Therapeutic Application of Virtual Reality in the Rehabilitation of Mild Cognitive Impairment: A Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy and Selection of Studies
2.2.1. Inclusion Criteria
- ParticipantsParticipants were individuals with MCI alone.
- InterventionInterventions included VR alone or combined interventions.
- ComparisonsActivities that did not involve an intervention or did not include VR were selected for comparisons.
- OutcomesTo perform a meta-analysis, a comparative analysis was performed when there were three or more identical variables in the studies.
- Types of studiesAmong different study designs, only RCTs were selected.
2.2.2. Exclusion Criteria
2.2.3. Strategy for Literature Search
2.2.4. Study Selection and Data Extraction
2.2.5. Quality Assessment
2.3. Strategy for Data Synthesis
3. Results
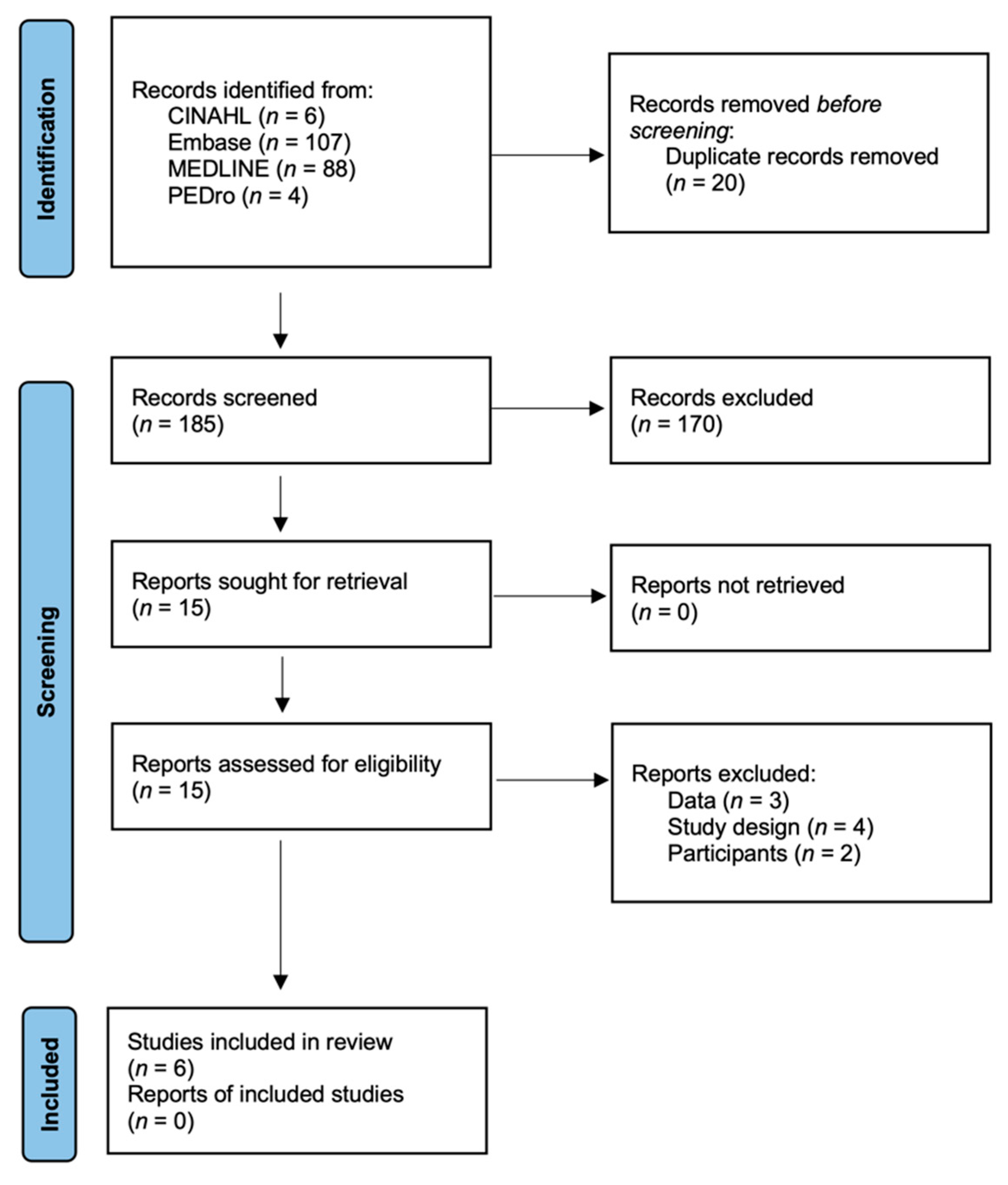
3.1. Literature Search and Characteristics of the Included Trials
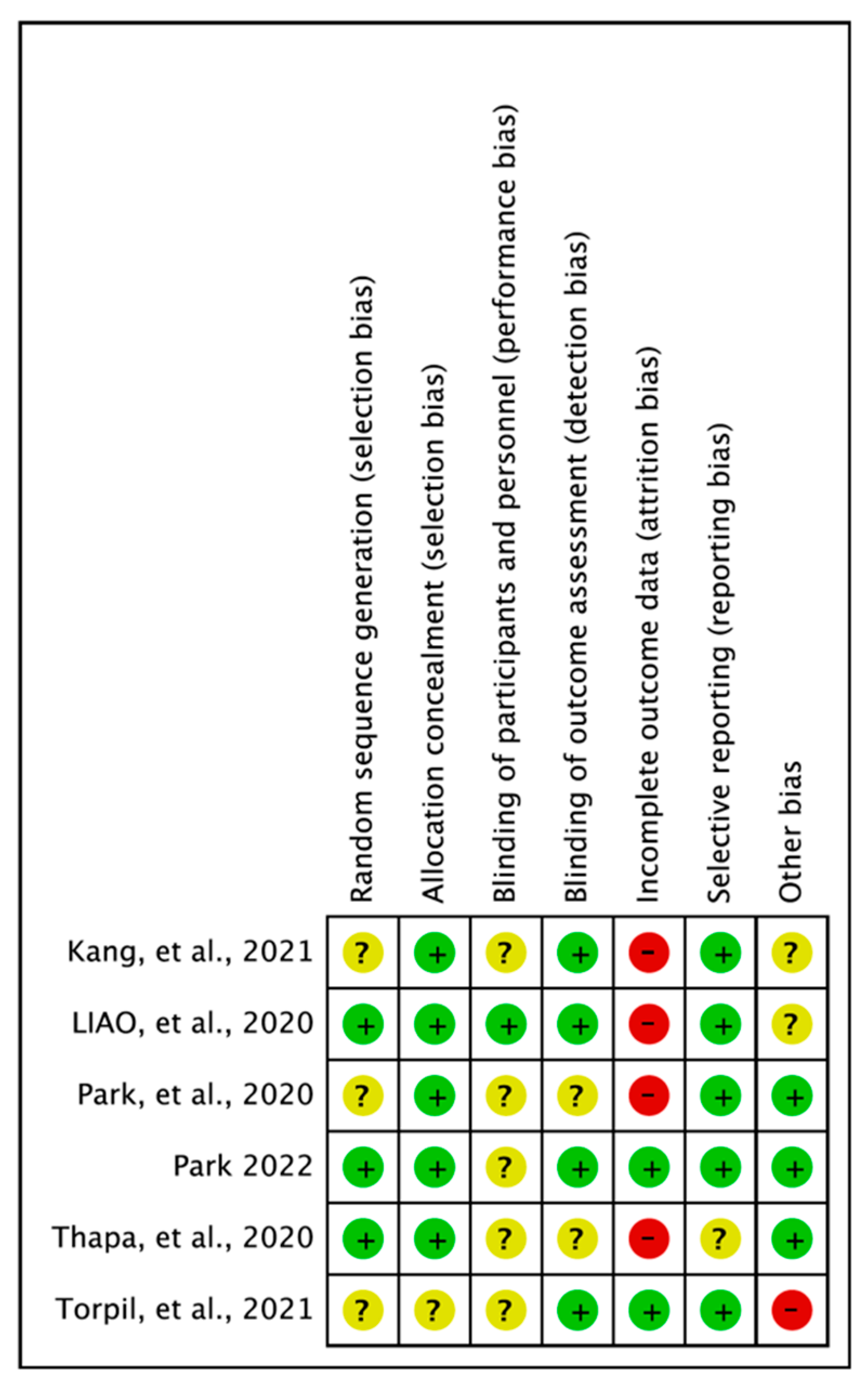
3.2. Assessment of Methodological Quality
3.3. Virtual Reality for Individuals with Mild Cognitive Impairment
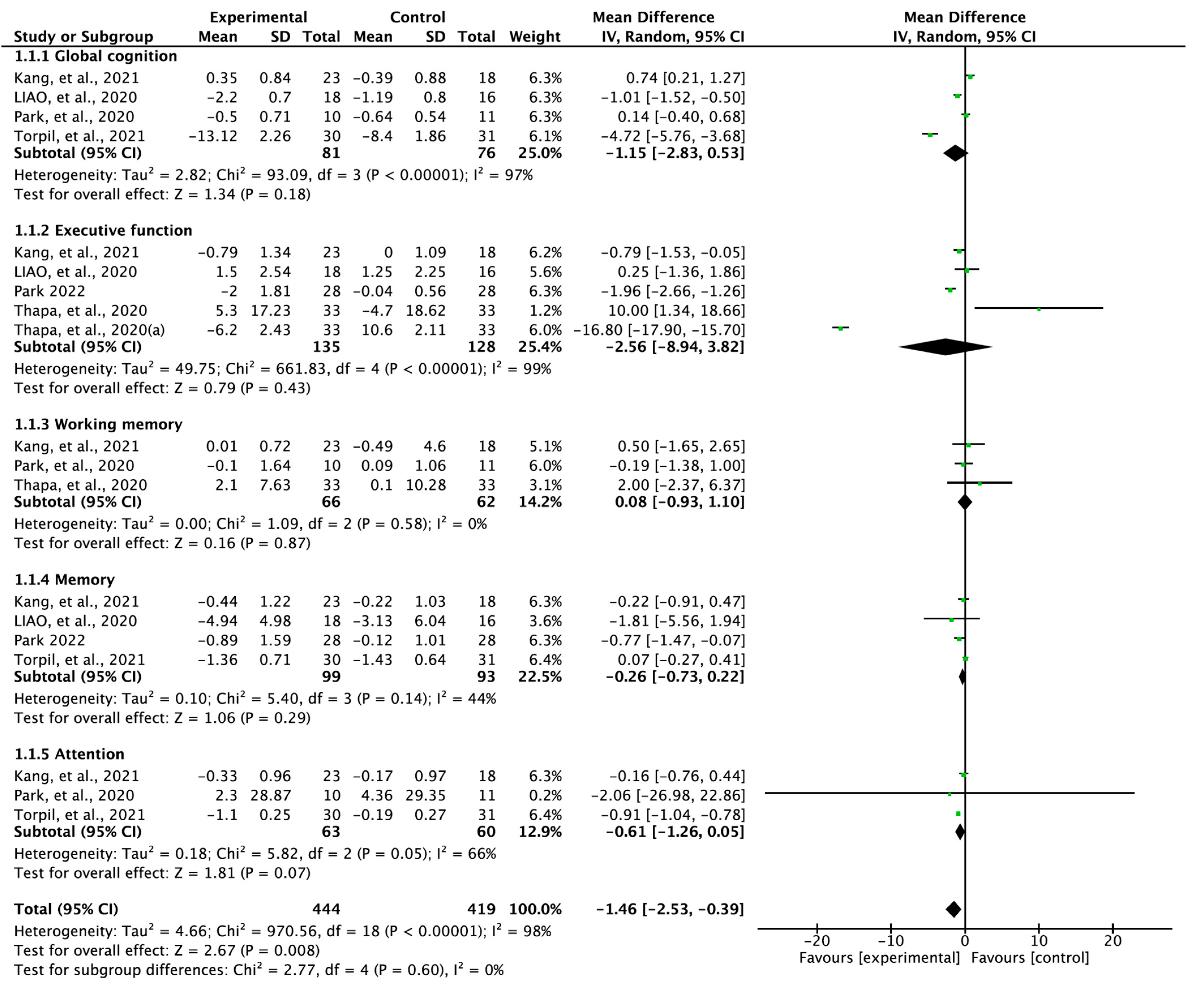
3.4. Effectiveness of Virtual Reality in Treating Mild Cognitive Impairment
3.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef]
- Grueso, S.; Raquel, V.-S. Machine learning methods for predicting progression from mild cognitive impairment to Alzheimer’s disease dementia: A systematic review. Alzheimers Res. Ther. 2021, 13, 1–29. [Google Scholar] [CrossRef]
- Petersen, R.C.; Lopez, O.; Armstrong, M.J.; Getchius, T.S.D.; Ganguli, M.; Gloss, D.; Gronseth, G.S.; Marson, D.; Pringsheim, T.; Day, G.S. Practice guideline update summary: Mild cognitive impairment: Report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology 2018, 90, 126–135. [Google Scholar] [CrossRef]
- Langa, K.M.; Levine, D.A. The diagnosis and management of mild cognitive impairment: A clinical review. Jama 2014, 312, 2551–2561. [Google Scholar] [CrossRef]
- Halter, J.; Ouslander, J.; Tinetti, M.; Studenski, S.; High, K.; Asthana, S. Hazzard’s Geriatric Medicine and Gerontology; McGraw-Hill Professional: New York, NY, USA, 2009. [Google Scholar]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Nelson, A.P.; O’Connor, M.G. Mild cognitive impairment: A neuropsychological perspective. CNS Spectr. 2008, 13, 56–64. [Google Scholar] [CrossRef]
- Wild, K.; Howieson, D.; Webbe, F.; Seelye, A.; Kaye, J. Status of computerized cognitive testing in aging: A systematic review. Alzheimers Dement. 2008, 4, 428–437. [Google Scholar] [CrossRef]
- Daviglus, M.L.; Bell, C.C.; Berrettini, W.; Bowen, P.E.; Connolly, E.S., Jr.; Cox, N.J.; Dunbar-Jacob, J.M.; Granieri, E.C.; Hunt, G.; McGarry, K. National Institutes of Health state-of-the-science conference statement: Preventing Alzheimer disease and cognitive decline. Ann. Intern. Med. 2010, 153, 176–181. [Google Scholar] [CrossRef]
- Park, H.; Park, J.H.; Na, H.R.; Hiroyuki, S.; Kim, G.M.; Jung, M.K.; Kim, W.K.; Park, K.W. Combined intervention of physical activity, aerobic exercise, and cognitive exercise intervention to prevent cognitive decline for patients with mild cognitive impairment: A randomized controlled clinical study. J. Clin. Med. 2019, 8, 940. [Google Scholar] [CrossRef]
- Zucchella, C.; Sinforiani, E.; Tamburin, S.; Federico, A.; Mantovani, E.; Bernini, S.; Casale, R.; Bartolo, M. The multidisciplinary approach to Alzheimer’s disease and dementia. A narrative review of non-pharmacological treatment. Front. Neurol. 2018, 9, 1058. [Google Scholar] [CrossRef]
- Htut, T.Z.C.; Hiengkaew, V.; Jalayondeja, C.; Vongsirinavarat, M. Effects of physical, virtual reality-based, and brain exercise on physical, cognition, and preference in older persons: A randomized controlled trial. Eur. Rev. Aging Phys. Act. 2018, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Optale, G.; Urgesi, C.; Busato, V.; Marin, S.; Piron, L.; Priftis, K.; Gamberini, L.; Capodieci, S.; Bordin, A. Controlling memory impairment in elderly adults using virtual reality memory training: A randomized controlled pilot study. Neurorehabil. Neural Repair 2010, 24, 348–357. [Google Scholar] [CrossRef] [PubMed]
- Kim, O.; Pang, Y.; Kim, J.-H. The effectiveness of virtual reality for people with mild cognitive impairment or dementia: A meta-analysis. BMC Psychiatry 2019, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Li, X.; Lai, F.H.-Y. The effect of virtual reality on executive function in older adults with mild cognitive impairment: A systematic review and meta-analysis. Aging Ment. Health 2022, 1–11. [Google Scholar] [CrossRef]
- Papaioannou, T.; Voinescu, A.; Petrini, K.; Fraser, D.S. Efficacy and moderators of virtual reality for cognitive training in people with dementia and mild cognitive impairment: A systematic review and meta-analysis. J. Alzheimers Dis. 2022, 1–30. [Google Scholar] [CrossRef]
- Yan, M.; Zhao, Y.; Meng, Q.; Wang, S.; Ding, Y.; Liu, Q.; Yin, H.; Chen, L. Effects of virtual reality combined cognitive and physical interventions on cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis. Aging Res. Rev. 2022, 101708. [Google Scholar] [CrossRef]
- Chao, G.; Chen, L. Meta-analysis of virtual reality based on delaying mild cognitive impairment. J. Nerv. Ment. Dis. 2022, 210, 194–198. [Google Scholar] [CrossRef]
- Zhu, S.; Sui, Y.; Shen, Y.; Zhu, Y.; Ali, N.; Guo, C.; Wang, T. Effects of virtual reality intervention on cognition and motor function in older adults with mild cognitive impairment or dementia: A systematic review and meta-analysis. Front. Aging Neurosci. 2021, 13, 586999. [Google Scholar] [CrossRef]
- Wu, J.; Ma, Y.; Ren, Z. Rehabilitative effects of virtual reality technology for mild cognitive impairment: A systematic review with meta-analysis. Front. Psychol. 2020, 11, 1811. [Google Scholar] [CrossRef]
- Zhong, D.; Chen, L.; Feng, Y.; Song, R.; Huang, L.; Liu, J.; Zhang, L. Effects of virtual reality cognitive training in individuals with mild cognitive impairment: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 2021, 36, 1829–1847. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G.; Cochrane Statistical Methods Group. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2019; pp. 241–284. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Kang, J.M.; Kim, N.; Lee, S.Y.; Woo, S.K.; Park, G.; Yeon, B.K.; Park, J.W.; Youn, J.-H.; Ryu, S.-H.; Lee, J.-Y. Effect of cognitive training in fully immersive virtual reality on visuospatial function and frontal-occipital functional connectivity in predementia: Randomized controlled trial. J. Med. Internet Res. 2021, 23, e24526. [Google Scholar] [CrossRef]
- Liao, Y.-Y.; Tseng, H.-Y.; Lin, Y.-J.; Wang, C.-J.; Hsu, W.-C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 2020, 56, 47–57. [Google Scholar] [CrossRef]
- Park, J.-H. Effects of virtual reality-based spatial cognitive training on hippocampal function of older adults with mild cognitive impairment. Int. Psychogeriatr. 2022, 34, 157–163. [Google Scholar] [CrossRef]
- Park, J.-H.; Liao, Y.; Kim, D.-R.; Song, S.; Lim, J.H.; Park, H.; Lee, Y.; Park, K.W. Feasibility and tolerability of a culture-based virtual reality (Vr) training program in patients with mild cognitive impairment: A randomized controlled pilot study. Int. J. Environ. Res. Public Health 2020, 17, 3030. [Google Scholar] [CrossRef]
- Thapa, N.; Park, H.J.; Yang, J.-G.; Son, H.; Jang, M.; Lee, J.; Kang, S.W.; Park, K.W.; Park, H. The effect of a virtual reality-based intervention program on cognition in older adults with mild cognitive impairment: A randomized control trial. J. Clin. Med. 2020, 9, 1283. [Google Scholar] [CrossRef]
- Torpil, B.; Şahin, S.; Pekçetin, S.; Uyanık, M. The effectiveness of a virtual reality-based intervention on cognitive functions in older adults with mild cognitive impairment: A single-blind, randomized controlled trial. Games Health 2021, 10, 109–114. [Google Scholar] [CrossRef]
- Babic, A.; Pijuk, A.; Brázdilová, L.; Georgieva, Y.; Pereira, M.A.R.; Pericic, T.P.; Puljak, L. The judgement of biases included in the category “other bias” in cochrane systematic reviews of interventions: A systematic survey. BMC Med. Res. Methodol. 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The montreal cognitive assessment, Moca: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Zwecker, M.; Levenkrohn, S.; Fleisig, Y.; Zeilig, G.; Ohry, A.; Adunsky, A. Mini-mental state examination, cognitive fim instrument, and the loewenstein occupational therapy cognitive assessment: Relation to functional outcome of stroke patients. Arch. Phys. Med. Rehabil. 2002, 83, 342–345. [Google Scholar] [CrossRef]
- Tamura, I.; Kikuchi, S.; Otsuki, M.; Kitagawa, M.; Tashiro, K. Deficits of working memory during mental calculation in patients with Parkinson’s disease. J. Neurol. Sci. 2003, 209, 19–23. [Google Scholar] [CrossRef]
- Crowe, S.F. The differential contribution of mental tracking, cognitive flexibility, visual search, and motor speed to performance on parts a and b of the trail making test. J. Clin. Psychol. 1998, 54, 585–591. [Google Scholar] [CrossRef]
- Lynn, R.; Irwing, P. Sex differences in mental arithmetic, digit span, and G defined as working memory capacity. Intelligence 2008, 36, 226–235. [Google Scholar] [CrossRef]
- Jaeger, J. Digit symbol substitution test: The case for sensitivity over specificity in neuropsychological testing. J. Clin. Psychopharmacol. 2018, 38, 513. [Google Scholar] [CrossRef]
- Ho, H.-T.; Lin, S.-I.; Guo, N.-W.; Yang, Y.-C.; Lin, M.-H.; Wang, C.-S. Executive function predict the quality of life and negative emotion in older adults with diabetes: A longitudinal study. Prim. Care Diabetes 2022, 16, 537–542. [Google Scholar] [CrossRef]
- Park, K.W.; Park, H.; Park, J.-H.; Sohn, S.W. P4-112: Sensitive task measure of memory function on the story recall test in patients with mild cognitive impairment and mild Alzheimer’s disease. Alzheimers Dement. 2015, 11, 819. [Google Scholar] [CrossRef]
- Hermann, B.P.; Wyler, A.R.; Steenman, H.; Richey, E.T. The interrelationship between language function and verbal learning/memory performance in patients with complex partial seizures. Cortex 1988, 24, 245–253. [Google Scholar] [CrossRef]
- Dos Santos, A.; Carolina, E.; Capovilla, A.G.S.; Capovilla, F.C. Computerized stroop test to assess selective attention in children with attention deficit hyperactivity disorder. Span. J. Psychol. 2007, 10, 33–40. [Google Scholar]
- Page, M.J.; Higgins, J.P.T.; Sterne, J.A.C. Assessing risk of bias due to missing results in a synthesis. Cochrane Handb. Syst. Rev. Interv. 2019, 349–374. [Google Scholar]
- Cherniack, E.P. Not just fun and games: Applications of Virtual reality in the identification and rehabilitation of cognitive disorders of the elderly. Disabil. Rehabil. Assist. Technol. 2011, 6, 283–289. [Google Scholar] [CrossRef]
- Tieri, G.; Morone, G.; Paolucci, S.; Iosa, M. Virtual reality in cognitive and motor rehabilitation: Facts, fiction and fallacies. Expert Rev. Med. Devices 2018, 15, 107–117. [Google Scholar] [CrossRef]
- Subramanian, S.K.; Lourenço, C.B.; Chilingaryan, G.; Sveistrup, H.; Levin, M.F. Arm motor recovery using a virtual reality intervention in chronic stroke: Randomized control trial. Neurorehabil. Neural. Repair 2013, 27, 13–23. [Google Scholar] [CrossRef]
- Coyle, H.; Traynor, V.; Solowij, N. Computerized and virtual reality cognitive training for individuals at high risk of cognitive decline: Systematic review of the literature. Am. J. Geriatr. Psychiatry 2015, 23, 335–359. [Google Scholar] [CrossRef]
- Meehan, M.; Razzaque, S.; Insko, B.; Whitton, M.; Brooks, F.P. Review of four studies on the use of physiological reaction as a measure of presence in stressfulvirtual environments. Appl. Psychophysiol. Biofeedback 2005, 30, 239–258. [Google Scholar] [CrossRef]
- Van Schaik, P.; Martyr, A.; Blackman, T.; Robinson, J. Involving persons with dementia in the evaluation of outdoor environments. Cyberpsychol. Behav. 2008, 11, 415–424. [Google Scholar] [CrossRef]
- Liao, Y.-Y.; Chen, I.-H.; Lin, Y.-J.; Chen, Y.; Hsu, W.-C. Effects of virtual reality-based physical and cognitive training on executive function and dual-task gait performance in older adults with mild cognitive impairment: A randomized control trial. Front. Aging Neurosci. 2019, 11, 162. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef]
- Kim, H.-J.; Lee, D.J.; Lee, Y.S. The effect of aerobic exercise on brain-derived neurotrophic factor (Bdnf) in individuals with mild cognitive impairment: A systematic review and meta-analysis of a randomized controlled trials. Phys. Ther. Rehabil. Sci. 2022, 11, 304–310. [Google Scholar] [CrossRef]
- Colcombe, S.J.; Erickson, K.I.; Scalf, P.E.; Kim, J.S.; Prakash, R.; McAuley, E.; Elavsky, S.; Marquez, D.X.; Hu, L.; Kramer, A.F. Aerobic exercise training increases brain volume in aging humans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1166–1170. [Google Scholar] [CrossRef]
- Hötting, K.; Röder, B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci. Biobehav. Rev. 2013, 37, 2243–2257. [Google Scholar] [CrossRef]
- Schmidt, L.; Lebreton, M.; Cléry-Melin, M.-L.; Daunizeau, J.; Pessiglione, M. Neural mechanisms underlying motivation of mental versus physical effort. PLoS Biol. 2012, 10, e1001266. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cognition | Kang et al., 2021 [24] | Liao et al., 2020 [25] | Park 2022 [26] | Park et al., 2020 [27] | Thapa et al., 2020 [28] | Torpil et al., 2021 [29] |
|---|---|---|---|---|---|---|
| Global cognition | MMSE | MoCA | K-MMSE | LOTCA-G | ||
| Working memory | TMT-A | Digit span | TMT-A | |||
| Executive function | TMT-B | EXIT-25 | WAIS-BDT | DSST, TMT-B | ||
| Memory function | SVLT | CVVLT | SVLT | LOTCA-G | ||
| Attention | Stroop test | Stroop test | LOTCA-G |
| Study | Sample Size | Duration | Intervention | Authors’ Conclusion |
|---|---|---|---|---|
| Kang et al., 2021 [24] | EG = 23 CG = 18 | 4 weeks | EG = VR cognitive training twice a week, total eight sessions, fully immersive 3D setting CG = usual care | Fully immersive VR cognitive training had positive effects on the visuospatial function, apathy, affect, and quality of life, and increased frontal-occipital functional connectivity in older individuals in a predementia state. |
| Liao et al., 2020 [25] | EG = 18 CG = 16 | 12 weeks | 60 min per session, three sessions per week, total of 36 sessions EG = VR-based PCT; take mass rapid transit, look for a store, kitchen chef, convenience-store clerk CG = PCT | VR-based physical and cognitive training improved cognitive function. |
| Park, 2022 [26] | EG = 28 CG = 28 | 8 weeks | EG = VR-based spatial cognitive training; 24 sessions (45 min per session, 3 days per week), program in Unity game engine CG = no intervention | VR-based spatial cognitive training might be clinically beneficial for improving spatial cognition and episodic memory in elderly individuals with MCI. |
| Park et al., 2020 [27] | EG = 10 CG = 11 | 3 months | EG = Culture-based VR training; 24 sessions (30 min per day, 2 days per week), training with games (Crows and Seagulls, Janggu, Automated Teller Machine, Shopping in the Mart, Fireworks Party, Fruit Cocktail) CG = no intervention | Culture-based VR training programs did not improve cognitive function. |
| Thapa et al., 2020 [28] | EG = 33 CG = 33 | 8 weeks | EG = VR; 100 min (three 20 min VR training sessions and three 10 min eye massage and stretching sessions), sessions held three times a week, VR training games (juice making, crow shooting, find the number of fireworks, memory object at the house) CG = HCE; 30–50 min per session, one session per week, total eight sessions | VR-based training improved cognitive and physical function in patients with MCI when compared with controls. |
| Torpil et al., 2021 [29] | EG = 30 CG = 31 | 10–12 weeks | 45 min per session, two sessions per week, total 24 sessions EG = Cognitive rehabilitation plus VR; Microsoft Kinect for PC without immersion (Boxing Trainer, Jet Run, Superkick, Air Challenge) CG = cognitive rehabilitation | Using VR applications in CR is recommended to improve cognitive function of older adults with MCI. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.; Jung, J.; Lee, S. Therapeutic Application of Virtual Reality in the Rehabilitation of Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Vision 2022, 6, 68. https://doi.org/10.3390/vision6040068
Kim H, Jung J, Lee S. Therapeutic Application of Virtual Reality in the Rehabilitation of Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Vision. 2022; 6(4):68. https://doi.org/10.3390/vision6040068
Chicago/Turabian StyleKim, Hyunjoong, Jihye Jung, and Seungwon Lee. 2022. "Therapeutic Application of Virtual Reality in the Rehabilitation of Mild Cognitive Impairment: A Systematic Review and Meta-Analysis" Vision 6, no. 4: 68. https://doi.org/10.3390/vision6040068
APA StyleKim, H., Jung, J., & Lee, S. (2022). Therapeutic Application of Virtual Reality in the Rehabilitation of Mild Cognitive Impairment: A Systematic Review and Meta-Analysis. Vision, 6(4), 68. https://doi.org/10.3390/vision6040068