Conjunctival Swab Findings in 484 COVID-19 Patients in Four Hospital Centers in Slovakia

 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization Declares Global Emergency: A Review of the 2019 Novel Coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Vesely, P.; Novakova, E.; Stubna, M.; Trnka, M.; Jurenova, D.; Lyskova, D.; Furda, R.; Plesnikova, P.; Himic, V.; Furdova, A. Coronavirus Disease (COVID-19) and Conjunctival Sac Swab Findings. J. Ophthalmic Inflamm. Infect. 2022, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Li, D.; Fang, J.; Liu, Q.; Cao, W.; Sun, X.; Xu, G. SARS-CoV-2 Receptor ACE2 Is Expressed in Human Conjunctival Tissue, Especially in Diseased Conjunctival Tissue. Ocul. Surf. 2021, 19, 249–251. [Google Scholar] [CrossRef] [PubMed]
- Coroneo, M.T. The Eye as the Discrete but Defensible Portal of Coronavirus Infection. Ocul. Surf. 2021, 19, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Barnett, B.P.; Wahlin, K.; Krawczyk, M.; Spencer, D.; Welsbie, D.; Afshari, N.; Chao, D. Potential of Ocular Transmission of SARS-CoV-2: A Review. Vision 2020, 4, 40. [Google Scholar] [CrossRef]
- Chen, L.; Liu, M.; Zhang, Z.; Qiao, K.; Huang, T.; Chen, M.; Xin, N.; Huang, Z.; Liu, L.; Zhang, G. Ocular Manifestations of a Hospitalised Patient with Confirmed 2019 Novel Coronavirus Disease. Br. J. Ophthalmol. 2020, 104, 748–751. [Google Scholar] [CrossRef]
- Xia, J.; Tong, J.; Liu, M.; Shen, Y.; Guo, D. Evaluation of Coronavirus in Tears and Conjunctival Secretions of Patients with SARS-CoV-2 Infection. J. Med. Virol. 2020, 92, 589–594. [Google Scholar] [CrossRef]
- Sawant, O.B.; Singh, S.; Wright, R.E.; Jones, K.M.; Titus, M.S.; Dennis, E.; Hicks, E.; Majmudar, P.A.; Kumar, A.; Mian, S.I. Prevalence of SARS-CoV-2 in Human Post-Mortem Ocular Tissues. Ocul. Surf. 2021, 19, 322–329. [Google Scholar] [CrossRef]
- Kumar, K.; Prakash, A.A.; Gangasagara, S.B.; Rathod, S.B.L.; Ravi, K.; Rangaiah, A.; Shankar, S.M.; Basawarajappa, S.G.; Bhushan, S.; Neeraja, T.G.; et al. Presence of Viral RNA of SARS-CoV-2 in Conjunctival Swab Specimens of COVID-19 Patients. Indian J. Ophthalmol. 2020, 68, 1015–1017. [Google Scholar] [CrossRef]
- Güemes-Villahoz, N.; Burgos-Blasco, B.; Arribi-Vilela, A.; Arriola-Villalobos, P.; Rico-Luna, C.M.; Cuiña-Sardiña, R.; Delgado-Iribarren, A.; García-Feijoó, J. Detecting SARS-CoV-2 RNA in Conjunctival Secretions: Is It a Valuable Diagnostic Method of COVID-19? J. Med. Virol. 2021, 93, 383–388. [Google Scholar] [CrossRef]
- Zimmerman, K.; Kearns, F.; Tzekov, R. Natural Protection of Ocular Surface from Viral Infections—A Hypothesis. Med. Hypotheses 2020, 143, 110082. [Google Scholar] [CrossRef] [PubMed]
- Belser, J.A.; Rota, P.A.; Tumpey, T.M. Ocular Tropism of Respiratory Viruses. Microbiol. Mol. Biol. Rev. MMBR 2013, 77, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Vabret, A.; Mourez, T.; Dina, J.; van der Hoek, L.; Gouarin, S.; Petitjean, J.; Brouard, J.; Freymuth, F. Human Coronavirus NL63, France. Emerg. Infect. Dis. 2005, 11, 1225–1229. [Google Scholar] [CrossRef] [PubMed]
- Peiris, J.S.M.; Yuen, K.Y.; Osterhaus, A.D.M.E.; Stöhr, K. The Severe Acute Respiratory Syndrome. N. Engl. J. Med. 2003, 349, 2431–2441. [Google Scholar] [CrossRef]
- Loon, S.-C.; Teoh, S.C.B.; Oon, L.L.E.; Se-Thoe, S.-Y.; Ling, A.-E.; Leo, Y.-S.; Leong, H.-N. The Severe Acute Respiratory Syndrome Coronavirus in Tears. Br. J. Ophthalmol. 2004, 88, 861–863. [Google Scholar] [CrossRef]
- Chan, W.M.; Yuen, K.S.C.; Fan, D.S.P.; Lam, D.S.C.; Chan, P.K.S.; Sung, J.J.Y. Tears and Conjunctival Scrapings for Coronavirus in Patients with SARS. Br. J. Ophthalmol. 2004, 88, 968–969. [Google Scholar] [CrossRef]
- Yuen, K.S.C.; Chan, W.-M.; Fan, D.S.P.; Chong, K.K.L.; Sung, J.J.Y.; Lam, D.S.C. Ocular Screening in Severe Acute Respiratory Syndrome. Am. J. Ophthalmol. 2004, 137, 773–774. [Google Scholar] [CrossRef]
- Bonn, D. SARS Virus in Tears? Lancet Infect. Dis. 2004, 4, 480. [Google Scholar] [CrossRef]
- Tong, T.; Lai, T.S. The Severe Acute Respiratory Syndrome Coronavirus in Tears. Br. J. Ophthalmol. 2005, 89, 392. [Google Scholar] [CrossRef][Green Version]
- Wu, P.; Duan, F.; Luo, C.; Liu, Q.; Qu, X.; Liang, L.; Wu, K. Characteristics of Ocular Findings of Patients with Coronavirus Disease 2019 (COVID-19) in Hubei Province, China. JAMA Ophthalmol. 2020, 138, 575–578. [Google Scholar] [CrossRef]
- Loffredo, L.; Pacella, F.; Pacella, E.; Tiscione, G.; Oliva, A.; Violi, F. Conjunctivitis and COVID-19: A Meta-Analysis. J. Med. Virol. 2020, 92, 1413–1414. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, S.; Nagata, N.; Shirato, K.; Kawase, M.; Takeda, M.; Taguchi, F. Efficient Activation of the Severe Acute Respiratory Syndrome Coronavirus Spike Protein by the Transmembrane Protease TMPRSS2. J. Virol. 2010, 84, 12658–12664. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Chen, C.-B.; Jhanji, V.; Xu, C.; Yuan, X.-L.; Liang, J.-J.; Huang, Y.; Cen, L.-P.; Ng, T.K. Expression of SARS-CoV-2 Receptor ACE2 and TMPRSS2 in Human Primary Conjunctival and Pterygium Cell Lines and in Mouse Cornea. Eye 2020, 34, 1212–1219. [Google Scholar] [CrossRef]
- Zhou, L.; Xu, Z.; Castiglione, G.M.; Soiberman, U.S.; Eberhart, C.G.; Duh, E.J. ACE2 and TMPRSS2 Are Expressed on the Human Ocular Surface, Suggesting Susceptibility to SARS-CoV-2 Infection. Ocul. Surf. 2020, 18, 537–544. [Google Scholar] [CrossRef]
- Raboud, J.; Shigayeva, A.; McGeer, A.; Bontovics, E.; Chapman, M.; Gravel, D.; Henry, B.; Lapinsky, S.; Loeb, M.; McDonald, L.C. Risk Factors for SARS Transmission from Patients Requiring Intubation: A Multicentre Investigation in Toronto, Canada. PLoS ONE 2010, 5, e10717. [Google Scholar] [CrossRef]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor Recognition by the Novel Coronavirus from Wuhan: An Analysis Based on Decade-Long Structural Studies of SARS Coronavirus. J. Virol. 2020, 94, e00127-20. [Google Scholar] [CrossRef]
- Ozturker, Z.K. Conjunctivitis as Sole Symptom of COVID-19: A Case Report and Review of Literature. Eur. J. Ophthalmol. 2021, 31, NP161–NP166. [Google Scholar] [CrossRef]
- Robbins, S.G.; Detrick, B.; Hooks, J.J. Ocular Tropisms of Murine Coronavirus (Strain JHM) after Inoculation by Various Routes. Investig. Ophthalmol. Vis. Sci. 1991, 32, 1883–1893. [Google Scholar]
- Nagata, N.; Iwata-Yoshikawa, N.; Taguchi, F. Studies of Severe Acute Respiratory Syndrome Coronavirus Pathology in Human Cases and Animal Models. Vet. Pathol. 2010, 47, 881–892. [Google Scholar] [CrossRef]
- Martina, B.E.E.; Haagmans, B.L.; Kuiken, T.; Fouchier, R.A.M.; Rimmelzwaan, G.F.; van Amerongen, G.; Peiris, J.S.M.; Lim, W.; Osterhaus, A.D.M.E. Virology: SARS Virus Infection of Cats and Ferrets. Nature 2003, 425, 915. [Google Scholar] [CrossRef] [PubMed]
- Andries, K.; Pensaert, M.B. Immunofluorescence Studies on the Pathogenesis of Hemagglutinating Encephalomyelitis Virus Infection in Pigs after Oronasal Inoculation. Am. J. Vet. Res. 1980, 41, 1372–1378. [Google Scholar] [PubMed]
- Doherty, M.J. Ocular Manifestations of Feline Infectious Peritonitis. J. Am. Vet. Med. Assoc. 1971, 159, 417–424. [Google Scholar] [PubMed]
- Lai, Y.L.; Jacoby, R.O.; Bhatt, P.N.; Jonas, A.M. Keratoconjunctivitis Associated with Sialodacryoadenitis in Rats. Investig. Ophthalmol. 1976, 15, 538–541. [Google Scholar]
- Ulhaq, Z.S.; Soraya, G.V. The Prevalence of Ophthalmic Manifestations in COVID-19 and the Diagnostic Value of Ocular Tissue/Fluid. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1351–1352. [Google Scholar] [CrossRef]
- Zhou, Y.; Duan, C.; Zeng, Y.; Tong, Y.; Nie, Y.; Yang, Y.; Chen, Z.; Chen, C. Ocular Findings and Proportion with Conjunctival SARS-CoV-2 in COVID-19 Patients. Ophthalmology 2020, 127, 982–983. [Google Scholar] [CrossRef]
- Gunduz, A.; Firat, M.; Turkoglu, G. Comparison of the Simultaneous Conjunctiva and Oropharynx-Nasopharynx Swab Results in Patients Applying to the SARS-CoV-2 Outpatient Clinic for the First Time. J. Med. Virol. 2021, 93, 4516–4522. [Google Scholar] [CrossRef]
- Nasiri, N.; Sharifi, H.; Bazrafshan, A.; Noori, A.; Karamouzian, M.; Sharifi, A. Ocular Manifestations of COVID-19: A Systematic Review and Meta-Analysis. J. Ophthalmic Vis. Res. 2021, 16, 103–112. [Google Scholar] [CrossRef]
- Jones, L.; Walsh, K.; Willcox, M.; Morgan, P.; Nichols, J. The COVID-19 Pandemic: Important Considerations for Contact Lens Practitioners. Contact Lens Anterior Eye 2020, 43, 196–203. [Google Scholar] [CrossRef]
- Lai, T.H.; Tang, E.W.; Chau, S.K.; Fung, K.S.; Li, K.K. Stepping up Infection Control Measures in Ophthalmology during the Novel Coronavirus Outbreak: An Experience from Hong Kong. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 1049–1055. [Google Scholar] [CrossRef]
- Romano, M.R.; Montericcio, A.; Montalbano, C.; Raimondi, R.; Allegrini, D.; Ricciardelli, G.; Angi, M.; Pagano, L.; Romano, V. Facing COVID-19 in Ophthalmology Department. Curr. Eye Res. 2020, 45, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Sadhu, S.; Agrawal, R.; Pyare, R.; Pavesio, C.; Zierhut, M.; Khatri, A.; Smith, J.R.; de Smet, M.D.; Biswas, J. COVID-19: Limiting the Risks for Eye Care Professionals. Ocul. Immunol. Inflamm. 2020, 28, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, S.; Honavar, S.G.; Sachdev, M.S.; Sharma, N.; Kumar, A.; Ram, J.; Shetty, R.; Rao, G.S.; Ramasamy, K.; Khanna, R. All India Ophthalmological Society–Indian Journal of Ophthalmology Consensus Statement on Preferred Practices during the COVID-19 Pandemic. Indian J. Ophthalmol. 2020, 68, 711. [Google Scholar] [PubMed]
- Aggarwal, K.; Agarwal, A.; Jaiswal, N.; Dahiya, N.; Ahuja, A.; Mahajan, S.; Tong, L.; Duggal, M.; Singh, M.; Agrawal, R.; et al. Ocular Surface Manifestations of Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis. PLoS ONE 2020, 15, e0241661. [Google Scholar] [CrossRef]
- Shimmura, S.; Shimazaki, J.; Tsubota, K. Results of a Population-Based Questionnaire on the Symptoms and Lifestyles Associated with Dry Eye. Cornea 1999, 18, 408–411. [Google Scholar] [CrossRef]
- Marinho, P.M.; Marcos, A.A.; Romano, A.C.; Nascimento, H.; Belfort, R. Retinal Findings in Patients with COVID-19. Lancet 2020, 395, 1610. [Google Scholar] [CrossRef]
- Tostmann, A.; Bradley, J.; Bousema, T.; Yiek, W.-K.; Holwerda, M.; Bleeker-Rovers, C.; Ten Oever, J.; Meijer, C.; Rahamat-Langendoen, J.; Hopman, J. Strong Associations and Moderate Predictive Value of Early Symptoms for SARS-CoV-2 Test Positivity among Healthcare Workers, the Netherlands, March 2020. Eurosurveillance 2020, 25, 2000508. [Google Scholar] [CrossRef]
- Zhang, X.; Chen, X.; Chen, L.; Deng, C.; Zou, X.; Liu, W.; Yu, H.; Chen, B.; Sun, X. The Evidence of SARS-CoV-2 Infection on Ocular Surface. Ocul. Surf. 2020, 18, 360–362. [Google Scholar] [CrossRef]
- Jin, Y.-P.; Trope, G.E.; El-Defrawy, S.; Liu, E.Y.; Buys, Y.M. Ophthalmology-Focused Publications and Findings on COVID-19: A Systematic Review. Eur. J. Ophthalmol. 2021, 31, 1677–1687. [Google Scholar] [CrossRef]


{kind=link}
| Gender | Number | Gestational Age a (Years) | Non-Mechanically Ventilated Patients b | Mechanically Ventilated Patients b | Positive Result from the Conjunctival Sac | Eye Symptoms b |
|---|---|---|---|---|---|---|
| Male | 264 | 65.59 ± 13.43 | 215 (26) | 5 (0) | 31 | 36 (4) |
| Female | 220 | 68.01 ± 13.71 | 179 (22) | 6 (2) | 27 | 23 (4) |
| Overall | 484 | 66.69 ± 13.59 | 394 (48) | 11 (2) | 58 | 59 (8) |
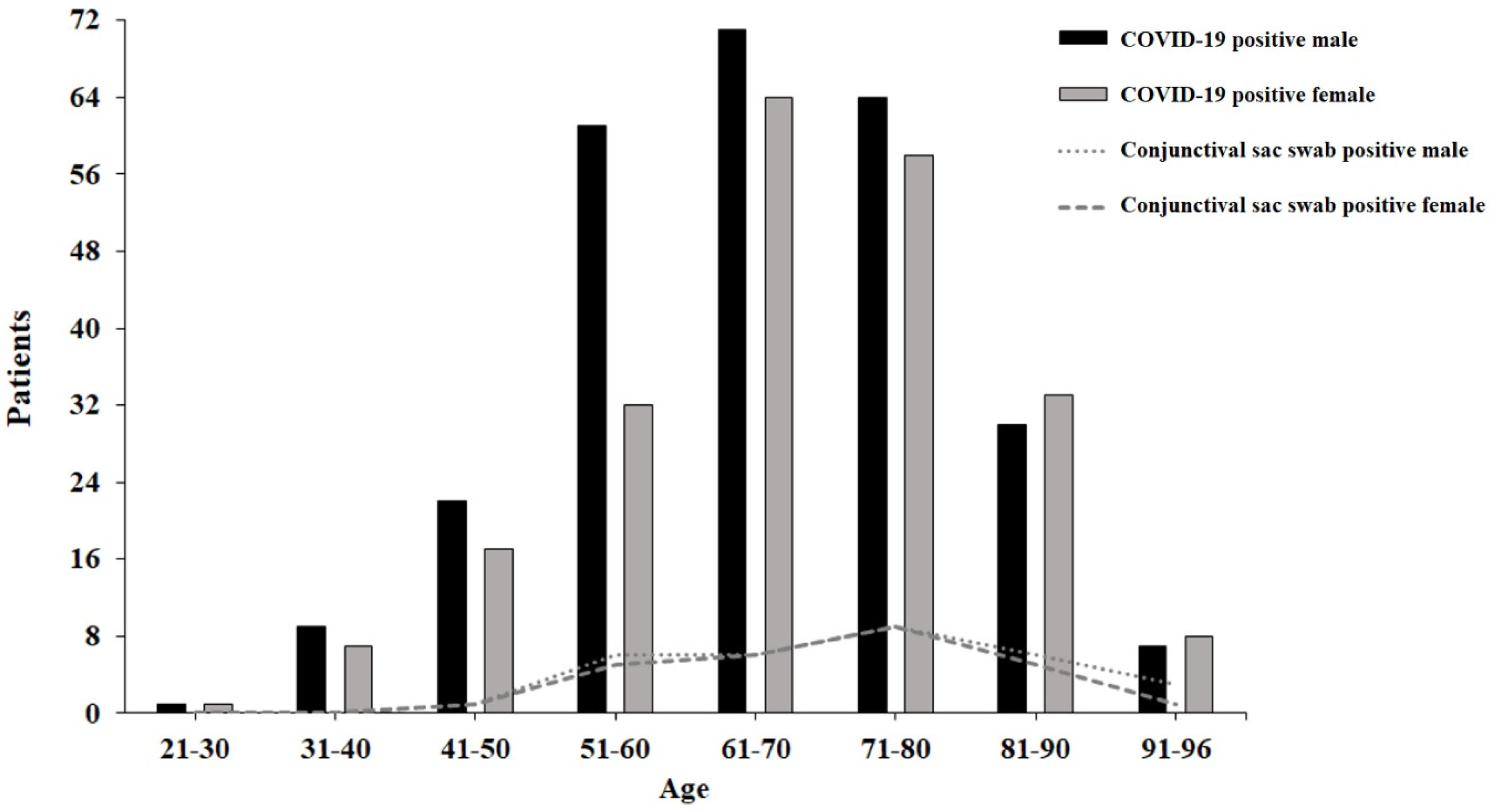
| Age Range (Years) | Male a | Female a | Non-Mechanically Ventilated Patients b | Mechanically Ventilated Patients b | Eye Symptoms b |
|---|---|---|---|---|---|
| 21–30 | 1 (0) | 1 (0) | 1 (1) | 0 (0) | 0 (0) |
| 31–40 | 9 (0) | 7 (0) | 8 (5) | 0 (0) | 0 (0) |
| 41–50 | 22 (1) | 17 (1) | 16 (13) | 0 (1) | 8 (1) |
| 51–60 | 60 (6) | 32 (5) | 46 (25) | 2 (3) | 5 (8) |
| 61–70 | 71 (6) | 64 (6) | 49 (55) | 3 (1) | 9 (9) |
| 71–80 | 64 (9) | 58 (9) | 59 (45) | 0 (1) | 9 (3) |
| 81–90 | 30 (6) | 33 (5) | 29 (29) | 0 (0) | 5 (1) |
| >91 | 7 (3) | 8 (1) | 7 (6) | 0 (0) | 0 (1) |
| Gender | Number | CT Value in Nasopharynx a | CT Value in Conjunctiva a | p |
|---|---|---|---|---|
| Male | 27 | 22.98 ± 5.14 | 29.53 ± 4.11 | <0.001 |
| Female | 31 | 22.47 ± 4.98 | 32.32 ± 3.87 | <0.001 |
| Overall | 58 | 22.71 ± 5.01 | 30.98 ± 4.19 | <0.001 |
| Age Range (Years) | Male | Female | ||||
|---|---|---|---|---|---|---|
| Number | CT Value in Nasopharynx a | CT Value in Conjunctiva a | Number | CT Value in Nasopharynx a | CT Value in Conjunctiva a | |
| 40–49 | 1 | 29.80 ± 0.00 | 33.54 ± 0.00 | 1 | 18.50 ± 0.00 | 32.02 ± 0.00 |
| 50–59 | 6 | 20.87 ± 5.08 | 31.13 ± 4.12 | 5 | 21.78 ± 5.41 | 35.35 ± 2.17 |
| 60–69 | 6 | 21.47 ± 6.60 | 31.11 ± 4.97 | 6 | 26.39 ± 5.01 | 33.28 ± 5.08 |
| 70–79 | 9 | 24.06 ± 6.33 | 29.81 ± 3.92 | 9 | 21.96 ± 4.62 | 33.05 ± 4.22 |
| 80–89 | 6 | 23.60 ± 3.22 | 29.09 ± 5.82 | 5 | 22.49 ± 4.12 | 31.41 ± 1.96 |
| >90 | 3 | 21.51 ± 4.78 | 29.99 ± 3.62 | 1 | 14.00 ± 0.00 | 22.56 ± 0.00 |
| Bratislava | Zilina | Nitra | Nove Zamky | Overall | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number | % a | Number | % a | Number | % a | Number | % | Number | % a | |
| Male | 76 | 51.01 | 70 | 59.83 | 58 | 58.59 | 60 | 50.42 | 264 | 54.55 |
| Female | 73 | 48.99 | 47 | 40.17 | 41 | 41.41 | 59 | 49.58 | 220 | 45.45 |
| Overall | 149 | 100 | 117 | 100 | 99 | 100 | 119 | 100 | 484 | 100 |
| Positive d overall | 25 | 16.78 | 9 | 7.69 | 9 | 9.09 | 15 | 12.61 | 58 | 11.98 |
| Positive d male | 13 | 8.72 | 3 | 2.56 | 7 | 7.07 | 8 | 6.72 | 31 | 6.40 |
| Positive d female | 12 | 8.05 | 6 | 5.13 | 2 | 2.02 | 7 | 5.88 | 27 | 5.58 |
| Negative d overall | 115 | 77.18 | 108 | 92.31 | 90 | 90.91 | 104 | 87.39 | 417 | 86.16 |
| Negative d male | 58 | 38.93 | 67 | 57.26 | 51 | 51.52 | 52 | 43.70 | 228 | 47.11 |
| Negative d female | 57 | 38.26 | 41 | 35.04 | 39 | 39.39 | 52 | 43.70 | 189 | 39.05 |
| Unclear overall | 9 | 6.04 | - | - | - | 9 | 1.86 | |||
| Unclear male | 5 | 3.36 | - | - | - | 5 | 1.03 | |||
| Unclear female | 4 | 2.68 | - | - | - | 4 | 0.83 | |||
| Eye symptoms male | 1 | 0.67 | 27 | 23.08 | 5 | 5.05 | 3 | 2.52 | 36 | 7.42 |
| Eye symptoms female | 1 | 0.67 | 14 | 11.97 | 6 | 6.06 | 2 | 1.68 | 23 | 4.74 |
| Eye symptoms overall | 2 | 1.33 | 41 | 35.04 | 11 | 11.11 | 5 | 4.20 | 59 | 12.16 |
| Number b | Number b | Number b | Number b | Number b | ||||||
| Mean duration c of interval in all patients | 6.13 ± 4.86 | 7.20 ± 3.18 | 13.53 ± 7.13 | 10.79 ± 6.26 | 9.01 ± 6.14 | |||||
| Mean duration c of interval in positive d patients | 5.88 ± 4.68 | 5.89 ± 2.57 | 13.11 ± 7.72 | 9.50 ± 5.52 | 7.85 ± 5.78 | |||||
| Mean duration c of interval in negative d patients | 6.27 ± 4.92 | 7.31 ± 3.21 | 13.57 ± 7.12 | 10.98 ± 6.36 | 9.26 ± 6.18 | |||||
| Average age | 70 ± 13.09 | 62.41 ± 13.60 | 65.59 ± 12.67 | 67.71 ± 13.86 | 66.67 ± 13.59 | |||||
| The average age of the positive d patients | 73.76 ± 14.11 | 69.00 ± 13.35 | 65.33 ± 10.97 | 71.33 ± 9.51 | 71.09 ± 12.53 | |||||
| The average age of the negative d patients | 68.71 ± 12.66 | 61.86 ± 13.53 | 65.62 ± 12.88 | 67.19 ± 14.34 | 65.85 ± 13.58 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furdova, A.; Vesely, P.; Trnka, M.; Novakova, E.; Stubna, M.; Furda, R.; Branikova, L.; Pridavkova, Z. Conjunctival Swab Findings in 484 COVID-19 Patients in Four Hospital Centers in Slovakia. Vision 2022, 6, 46. https://doi.org/10.3390/vision6030046
Furdova A, Vesely P, Trnka M, Novakova E, Stubna M, Furda R, Branikova L, Pridavkova Z. Conjunctival Swab Findings in 484 COVID-19 Patients in Four Hospital Centers in Slovakia. Vision. 2022; 6(3):46. https://doi.org/10.3390/vision6030046
Chicago/Turabian StyleFurdova, Alena, Pavol Vesely, Michal Trnka, Elena Novakova, Michal Stubna, Robert Furda, Lubica Branikova, and Zuzana Pridavkova. 2022. "Conjunctival Swab Findings in 484 COVID-19 Patients in Four Hospital Centers in Slovakia" Vision 6, no. 3: 46. https://doi.org/10.3390/vision6030046
APA StyleFurdova, A., Vesely, P., Trnka, M., Novakova, E., Stubna, M., Furda, R., Branikova, L., & Pridavkova, Z. (2022). Conjunctival Swab Findings in 484 COVID-19 Patients in Four Hospital Centers in Slovakia. Vision, 6(3), 46. https://doi.org/10.3390/vision6030046