Features Associated with Visible Lamina Cribrosa Pores in Individuals of African Ancestry with Glaucoma: Primary Open-Angle African Ancestry Glaucoma Genetics (POAAGG) Study


 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subject Recruitment and Clinical Assessment
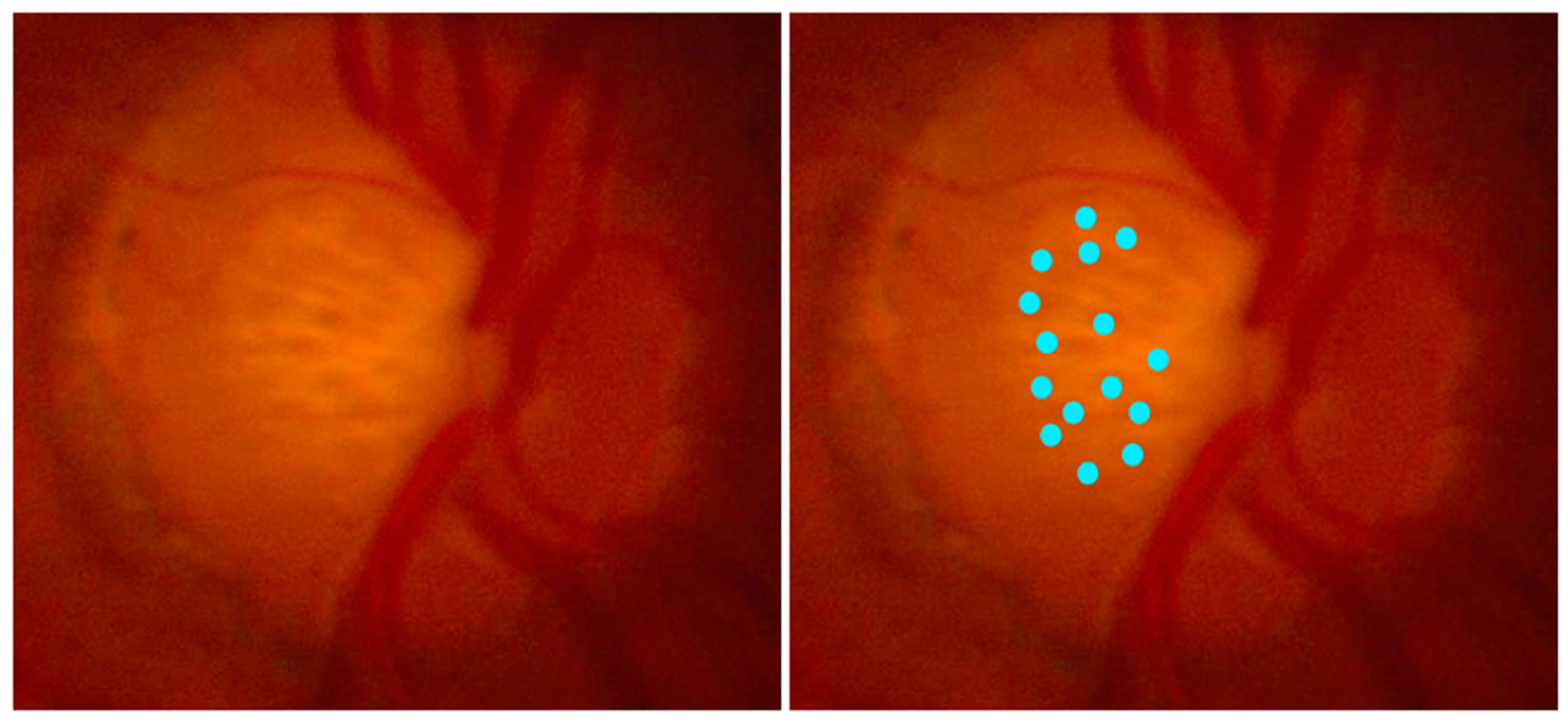
2.2. Grading of Color Stereo Images of the ONH
2.3. Re-Grading for LCPs
2.4. Specimen Collection and Ancestry Analysis
2.5. Genetic Analysis
2.6. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cole, B.S.; Gudiseva, H.V.; Pistilli, M.; Salowe, R.; McHugh, C.P.; Zody, M.C.; Chavali, V.R.M.; Ying, G.S.; Moore, J.H.; O’Brien, J.M. The Role of Genetic Ancestry as a Risk Factor for Primary Open-Angle Glaucoma in African Americans. Investig. Ophthalmol. Vis. Sci. 2021, 62, 28. [Google Scholar] [CrossRef]
- Broman, A.T.; Quigley, H.A.; West, S.K.; Katz, J.; Munoz, B.; Bandeen-Roche, K.; Tielsch, J.M.; Friedman, D.S.; Crowston, J.; Taylor, H.R.; et al. Estimating the Rate of Progressive Visual Field Damage in Those with Open-Angle Glaucoma, from Cross-Sectional Data. Investig. Ophthalmol. Vis. Sci. 2008, 49, 66. [Google Scholar] [CrossRef]
- Tielsch, J.M. Racial Variations in the Prevalence of Primary Open-Angle Glaucoma: The Baltimore Eye Survey. JAMA 1991, 266, 369. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, B. Causes of Blindness and Visual Impairment in a Population of Older AmericansThe Salisbury Eye Evaluation Study. Arch. Ophthalmol. 2000, 118, 819. [Google Scholar] [CrossRef] [PubMed]
- Sommer, A.; Tielsch, J.M.; Katz, J.; Quigley, H.A.; Gottsch, J.D.; Javitt, J.C.; Martone, J.F.; Royall, R.M.; Witt, K.A.; Ezrine, S. Racial Differences in the Cause-Specific Prevalence of Blindness in East Baltimore. N. Engl. J. Med. 1991, 325, 1412–1417. [Google Scholar] [CrossRef] [PubMed]
- Abu-Amero, K.K.; González, A.M.; Osman, E.A.; Larruga, J.M.; Cabrera, V.M.; Al-Obeidan, S.A. Mitochondrial DNA Lineages of African Origin Confer Susceptibility to Primary Open-Angle Glaucoma in Saudi Patients. Mol. Vis. 2011, 17, 1468–1472. [Google Scholar] [PubMed]
- Tsai, C.; Zangwill, L.; Gonzalez, C.; Irak, I.; Garden, V.; Hoffman, R.; Weinreb, R. Ethnic Differences in Optic Nerve Head Topography. J. Glaucoma 1995, 4, 248–257. [Google Scholar] [CrossRef]
- Zangwill, L.M.; Weinreb, R.N.; Berry, C.C.; Smith, A.R.; Dirkes, K.A.; Coleman, A.L.; Piltz-Seymour, J.R.; Liebmann, J.M.; Cioffi, G.A.; Trick, G.; et al. Racial Differences in Optic Disc Topography: Baseline Results from the Confocal Scanning Laser Ophthalmoscopy Ancillary Study to the Ocular Hypertension Treatment Study. Arch. Ophthalmol. 2004, 122, 22–28. [Google Scholar] [CrossRef]
- Quigley, H.A.; Addicks, E.M.; Green, W.R.; Maumenee, A.E. Optic Nerve Damage in Human Glaucoma. II. The Site of Injury and Susceptibility to Damage. Arch. Ophthalmol. 1981, 99, 635–649. [Google Scholar] [CrossRef]
- Morgan, W.H.; Yu, D.Y.; Alder, V.A.; Cringle, S.J.; Cooper, R.L.; House, P.H.; Constable, I.J. The Correlation between Cerebrospinal Fluid Pressure and Retrolaminar Tissue Pressure. Investig. Ophthalmol. Vis. Sci. 1998, 39, 1419–1428. [Google Scholar]
- Morgan, W.H.; Chauhan, B.C.; Yu, D.-Y.; Cringle, S.J.; Alder, V.A.; House, P.H. Optic Disc Movement with Variations in Intraocular and Cerebrospinal Fluid Pressure. Investig. Ophthalmol. Vis. Sci. 2002, 43, 3236–3242. [Google Scholar]
- Siaudvytyte, L.; Januleviciene, I.; Daveckaite, A.; Ragauskas, A.; Bartusis, L.; Kucinoviene, J.; Siesky, B.; Harris, A. Literature Review and Meta-Analysis of Translaminar Pressure Difference in Open-Angle Glaucoma. Eye 2015, 29, 1242–1250. [Google Scholar] [CrossRef] [PubMed]
- Shoji, T.; Kuroda, H.; Suzuki, M.; Ibuki, H.; Araie, M.; Yoneya, S. Glaucomatous Changes in Lamina Pores Shape within the Lamina Cribrosa Using Wide Bandwidth, Femtosecond Mode-Locked Laser OCT. PLoS ONE 2017, 12, e0181675. [Google Scholar] [CrossRef]
- Miller, K.M.; Quigley, H.A. The Clinical Appearance of the Lamina Cribrosa as a Function of the Extent of Glaucomatous Optic Nerve Damage. Ophthalmology 1988, 95, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Tezel, G.; Trinkaus, K.; Wax, M.B. Alterations in the Morphology of Lamina Cribrosa Pores in Glaucomatous Eyes. Br. J. Ophthalmol. 2004, 88, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Lucy, K.A.; Schuman, J.S.; Sigal, I.A.; Bilonick, R.A.; Lu, C.; Liu, J.; Grulkowski, I.; Nadler, Z.; Ishikawa, H.; et al. Tortuous Pore Path Through the Glaucomatous Lamina Cribrosa. Sci. Rep. 2018, 8, 7281. [Google Scholar] [CrossRef] [PubMed]
- Healey, P.R.; Mitchell, P. Visibility of Lamina Cribrosa Pores and Open-Angle Glaucoma. Am. J. Ophthalmol. 2004, 138, 871–872. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Li, L.; Song, F. Study on the Deformations of the Lamina Cribrosa during Glaucoma. Acta Biomater. 2017, 55, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Glidai, Y.; Lucy, K.A.; Schuman, J.S.; Alexopoulos, P.; Wang, B.; Wu, M.; Liu, M.; Vande Geest, J.P.; Kollech, H.G.; Lee, T.; et al. Microstructural Deformations within the Depth of the Lamina Cribrosa in Response to Acute In Vivo Intraocular Pressure Modulation. Investig. Ophthalmol. Vis. Sci. 2022, 63, 25. [Google Scholar] [CrossRef]
- Kiumehr, S.; Park, S.C.; Dorairaj, S.; Teng, C.C.; Tello, C.; Liebmann, J.M.; Ritch, R. In Vivo Evaluation of Focal Lamina Cribrosa Defects in Glaucoma. Arch. Ophthalmol. 2012, 130, 552–559. [Google Scholar] [CrossRef]
- Salowe, R.J.; Lee, R.; Zenebe-Gete, S.; Vaughn, M.; Gudiseva, H.V.; Pistilli, M.; Kikut, A.; Becker, E.; Collins, D.W.; He, J.; et al. Recruitment Strategies and Lessons Learned from a Large Genetic Study of African Americans. PLoS Glob. Public Health 2022, 2, e0000416. [Google Scholar] [CrossRef]
- Kikut, A.; Vaughn, M.; Salowe, R.; Sanyal, M.; Merriam, S.; Lee, R.; Becker, E.; Lomax-Reese, S.; Lewis, M.; Ryan, R.; et al. Evaluation of a Multimedia Marketing Campaign to Engage African American Patients in Glaucoma Screening. Prev. Med. Rep. 2020, 17, 101057. [Google Scholar] [CrossRef]
- Charlson, E.S.; Sankar, P.S.; Miller-Ellis, E.; Regina, M.; Fertig, R.; Salinas, J.; Pistilli, M.; Salowe, R.J.; Rhodes, A.L.; Merritt, W.T.; et al. The Primary Open-Angle African American Glaucoma Genetics Study: Baseline Demographics. Ophthalmology 2015, 122, 711–720. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Addis, V.; Oyeniran, E.; Daniel, E.; Salowe, R.; Zorger, R.; Lee, R.; Pistilli, M.; Maguire, M.; Cui, Q.; Miller-Ellis, E.; et al. Non-Physician Grader Reliability in Measuring Morphological Features of the Optic Nerve Head in Stereo Digital Images. Eye 2019, 33, 838–844. [Google Scholar] [CrossRef]
- Daniel, E.; Addis, V.; Maguire, M.G.; McGeehan, B.; Chen, M.; Salowe, R.J.; Zenebe-Gete, S.; Meer, E.; Lee, R.; Smith, E.; et al. Prevalence and Factors Associated with Optic Disc Tilt in the Primary Open-Angle African American Glaucoma Genetics Study. Ophthalmol. Glaucoma 2022, 5, 544–553. [Google Scholar] [CrossRef]
- Verma, S.S.; Gudiseva, H.V.; Chavali, V.R.M.; Salowe, R.J.; Bradford, Y.; Guare, L.; Lucas, A.; Collins, D.W.; Vrathasha, V.; Nair, R.M.; et al. A Multi-Cohort Genome-Wide Association Study in African Ancestry Individuals Reveals Risk Loci for Primary Open-Angle Glaucoma. Cell 2024, 187, 464–480.e10. [Google Scholar] [CrossRef]
- Raj, A.; Stephens, M.; Pritchard, J.K. fastSTRUCTURE: Variational Inference of Population Structure in Large SNP Data Sets. Genetics 2014, 197, 573–589. [Google Scholar] [CrossRef]
- Zangwill, L.M.; Ayyagari, R.; Liebmann, J.M.; Girkin, C.A.; Feldman, R.; Dubiner, H.; Dirkes, K.A.; Holmann, M.; Williams-Steppe, E.; Hammel, N.; et al. The African Descent and Glaucoma Evaluation Study (ADAGES) III: Contribution of Genotype to Glaucoma Phenotype in African Americans: Study Design and Baseline Data. Ophthalmology 2019, 126, 156–170. [Google Scholar] [CrossRef]
- Taylor, K.D.; Guo, X.; Zangwill, L.M.; Liebmann, J.M.; Girkin, C.A.; Feldman, R.M.; Dubiner, H.; Hai, Y.; Samuels, B.C.; Panarelli, J.F.; et al. Genetic Architecture of Primary Open Angle Glaucoma in Individuals of African Descent: The African Descent & Glaucoma Evaluation Study (ADAGES) III. Ophthalmology 2019, 126, 38–48. [Google Scholar] [CrossRef]
- Koprubasi, S.; Bulut, E. Impact of Obesity on Peripapillary Choroidal Thickness, Macular Choroidal Thickness, and Lamina Cribrosa Morphology. Photodiagnosis Photodyn. Ther. 2023, 43, 103724. [Google Scholar] [CrossRef]
- Tan, N.Y.Q.; Koh, V.; Girard, M.J.A.; Cheng, C.Y. Imaging of the Lamina Cribrosa and Its Role in Glaucoma: A Review. Clin. Experiment. Ophthalmol. 2018, 46, 177–188. [Google Scholar] [CrossRef]
- Park, H.-Y.L.; Shin, D.Y.; Jeon, S.J.; Kim, Y.-C.; Jung, Y.; Kim, E.K.; Shin, H.-Y.; Jung, K.I.; Choi, J.A.; Lee, N.Y.; et al. Predicting the Development of Normal Tension Glaucoma and Related Risk Factors in Normal Tension Glaucoma Suspects. Sci. Rep. 2021, 11, 16697. [Google Scholar] [CrossRef]
- Omodaka, K.; Takahashi, S.; Matsumoto, A.; Maekawa, S.; Kikawa, T.; Himori, N.; Takahashi, H.; Maruyama, K.; Kunikata, H.; Akiba, M.; et al. Clinical Factors Associated with Lamina Cribrosa Thickness in Patients with Glaucoma, as Measured with Swept Source Optical Coherence Tomography. PLoS ONE 2016, 11, e0153707. [Google Scholar] [CrossRef]
- Jung, K.I.; Jeon, S.; Park, C.K. Lamina Cribrosa Depth Is Associated With the Cup-to-Disc Ratio in Eyes with Large Optic Disc Cupping and Cup-to-Disc Ratio Asymmetry. J. Glaucoma 2016, 25, e536–e545. [Google Scholar] [CrossRef]
- Jeon, S.-J.; Park, H.-Y.L.; Park, C.-K. Vessel Density Loss of the Deep Peripapillary Area in Glaucoma Suspects and Its Association with Features of the Lamina Cribrosa. J. Clin. Med. 2021, 10, 2373. [Google Scholar] [CrossRef]
- Wu, J.; Du, Y.; Li, J.; Fan, X.; Lin, C.; Wang, N. The Influence of Different Intraocular Pressure on Lamina Cribrosa Parameters in Glaucoma and the Relation Clinical Implication. Sci. Rep. 2021, 11, 9755. [Google Scholar] [CrossRef]
- Ivers, K.M.; Sredar, N.; Patel, N.B.; Rajagopalan, L.; Queener, H.M.; Twa, M.D.; Harwerth, R.S.; Porter, J. In Vivo Changes in Lamina Cribrosa Microarchitecture and Optic Nerve Head Structure in Early Experimental Glaucoma. PLoS ONE 2015, 10, e0134223. [Google Scholar] [CrossRef]
- Kim, J.-A.; Kim, T.-W.; Weinreb, R.N.; Lee, E.J.; Girard, M.J.A.; Mari, J.M. Lamina Cribrosa Morphology Predicts Progressive Retinal Nerve Fiber Layer Loss In Eyes with Suspected Glaucoma. Sci. Rep. 2018, 8, 738. [Google Scholar] [CrossRef]
- Burgoyne, C. The Morphological Difference between Glaucoma and Other Optic Neuropathies. J. Neuro-Ophthalmol. Off. J. N. Am. Neuro-Ophthalmol. Soc. 2015, 35 (Suppl. S1), S8–S21. [Google Scholar] [CrossRef]
- Esfandiari, H.; Efatizadeh, A.; Hassanpour, K.; Doozandeh, A.; Yaseri, M.; Loewen, N.A. Factors Associated with Lamina Cribrosa Displacement after Trabeculectomy Measured by Optical Coherence Tomography in Advanced Primary Open-Angle Glaucoma. Graefes Arch. Clin. Exp. Ophthalmol. Albrecht Graefes Arch. Klin. Exp. Ophthalmol. 2018, 256, 2391–2398. [Google Scholar] [CrossRef]
- Shon, K.; Hye Jo, Y.; Won Shin, J.; Kwon, J.; Jeong, D.; Kook, M.S. Nasalization of Central Retinal Vessel Trunk Predicts Rapid Progression of Central Visual Field in Open-Angle Glaucoma. Sci. Rep. 2020, 10, 3789. [Google Scholar] [CrossRef]
- Wang, M.; Wang, H.; Pasquale, L.R.; Baniasadi, N.; Shen, L.Q.; Bex, P.J.; Elze, T. Relationship Between Central Retinal Vessel Trunk Location and Visual Field Loss in Glaucoma. Am. J. Ophthalmol. 2017, 176, 53–60. [Google Scholar] [CrossRef]
- Sawada, Y.; Araie, M.; Shibata, H.; Iwase, T. Nasal Displacement of Retinal Vessels on the Optic Disc in Glaucoma Associated with a Nasally Angled Passage through Lamina Cribrosa. Sci. Rep. 2021, 11, 4176. [Google Scholar] [CrossRef]
- Chi, T.; Ritch, R.; Stickler, D.; Pitman, B.; Tsai, C.; Hsieh, F.Y. Racial Differences in Optic Nerve Head Parameters. Arch. Ophthalmol. 1989, 107, 836–839. [Google Scholar] [CrossRef]
- Girkin, C.A.; McGwin, G.; Xie, A.; Deleon-Ortega, J. Differences in Optic Disc Topography between Black and White Normal Subjects. Ophthalmology 2005, 112, 33–39. [Google Scholar] [CrossRef]
- Wilson, R.; Richardson, T.M.; Hertzmark, E.; Grant, W.M. Race as a Risk Factor for Progressive Glaucomatous Damage. Ann. Ophthalmol. 1985, 17, 653–659. [Google Scholar]
- Skaat, A.; De Moraes, C.G.; Bowd, C.; Sample, P.A.; Girkin, C.A.; Medeiros, F.A.; Ritch, R.; Weinreb, R.N.; Zangwill, L.M.; Liebmann, J.M.; et al. African Descent and Glaucoma Evaluation Study (ADAGES): Racial Differences in Optic Disc Hemorrhage and Beta-Zone Parapapillary Atrophy. Ophthalmology 2016, 123, 1476–1483. [Google Scholar] [CrossRef]
- Yang, S.-A.; Ciociola, E.C.; Mitchell, W.; Hall, N.; Lorch, A.C.; Miller, J.W.; Friedman, D.S.; Boland, M.V.; Elze, T.; Zebardast, N.; et al. Effectiveness of Microinvasive Glaucoma Surgery in the United States: Intelligent Research in Sight Registry Analysis 2013–2019. Ophthalmology 2023, 130, 242–255. [Google Scholar] [CrossRef]
- Kang, J.H.; Wang, M.; Frueh, L.; Rosner, B.; Wiggs, J.L.; Elze, T.; Pasquale, L.R. Cohort Study of Race/Ethnicity and Incident Primary Open-Angle Glaucoma Characterized by Autonomously Determined Visual Field Loss Patterns. Transl. Vis. Sci. Technol. 2022, 11, 21. [Google Scholar] [CrossRef]
- Halawa, O.A.; Kolli, A.; Oh, G.; Mitchell, W.G.; Glynn, R.J.; Kim, D.H.; Friedman, D.S.; Zebardast, N. Racial and Socioeconomic Differences in Eye Care Utilization among Medicare Beneficiaries with Glaucoma. Ophthalmology 2022, 129, 397–405. [Google Scholar] [CrossRef]
- Allison, K.; Patel, D.G.; Greene, L. Racial and Ethnic Disparities in Primary Open-Angle Glaucoma Clinical Trials. JAMA Netw. Open 2021, 4, e218348. [Google Scholar] [CrossRef]
- Bonnemaijer, P.W.M.; Lo Faro, V.; Sanyiwa, A.J.; Hassan, H.G.; Cook, C.; GIGA Study Group; Van de Laar, S.; Lemij, H.G.; Klaver, C.C.W.; Jansonius, N.M.; et al. Differences in Clinical Presentation of Primary Open-Angle Glaucoma between African and European Populations. Acta Ophthalmol. 2021, 99, e1118–e1126. [Google Scholar] [CrossRef]
- Rhodes, L.A.; Huisingh, C.; Johnstone, J.; Fazio, M.; Smith, B.; Clark, M.; Downs, J.C.; Owsley, C.; Girard, M.J.A.; Mari, J.M.; et al. Variation of Laminar Depth in Normal Eyes with Age and Race. Investig. Ophthalmol. Vis. Sci. 2014, 55, 8123–8133. [Google Scholar] [CrossRef]
- Gracitelli, C.P.B.; Zangwill, L.M.; Diniz-Filho, A.; Abe, R.Y.; Girkin, C.A.; Weinreb, R.N.; Liebmann, J.M.; Medeiros, F.A. Detection of Glaucoma Progression in Individuals of African Descent Compared with Those of European Descent. JAMA Ophthalmol. 2018, 136, 329–335. [Google Scholar] [CrossRef]
- Gupta, P.; Zhao, D.; Guallar, E.; Ko, F.; Boland, M.V.; Friedman, D.S. Prevalence of Glaucoma in the United States: The 2005–2008 National Health and Nutrition Examination Survey. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2905–2913. [Google Scholar] [CrossRef]
- Girkin, C.A.; Fazio, M.A.; Bowd, C.; Medeiros, F.A.; Weinreb, R.N.; Liebmann, J.M.; Proudfoot, J.; Zangwill, L.M.; Belghith, A. Racial Differences in the Association of Anterior Lamina Cribrosa Surface Depth and Glaucoma Severity in the African Descent and Glaucoma Evaluation Study (ADAGES). Investig. Ophthalmol. Vis. Sci. 2019, 60, 4496–4502. [Google Scholar] [CrossRef]
- Girkin, C.A.; Belghith, A.; Bowd, C.; Medeiros, F.A.; Weinreb, R.N.; Liebmann, J.M.; Proudfoot, J.A.; Zangwill, L.M.; Fazio, M.A. Racial Differences in the Rate of Change in Anterior Lamina Cribrosa Surface Depth in the African Descent and Glaucoma Evaluation Study. Investig. Ophthalmol. Vis. Sci. 2021, 62, 12. [Google Scholar] [CrossRef]
- Fazio, M.A.; Johnstone, J.K.; Smith, B.; Wang, L.; Girkin, C.A. Displacement of the Lamina Cribrosa in Response to Acute Intraocular Pressure Elevation in Normal Individuals of African and European Descent. Investig. Ophthalmol. Vis. Sci. 2016, 57, 3331–3339. [Google Scholar] [CrossRef]
- Girkin, C.A.; Fazio, M.A.; Yang, H.; Reynaud, J.; Burgoyne, C.F.; Smith, B.; Wang, L.; Downs, J.C. Variation in the Three-Dimensional Histomorphometry of the Normal Human Optic Nerve Head with Age and Race: Lamina Cribrosa and Peripapillary Scleral Thickness and Position. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3759–3769. [Google Scholar] [CrossRef]
- Morgan-Davies, J.; Taylor, N.; Hill, A.R.; Aspinall, P.; O’Brien, C.J.; Azuara-Blanco, A. Three Dimensional Analysis of the Lamina Cribrosa in Glaucoma. Br. J. Ophthalmol. 2004, 88, 1299–1304. [Google Scholar] [CrossRef][Green Version]


{kind=link}
| n | Visible Pores in the Lamina Cribrosa (n = 2117 Eyes) | RR (95%CI) | p-Value | ||
|---|---|---|---|---|---|
| Age (years) | ≤60 | 682 | 511 (74.9%) | Ref | 0.08 |
| (60, 70] | 836 | 618 (73.9%) | 0.99 (0.92, 1.06) | ||
| (70, 80] | 880 | 606 (68.9%) | 0.92 (0.85, 0.99) | ||
| ≥80 | 545 | 382 (70.1%) | 0.94 (0.86, 1.02) | ||
| Sex | Male | 1213 | 890 (73.4%) | Ref | 0.22 |
| Female | 1730 | 1227 (70.9%) | 0.97 (0.92, 1.02) | ||
| Body mass index | <25 | 689 | 502 (72.9%) | 0.97 (0.91, 1.04) | 0.048 |
| 25–30 | 979 | 732 (74.8%) | Ref | ||
| ≥30 | 1275 | 883 (69.3%) | 0.93 (0.87, 0.99) | ||
| Diabetes | No | 1794 | 1312 (73.1%) | Ref | 0.14 |
| Yes | 1143 | 801 (70.1%) | 0.96 (0.91, 1.01) | ||
| Missing | 6 | 4 | |||
| q0 (per 0.1 increase in q0) | 1807 | 1278 (70.7%) | 0.97 (0.95,0.99) | 0.006 | |
| Hypertension | No | 641 | 490 (76.4%) | Ref | 0.01 |
| Yes | 2296 | 1623 (70.7%) | 0.92 (0.87, 0.98) | ||
| Missing | 6 | 4 | |||
| Family history of glaucoma | No | 1191 | 847 (71.1%) | Ref | 0.63 |
| Yes | 1599 | 1153 (72.1%) | 1.01 (0.96, 1.07) | ||
| Missing | 153 | 117 | |||
| Alcohol use | No | 1556 | 1114 (71.6%) | Ref | 0.79 |
| Yes | 1346 | 971 (72.1%) | 1.01 (0.95, 1.06) | ||
| Missing | 41 | 32 | |||
| Tobacco use | No | 1339 | 982 (73.3%) | Ref | 0.19 |
| Yes | 1604 | 1135 (70.8%) | 0.96 (0.91, 1.02) | ||
| Previous glaucoma surgery | No | 2067 | 1497 (72.4%) | Ref | 0.43 |
| Yes | 868 | 614 (70.7%) | 0.98 (0.92, 1.04) | ||
| Missing | 8 | 6 | |||
| n | Visible Pores in the Lamina Cribrosa (n = 2117 Eyes) | RR (95%CI) | p-Value | ||
|---|---|---|---|---|---|
| Disc shape | Round | 1247 | 940 (75.4%) | Ref | 0.003 |
| Oval | 1592 | 1102 (69.2%) | 0.92 (0.87, 0.96) | ||
| Other | 10 | 6 (60.0%) | 0.80 (0.45, 1.42) | ||
| Missing | 94 | 69 | |||
| Cup disc ratio | <0.9 | 1003 | 683 (68.1%) | Ref | <0.0001 |
| ≥0.9 | 268 | 235 (87.7%) | 1.29 (1.20, 1.38) | ||
| Missing | 1672 | 1199 | |||
| Shape of cup | Conical | 1107 | 645 (58.3%) | Ref | <0.0001 |
| Cylindrical | 1241 | 965 (77.8%) | 1.33 (1.25, 1.42) | ||
| Bean pot/partial bean pot | 395 | 365 (92.4%) | 1.59 (1.49, 1.69) | ||
| Other | 14 | 8 (57.1%) | 0.98 (0.62, 1.55) | ||
| Missing | 186 | 134 | |||
| Cup depth | Shallow | 317 | 154 (48.6%) | Ref | <0.0001 |
| Moderate | 1737 | 1225 (70.5%) | 1.45 (1.28, 1.65) | ||
| Deep | 704 | 605 (85.9%) | 1.77 (1.56, 2.01) | ||
| Missing | 185 | 133 | |||
| Tilted disc | No | 2547 | 1832 (71.9%) | Ref | 0.80 |
| Yes | 275 | 200 (72.7%) | 1.01 (0.93, 1.10) | ||
| Missing | 121 | 85 | |||
| Disc hemorrhage | No | 2802 | 2017 (72.0%) | Ref | 0.29 |
| Yes | 48 | 31 (64.6%) | 0.90 (0.73, 1.11) | ||
| Missing | 93 | 69 | |||
| Arteriole narrowing | No | 2802 | 2010 (71.7%) | Ref | 0.22 |
| Yes | 48 | 38 (79.2%) | 1.10 (0.95, 1.28) | ||
| Missing | 93 | 69 | |||
| Beta parapapillary atrophy | No | 856 | 627 (73.2%) | Ref | 0.36 |
| Yes | 2087 | 1490 (71.4%) | 0.97 (0.92, 1.03) | ||
| Venule narrowing | No | 2806 | 2016 (71.8%) | Ref | 0.90 |
| Yes | 44 | 32 (72.7%) | 1.01 (0.84, 1.21) | ||
| Missing | 93 | 69 | |||
| Bayonetting | No | 2462 | 1703 (69.2%) | Ref | <0.0001 |
| Yes | 481 | 414 (86.1%) | 1.24 (1.19, 1.30) | ||
| Nasalization of central vessels | No | 1751 | 1095 (62.5%) | Ref | <0.0001 |
| Yes | 1095 | 949 (86.7%) | 1.39 (1.32, 1.45) | ||
| Missing | 97 | 73 | |||
| Pallor of the neural rim | No | 2730 | 1958 (71.7%) | Ref | 0.37 |
| Yes | 119 | 90 (75.6%) | 1.05 (0.94, 1.18) | ||
| Missing | 94 | 69 | |||
| Visible Lamina Cribrosa Pores (n = 2117 Eyes) | No Visible Lamina Cribrosa Pores (n = 826 Eyes) | p-Value | |
|---|---|---|---|
| Highest IOP (mmHg) | |||
| N | 1149 | 441 | 0.46 |
| Mean (SD) | 19.15 (6.56) | 19.47 (6.76) | |
| Range | (2.00, 56.00) | (7.00, 52.00) | |
| Central corneal thickness (µm) | |||
| N | 869 | 332 | 0.28 |
| Mean (SD) | 533.43 (38.34) | 536.71 (40.06) | |
| Range | (420.00, 690.00) | (433.00, 659.00) | |
| Cup disc ratio | |||
| N | 918 | 353 | <0.0001 |
| Mean (SD) | 0.76 (0.15) | 0.62 (0.20) | |
| Range | (0.10, 1.00) | (0.10, 1.00) | |
| Visual acuity (logMAR) | |||
| N | 872 | 328 | 0.56 |
| Mean (SD) | 0.31 (0.66) | 0.29 (0.62) | |
| Range | (−0.12, 5.00) | (−0.12, 6.00) | |
| Nerve Fiber layer thickness (µm) | |||
| N | 410 | 159 | 0.16 |
| Mean (SD) | 73.38 (14.69) | 75.38 (12.38) | |
| Range | (38.00, 120.00) | (46.00, 100.00) | |
| Visual field MD | |||
| N | 489 | 200 | 0.007 |
| Mean (SD) | −8.72 (9.59) | −6.35 (8.71) | |
| Range | (−33.15, 22.08) | (−32.00, 21.01) | |
| n | Visible Pores in Lamina Cribrosa Present (n = 457 Eyes) | aRR (95%CI) | p-Value * | ||
|---|---|---|---|---|---|
| Cup Disc Ratio | <0.9 | 526 | 342 (65.0%) | Ref | <0.0001 |
| ≥0.9 | 128 | 115 (89.8%) | 1.21 (1.11, 1.33) | ||
| Shape of cup | Conical | 277 | 149 (53.8%) | Ref | <0.0001 |
| Cylindrical | 273 | 214 (78.4%) | 1.41 (1.24, 1.61) | ||
| Bean pot/partial bean pot | 100 | 92 (92.0%) | 1.36 (1.19, 1.55) | ||
| Other | 4 | 2 (50.0%) | 1.07 (0.38, 3.01) | ||
| Nasalization of central vessels | No | 387 | 225 (58.1%) | Ref | <0.0001 |
| Yes | 267 | 232 (86.9%) | 1.34 (1.20, 1.48) | ||
| q0 (per 0.1 increase in q0) | 645 | 457 (69.9%) | 0.96 (0.93, 0.99) | 0.005 | |
| n | Visible Pores in Lamina Cribrosa (n = 856 Eyes) | aRR (95%CI) | p-Value * | ||
|---|---|---|---|---|---|
| Cup Disc Ratio | <0.9 | 945 | 644 (68.1%) | Ref | 0.005 |
| ≥0.9 | 242 | 212 (87.6%) | 1.11 (1.04, 1.19) | ||
| Shape of cup | Conical | 525 | 317 (60.4%) | Ref | <0.0001 |
| Cylindrical | 480 | 372 (77.5%) | 1.22 (1.11, 1.33) | ||
| Bean Pot/Partial Bean Pot | 174 | 162 (93.1%) | 1.24 (1.13, 1.36) | ||
| Other | 8 | 5 (62.5%) | 1.06 (0.65, 1.72) | ||
| Cup depth | Shallow | 167 | 86 (51.5%) | Ref | 0.01 |
| Moderate | 735 | 520 (70.7%) | 1.24 (1.06, 1.46) | ||
| Deep | 285 | 250 (87.7%) | 1.27 (1.07, 1.50) | ||
| Nasalization of central vessels | No | 673 | 405 (60.2%) | Ref | <0.0001 |
| Yes | 514 | 451 (87.7%) | 1.33 (1.23, 1.44) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jordan, J.A.; Daniel, E.; Chen, Y.; Salowe, R.J.; Zhu, Y.; Miller-Ellis, E.; Addis, V.; Sankar, P.S.; Zhu, D.; Smith, E.J.; et al. Features Associated with Visible Lamina Cribrosa Pores in Individuals of African Ancestry with Glaucoma: Primary Open-Angle African Ancestry Glaucoma Genetics (POAAGG) Study. Vision 2024, 8, 24. https://doi.org/10.3390/vision8020024
Jordan JA, Daniel E, Chen Y, Salowe RJ, Zhu Y, Miller-Ellis E, Addis V, Sankar PS, Zhu D, Smith EJ, et al. Features Associated with Visible Lamina Cribrosa Pores in Individuals of African Ancestry with Glaucoma: Primary Open-Angle African Ancestry Glaucoma Genetics (POAAGG) Study. Vision. 2024; 8(2):24. https://doi.org/10.3390/vision8020024
Chicago/Turabian StyleJordan, Jalin A., Ebenezer Daniel, Yineng Chen, Rebecca J. Salowe, Yan Zhu, Eydie Miller-Ellis, Victoria Addis, Prithvi S. Sankar, Di Zhu, Eli J. Smith, and et al. 2024. "Features Associated with Visible Lamina Cribrosa Pores in Individuals of African Ancestry with Glaucoma: Primary Open-Angle African Ancestry Glaucoma Genetics (POAAGG) Study" Vision 8, no. 2: 24. https://doi.org/10.3390/vision8020024
APA StyleJordan, J. A., Daniel, E., Chen, Y., Salowe, R. J., Zhu, Y., Miller-Ellis, E., Addis, V., Sankar, P. S., Zhu, D., Smith, E. J., Lee, R., Ying, G.-S., & O’Brien, J. M. (2024). Features Associated with Visible Lamina Cribrosa Pores in Individuals of African Ancestry with Glaucoma: Primary Open-Angle African Ancestry Glaucoma Genetics (POAAGG) Study. Vision, 8(2), 24. https://doi.org/10.3390/vision8020024