
Treatment of Diabetes Mellitus by Acupuncture: Dynamics of Blood Glucose Level and Its Mathematical Modelling



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
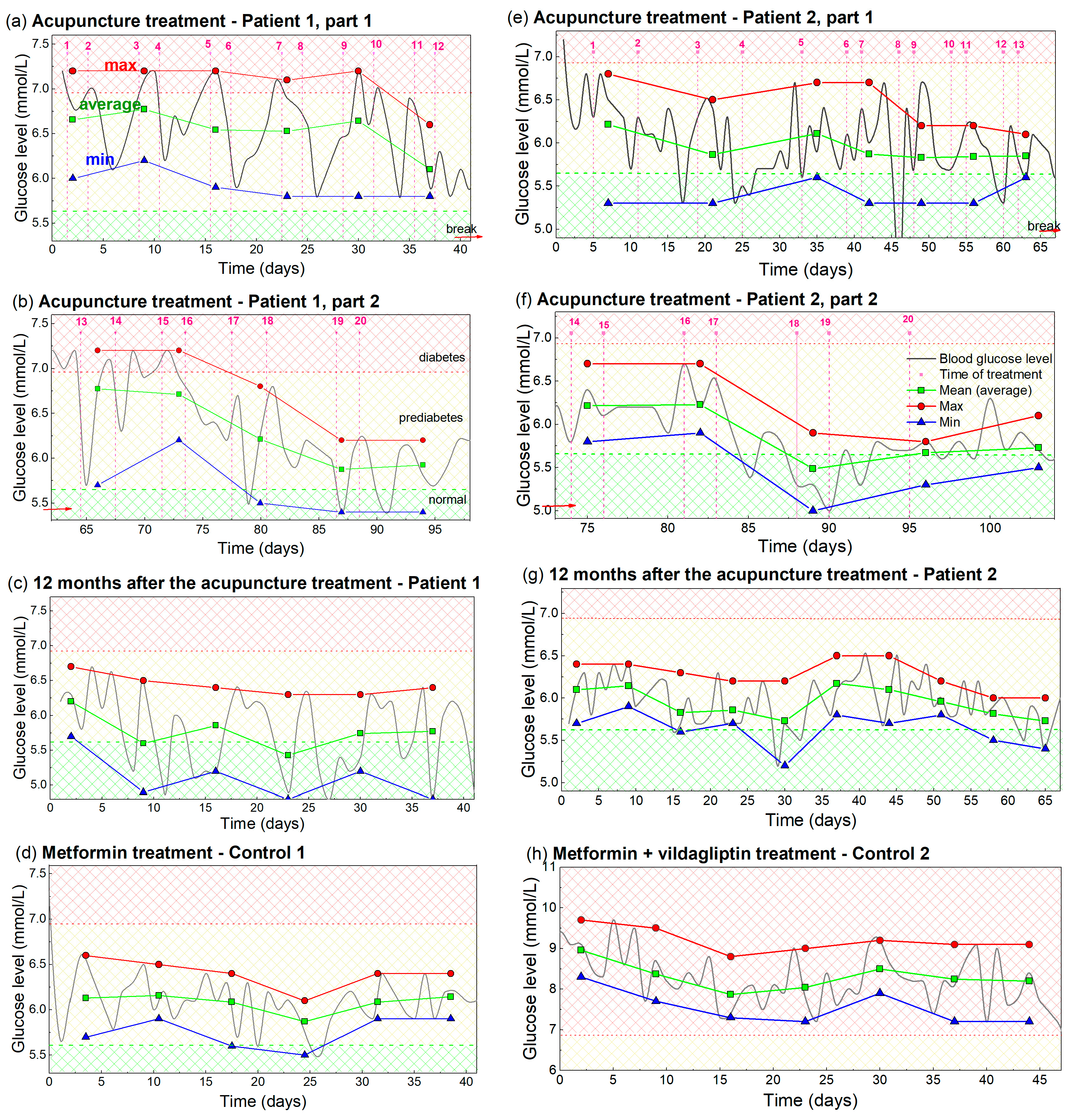
3.1. Measurement and Analysis of the Glucose Level
- (i)
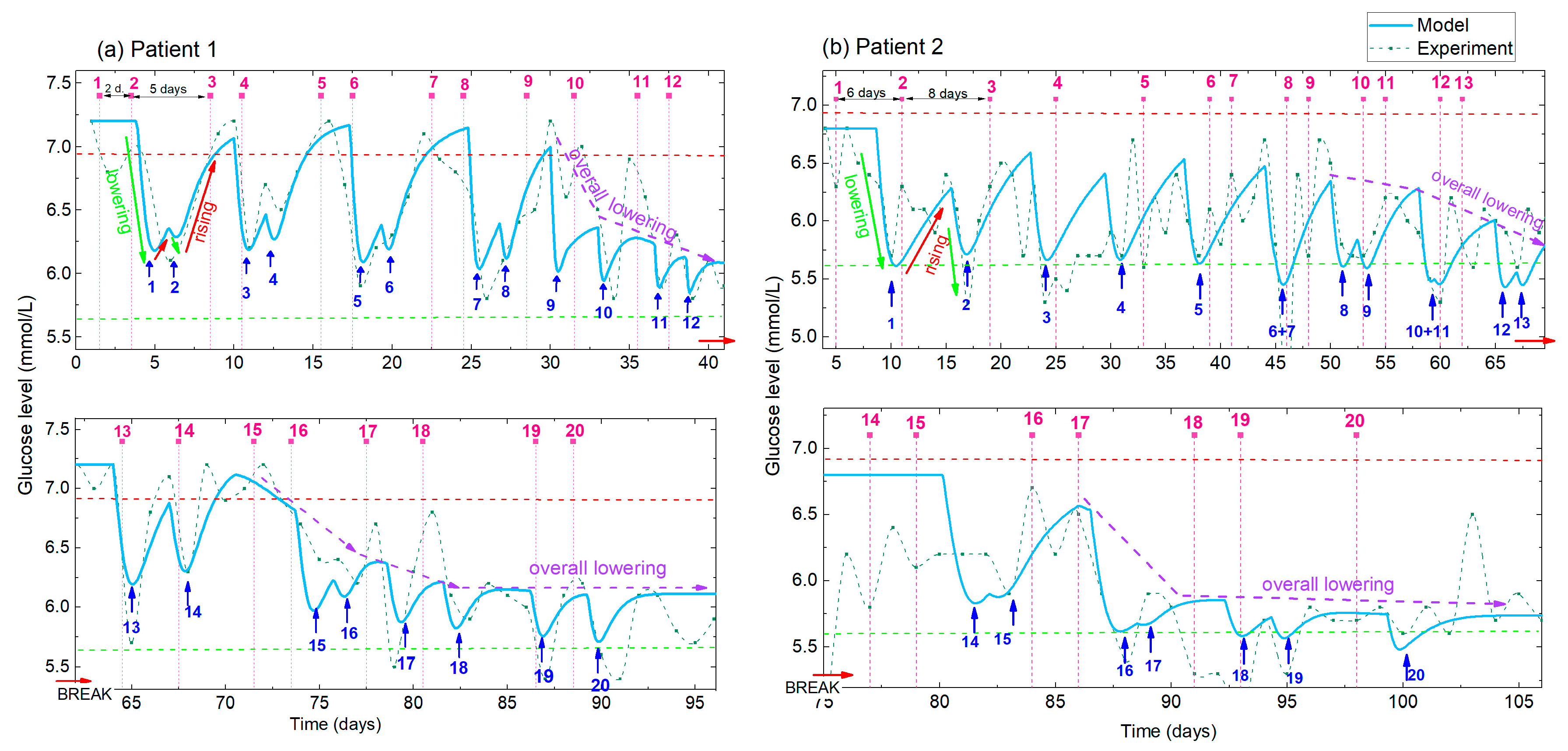
- Lowering effect. The glucose level significantly lowers after each single acupuncture treatment (green arrows); the reduction is especially strong after 2 treatments that are closer together in time (2 days separation). A delay in the response of the body of about 2–3 days is evident.
- (ii)
- Rising effect. The glucose level rises back to the initial high value during the 5 day acupuncture-free period for the first 9 acupuncture treatments (red arrows).
- (iii)
- Overall lowering effect. An overall lowering effect, i.e., BGL normalization, was observed after the 10th treatment, so the glucose level dropped below 6.2 mmol/L after the 12 treatments (violet dashed-line arrow).
3.2. Modelling of the Glucose Levels
3.3. Simulations and the Predictions of the Glucose Levels
3.4. Analysis of the Measured Glucose Using the Proposed Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Functions for Description of BGL Time Evolution during the Multiple Acupuncture Treatment
- BGL lowering effect:
- 2.
- BGL rising effect:
- 3.
- Overall BGL lowering effect:
References
- DeFronzo, R.A. Lilly lecture 1987. The triumvirate: Beta-cell, muscle, liver. A collusion responsible for NIDDM. Diabetes 1988, 37, 667–687. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization [Homepage on the Internet]. Updated 9 December 2020. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 20 June 2023).
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Riddle, M.C.; Herman, W.H. The cost of diabetes care—An elephant in the room. Diabetes Care 2018, 41, 929–932. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Xing, M.; Sun, W.; Yuan, X.; Dai, H.; Ding, H. Plasma Nesfatin-1 Level in Obese Patients after Acupuncture: A Randomised Controlled Trial. Acupunct. Med. 2014, 32, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Belivani, M.; Lundeberg, T.; Cummings, M.; Dimitroula, C.; Belivani, N.; Vasilakos, D.; Hatzitolios, A. Immediate Effect of Three Different Electroacupuncture Protocols on Fasting Blood Glucose in Obese Patients: A Pilot Study. Acupunct. Med. 2015, 33, 110–114. [Google Scholar] [CrossRef]
- Yin, J.; Kuang, J.; Chandalia, M.; Tuvdendorj, D.; Tumurbaatar, B.; Abate, N.; Chen, J.D.Z. Hypoglycemic effects and mechanisms of electroacupuncture on insulin resistance. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2014, 307, R332–R339. [Google Scholar] [CrossRef]
- Tomina, A.; Ishizaki, N.; Naruse, Y.; Kitakoji, H.; Yamamura, Y. Repeated application of low-frequency electroacupuncture improves high-fructose diet-induced insulin resistance in rats. Acupunct. Med. 2011, 29, 276–283. [Google Scholar] [CrossRef]
- Yu, Z.; Xia, Y.; Ju, C.; Mao, Z.; Gu, Y.; Xu, B. Electroacupuncture regulates glucose-inhibited neurons in treatment of simple obesity. Neural Regen. Res. 2013, 8, 809–816. [Google Scholar]
- Tzeng, C.Y.; Lee, Y.C.; Ho, T.Y.; Chen, Y.I.; Hsu, T.H.; Lin, J.G.; Lee, K.R.; Chang, S.L. Intracellular signalling pathways associated with the glucose-lowering effect of ST36 electroacupuncture in streptozotocin-induced diabetic rats. Acupunct. Med. 2015, 33, 395–399. [Google Scholar] [CrossRef]
- Lee, Y.C.; Li, T.M.; Tzeng, C.Y.; Cheng, Y.W.; Chen, Y.I.; Ho, W.J.; Lin, J.G.; Chang, S.L. Electroacupuncture-induced cholinergic nerve activation enhances the hypoglycemic effect of exogenous insulin in a rat model of streptozotocin-induced diabetes. Exp. Diabetes Res. 2011, 2011, 947138. [Google Scholar] [CrossRef]
- Lin, R.T.; Tzeng, C.Y.; Lee, Y.C.; Ho, W.J.; Cheng, J.T.; Lin, J.G.; Chang, S.L. Acute effect of electroacupuncture at the Zusanli acupoints on decreasing insulin resistance as shown by lowering plasma free fatty acid levels in steroid-background male rats. BMC Complement. Altern. Med. 2009, 9, 26. [Google Scholar] [CrossRef]
- Liao, H.Y.; Sun, M.F.; Lin, J.G.; Chang, S.L.; Lee, Y.C. Electroacupuncture plus metformin lowers glucose levels and facilitates insulin sensitivity by activating MAPK in steroid-induced insulin-resistant rats. Acupunct. Med. 2015, 33, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Benrick, A.; Maliqueo, M.; Johansson, J.; Sun, M.; Wu, X.; Mannerås-Holm, L.; Stener-Victorin, E. Enhanced insulin sensitivity and acute regulation of metabolic genes and signaling pathways after a single electrical or manual acupuncture session in female insulin-resistant rats. Acta Diabetol. 2014, 51, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Peplow, P.V. Electroacupuncture treatment of insulin resistance in diabetes mellitus. Acupunct. Med. 2015, 33, 347–349. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.; Koya, D. Acupuncture: Is it effective for treatment of insulin resistance? Diabetes Obes. Metab. 2010, 12, 555–569. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Chen, L.; Tang, L.; Chang, L.; Liu, S.; Tan, J.; Chen, Y.; Ren, Y.; Liang, F.; Cui, J. Electroacupuncture inhibits weight gain in diet-induced obese rats by activating hypothalamic LKB1-AMPK signaling. BMC Complement. Altern. Med. 2015, 15, 147. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.; Chen, R.; Nakagawa, A.; Nishizawa, M.; Tsuda, S.; Wang, H.; Koya, D. Low-frequency electroacupuncture improves insulin sensitivity in obese diabetic mice through activation of SIRT1/PGC-1α in skeletal muscle. Evid. Based Complement. Altern. Med. 2011, 2011, 735297. [Google Scholar] [CrossRef]
- Firouzjaei, A.; Li, G.C.; Wang, N.; Liu, W.X.; Zhu, B.M. Comparative evaluation of the therapeutic effect of metformin monotherapy with metformin and acupuncture combined therapy on weight loss and insulin sensitivity in diabetic patients. Nutr. Diabetes 2016, 6, e209. [Google Scholar] [CrossRef]
- Ma, F.Q.; Sun, C.J.; Wei, J.J.; Wang, Y.D.; Shen, J.C.; Chang, J.J. Electro-acupuncture regulates glucose metabolism in chronic stress model rats. Sci. Rep. 2020, 10, 11281. [Google Scholar] [CrossRef]
- Martinez, B.; Peplow, P.V. Treatment of insulin resistance by acupuncture: A review of human and animal studies. Acupunct. Med. 2016, 34, 310–319. [Google Scholar] [CrossRef]
- Choate, C.J. Modern Medicine and Traditional Chinese Medicine: Diabetes Mellitus, Part two. J. Chin. Med. 1999, 59, 1. [Google Scholar]
- Zhang, H.; Han, G.; Litscher, G. Traditional Acupuncture Meets Modern Nanotechnology: Opportunities and Perspectives. Evid. Based Complement. Altern. Med. 2019, 2019, 2146167. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Acupuncture: Review and Analysis of Reports on Controlled Clinical Trials; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- López-Palau, N.E.; Olais-Govea, J.M. Mathematical model of blood glucose dynamics by emulating the pathophysiology of glucose metabolism in type 2 diabetes mellitus. Sci. Rep. 2020, 10, 12697. [Google Scholar] [CrossRef] [PubMed]
- Vasquez-Muñoz, M.; Arce-Alvarez, A.; von Igel, M.; Veliz, C.; Ruiz-Esquide, G.; Ramirez-Campillo, R.; Alvarez, C.; Ramirez-Velez, R.; Crespo, F.A.; Izquierdo, M.; et al. Oscillatory pattern of glycemic control in patients with diabetes mellitus. Sci. Rep. 2021, 11, 5789. [Google Scholar] [CrossRef] [PubMed]
- Cedersund, G.; Strålfors, P. Putting the pieces together in diabetes research: Towards a hierarchical model of whole-body glucose homeostasis. Eur. J. Pharm. Sci. 2009, 36, 91–104. [Google Scholar] [CrossRef]
- Seo, W.; Park, S.W.; Kim, N.; Jin, S.M.; Park, S.M. A personalized blood glucose level prediction model with a fine-tuning strategy: A proof-of-concept study. Comput. Methods Programs Biomed. 2021, 211, 106424. [Google Scholar] [CrossRef]
- Chou, C.-Y.; Hsu, D.-Y.; Chou, C.-H. Predicting the Onset of Diabetes with Machine Learning Methods. J. Pers. Med. 2023, 13, 406. [Google Scholar] [CrossRef]
- World Health Organization [Homepage on the Internet]. Updated 10 July 2023. Mean Fasting Blood Glucose. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/2380 (accessed on 20 June 2023).
- Cosman, F.; Lindsay, R. Chapter 85—Parathyroid Hormone Treatment for Osteoporosis, In Osteoporosis, 4th ed.; Marcus, R., Feldman, D., Dempster, D.W., Luckey, M., Cauley, J.A., Eds.; Academic Press: Cambridge, MA, USA, 2013; pp. 1949–1961. ISBN 9780124158535. [Google Scholar]
- Chen, Y.; Wu, S.; Tian, Y. Cholecystectomy as a risk factor of metabolic syndrome: From epidemiologic clues to biochemical mechanisms. Lab. Investig. 2018, 98, 7–14. [Google Scholar] [CrossRef]
- Oestreich, A.K.; Moley, K.H. Developmental and Transmittable Origins of Obesity-Associated Health Disorders. Trends Genet. 2017, 33, 399–407. [Google Scholar] [CrossRef]
- Rivera, E.J.; Goldin, A.; Fulmer, N.; Tavares, R.; Wands, J.R.; de la Monte, S.M. Insulin and insulin-like growth factor expression and function deteriorate with progression of Alzheimer’s disease: Link to brain reductions in acetylcholine. J. Alzheimer’s Dis. 2005, 8, 247–268. [Google Scholar] [CrossRef]
- Gudala, K.; Bansal, D.; Schifano, F.; Bhansali, A. Diabetes mellitus and risk of dementia: A meta-analysis of prospective observational studies. J. Diabetes Investig. 2013, 4, 640–650. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z.; Jiao, R.; Wang, P.; Zhu, Y.; Zhao, J.; De Jager, P.; Bennett, D.A.; Jin, L.; Xiong, M. Shared Causal Paths underlying Alzheimer’s dementia and Type 2 Diabetes. Sci. Rep. 2020, 10, 4107. [Google Scholar] [CrossRef] [PubMed]
- Moloney, A.M.; Griffin, R.J.; Timmons, S.; O’Connor, R.; Ravid, R.; O’Neill, C. Defects in IGF-1 receptor, insulin receptor and IRS-1/2 in Alzheimer’s disease indicate possible resistance to IGF-1 and insulin signalling. Neurobiol. Aging 2010, 31, 224–243. [Google Scholar] [CrossRef] [PubMed]
- Steen, E.; Terry, B.M.; Rivera, E.J.; Cannon, J.L.; Neely, T.R.; Tavares, R.; Xu, X.J.; Wands, J.R.; de La Monte, S.M. Impaired insulin and insulin-like growth factor expression and signaling mechanisms in Alzheimer’s disease-is this type 3 diabetes? J. Alzheimer’s Dis. 2005, 7, 63–80. [Google Scholar] [CrossRef]
- Hoyer, S.; Nitsch, R. Cerebral excess release of neurotransmitter amino acids subsequent to reduced cerebral glucose metabolism in early-onset dementia of Alzheimer type. J. Neural Transm. 1989, 75, 227–232. [Google Scholar] [CrossRef]
- Talbot, K.; Wang, H.Y.; Kazi, H.; Han, L.Y.; Bakshi, K.P.; Stucky, A.; Fuino, R.L.; Kawaguchi, K.R.; Samoyedny, A.J.; Wilson, R.S.; et al. Demonstrated brain insulin resistance in Alzheimer’s disease patients is associated with IGF-1 resistance, IRS-1 dysregulation, and cognitive decline. J. Clin. Investig. 2012, 122, 1316–1338. [Google Scholar] [CrossRef]
- Correia, S.C.; Santos, R.X.; Carvalho, C.; Cardoso, S.; Candeias, E.; Santos, M.S.; Oliveira, C.R.; Moreira, P.I. Insulin signaling, glucose metabolism and mitochondria: Major players in Alzheimer’s disease and diabetes interrelation. Brain Res. 2012, 1441, 64–78. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Ta, Q.T.H.; Nguyen, T.K.O.; Nguyen, T.T.D.; Giau, V.V. Type 3 Diabetes and Its Role Implications in Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 3165. [Google Scholar] [CrossRef]
- Baker, L.D.; Cross, D.J.; Minoshima, S.; Belongia, D.; Watson, G.S.; Craft, S. Insulin resistance and Alzheimer-like reductions in regional cerebral glucose metabolism for cognitively normal adults with prediabetes or early type 2 diabetes. Arch. Neurol. 2011, 68, 51–57. [Google Scholar] [CrossRef]
- Samuraki, M.; Matsunari, I.; Chen, W.P.; Yajima, K.; Yanase, D.; Fujikawa, A.; Takeda, N.; Nishimura, S.; Matsuda, H.; Yamada, M. Partial volume effect-corrected FDG PET and grey matter volume loss in patients with mild Alzheimer’s disease. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 1658–1669. [Google Scholar] [CrossRef]
- Dukart, J.; Kherif, F.; Mueller, K.; Adaszewski, S.; Schroeter, M.L.; Frackowiak, R.S.; Draganski, B.; Alzheimer’s Disease Neuroimaging Initiative. Generative FDG-PET and MRI model of aging and disease progression in Alzheimer’s disease. PLoS Comput. Biol. 2013, 9, e1002987. [Google Scholar] [CrossRef] [PubMed]
- Barrett, C.E.; Koyama, A.K.; Alvarez, P.; Chow, W.; Lundeen, E.A.; Perrine, C.G.; Pavkov, M.E.; Rolka, D.B.; Wiltz, J.L.; Bull-Otterson, L.; et al. Risk for Newly Diagnosed Diabetes >30 Days After SARS-CoV-2 Infection Among Persons Aged <18 Years—United States, 1 March 2020-28 June 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 59–65. [Google Scholar] [PubMed]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Ayoubkhani, D.; Khunti, K.; Nafilyan, V.; Maddox, T.; Humberstone, B.; Diamond, I.; Banerjee, A. Post-COVID syndrome in individuals admitted to hospital with COVID-19: Retrospective cohort study. BMJ 2021, 372, 693. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šimat, M.; Janković Makek, M.; Mičetić, M. Treatment of Diabetes Mellitus by Acupuncture: Dynamics of Blood Glucose Level and Its Mathematical Modelling. Sci 2023, 5, 38. https://doi.org/10.3390/sci5040038
Šimat M, Janković Makek M, Mičetić M. Treatment of Diabetes Mellitus by Acupuncture: Dynamics of Blood Glucose Level and Its Mathematical Modelling. Sci. 2023; 5(4):38. https://doi.org/10.3390/sci5040038
Chicago/Turabian StyleŠimat, Marija, Mateja Janković Makek, and Maja Mičetić. 2023. "Treatment of Diabetes Mellitus by Acupuncture: Dynamics of Blood Glucose Level and Its Mathematical Modelling" Sci 5, no. 4: 38. https://doi.org/10.3390/sci5040038
APA StyleŠimat, M., Janković Makek, M., & Mičetić, M. (2023). Treatment of Diabetes Mellitus by Acupuncture: Dynamics of Blood Glucose Level and Its Mathematical Modelling. Sci, 5(4), 38. https://doi.org/10.3390/sci5040038