |
| Political | - | - | - | - |
| Sports/physical exercises | 10 | 45 | 9 | 50 |
| Recreational | 5 | 23 | 3 | 17 |
| Productive–artistic 3 | 2 | 9 | 3 | 17 |
| Travelling | 2 | 9 | - | - |
| Watching TV | 15 | 68 | 10 | 56 |
| Total cases/respondents | 22 | 100 | 18 | 100 |
| Macro-Categories of Social–Leisure Activities 1 | Loneliness | |||
|---|---|---|---|---|
| Absent/Mild-Moderate | High/Very High | |||
| n | % | n | % | |
| Social/religious 2 | 13 | 81 | 6 | 75 |
| Cultural | 4 | 25 | - | - |
| Political | - | - | - | - |
| Sports/physical exercises | 5 | 31 | 2 | 25 |
| Recreational | 4 | 25 | 1 | 13 |
| Productive–artistic 3 | - | - | 1 | 13 |
| Travelling | 1 | 6 | - | - |
| Watching TV | 9 | 56 | 1 | 13 |
| Total cases/respondents | 16 | 100 | 8 | 100 |
| Macro-Categories of Social–Leisure Activities 1 | Loneliness | |||
|---|---|---|---|---|
| Absent/Mild-Moderate | High/Very High | |||
| n | % | n | % | |
| Social/religious 2 | 6 | 100 | 10 | 100 |
| Cultural | 1 | 17 | 4 | 40 |
| Political | - | - | - | - |
| Sports/physical exercises | 5 | 83 | 7 | 70 |
| Recreational | 1 | 17 | 2 | 20 |
| Productive–artistic | 2 | 33 | 2 | 20 |
| Travelling | 1 | 17 | - | - |
| Watching TV | 6 | 100 | 9 | 90 |
| Total cases/respondents | 6 | 100 | 10 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melchiorre, M.G.; Socci, M.; Lamura, G.; Quattrini, S. Social Participation of Frail Older People with Functional Limitations Ageing Alone in Place in Italy, and Its Impact on Loneliness: An Urban–Rural Comparison. Urban Sci. 2025, 9, 233. https://doi.org/10.3390/urbansci9060233
Melchiorre MG, Socci M, Lamura G, Quattrini S. Social Participation of Frail Older People with Functional Limitations Ageing Alone in Place in Italy, and Its Impact on Loneliness: An Urban–Rural Comparison. Urban Science. 2025; 9(6):233. https://doi.org/10.3390/urbansci9060233
Chicago/Turabian StyleMelchiorre, Maria Gabriella, Marco Socci, Giovanni Lamura, and Sabrina Quattrini. 2025. "Social Participation of Frail Older People with Functional Limitations Ageing Alone in Place in Italy, and Its Impact on Loneliness: An Urban–Rural Comparison" Urban Science 9, no. 6: 233. https://doi.org/10.3390/urbansci9060233
APA StyleMelchiorre, M. G., Socci, M., Lamura, G., & Quattrini, S. (2025). Social Participation of Frail Older People with Functional Limitations Ageing Alone in Place in Italy, and Its Impact on Loneliness: An Urban–Rural Comparison. Urban Science, 9(6), 233. https://doi.org/10.3390/urbansci9060233