Abstract
The COVID-19 pandemic is a severe ongoing health crisisworldwide. Studying the socio-economic impacts of COVID-19 can help policymakers develop successful pandemic management plans. This paper focuses on the spatial epidemiology of COVID-19 among different social classes in the Kermanshah metropolis, Iran. This cross-sectional study uses the data of people infected with COVID-19 in the Kermanshah metropolis in 2020, acquired from the official COVID-19 Registry of Kermanshah. The results show that 2013 people were infected with COVID-19 (male = 1164 and female = 849). The mean age of the patients was 45 ± 18.69. The Moran’s I show that COVID-19 in different social classes was clustered across the neighbourhoods in the Kermanshah metropolis. The mean ages of men and women were 44.51 ± 18.62 and 45.69 ± 18.76, respectively. Importantly, COVID-19 was highly prevalent in the middle-class groups. Age group comparisons indicate that older people were the most infected in poorer neighbourhoods. In the middle-classtheage group of 0–14 years and in the rich neighbourhoods the age group of 15–64 years were the most exposed to the disease. The findings of this study suggest that older people and lower socioeconomic classes should be prioritised while developing and implementing preventative programs for COVID-19 and similar pandemics.
1. Introduction
The COVID-19 is one of the world’s worst health crises in recent years, affecting 210 countries and territories. Iran is among the top ten countries with the highest number of infected cases. The pandemic started in Iran on 19 February 2020, when two cases were confirmed in the central Iranian city of Qom. Qom is a pilgrim city and hosts millions of pilgrims from other parts of Iran and the rest of the world. Within 15 days of the first two cases in Qom, the disease swept through all of Iran’s provinces. By the end of June 2020, Iran experienced two waves of COVID-19, reporting 160,696 cases and 8012 deaths [1]. Iran’s already strained health system has been under enormous pressure due to COVID-19 [2].
Since COVID-19 is a new phenomenon, all people are susceptible to infection, although it is undeniable that biological and epidemiological factors contribute to the rapid spread of the disease. However, as with other health conditions, socioeconomic status can have a significant impact on the spread and incidence of the disease [3].
A large body of researchhas analysed the short-term and long-term economic impacts of COVID-19 [4,5,6]. The findings of the studies suggest that the pandemic has had serious negative impacts on households [7] as well as regional [8] and global [9] economies. Additionally, policymakers around the world have been initiating large-scale interventions and policies to address and manage the economic outcomes of COVID-19.
However, there is a considerably small number of studies focusing on the socioeconomic impacts of COVID 19 across social classes [10]. Focusing only on the economic dimension represents a limitation of the current state of research on COVID-19 [11]. A social perspective is important as socioeconomically marginalised groups have poor health outcomes due to educational barriers, lack of access to medical centres, poor quality of life, and pre-existing inequalities in communities [12,13,14,15]. The impacts of COVID-19 surely encompass economic, social, and cultural risks.
A study from South Korea shows that all people (more in the elderly age group of ≥60 years) in lower socioeconomic classes are at high risk of infecting with COVID-19 [13]. While young people (ages 20–39) in both lower and higher socioeconomic classes are associated with a higher risk of infecting with COVID-19 [13]. A similar study in Japan revealsthat social inequality exacerbates the impact of COVID-19 [16]. COVID-19 has mainly exacerbated gender inequality: compared with men, women are more likely to lose income and employment [17,18]. Uncommonly, Hussein (2021) finds that in Ethiopia and India, men are more vulnerable to the pandemic. According to Choi et al. (2021), the pandemic has negatively impacted children’s well-being. Furthermore, COVID-19 has been associated with exacerbating existing social inequalities and leading to new ones [19]. For example, existing socioeconomically marginalized groups lack technology-related skills, which may further exacerbate social inequalities [20].
Despite these emerging studies, there is surprisingly little knowledge on the relationship between COVID-19 and social classes in developing countries. The main goal of this study is to bridge this gap and contribute to the literature on the spatiality of pandemics.
COVID-19 is a new phenomenon, so accurate data on the relationship between socioeconomic status and COVID-19 risk are not available in Iran and other developing countries [21], which may pose challenges to capturing the spread of the pandemic. Therefore, the spatial analysis method was used in this study [22]. In the field of health [23,24,25], identifying the spatial characteristics of communities [26] can help understand and analyse different hotspots of the pandemic [27] and develop policies and interventions [27,28]. Furthermore, spatial analysis methods can help to quickly review and understand the evolution of the pandemic and provide timely support for preventive decision-making and measures [29]. Although some studies in the health domain have employed spatial analysis [30], little is known about the spatiality of COVID-19 among social classes in Iran.
This research aims to provide sufficient evidence on the spatial distribution of COVID-19 among different social classes by exploring the following research questions: (a) What has been the prevalence of COVID-19 in the social classes of Kermanshah metropolis? (b) What specific spatial pattern does COVID-19 follow in cities of developing countries? (c) What has been the spatial pattern of COVID-19 in different age groups and genders among social classes in cities of developing countries?
As aforementioned, there are no studies on social classes and COVID-19 in Iran, and this is the first in this area. Given this, this work aims to analyse the spatial epidemiological patterns of COVID-19 in the Kermanshah metropolis, highlighting socioeconomic status. Analysing the relationship between socioeconomic status and disease infection can help develop target-group oriented policy interventions and preventive measures [22].
2. Methodology
2.1. Case Study
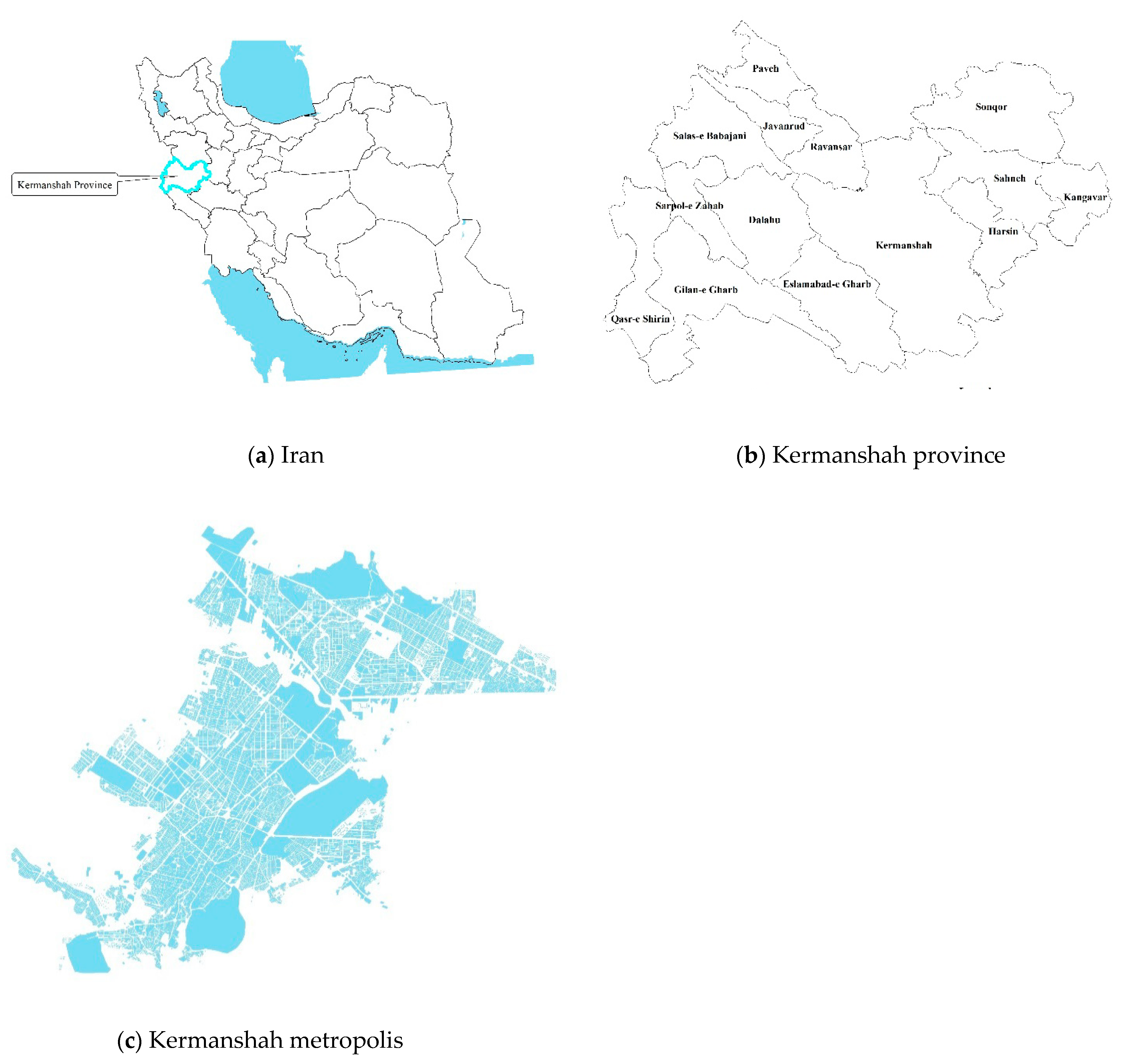
Kermanshah is one of the western provinces of Iran and comprises of 14 cities (Figure 1). Kermanshah Metropolis is the capital of Kermanshah Province. According to the 2016 census, the Kermanshah metropolis has a population of 937,527 and an area of over 10,000 hectares. In recent years, the Kermanshah metropolis has been facing several socioeconomic issues such as increased poverty, unemployment, suicide, HIV, and cancer [30,31,32,33,34,35]. More recently, there is evidence that unequal social, cultural, and economic opportunities underlie social disparities in the metropolis’ neighbourhoods [34,35]. In addition, the metropolis has been facing high levels of social inequality, which may also exacerbate the incidence and spread of COVID-19. In this context, the Kermanshah metropolis could be a good case study for understanding the spatial epidemiology of COVID-19 in Iran.
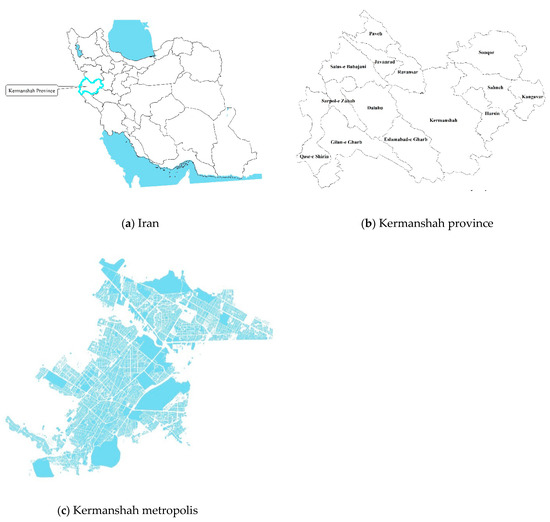
Figure 1.
(a–c) Location of Kermanshah metropolis in Kermanshah Province, Iran (source: authors).
2.2. Methods
In this study, the statistical data of COVID-19 were people infected with the disease in the Kermanshah metropolis area (March–June 2020). A total of 2144 people were infected by the disease in the metropolis during the study period. A total of131 people with no residential address were excluded from the analysis (missing data = 6.11%). Finally, data from 2013 patients were analysed.
To determine the social classes of the Kermanshah metropolis, the latest statistical block data were collected from the Statistics Center of Iran. Previous studies used social class based on economic factors, social status, cultural diversity, and material housing conditions [33,35]. Therefore, this study also used social class in the statistical block to identify poor, middle, and wealthy neighbourhoods in the metropolis.
Arc/GIS10.6 was used for data analysis. In addition, MeanCentre (MC), Standard Distance (SD), and Standard Deviational Ellipse (SDE) were used to analyse the research data. These spatial statistics methods have been extensively used by geographers to analyse point patterns statistically and depict trends in the spatial distribution of economic elements by summarising the direction and dispersion of those elements [36,37]. More specifically, they can help analyse the economic elements of spatiotemporal change processes from a multi-dimensional perspective, depict quantitative identification, and accurately reveal the economic characteristics of spatial distribution [38]. For example, the SDE reflects “the overall center using two-dimensional geographic coordinates with the weight of the economic elements in the spatial distribution”. All these methods have now become a conventional module in ArcGIS spatial statistical tools [39]. Applying these methods to this research can determine the direction and trends of the disease.
- (A)
- MC:
MC is the average x- and y-coordinate values of all the features of individuals infected with the disease [38,40], and is given as:
where,
xi and yi are the coordinate values for feature i;
n is the total number of features [38,40].
The weighted MC is:
where,
wi is the weight at feature i [40].
The tool also calculates the centre for a 3rd dimension if, a z attribute for each feature [34,40] is:
- (B)
- SD:
“Measuring the distribution compactness presents a single value that provides the dispersion of features around the center. The value is a distance, so the compactness of a set of features can be represented on a map by drawing a circle with a radius equal to the standard distance value” [34,38].
SD is given as:
where,
xi, yi and zi are the coordinates for feature i;
{, , } represents the MC for the features;
n is the total number of features [34,38].
The weighted SD is:
where,
wi is the weight at feature i and [23] represents the weighted MC [34,40].
- (C)
- SDE:
“This method calculates the standard deviation of the x- and y-coordinates from the MC to define the axes of the ellipse. Ellipses allow to see if the distribution of features is elongated and has a particular orientation” [34,38].
The SDE is given as:
where
where,
x and y are the coordinates for feature i;
{, } represent the MC for the features;
n is the total number of features.
The sample covariate matrix is decomposed into a standard form, resulting in the matrix being represented by its eigenvalues and eigenvectors.
The standard deviations for the x- and y-axis are [38,40]:
Moran’s I: This technique measures spatial autocorrelation of individuals infected with COVID-19 regarding locations and feature valuations. Considering a set of features and related characteristics, it assessesif the expressive patterns are random, clustered, or dispersed. It was calculated using 0.
“The Moran’s I Index value along with z-score and p-value assess the significationof the indicator. The p-value was numerous approximations to the area under the curve of a known distribution, limited by the test statistics” [35,38].
The statistics for spatial autocorrelation was given as [30,41]:
where,
zi is the deviation from an attribute for the feature i to its mean (xi-X);
wi,j is the spatial weight between features i and j;
n is the whole numerical features;
S0 is the aggregate of all spatial weights [32,38,41,42]:
The ZI-score for the statistic is computed as [41]:
where:
Kernel Density: It is calculated using the density of individuals infected with COVID-19 in a neighbourhood around these features. It is given as [41,43]:
where: SD is the standard interval, Dm is the average distance, and n is the number of individuals infected with COVID-19.
3. Results
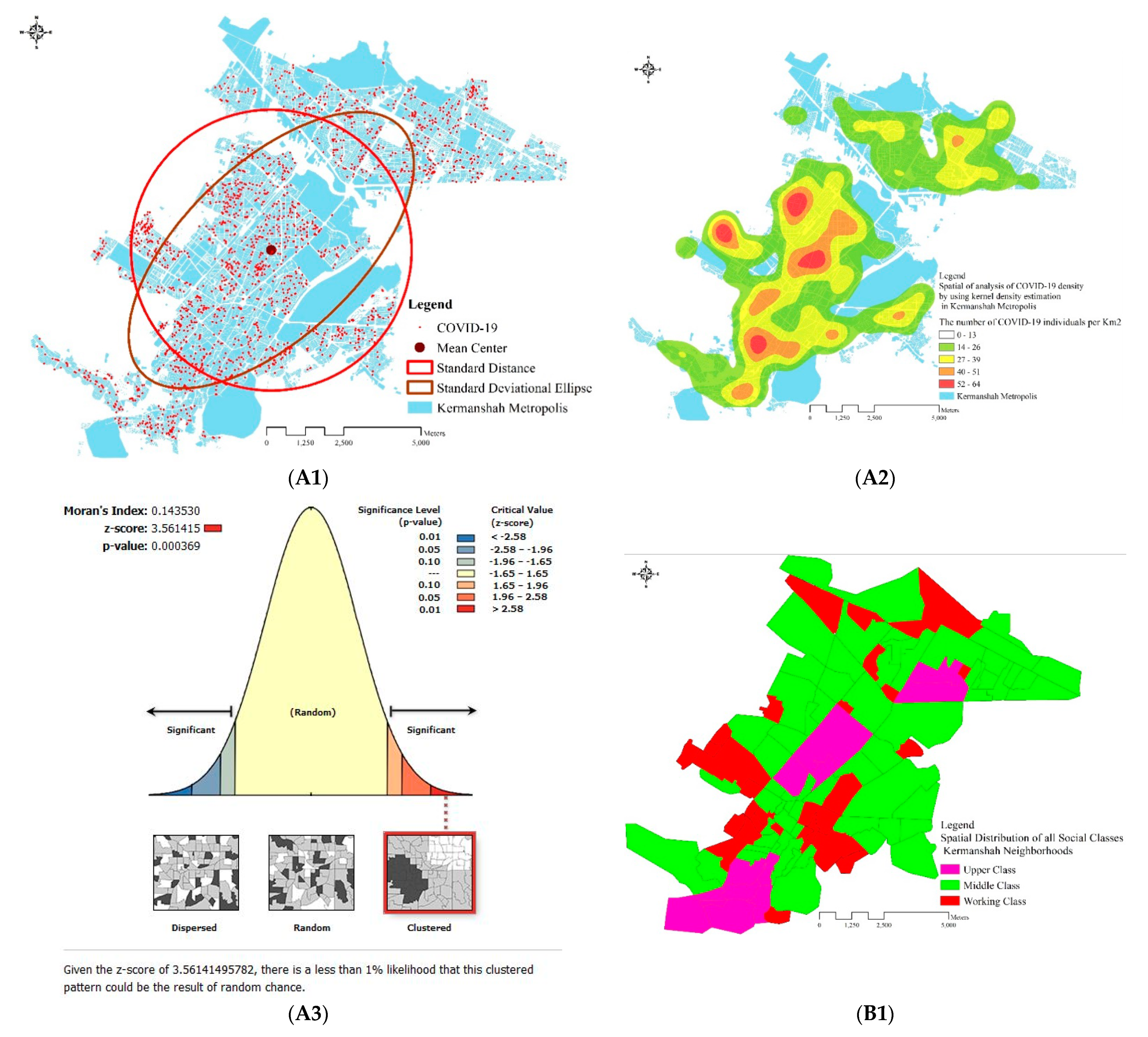
The results of MC and SD show that more than 70% of people intheKermanshah metropolis were infected with COVID19 (Figure 2A1). The SDE of COVID-19 reveals that the COVID-19 outbreak is distributed in all parts of the city. Importantly, the SDE of the pandemic was developed on the northeast-southwest side of the city (Figure 2A1). The KD estimation test is one of the most suitable methods to display COVID-19 data at continuous levels. The prevalence of COVID-19 was higher in certain areas of the metropolis. The results also indicate that 52–64 people per km2 were infected with COVID-19 (Figure 2A2).
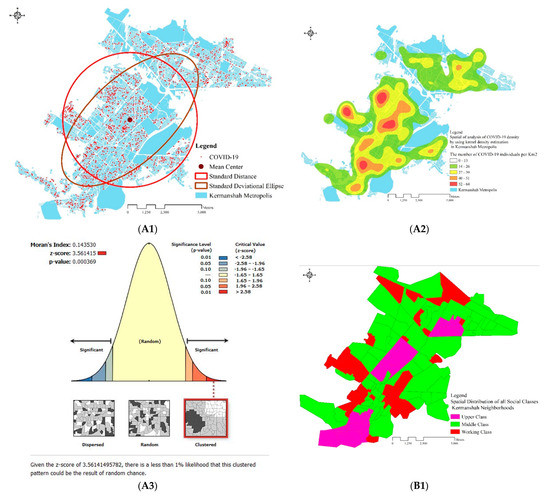
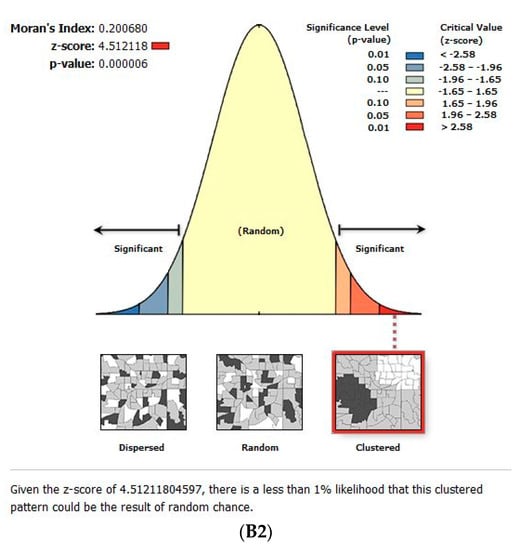
Figure 2.
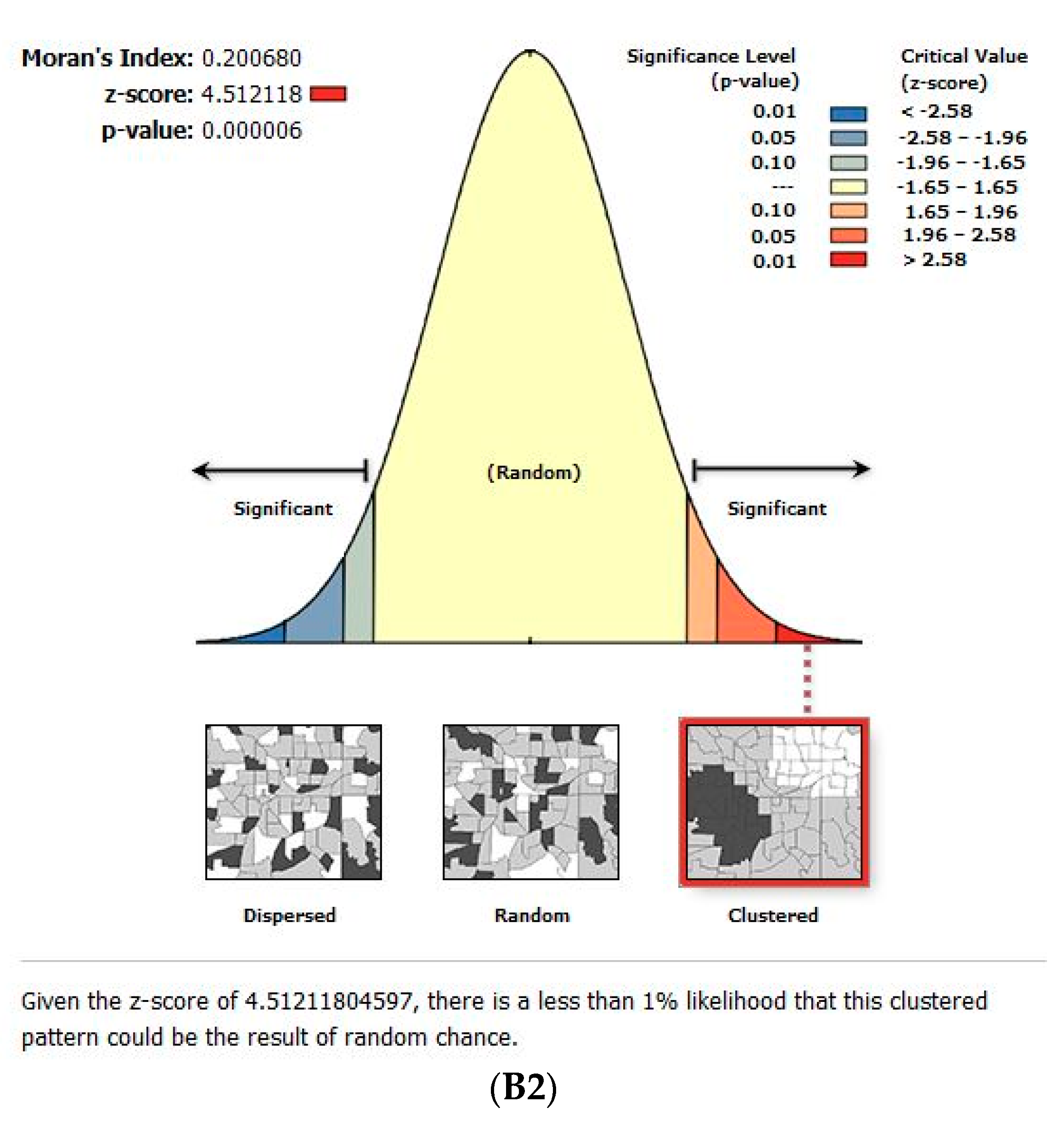
(A1) Geographic distribution using Mean Center, Standard Distance, and Standard Deviational Ellipse. (A2) Spatial analysis using Kernel Density. (A3) Moran’s I for COVID-19 (B1,B2) Cluster and Outlier analysis for the social class classifications of all 106 neighbourhoods in Kermanshah metropolis based on Moran’s I.
The results for COVID-19 in the neighbourhoods of Kermanshah metropolis are as follows: (a) the Moran’s I = 0.14 and (b) the Z score = 3.56 is less than 2.58 at the confidence level of 0.01, which is statistically significant. On the other hand, the computed values of social classes throughout the neighbourhoods in the metropolis are as follows: (a) Moran’s I = 0.20 and (b) the Z score = 4.51 is less than 2.58 at the confidence level of 0.01, which is statistically significant. Moran’s I indicate that COVID-19 and social classes exists in clusters across the neighbourhoods in Kermanshah metropolis (Figure 2B2,A3).
Between March 2020 and June 2020, 2013 people were infected with COVID-19 (male = 1164 and female = 849). The mean age of patients was 45 ± 18.69. The mean age of men and women was 44.51 ± 18.62 and 45.69 ± 18.76, respectively. In the poor, middle, and rich neighbourhoods, the mean age was 46.91 ± 20.78, 44.51 ± 18.24, and 45 ± 18.69, respectively. The mean age of women in poor, middle class, and rich neighbourhoods was 50.10 ± 21.46, 44.64 ± 17.89, and 43.71 ± 17.08, respectively. In addition, the mean age of men in these neighbourhoods was 44.33 ± 19.84, 44.43 ± 18.48, and 44.85 ± 17.80, respectively. It can be observed that COVID-19 was most prevalent among the middle class in the Kermanshah metropolis. On the other hand, age group comparisons indicate that in poorer communities, the elderly were more susceptible to the disease. However, in the middle-class 0–14 age group and in affluent neighbourhoods, people in the 15–64 age group were more exposed to the disease (Table 1).

Table 1.
Characteristics of patients with COVID-19 social classes in Kermanshah Metropolis.
4. Conclusions
The COVID-19 pandemic is a serious ongoing health issue worldwide. Studying people’s environment and socioeconomic status can contribute to the success of healthcare interventions. This study investigated the spatial patterns of COVID-19 among poor, middle-class, and affluent social classes in the Kermanshah metropolis, Iran. Five main conclusions can be drawn from this study.
First, the spread of COVID-19 occurs in a cluster shape in the Kermanshah metropolis [29,44]. The cluster formation indicates the unexpected occurrence of disease and the possibility of disease growth in the new centres that form in the future. This situation directly affects economic and social issues as well as government policies. Preventing COVID spread from the centres to other regions can be a fundamental challenge for decision-makers and other health organizations.
Second, the distribution of COVID-19 in the Kermanshah metropolis is uneven. Several studies found that differences in social welfare levels between different social classes and urban communities can be effective [45]. However, the results of this study highlighted that people in poor neighbourhoods and communities are less likely to be exposed to COVID-19 than others [13]. The disease is most prevalent among the middle class in the Kermanshah metropolis. This situation may be influenced by factors such as income, distance from healthcare centres, and education level [10,12]. For example, lower socioeconomic classes may face challenges in obtaining social support to deal with the pandemic. In addition, people from lower social classes are much less likely to see a specialist doctor than those from other social classes due to lack of financial means, unemployment, low daily wages, and distance from the community to specialized hospitals [46,47].
Third, the elderly in poorer neighbourhoods are more vulnerable to the disease than other age groups. During the study period, the prevalence of the disease among the elderly in the poorer classes was about 1.5 times that of the richer classes. This is consistent with evidence from other studies [13]. The higher mortality rates for these vulnerable groups are due to unsuitable conditions in their neighbourhoods. In middle class and rich neighbourhoods, people in the 0–14 and 15–64 age groups were more exposed to the disease. Although other studies posit that there is not sufficient information on this issue, it is expected that young people of higher socioeconomic status may attend social gatherings or participate in concerts that disrupt social distancing [48]. However, more research should be carried out to clarify this issue.
Fourth, social classes were clustered in the neighbourhoods of Kermanshah Metropolis. This condition could have been affected by inadequate economic, social, and cultural conditions in these neighbourhoods [30,33,35] and a shortage of material resources that are needed to meet people’s daily needs. Findings from other studies suggest that Kermanshah has high unemployment, and unemployment is often the most common cause of poverty [49]. As such, a direct link between poverty, unemployment, and the formation of social classes can be applied to Kermanshah. More likely, the segregation of cities into impoverished and rich residential areas, and the increasing distance between them in the face of neoliberalism can be the key reasons for the clustering of social classes in Kermanshah metropolis.
Finally, in line with existing scholarship [13,15,46], the findings of this study emphasized that the high incidence and spread of COVID-19 are related to the socioeconomic status of families and the cultural structure of neighbourhoods. Most residents of poor neighbourhoods see COVID-19 as a social stigma, so if they become infected, they try to hide the disease. This situation and other socioeconomic factors (as discussed above) prevent them from seeking medical treatment. Prevention programs and policy measures to control the spread of COVID-19 should target all people from the lower and middle classes, and young people from the higher class [13] in order to boost resilience of communities [5].
This study has several limitations. First, the sample was derived from Kermanshah only between March and June 2020. Second, the study relied on cross-sectional data and did not consider the individuals infected with COVID-19 for a long time. The implementation of a longitudinal scheme could be a feasible way to examine the robustness of the outcomes. Finally, the environmental, behavioural, genetic, and infection risk factors were not examined. It is suggested that these factors are investigated in the future study.
Nevertheless, the results of this study suggest that GIS-based spatial techniques can be useful for simplifying and measuring the prevalence of COVID-19 in specific regions and provide a basis for further studies on the impact of spatial factors on disease spread and transmission. Furthermore, the analysis of spatial distribution patterns can provide valuable information for government monitoring processes [46,50]. This study can be further improved by considering the impact of cultural factors on spatial patterns of COVID-19 and incorporating recent data (after June 2020).
Author Contributions
Conceptualization, A.Z.; Data curation, A.Z.; Formal analysis, A.Z. and K.Y.; Investigation, A.Z.; Methodology, A.Z., K.Y. and R.T.; Resources, A.Z., K.Y. and R.T.; Software, A.Z., K.Y. and R.T.; Supervision, K.Y. and R.T.; Validation, A.Z., K.Y. and R.T.; Visualization, A.Z.; Writing—original draft, A.Z., K.Y., R.T., S.S., F.N., E.S., S.M. and F.K.S.; Writing—review & editing, Komali Yenneti, A.Z., K.Y., R.T., S.S., F.N., E.S., S.M. and F.K.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of KERMANSHAH UNIVERSITY OF MEDICAL SCIENCES (IR.KUMS.REC.1400.228).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data will be made available upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Worldometer. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 3 July 2020).
- Arab-Zozani, M.; Ghoddoosi-Nejad, D. COVID-19 in Iran: The Good, the Bad, and the Ugly Strategies for Preparedness—A Report from the Field. Disaster Med. Public Health Prep. 2020, 15, e43–e45. [Google Scholar] [CrossRef] [PubMed]
- Stojkoski, V.; Utkovski, Z.; Jolakoski, P.; Tevdovski, D.; Kocarev, L. The socio-economic determinants of the coronavirus disease (COVID-19) pandemic. arXiv 2020, arXiv:2004.07947. [Google Scholar] [CrossRef]
- McKibbin, W.; Fernando, R. The global macroeconomic impacts of COVID-19: Seven scenarios. Asian Econ. Pap. 2021, 20, 1–30. [Google Scholar] [CrossRef]
- Jagrič, T.; Fister, D.; Jagrič, V. Reshaping the Healthcare Sector with Economic Policy Measures Based on COVID-19 Epidemic Severity: A Global Study. Healthcare 2022, 10, 315. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.K.; Saunoris, J.W.; Goel, S.S. Supply chain performance and economic growth: The impact of COVID-19 disruptions. J. Policy Modeling 2021, 43, 298–316. [Google Scholar] [CrossRef]
- Gupta, A.; Zhu, H.; Doan, M.K.; Michuda, A.; Majumder, B. Economic impacts of the COVID-19 lockdown in a remittance-dependent region. Am. J. Agric. Econ. 2021, 103, 466–485. [Google Scholar] [CrossRef]
- Islam, M.; Jannat, A.; Al Rafi, D.A.; Aruga, K. Potential economic impacts of the COVID-19 Pandemic on South Asian economies: A review. World 2020, 1, 283–299. [Google Scholar] [CrossRef]
- Açikgöz, Ö.; Günay, A. The early impact of the Covid-19 pandemic on the global and Turkish economy. Turk. J. Med. Sci. 2020, 50, 520–526. [Google Scholar] [CrossRef]
- Asna-ashary, M.; Farzanegan, M.R.; Feizi, M.; Sadati, S.M. COVID-19 Outbreak and Air Pollution in Iran: A Panel VAR Analysis; Joint Discussion Paper Series in Economics; Philipps-University Marburg, School of Business and Economics: Marburg, Germany, 2020. [Google Scholar]
- Holst, H.; Fessler, A.; Niehoff, S. Covid-19, social class and work experience in Germany: Inequalities in work-related health and economic risks. Eur. Soc. 2021, 23, S495–S512. [Google Scholar] [CrossRef]
- Sachedina, N.; Donaldson, L.J. Paediatric mortality related to pandemic influenza A H1N1 infection in England: An observational population-based study. Lancet 2010, 376, 1846–1852. [Google Scholar] [CrossRef] [Green Version]
- Oh, T.K.; Choi, J.-W.; Song, I.-A. Socioeconomic disparity and the risk of contracting COVID-19 in South Korea: An NHIS-COVID-19 database cohort study. BMC Public Health 2021, 21, 144. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y. Intersecting ethnic and native–migrant inequalities in the economic impact of the COVID-19 pandemic in the UK. Res. Soc. Stratif. Mobil. 2020, 68, 100528. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Li, X.; Lu, Y.; Hout, M. Two tales of one city: Unequal vulnerability and resilience to COVID-19 by socioeconomic status in Wuhan, China. Res. Soc. Stratif. Mobil. 2021, 72, 100584. [Google Scholar] [CrossRef]
- Sudo, N. The positive and negative effects of the COVID-19 pandemic on subjective well-being and changes in social inequality: Evidence from prefectures in Japan. SSM-Popul. Health 2022, 17, 101029. [Google Scholar] [CrossRef]
- King, M.M.; Frederickson, M.E. The Pandemic Penalty: The gendered effects of COVID-19 on scientific productivity. Socius 2021, 7, 23780231211006977. [Google Scholar] [CrossRef]
- Kristal, T.; Yaish, M. Does the coronavirus pandemic level the gender inequality curve? (It doesn’t). Res. Soc. Stratif. Mobil. 2020, 68, 100520. [Google Scholar] [CrossRef]
- Qian, Y.; Fan, W. Who loses income during the COVID-19 outbreak? Evidence from China. Res. Soc. Stratif. Mobil. 2020, 68, 100522. [Google Scholar] [CrossRef]
- Canale, N.; Marino, C.; Lenzi, M.; Vieno, A.; Griffiths, M.D.; Gaboardi, M.; Giraldo, M.; Cervone, C.; Massimo, S. How communication technology fosters individual and social wellbeing during the COVID-19 pandemic: Preliminary support for a digital interaction model. J. Happiness Stud. 2021, 23, 727–745. [Google Scholar] [CrossRef]
- Ahmadi, A.; Fadaei, Y.; Shirani, M.; Rahmani, F. Modeling and forecasting trend of COVID-19 epidemic in Iran until May 13, 2020. Med. J. Islamic Repub. Iran 2020, 34, 27. [Google Scholar] [CrossRef]
- Clayton, D.; Kaldor, J. Empirical Bayes estimates of age-standardized relative risks for use in disease mapping. Biometrics 1987, 43, 671–681. [Google Scholar] [CrossRef]
- Kazda, M.J.; Beel, E.R.; Villegas, D.; Martinez, J.G.; Patel, N.; Migala, W. Methodological complexities and the use of GIS in conducting a community needs assessment of a large US municipality. J. Community Health 2009, 34, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Schempf, A.H.; Kaufman, J.S.; Messer, L.C.; Mendola, P. The neighborhood contribution to black-white perinatal disparities: An example from two north Carolina counties, 1999–2001. Am. J. Epidemiol. 2011, 174, 744–752. [Google Scholar] [CrossRef] [Green Version]
- Bazemore, A.; Diller, P.; Carrozza, M. The impact of a clinic move on vulnerable patients with chronic disease: A geographic information systems (GIS) analysis. J. Am. Board Fam. Med. 2010, 23, 128–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morra, P.; Bagli, S.; Spadoni, G. The analysis of human health risk with a detailed procedure operating in a GIS environment. Environ. Int. 2006, 32, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Musa, G.J.; Chiang, P.-H.; Sylk, T.; Bavley, R.; Keating, W.; Lakew, B.; Tsou, H.-C.; Hoven, C.W. Use of GIS mapping as a public health tool–-from cholera to cancer. Health Serv. Insights 2013, 6, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Clarke, K.C.; McLafferty, S.L.; Tempalski, B.J. On epidemiology and geographic information systems: A review and discussion of future directions. Emerg. Infect. Dis. 1996, 2, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Murugesan, B.; Karuppannan, S.; Mengistie, A.T.; Ranganathan, M.; Gopalakrishnan, G. Distribution and Trend Analysis of COVID-19 in India: Geospatial Approach. J. Geogr. Stud. 2020, 4, 1–9. [Google Scholar] [CrossRef]
- Reshadat, S.; Zangeneh, A.; Saeidi, S.; Khademi, N.; Izadi, N.; Ghasemi, S.R.; Rajabi-Gilan, N. The spatial clustering analysis of HIV and poverty through GIS in the Metropolis of Kermanshah, Western Iran. Acta Med. Mediterr. 2016, 32, 1995–1999. [Google Scholar]
- Khademi, N.; Reshadat, S.; Zanganeh, A.; Saeidi, S.; Ghasemi, S.; Zakiei, A. Identifying HIV distribution pattern based on clustering test using GIS software, Kermanshah, Iran. HIV AIDS Rev. 2016, 15, 147–152. [Google Scholar] [CrossRef]
- Khademi, N.; Reshadat, S.; Zangeneh, A.; Saeidi, S.; Ghasemi, S.; Rajabi-Gilan, N.; Zakiei, A. A comparative study of the spatial distribution of HIV prevalence in the metropolis of Kermanshah, Iran, in 1996−2014 using geographical information systems. HIV Med. 2017, 18, 220–224. [Google Scholar] [CrossRef]
- Ghasemi, S.R.; Zangeneh, A.; Rajabi-Gilan, N.; Reshadat, S.; Saeidi, S.; Ziapour, A. Health-related quality of life in informal settlements in Kermanshah, Islamic Republic of Iran: Role of poverty and perception of family socioeconomic status. East. Mediterr. Health J. 2019, 25, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Reshadat, S.; Saedi, S.; Zangeneh, A.; Ghasemi, S.; Gilan, N.; Karbasi, A.; Bavandpoor, E. Spatial accessibility of the population to urban health centres in Kermanshah, Islamic Republic of Iran: A geographic information systems analysis. EMHJ-East. Mediterr. Health J. 2015, 21, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Reshadat, S.; Zangeneh, A.; Saeidi, S.; Izadi, N.; Ghasemi, S.R.; Rajabi-Gilan, N. A feasibility study of implementing the policies on increasing birth rate with an emphasis on socio-economic status: A case study of Kermanshah Metropolis, western Iran. Soc. Indic. Res. 2018, 140, 619–636. [Google Scholar] [CrossRef]
- Fortaleza, C.M.C.B.; Guimarães, R.B.; de Castro Catão, R.; Ferreira, C.P.; de Almeida, G.B.; Nogueira Vilches, T.; Pugliesi, E. The use of health geography modeling to understand early dispersion of COVID-19 in São Paulo, Brazil. PLoS ONE 2021, 16, e0245051. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Zhang, C. Development and applications of GIS-based spatial analysis in environmental geochemistry in the big data era. Environ. Geochem. Health 2022, 1–12. [Google Scholar] [CrossRef]
- Yang, X.; Grigorescu, A. Measuring economic spatial evolutional trend of Central and Eastern Europe by SDE method. Contemp. Econ. 2017, 11, 253–267. [Google Scholar]
- Ahemaitihali, A.; Dong, Z. Spatiotemporal Characteristics Analysis and Driving Forces Assessment of Flash Floods in Altay. Water 2022, 14, 331. [Google Scholar] [CrossRef]
- Lee, J.; Wong, D.W. Statistical Analysis with ArcView GIS; John Wiley & Sons: New York, NY, USA, 2001. [Google Scholar]
- Cromley, E.K.; McLafferty, S.L. GIS and Public Health; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Grekousis, G. Spatial Analysis Theory and Practice: Describe–Explore–Explain through GIS; Cambridge University Press: Cornwall, UK, 2020. [Google Scholar]
- Reshadat, S.; Zangeneh, A.; Saeidi, S.; Teimouri, R.; Yigitcanlar, T. Measures of spatial accessibility to health centers: Investigating urban and rural disparities in Kermanshah, Iran. J. Public Health 2019, 27, 519–529. [Google Scholar] [CrossRef]
- Yahya, M.S.S.; Safian, E.E.M.; Burhan, B. The Trend Distribution and Temporal Pattern Analysis of COVID-19 Pandemic using GIS framework in Malaysia. AIJR Prepr. 2020, 1–14. [Google Scholar] [CrossRef]
- Marmot, M. Social justice, epidemiology and health inequalities. Eur. J. Epidemiol. 2017, 32, 537–546. [Google Scholar] [CrossRef]
- Acharya, S.S. Population-Poverty Linkages and Health Consequences. CASTE/A Glob. J. Soc. Exclusion 2020, 1, 29–50. [Google Scholar] [CrossRef]
- Shaikh, M.; Miraldo, M.; Renner, A.-T. Waiting time at health facilities and social class: Evidence from the Indian caste system. PLoS ONE 2018, 13, e0205641. [Google Scholar] [CrossRef] [PubMed]
- Sugano, N.; Ando, W.; Fukushima, W. A Cluster Investigation of COVID-19 Occurring at Music Clubs in Osaka, Japan: Asymptomatic Carriers Can Transmit the Virus from Two Days after Exposure; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Razeghi Nasrabad, H.B.; Alimondegari, M.; Miri, R.; Kargar Shoraki, M.R. Sociological Understanding of the Causes of Youth Unemployment in Kermanshah Citybased on grounded theory. J. Sociol. Soc. Inst. 2021, 8, 47–82. [Google Scholar]
- Sarwar, S.; Waheed, R.; Sarwar, S.; Khan, A. COVID-19 challenges to Pakistan: Is GIS analysis useful to draw solutions? Sci. Total Environ. 2020, 730, 139089. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).