Use of Plasma Rich in Growth Factors and ReGeneraTing Agent Matrix for the Treatment of Corneal Diseases

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Desing
2.2. Treatment
2.3. PRGF Preparation
2.4. Follow-Up Period
2.5. Outcomes Measures
2.6. Statistical Analysis
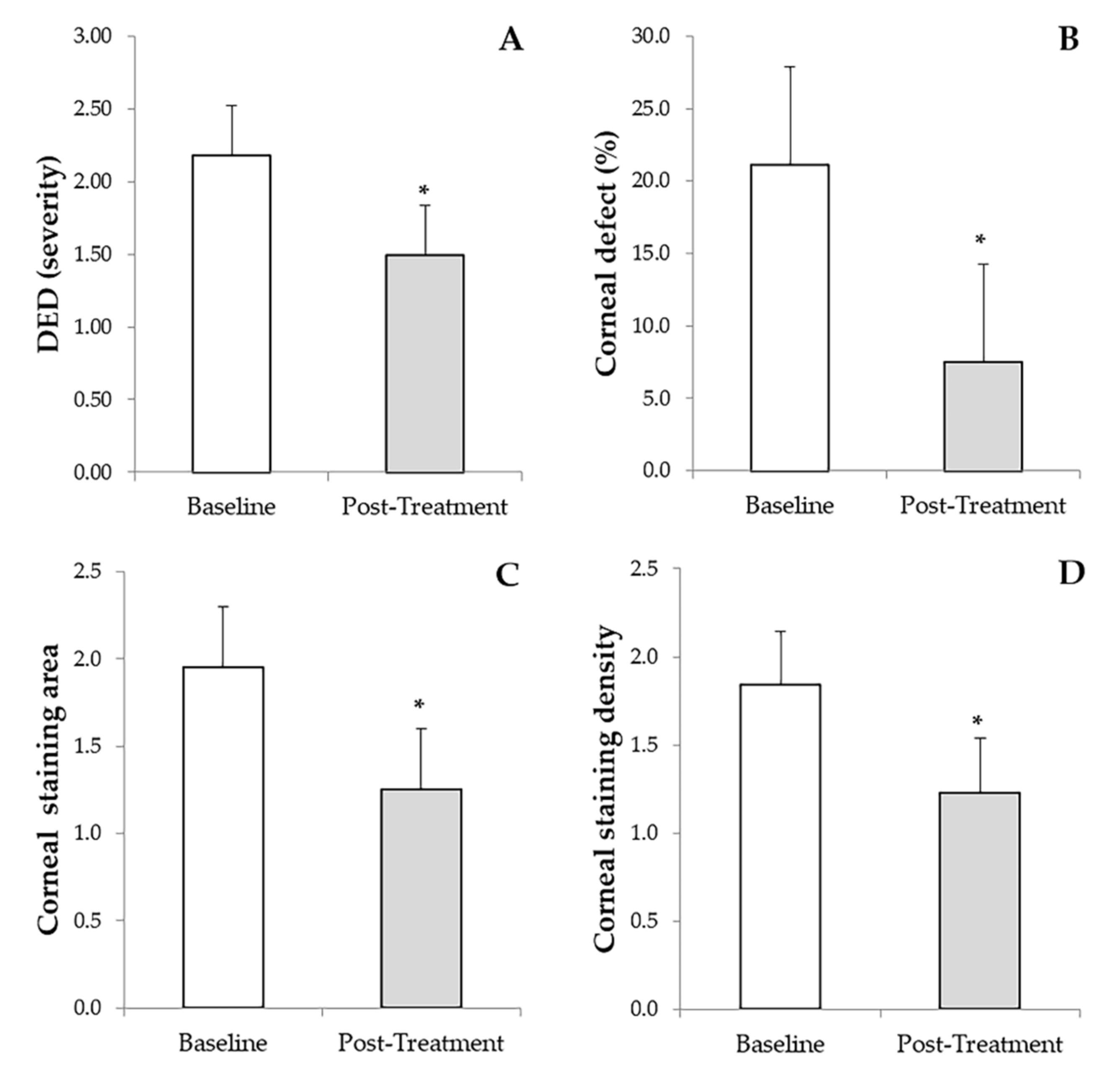
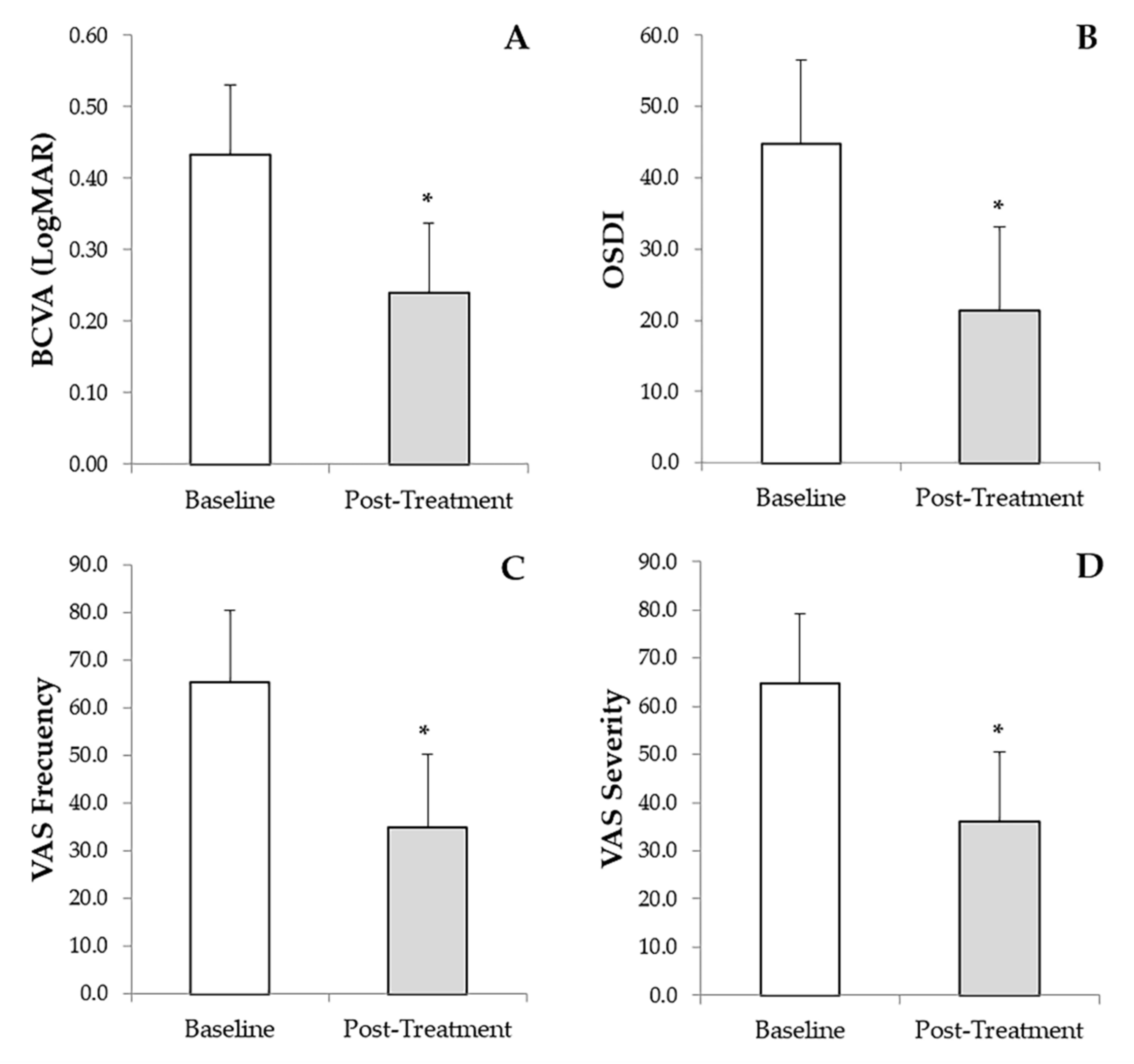
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Merayo-Lloves, J.; Sanchez, R.M.; Riestra, A.C.; Anitua, E.; Begoña, L.; Orive, G.; Fernandez-Vega, L. Autologous Plasma Rich in Growth Factors Eyedrops in Refractory Cases of Ocular Surface Disorders. Ophthalmic Res. 2016, 55, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Bremond-Gignac, D.; Daruich, A.; Robert, M.P.; Chiambaretta, F. Recent innovations with drugs in clinical trials for neurotrophic keratitis and refractory corneal ulcers. Expert Opin. Investig. Drugs 2019, 28, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Sakimoto, T.; Ohnishi, T.; Ishimori, A. Simultaneous study of matrix metalloproteinases, proinflammatory cytokines, and soluble cytokine receptors in the tears of noninfectious corneal ulcer patients. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 1451–1456. [Google Scholar] [CrossRef]
- De Paiva, C.; Pflugfelder, S. Rationale for anti-inflammatory therapy in dry eye syndrome. Arq. Bras. Oftalmol. 2008, 71, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, C. Ophthalmology and Eye Diseases Safety and Efficacy of Cyclosporine in the Treatment of Chronic Dry Eye. Ophthalmol. Eye Dis. 2014, 6, 37–42. [Google Scholar] [CrossRef]
- Bernabei, F.; Roda, M.; Buzzi, M.; Pellegrini, M.; Giannaccare, G.; Versura, P. Blood-Based Treatments for Severe Dry Eye Disease: The Need of a Consensus. J. Clin. Med. 2019, 8, 1478. [Google Scholar] [CrossRef] [Green Version]
- Anitua, E.; Muruzabal, F.; de la Fuente, M.; Merayo, J.; Duran, J.; Orive, G. Plasma Rich in Growth Factors for the Treatment of Ocular Surface Diseases. Curr. Eye Res. 2016, 41, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Muruzabal, F.; Alcalde, I.; Merayo-Lloves, J.; Orive, G. Plasma rich in growth factors (PRGF-Endoret) stimulates corneal wound healing and reduces haze formation after PRK surgery. Exp. Eye Res. 2013, 115, 153–161. [Google Scholar] [CrossRef]
- Anitua, E.; Muruzabal, F.; De la Fuente, M.; Merayo-Lloves, J.; Orive, G. Effects of heat-treatment on plasma rich in growth factors-derived autologous eye drop. Exp. Eye Res. 2014, 119, 27–34. [Google Scholar] [CrossRef]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef]
- Craig, J.P.; Nelson, J.D.; Azar, D.T.; Belmonte, C.; Bron, A.J.; Chauhan, S.K.; de Paiva, C.S.; Gomes, J.A.P.; Hammitt, K.M.; Jones, L.; et al. TFOS DEWS II Report Executive Summary. Ocul. Surf. 2017, 15, 802–812. [Google Scholar] [CrossRef]
- Tuli, S.S.; Schultz, G.S.; Downer, D.M. Science and strategy for preventing and managing corneal ulceration. Ocul. Surf. 2007, 5, 23–39. [Google Scholar] [CrossRef]
- Goins, K.M. New insights into the diagnosis and treatment of neurotrophic keratopathy. Ocul. Surf. 2005, 3, 96–110. [Google Scholar] [CrossRef]
- Pan, Q.; Angelina, A.; Marrone, M.; Stark, W.J.; Akpek, E.K. Autologous serum eye drops for dry eye [Systematic Review]. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Pelacho, B.; Prado, R.; Aguirre, J.J.; Sánchez, M.; Padilla, S.; Aranguren, X.L.; Abizanda, G.; Collantes, M.; Hernandez, M.; et al. Infiltration of plasma rich in growth factors enhances in vivo angiogenesis and improves reperfusion and tissue remodeling after severe hind limb ischemia. J. Control. Release 2015, 202, 31–39. [Google Scholar] [CrossRef]
- Anitua, E.; Alonso, R.; Girbau, C.; Aguirre, J.J.; Muruzabal, F.; Orive, G. Antibacterial effect of plasma rich in growth factors (PRGF®- Endoret®) against Staphylococcus aureus and Staphylococcus epidermidis strains. Clin. Exp. Dermatol. 2012, 37, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; de la Fuente, M.; Riestra, A.; Merayo-Lloves, J.; Muruzábal, F.; Orive, G. Preservation of Biological Activity of Plasma and Platelet-Derived Eye Drops After Their Different Time and Temperature Conditions of Storage. Cornea 2015, 34, 1144–1148. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Muruzabal, F.; Pino, A.; Merayo-Lloves, J.; Orive, G. Biological Stability of Plasma Rich in Growth Factors Eye Drops After Storage of 3 Months. Cornea 2013, 32, 1380–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, R.J.; Marchesi, S.; Royer, T.; Davis, I.S. The Effect of a Subject-Specific Amount of Lateral Wedge on Knee. J. Orthop. Res. Sept. 2007, 25, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Aifa, A.; Gueudry, J.; Portmann, A.; Delcampe, A.; Muraine, M. Topical treatment with a new matrix therapy agent (RGTA) for the treatment of corneal neurotrophic ulcers. Investig. Ophthalmol. Vis. Sci. 2012, 53, 8181–8185. [Google Scholar] [CrossRef] [Green Version]
- Cejkova, J.; Olmiere, C.; Cejka, C.; Trosan, P.; Holan, V. The healing of alkali-injured cornea is stimulated by a novel matrix regenerating agent (RGTA, CACICOL20)-A biopolymer mimicking heparan sulfates reducing proteolytic, oxidative and nitrosative damage. Histol. Histopathol. 2014, 29, 457–478. [Google Scholar] [CrossRef]
- Alcalde, I.; Íñigo-Portugués, A.; Carreño, N.; Riestra, A.C.; Merayo-Lloves, J.M. Efectos de nuevos agentes regenerativos biomiméticos sobre la cicatrización corneal en un modelo experimental de úlceras posquirúrgicas. Arch. Soc. Esp. Oftalmol. 2015, 90, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Avila, R.M.; Merayo-Lloves, J.; Riestra, A.C.; Fernandez-Vega Cueto, L.; Anitua, E.; Begona, L.; Muruzabal, F.; Orive, G. Treatment of patients with neurotrophic keratitis stages 2 and 3 with plasma rich in growth factors (PRGF-Endoret) eye-drops. Int. Ophthalmol. 2017, 38, 1193–1204. [Google Scholar] [CrossRef] [PubMed]
- Vaquerizo, V.; Plasencia, M.Á.; Arribas, I.; Seijas, R.; Padilla, S.; Orive, G.; Anitua, E. Comparison of intra-articular injections of plasma rich in growth factors (PRGF-Endoret) versus durolane hyaluronic acid in the treatment of patients with symptomatic osteoarthritis: A randomized controlled trial. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1635–1643. [Google Scholar] [CrossRef]
- Aynsley, T.R. The use of insulin in the treatment of corneal ulcers. Br. J. Ophthalmol. 1945, 29, 361–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galvis, V.; Niño, C.A.; Tello, A.; Grice, J.M.; Gómez, M.A. Topical insulin in neurotrophic keratopathy after resection of acoustic neuroma. Arch. Soc. Esp. Oftalmol. 2019, 94, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Yamada, N.; Matsuda, R.; Morishige, N.; Yanai, R.; Chikama, T.I.; Nishida, T.; Ishimitsu, T.; Kamiya, A. Open clinical study of eye-drops containing tetrapeptides derived from substance P and insulin-like growth factor-1 for treatment of persistent corneal epithelial defects associated with neurotrophic keratopathy. Br. J. Ophthalmol. 2008, 92, 896–900. [Google Scholar] [CrossRef]
- Bonini, S.; Lambiase, A.; Rama, P.; Sinigaglia, F.; Allegretti, M.; Chao, W.; Mantelli, F.; Bonini, S.; Lambiase, A.; Rama, P.; et al. Phase II Randomized, Double-Masked, Vehicle-Controlled Trial of Recombinant Human Nerve Growth Factor for Neurotrophic Keratitis. Ophthalmology 2018, 125, 1332–1343. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients/Eyes | 74/79 |
|---|---|
| Affected eye | |
| RE, n (%) | 36 (45.6) |
| LE, n (%) | 43 (54.4) |
| Gender | |
| Female, n (%) | 46 (62.2) |
| Male, n (%) | 28 (37.8) |
| Years | |
| Overall, mean ± SD (range) | 56.8 ± 17.3 (25.9–87.8) |
| Female, mean ± SD (range) | 55.7 ± 17.7 (25.9–86.6) |
| Male, mean ± SD (range) | 58.6 ± 16.7 (30.2–87.8) |
| Corneal disorders | |
| Neurotrophic corneal ulcer, n (%) | 27 (34.2) |
| Herpetic, n (%) | 15 (19.0) |
| Post-LASIK, n (%) | 4 (5.1) |
| Diabetes mellitus, n (%) | 3 (3.8) |
| Traumatic, n (%) | 1 (1.3) |
| Post-PRK, n (%) | 1 (1.3) |
| Anti-glaucoma eye-drops, n (%) | 1 (1.3) |
| GVHD, n (%) | 1 (1.3) |
| Post-phaco, n (%) | 1 (1.3) |
| Severe DED, n (%) | 22 (27.8) |
| Exposure keratopathy (ulcer), n (%) | 12 (15.2) |
| Causticization corneal ulcers, n (%) | 5 (6.3) |
| Persistent epithelial defect, n (%) | 3 (3.8) |
| Post-infection corneal ulcer, n (%) * | 3 (3.8) |
| Chronic cicatricial conjunctivitis, n (%) † | 2 (2.5) |
| Peripheral ulcerative keratitis, n (%) | 2 (2.5) |
| Cogan’s epithelial dystrophy, n (%) | 1 (1.3) |
| Salzmann’s nodular degeneration, n (%) | 1 (1.3) |
| Filamentous keratopathy, n (%) | 1 (1.3) |
| Corneal Disorder | Number of PRGF Cycles (Mean ± SD (Range)) | PRGF Treatment in Months (Mean ± SD (Range)) | Clinic Follow-Up in Months (Mean ± SD (Range)) |
|---|---|---|---|
| Neurotrophic corneal ulcer | 2.6 ± 1.2 (1.0–6.0) | 3.9 ± 1.8 (1.5–9.0) | 43.4 ± 30.5 (0.3–113.4) |
| Severe dry eye disease | 1.9 ± 0.8 (1.0–4.0) | 2.9 ± 1.3 (1.5–6.0) | 46.0 ± 34.5 (0.9–118.8) |
| Exposure keratopathy (ulcer) | 3.3 ± 1.4 (1.0–6.0) | 5.6 ± 2.4 (1.5–9.0) | 54.8 ± 33.8 (1.8–120.8) |
| Corneal ulcer from chemical burns | 2.0 ± 0.0 (2.0–2.0) | 3.0 ± 0.0 (3.0–3.0) | 38.2 ± 33.3 (2.3–68.7) |
| Persistent epithelial defect | 2.7 ± 0.6 (2.0–3.0) | 4.0 ± 0.9 (3.0–4.5) | 42.8 ± 28.0 (10.5 –61.1) |
| Post–infection corneal ulcer | 2.0 ± 0.0 (2.0–2.0) | 4.5 ± 2.6 (3.0–7.5) | 36.1 ± 19.6 (14.5–52.7) |
| Chronic cicatricial conjunctivitis | 6.0 ± 0.0 (6.0–6.0) | 9.0 ± 0.0 (9.0–9.0) | 35.9 ± 42.1 (6.1–65.6) |
| Peripheral ulcerative keratitis | 4.0 ± 2.8 (2.0–6.0) | 6.0 ± 4.2 (3.0–9.0) | 33.5 ± 45.5 (1.3–65.7) |
| Cogan’s epithelial dystrophy | 4.0 | 6.0 | 6.3 |
| Salzmann’s nodular degeneration | 3.0 | 4.5 | 80.5 |
| Filamentous keratopathy | 6.0 | 9.0 | 49.0 |
| Total | 2.6 ± 1.4 (1.0–6.0) | 4.2 ± 2.2 (1.5–9.0) | 44.9 ± 31.5 (0.3–120.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Ávila, R.M.; Uribe-Badillo, E.; Fernández-Vega González, C.; Muruzabal, F.; de la Sen-Corcuera, B.; Baamonde, B.; Quirós, L.M.; Anitua, E.; Merayo-Lloves, J. Use of Plasma Rich in Growth Factors and ReGeneraTing Agent Matrix for the Treatment of Corneal Diseases. Vision 2021, 5, 34. https://doi.org/10.3390/vision5030034
Sánchez-Ávila RM, Uribe-Badillo E, Fernández-Vega González C, Muruzabal F, de la Sen-Corcuera B, Baamonde B, Quirós LM, Anitua E, Merayo-Lloves J. Use of Plasma Rich in Growth Factors and ReGeneraTing Agent Matrix for the Treatment of Corneal Diseases. Vision. 2021; 5(3):34. https://doi.org/10.3390/vision5030034
Chicago/Turabian StyleSánchez-Ávila, Ronald M., Edmar Uribe-Badillo, Carlos Fernández-Vega González, Francisco Muruzabal, Borja de la Sen-Corcuera, Begoña Baamonde, Luis M. Quirós, Eduardo Anitua, and Jesús Merayo-Lloves. 2021. "Use of Plasma Rich in Growth Factors and ReGeneraTing Agent Matrix for the Treatment of Corneal Diseases" Vision 5, no. 3: 34. https://doi.org/10.3390/vision5030034
APA StyleSánchez-Ávila, R. M., Uribe-Badillo, E., Fernández-Vega González, C., Muruzabal, F., de la Sen-Corcuera, B., Baamonde, B., Quirós, L. M., Anitua, E., & Merayo-Lloves, J. (2021). Use of Plasma Rich in Growth Factors and ReGeneraTing Agent Matrix for the Treatment of Corneal Diseases. Vision, 5(3), 34. https://doi.org/10.3390/vision5030034